


Adolescents with a Favorable Mediterranean-Style-Based Pattern Show Higher Cognitive and Academic Achievement: A Cluster Analysis—The Cogni-Action Project

 , , ,
, , ,  ,
,  , ,
, ,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Participants
2.2. Procedures and Measurements
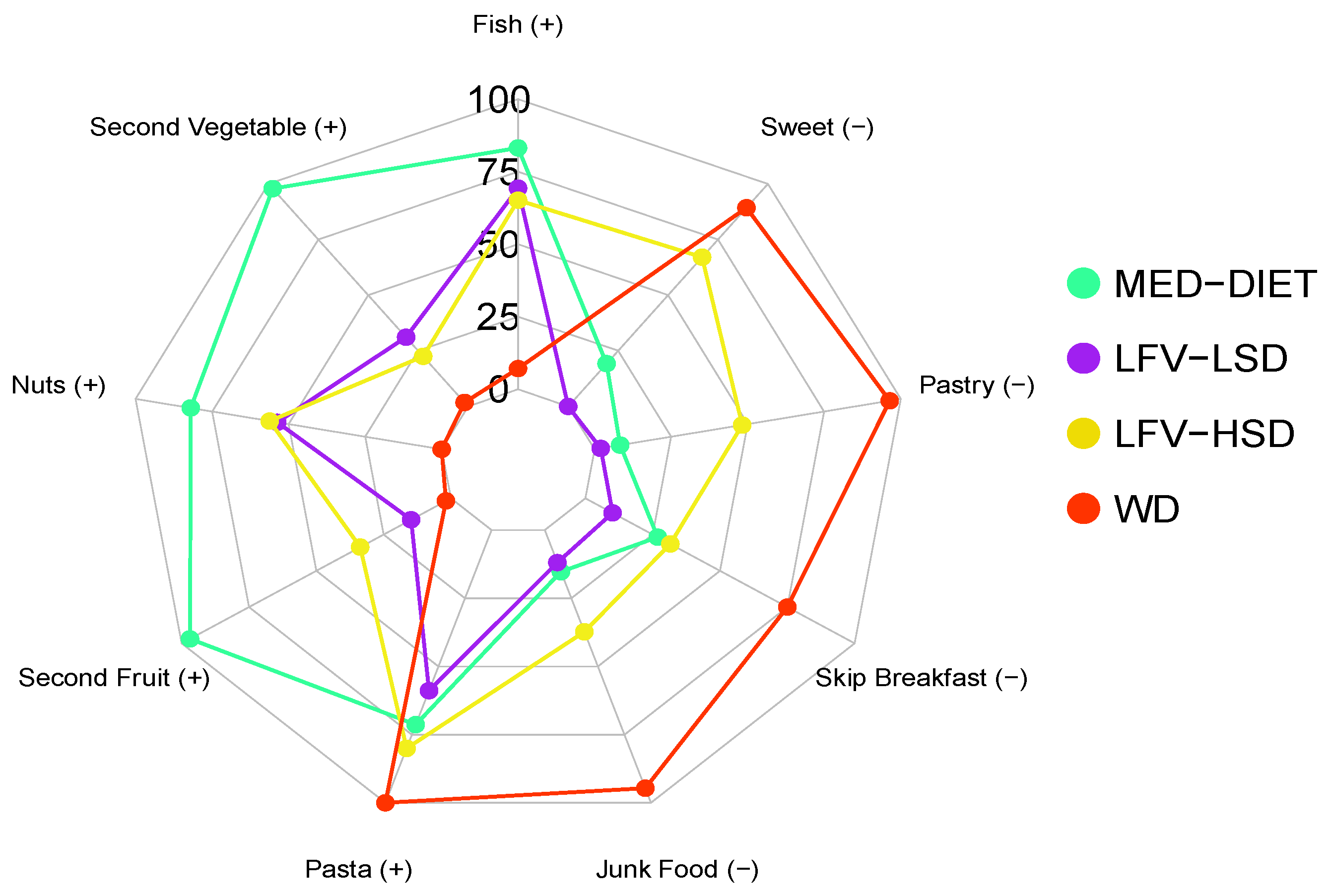
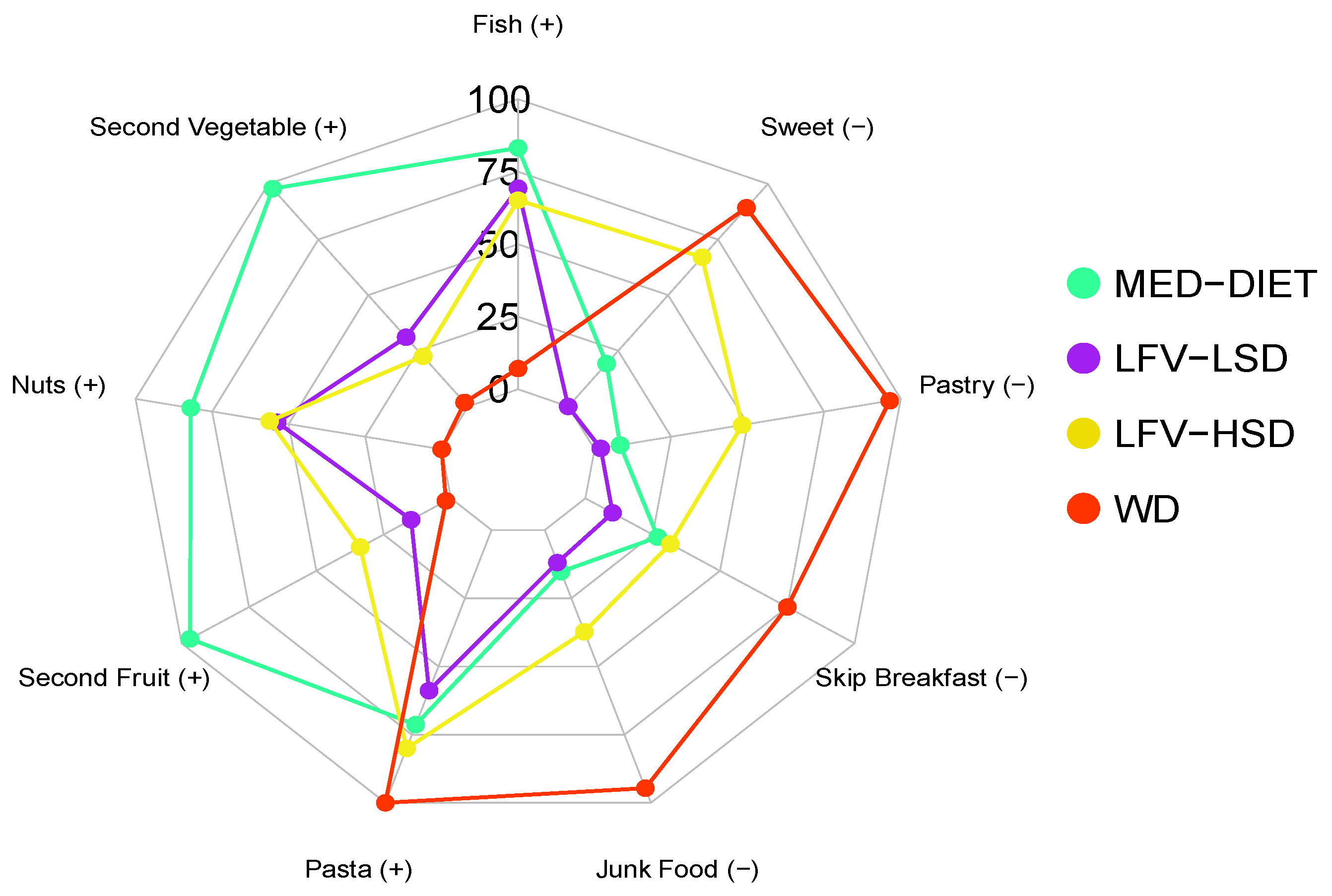
2.3. Mediterranean-Style-Based Pattern
2.4. Academic Achievement (ACA)
2.5. Cognitive Performance
2.6. Covariates
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
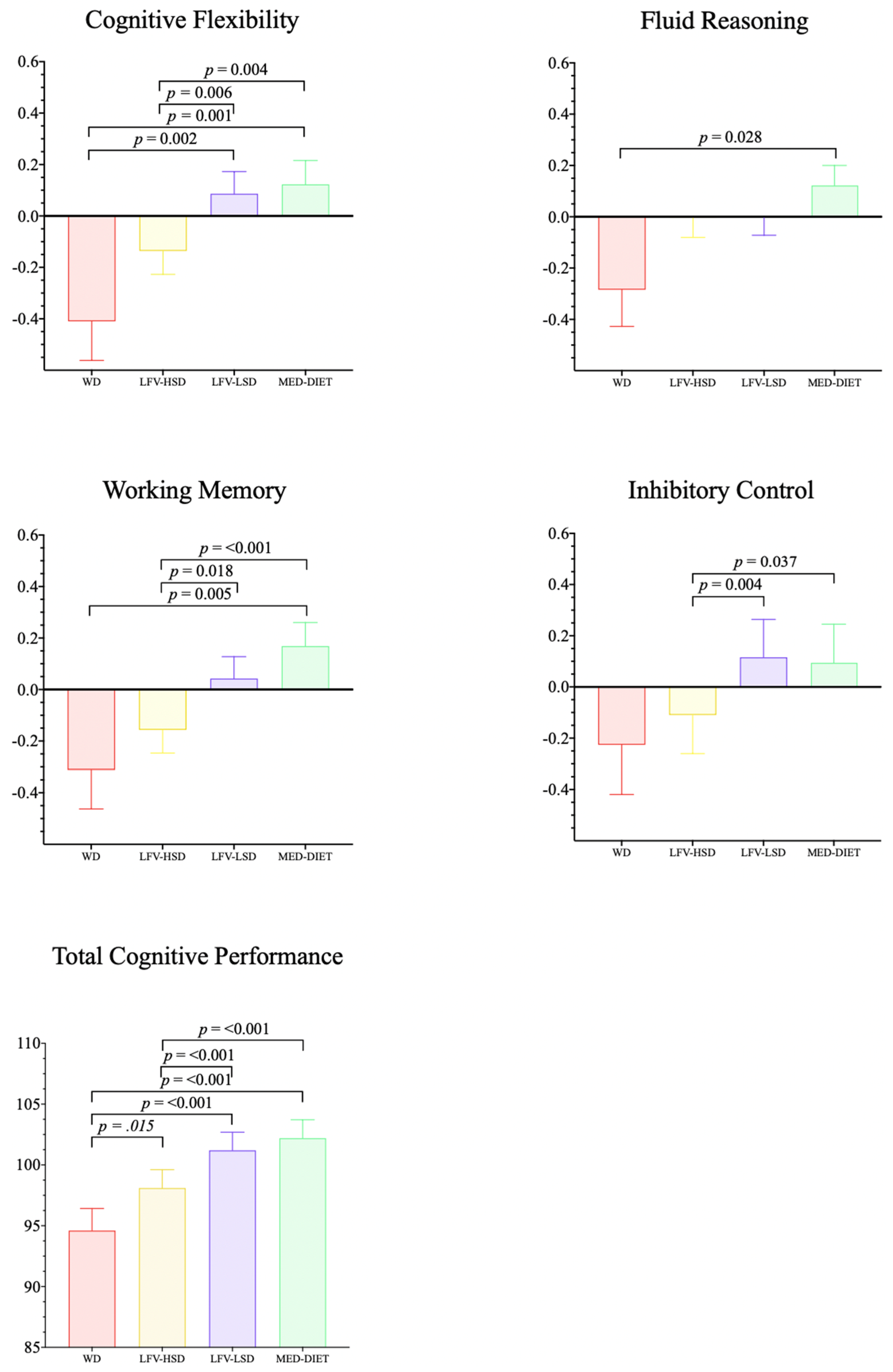
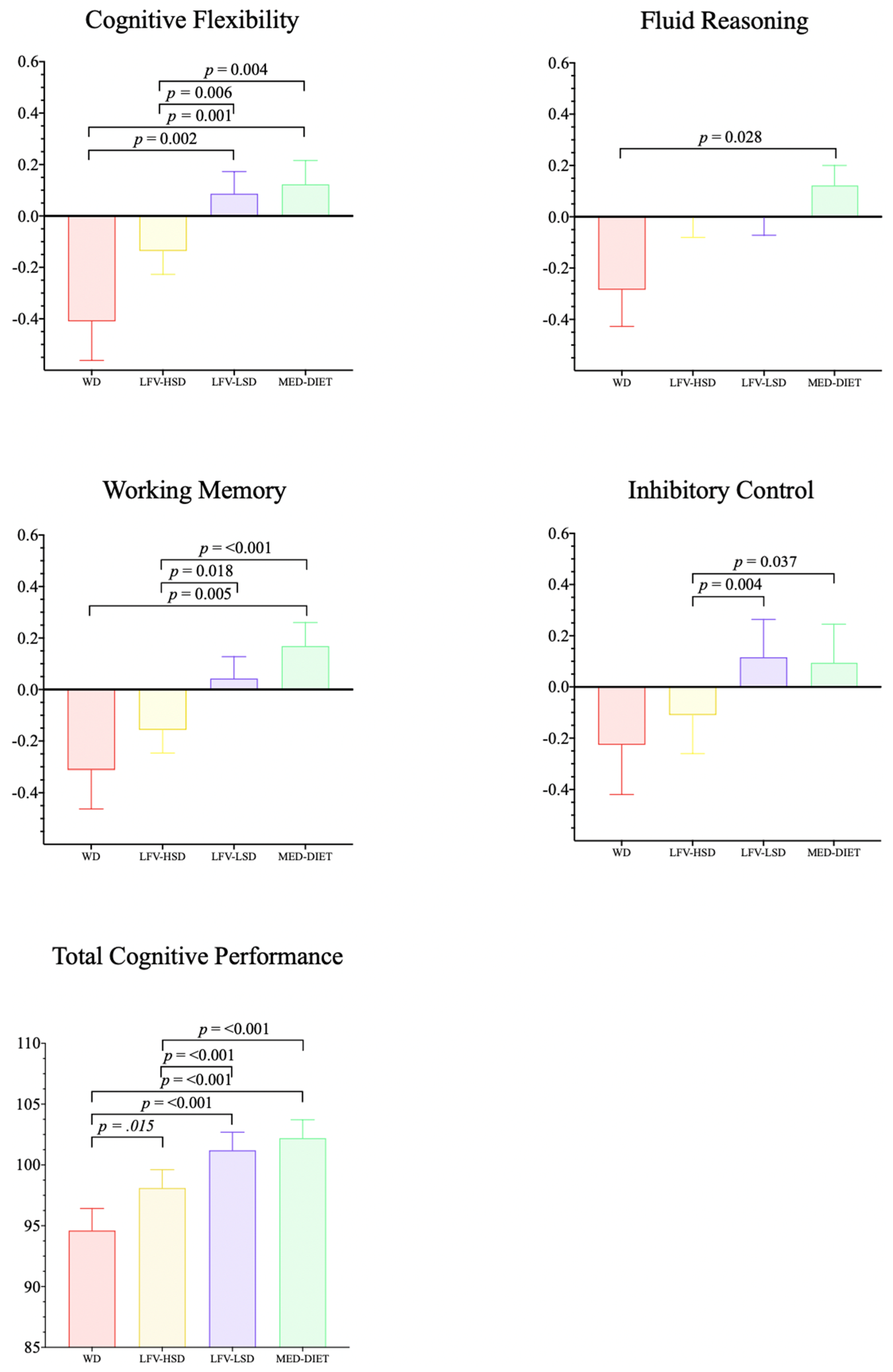
3.2. Differences in Cognitive Performance concerning Clusters
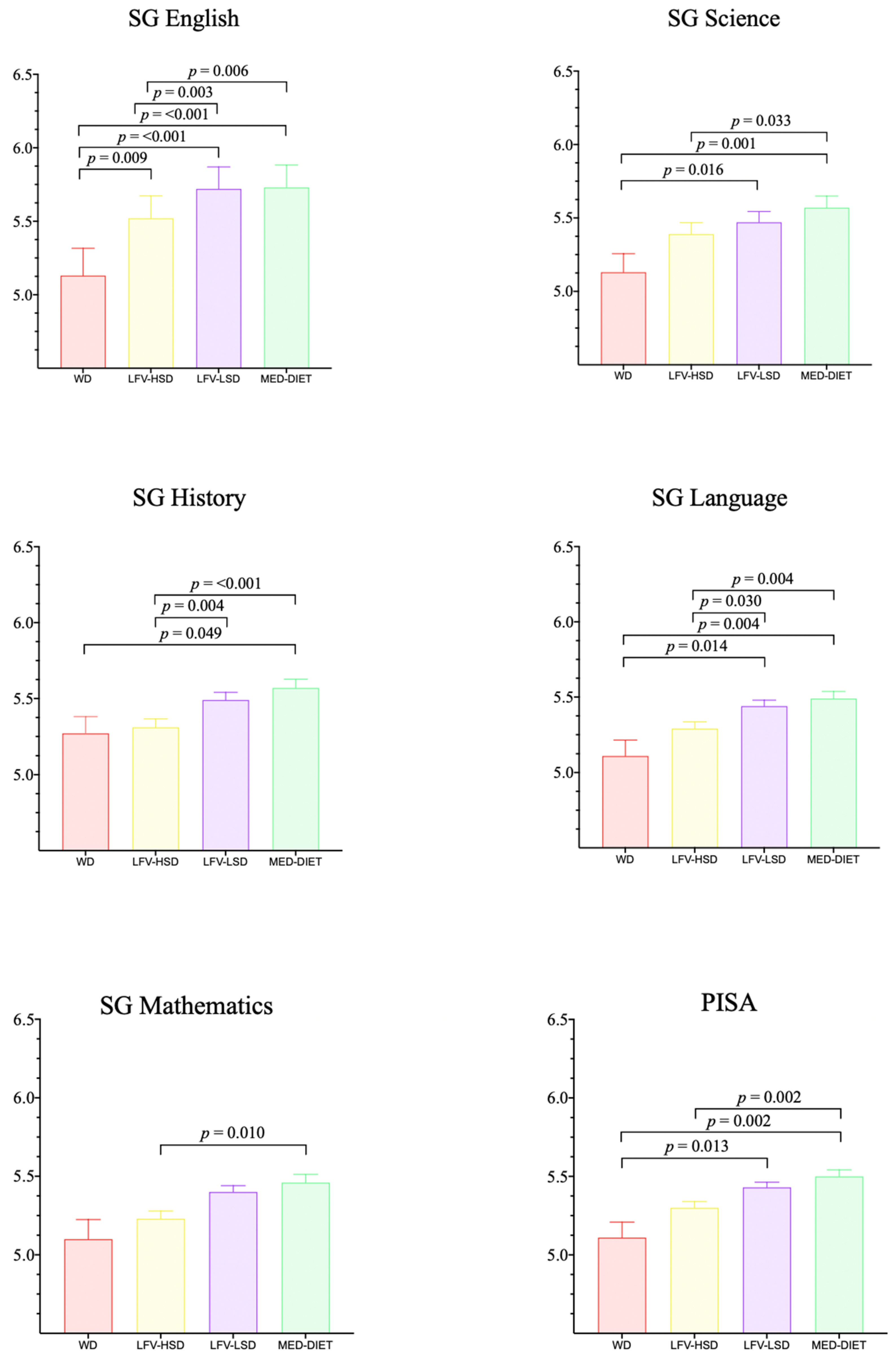
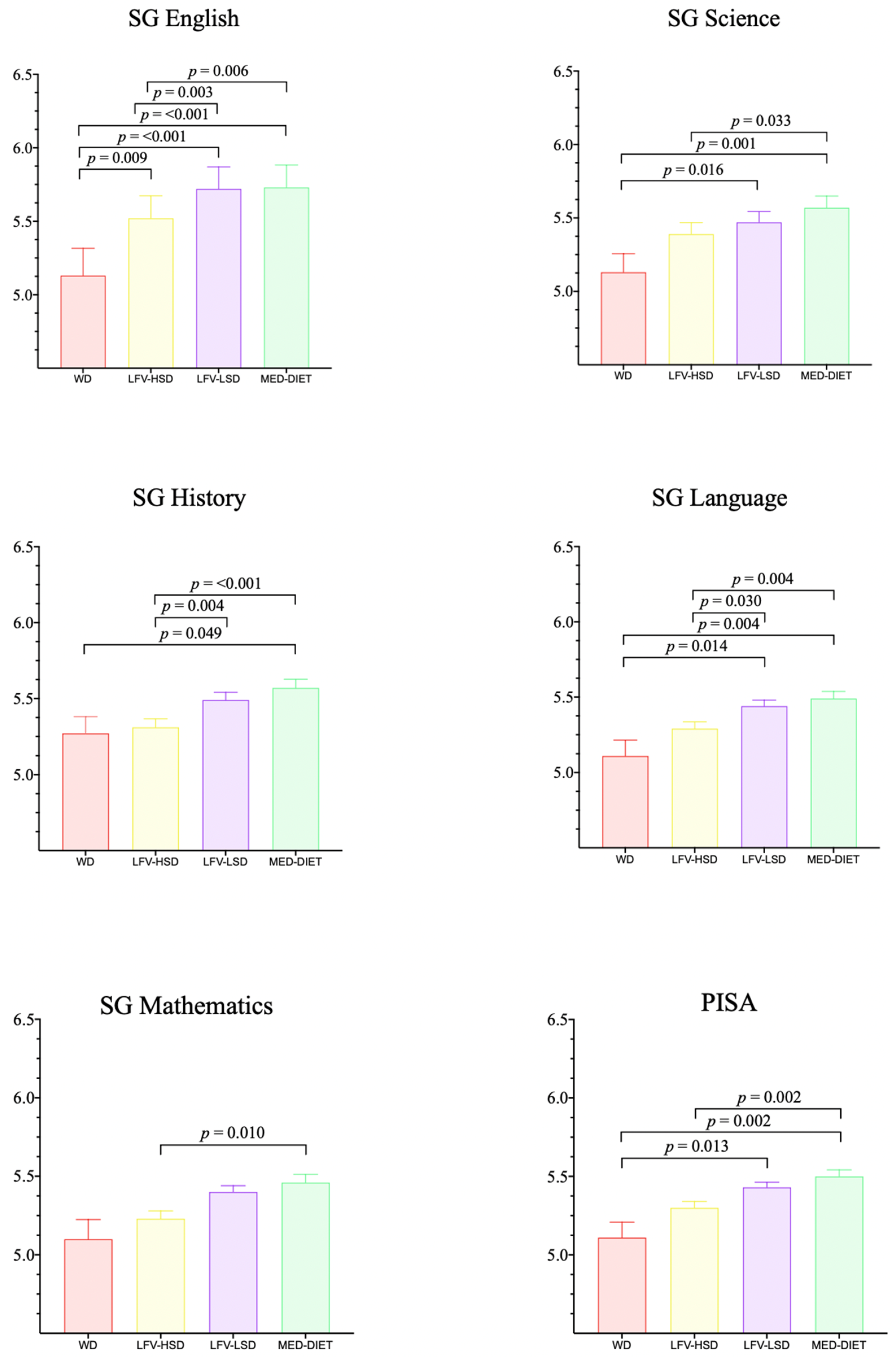
3.3. Differences in Academic Achievement concerning Clusters
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z.; et al. Health Effects of Dietary Risks in 195 Countries, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Song, M.; Eliassen, A.H.; Wang, M.; Fung, T.T.; Clinton, S.K.; Rimm, E.B.; Hu, F.B.; Willett, W.C.; Tabung, F.K.; et al. Optimal Dietary Patterns for Prevention of Chronic Disease. Nat. Med. 2023, 29, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Peña-Jorquera, H.; Cid-Jofré, V.; Landaeta-Díaz, L.; Petermann-Rocha, F.; Martorell, M.; Zbinden-Foncea, H.; Ferrari, G.; Jorquera-Aguilera, C.; Cristi-Montero, C. Plant-Based Nutrition: Exploring Health Benefits for Atherosclerosis, Chronic Diseases, and Metabolic Syndrome—A Comprehensive Review. Nutrients 2023, 15, 3244. [Google Scholar] [CrossRef]
- Naveed, S.; Lakka, T.; Haapala, E.A. An Overview on the Associations between Health Behaviors and Brain Health in Children and Adolescents with Special Reference to Diet Quality. Int. J. Environ. Res. Public. Health 2020, 17, 953. [Google Scholar] [CrossRef] [PubMed]
- Bleiweiss-Sande, R.; Chui, K.; Wright, C.; Amin, S.; Anzman-Frasca, S.; Sacheck, J.M. Associations between Food Group Intake, Cognition, and Academic Achievement in Elementary Schoolchildren. Nutrients 2019, 11, 2722. [Google Scholar] [CrossRef]
- De Amicis, R.; Menichetti, F.; Leone, A. The Effect of the Mediterranean Diet on Metabolic Health. Nutrients 2023, 15, 3397. [Google Scholar] [CrossRef]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Cornejo, I.; Izquierdo-Gomez, R.; Gómez-Martínez, S.; Padilla-Moledo, C.; Castro-Piñero, J.; Marcos, A.; Veiga, O.L. Adherence to the Mediterranean Diet and Academic Performance in Youth: The UP&DOWN Study. Eur. J. Nutr. 2016, 55, 1133–1140. [Google Scholar] [CrossRef]
- Masini, A.; Sanmarchi, F.; Kawalec, A.; Esposito, F.; Scrimaglia, S.; Tessari, A.; Scheier, L.M.; Sacchetti, R.; Dallolio, L. Mediterranean Diet, Physical Activity, and Family Characteristics Associated with Cognitive Performance in Italian Primary School Children: Analysis of the I-MOVE Project. Eur. J. Pediatr. 2023, 182, 917–927. [Google Scholar] [CrossRef]
- Ren, Y.; Peng, C.; Li, Y.; Zhou, F.; Yang, M.; Xiang, B.; Hao, L.; Yang, X.; Zeng, J. The Association between Sugar-Sweetened Beverages and High-Energy Diets and Academic Performance in Junior School Students. Nutrients 2022, 14, 3577. [Google Scholar] [CrossRef]
- Francis, H.; Stevenson, R. The Longer-Term Impacts of Western Diet on Human Cognition and the Brain. Appetite 2013, 63, 119–128. [Google Scholar] [CrossRef]
- Mazereeuw, G.; Lanctôt, K.L.; Chau, S.A.; Swardfager, W.; Herrmann, N. Effects of ω-3 Fatty Acids on Cognitive Performance: A Meta-Analysis. Neurobiol. Aging 2012, 33, 1482.e17–1482.e29. [Google Scholar] [CrossRef]
- Kesse-Guyot, E.; Andreeva, V.A.; Jeandel, C.; Ferry, M.; Hercberg, S.; Galan, P. A Healthy Dietary Pattern at Midlife Is Associated with Subsequent Cognitive Performance. J. Nutr. 2012, 142, 909–915. [Google Scholar] [CrossRef]
- Shi, Y.; Qu, S. The Effect of Cognitive Ability on Academic Achievement: The Mediating Role of Self-Discipline and the Moderating Role of Planning. Front. Psychol. 2022, 13, 1014655. [Google Scholar] [CrossRef] [PubMed]
- Tikhomirova, T.; Malykh, A.; Malykh, S. Predicting Academic Achievement with Cognitive Abilities: Cross-Sectional Study across School Education. Behav. Sci. 2020, 10, 158. [Google Scholar] [CrossRef]
- Tapia-Serrano, M.A.; Esteban-Cornejo, I.; Rodriguez-Ayllon, M.; Vaquero-Solís, M.; Sánchez-Oliva, D.; Sánchez-Miguel, P.A. Adherence to the Mediterranean Diet and Academic Performance in Adolescents: Does BMI Status Moderate This Association? Clin. Nutr. Edinb. Scotl. 2021, 40, 4465–4472. [Google Scholar] [CrossRef]
- Hayek, J.; de Vries, H.; Tueni, M.; Lahoud, N.; Winkens, B.; Schneider, F. Increased Adherence to the Mediterranean Diet and Higher Efficacy Beliefs Are Associated with Better Academic Achievement: A Longitudinal Study of High School Adolescents in Lebanon. Int. J. Environ. Res. Public. Health 2021, 18, 6928. [Google Scholar] [CrossRef]
- Iaccarino Idelson, P.; Scalfi, L.; Valerio, G. Adherence to the Mediterranean Diet in Children and Adolescents: A Systematic Review. Nutr. Metab. Cardiovasc. Dis. NMCD 2017, 27, 283–299. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Ezzatvar, Y.; López-Gil, J.F.; Ramírez-Vélez, R.; Olloquequi, J.; Izquierdo, M. Is Adherence to the Mediterranean Diet Associated with Healthy Habits and Physical Fitness? A Systematic Review and Meta-Analysis Including 565 421 Youths. Br. J. Nutr. 2022, 128, 1433–1444. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, L.; Flores-Barrantes, P.; Moreno, L.A.; Manios, Y.; Gonzalez-Gil, E.M. The Influence of Parental Dietary Behaviors and Practices on Children’s Eating Habits. Nutrients 2021, 13, 1138. [Google Scholar] [CrossRef] [PubMed]
- Zapata-Lamana, R.; Ibarra-Mora, J.; Carrasco-Marín, F.; Durán-Agüero, S.; Cuevas-Aburto, J.; Parra-Rizo, M.A.; Cigarroa, I. Low Sleep Hygiene Is Associated with Less Adherence to the Mediterranean Diet in Chilean Schoolchildren from Rural Public Schools—A Cross-Sectional Study. Children 2023, 10, 1499. [Google Scholar] [CrossRef]
- Desarrollo Biblioteca Del Congreso Nacional|SIIT|Clima y Vegetación Región de Valparaíso. Available online: https://www.bcn.cl/siit/nuestropais/region5/clima.htm (accessed on 13 December 2023).
- Echeverría, G.; Dussaillant, C.; McGee, E.E.; Mena, C.; Nitsche, M.P.; Urquiaga, I.; Bitran, M.; Pedrals, N.; Rigotti, A. Promoting and Implementing the Mediterranean Diet in the Southern Hemisphere: The Chilean Experience. Eur. J. Clin. Nutr. 2019, 72, 38–46. [Google Scholar] [CrossRef]
- Urquiaga, I.; Echeverría, G.; Dussaillant, C.; Rigotti, A. Origen, Componentes y Posibles Mecanismos de Acción de La Dieta Mediterránea. Rev. Méd. Chile 2017, 145, 85–95. [Google Scholar] [CrossRef]
- Camacho, W.J.M.; Zambrano, S.E.O.; Camacho, M.A.M.; Contreras, A.C.H.; Acevedo, A.R.; Valencia, E.J.D.; Cárdenas, A.C.; Alarcón, L.X.N.; Munar, L.C.A.; Sánchez, A.M.N.; et al. Nutritional Status and High Adherence to the Mediterranean Diet in Colombian School Children and Teenagers during the COVID-19 Pandemic According to Sex. J. Nutr. Sci. 2021, 10, e54. [Google Scholar] [CrossRef]
- Minihane, A.M.; Murphy, K.J. The Health Benefits and Practical Considerations for the Adoption of a Mediterranean-Style Dietary Pattern. Br. J. Nutr. 2022, 128, 1201–1205. [Google Scholar] [CrossRef]
- Weller, B.E.; Bowen, N.K.; Faubert, S.J. Latent Class Analysis: A Guide to Best Practice. 2020. Available online: https://journals.sagepub.com/doi/10.1177/0095798420930932 (accessed on 13 December 2023).
- Solis-Urra, P.; Olivares-Arancibia, J.; Suarez-Cadenas, E.; Sanchez-Martinez, J.; Rodríguez-Rodríguez, F.; Ortega, F.B.; Esteban-Cornejo, I.; Cadenas-Sanchez, C.; Castro-Piñero, J.; Veloz, A.; et al. Study Protocol and Rationale of the “Cogni-Action Project” a Cross-Sectional and Randomized Controlled Trial about Physical Activity, Brain Health, Cognition, and Educational Achievement in Schoolchildren. BMC Pediatr. 2019, 19, 260. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Castro-Piñero, J.; España-Romero, V.; Artero, E.G.; Ortega, F.B.; Cuenca, M.M.; Jimenez-Pavón, D.; Chillón, P.; Girela-Rejón, M.J.; Mora, J.; et al. Field-Based Fitness Assessment in Young People: The ALPHA Health-Related Fitness Test Battery for Children and Adolescents. Br. J. Sports Med. 2011, 45, 518–524. [Google Scholar] [CrossRef]
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, Youth and the Mediterranean Diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in Children and Adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef] [PubMed]
- PISA—PISA. Available online: https://www.oecd.org/pisa (accessed on 13 December 2023).
- Morrison, G.E.; Simone, C.M.; Ng, N.F.; Hardy, J.L. Reliability and Validity of the NeuroCognitive Performance Test, a Web-Based Neuropsychological Assessment. Front. Psychol. 2015, 6, 1652. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.H.; Rosales, K.P.; Looney, L. Improving Cognitive Abilities in School-Age Children via Computerized Cognitive Training: Examining the Effect of Extended Training Duration. Brain Sci. 2023, 13, 1618. [Google Scholar] [CrossRef] [PubMed]
- Solis-Urra, P.; Sanchez-Martinez, J.; Olivares-Arancibia, J.; Castro Piñero, J.; Sadarangani, K.P.; Ferrari, G.; Rodríguez-Rodríguez, F.; Gaya, A.; Fochesatto, C.F.; Cristi-Montero, C. Physical Fitness and Its Association with Cognitive Performance in Chilean Schoolchildren: The Cogni-Action Project. Scand. J. Med. Sci. Sports 2021, 31, 1352–1362. [Google Scholar] [CrossRef] [PubMed]
- Stillman, C.M.; Esteban-Cornejo, I.; Brown, B.; Bender, C.M.; Erickson, K.I. Effects of Exercise on Brain and Cognition Across Age Groups and Health States. Trends Neurosci. 2020, 43, 533–543. [Google Scholar] [CrossRef]
- Mirwald, R.L.; Baxter-Jones, A.D.G.; Bailey, D.A.; Beunen, G.P. An Assessment of Maturity from Anthropometric Measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Stekhoven, D.J.; Bühlmann, P. MissForest—Non-Parametric Missing Value Imputation for Mixed-Type Data. Bioinformatics 2012, 28, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Revelle, W. Psych: Procedures for Psychological, Psychometric, and Personality Research; Northwestern University: Evanston, Il, USA, 2023. [Google Scholar]
- Sinha, P.; Calfee, C.S.; Delucchi, K.L. Practitioner’s Guide to Latent Class Analysis: Methodological Considerations and Common Pitfalls. Crit. Care Med. 2021, 49, e63–e79. [Google Scholar] [CrossRef] [PubMed]
- Seol, H. SnowRMM: Rasch Mixture, LCA, and Test Equating Analysis (Version 5.4.4). 2023. Available online: https://github.com/hyunsooseol/snowRMM (accessed on 13 December 2023).
- Lumley, T.; Diehr, P.; Emerson, S.; Chen, L. The Importance of the Normality Assumption in Large Public Health Data Sets. Annu. Rev. Public Health 2002, 23, 151–169. [Google Scholar] [CrossRef]
- Taut, S.; Cortés, F.; Sebastian, C.; Preiss, D. Evaluating School and Parent Reports of the National Student Achievement Testing System (SIMCE) in Chile: Access, Comprehension, and Use. Eval. Program Plann. 2009, 32, 129–137. [Google Scholar] [CrossRef] [PubMed]
- GAMLj: General Analyses for the Linear Model in Jamovi. Available online: https://gamlj.github.io (accessed on 13 December 2023).
- Granziera, F.; Guzzardi, M.A.; Iozzo, P. Associations between the Mediterranean Diet Pattern and Weight Status and Cognitive Development in Preschool Children. Nutrients 2021, 13, 3723. [Google Scholar] [CrossRef]
- Cohen, J.F.W.; Rifas-Shiman, S.L.; Young, J.; Oken, E. Associations of Prenatal and Child Sugar Intake with Child Cognition. Am. J. Prev. Med. 2018, 54, 727–735. [Google Scholar] [CrossRef]
- Cohen, J.F.W.; Gorski, M.T.; Gruber, S.A.; Kurdziel, L.B.F.; Rimm, E.B. The Effect of Healthy Dietary Consumption on Executive Cognitive Functioning in Children and Adolescents: A Systematic Review. Br. J. Nutr. 2016, 116, 989–1000. [Google Scholar] [CrossRef]
- Khan, N.A.; Raine, L.B.; Drollette, E.S.; Scudder, M.R.; Kramer, A.F.; Hillman, C.H. Dietary Fiber Is Positively Associated with Cognitive Control among Prepubertal Children. J. Nutr. 2015, 145, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Berr, C.; Portet, F.; Carriere, I.; Akbaraly, T.N.; Feart, C.; Gourlet, V.; Combe, N.; Barberger-Gateau, P.; Ritchie, K. Olive Oil and Cognition: Results from the Three-City Study. Dement. Geriatr. Cogn. Disord. 2009, 28, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, A.; Barul, C.; Féart, C.; Helmer, C.; Bernard, C.; Periot, O.; Dilharreguy, B.; Dartigues, J.-F.; Allard, M.; Barberger-Gateau, P.; et al. Mediterranean Diet and Preserved Brain Structural Connectivity in Older Subjects. Alzheimers Dement. J. Alzheimers Assoc. 2015, 11, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Mosconi, L.; Walters, M.; Sterling, J.; Quinn, C.; McHugh, P.; Andrews, R.E.; Matthews, D.C.; Ganzer, C.; Osorio, R.S.; Isaacson, R.S.; et al. Lifestyle and Vascular Risk Effects on MRI-Based Biomarkers of Alzheimer’s Disease: A Cross-Sectional Study of Middle-Aged Adults from the Broader New York City Area. BMJ Open 2018, 8, e019362. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F.; Mesas, A.E.; Álvarez-Bueno, C.; Pascual-Morena, C.; Saz-Lara, A.; Cavero-Redondo, I. Association between Eating Habits and Perceived School Performance: A Cross-Sectional Study Among 46,455 Adolescents From 42 Countries. Front. Nutr. 2022, 9, 797415. [Google Scholar] [CrossRef]
- Hayek, J.; Schneider, F.; Tueni, M.; de Vries, H. Is Academic Achievement Related to Mediterranean Diet, Substance Use and Social-Cognitive Factors: Findings from Lebanese Adolescents. Nutrients 2020, 12, 1535. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-Pincheira, C.; Espinoza, J.; Durán-Agüero, S.; Obregón, A.M.; Fuentealba, F. Dietary Fibre Intake in Chile: 13 Years after the Last National Report. Nutrients 2023, 15, 3671. [Google Scholar] [CrossRef]
- Lloyd, H.M.; Green, M.W.; Rogers, P.J. Mood and Cognitive Performance Effects of Isocaloric Lunches Differing in Fat and Carbohydrate Content. Physiol. Behav. 1994, 56, 51–57. [Google Scholar] [CrossRef]
- Ma, X.; Nan, F.; Liang, H.; Shu, P.; Fan, X.; Song, X.; Hou, Y.; Zhang, D. Excessive Intake of Sugar: An Accomplice of Inflammation. Front. Immunol. 2022, 13, 988481. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Ta, Q.T.H.; Nguyen, T.K.O.; Nguyen, T.T.D.; Giau, V.V. Type 3 Diabetes and Its Role Implications in Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 3165. [Google Scholar] [CrossRef]
- Jastreboff, A.M.; Sinha, R.; Arora, J.; Giannini, C.; Kubat, J.; Malik, S.; Van Name, M.A.; Santoro, N.; Savoye, M.; Duran, E.J.; et al. Altered Brain Response to Drinking Glucose and Fructose in Obese Adolescents. Diabetes 2016, 65, 1929–1939. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 1296) | WD (n = 56) | LFV-HSD (n = 365) | LFV-LSD (n = 547) | MED-DIET (n = 328) |
|---|---|---|---|---|---|
| Sex (boys/girls) | 648/648 | 34/22 | 166/199 | 283/264 | 165/163 |
| Age (years) | 11.9 ± 1.2 | 12.2 ± 1.1 | 12.3 ± 1.2 | 12.3 ± 1.1 | 12.6 ± 1.1 |
| Peak high velocity | −0.41 ± 1.3 | −0.79 ± 1.4 | −0.39 ± 1.2 | −0.51 ± 1.2 | −0.21 ± 1.3 |
| Weight | 50.9 ± 12.0 | 50.8 ± 14.9 | 50.7 ± 12.5 | 50.6 ± 11.0 | 51.6 ± 12.4 |
| Height | 153 ± 9.31 | 150 ± 10.2 | 153 ± 9.4 | 153 ± 9.1 | 154 ± 9.3 |
| BMIz | 1.02 ± 1.06 | 1.22 ± 1.1 | 0.99 ± 1.1 | 1.1 ± 1.1 | 0.96 ± 1.1 |
| School type | |||||
| Public | 456 (35.2%) | 37 (66.1%) | 161 (44.1%) | 145 (26.5%) | 113 (34.5%) |
| Subsidized | 514 (39.7%) | 15 (26.8%) | 140 (38.4%) | 249 (45.5%) | 110 (33.5%) |
| Private | 326 (25.2%) | 4 (7.1%) | 64 (17.5%) | 153 (28.0%) | 105 (32.0%) |
| Variables | All (n = 1296) | WD (n = 56) | LFV-HSD (n = 365) | LFV-LSD (n = 547) | MED-DIET (n = 328) |
|---|---|---|---|---|---|
| Second serving of fruit daily | |||||
| Adheres | 523 (40.4%) | 1 (1.8%) | 123 (33.7%) | 81 (14.8%) | 318 (96.9%) |
| Does not adhere | 773 (59.6%) | 55 (98.2%) | 242 (66.3%) | 466 (85.2%) | 10 (3.1%) |
| Fresh or cooked vegetables 1/day | |||||
| Adheres | 574 (44.3%) | 1 (1.8%) | 82 (22.5%) | 170 (31.1%) | 321 (97.9%) |
| Does not adhere | 722 (55.7%) | 55 (98.2%) | 283 (77.5%) | 377 (68.9%) | 7 (2.1%) |
| Regular fish consumption (at least 2–3/week) | |||||
| Adheres | 894 (69.0%) | 4 (7.1%) | 238 (65.2%) | 379 (69.3%) | 273 (83.2%) |
| Does not adhere | 402 (31.0%) | 52 (92.9%) | 127 (34.8%) | 168 (30.7%) | 55 (16.8%) |
| Once/week fast-food (hamburger) restaurant | |||||
| Adheres | 304 (23.5%) | 53 (94.7%) | 136 (37.3%) | 65 (11.9%) | 50 (15.2%) |
| Does not adhere | 992 (76.5%) | 3 (5.3%) | 229 (62.7%) | 482 (88.1%) | 278 (84.8%) |
| Pasta or rice almost daily (≥5/week) | |||||
| Adheres | 904 (69.8%) | 56 (100.0%) | 292 (80.0%) | 322 (58.9%) | 234 (71.3%) |
| Does not adhere | 392 (30.2%) | 0 (0.0%) | 73 (20.0%) | 225 (41.1%) | 94 (28.7%) |
| Regular nut consumption (at least 2–3/week) | |||||
| Adheres | 768 (59.3%) | 0 (0.0%) | 205 (56.1%) | 294 (53.7%) | 269 (82.0%) |
| Does not adhere | 528 (40.7%) | 56 (100.0%) | 160 (43.9%) | 253 (46.3%) | 59 (18.0%) |
| No breakfast | |||||
| Adheres | 300 (23.1%) | 42 (75.0%) | 115 (31.5%) | 55 (10.1%) | 88 (26.8%) |
| Does not adhere | 996 (76.9%) | 14 (25.0%) | 250 (68.5%) | 492 (89.9%) | 240 (73.2%) |
| Commercially baked goods or pastries for breakfast | |||||
| Adheres | 304 (23.5%) | 54 (96.4%) | 176 (48.2%) | 11 (2.0%) | 27 (8.2%) |
| Does not adhere | 992 (76.5%) | 2 (3.6%) | 189 (51.8%) | 536 (98.0%) | 301 (91.8%) |
| Sweets and candy several times a day | |||||
| Adheres | 358 (27.6%) | 50 (89.3%) | 245 (67.1%) | 0 (0.0%) | 63 (19.2%) |
| Does not adhere | 938 (72.4%) | 6 (10.7%) | 120 (32.9%) | 547 (100.0%) | 265 (80.8%) |
| Variables | All (n = 1296) | WD (n = 56) | LFV-HSD (n = 365) | LFV-LSD (n = 547) | MED-DIET (n = 328) |
|---|---|---|---|---|---|
| Cognitive tasks | |||||
| Cognitive Flexibility | |||||
| Trail-making test A (p) | 100.0 ± 14.7 | 91.4 ± 13.5 | 97.7 ± 14.5 | 101.1 ± 14.3 | 102.2 ± 14.9 |
| Trail-making test B (p) | 100.0 ± 14.7 | 93.3 ± 15.3 | 97.1 ± 14.1 | 101.5 ± 14.6 | 101.8 ± 14.7 |
| Digit coding symbol (p) | 100.0 ± 14.7 | 92.3 ± 13.4 | 97.2 ± 14.6 | 101.6 ± 14.5 | 101.8 ± 14.4 |
| Working Memory | |||||
| Memory forward (p) | 100.0 ± 14.4 | 92.0 ± 14.9 | 97.2 ± 13.6 | 101.4 ± 14.2 | 102.1 ± 14.4 |
| Memory reverse (p) | 100.0 ± 14.4 | 94.8 ± 14.6 | 96.7 ± 14.3 | 101.2 ± 13.9 | 102.4 ± 14.2 |
| Inhibitory Control | |||||
| Go/No-Go (p) | 100.0 ± 14.7 | 93.9 ± 15.4 | 98.4 ± 15.5 | 100.5 ± 14.6 | 101.9 ± 13.4 |
| Fluid Reasoning | |||||
| Problem-solving (p) | 100.0 ± 14.5 | 92.8 ± 13.4 | 97.4 ± 13.9 | 101.3 ± 14.3 | 102.1 ± 14.8 |
| Progressive matrices (p) | 100.0 ± 14.3 | 94.1 ± 11.4 | 97.6 ± 13.4 | 101.6 ± 14.6 | 101.3 ± 14.5 |
| Academic achievement | |||||
| English (s) | 5.62 ± 0.9 | 5.16 ± 0.9 | 5.52 ± 0.9 | 5.68 ± 0.8 | 5.72 ± 0.9 |
| History (s) | 5.45 ± 0.8 | 5.20 ± 0.6 | 5.31 ± 0.8 | 5.50 ± 0.8 | 5.56 ± 0.8 |
| Language (s) | 5.40 ± 0.8 | 5.09 ± 0.7 | 5.31 ± 0.8 | 5.45 ± 0.8 | 5.47 ± 0.8 |
| Mathematics (s) | 5.35 ± 1.0 | 5.09 ± 0.9 | 5.24 ± 1.0 | 5.42 ± 0.9 | 5.42 ± 1.0 |
| Science (s) | 5.45 ± 0.8 | 5.10 ± 0.8 | 5.39 ± 0.9 | 5.46 ± 0.8 | 5.54 ± 0.8 |
| Academic-PISA average | 5.40 ± 0.8 | 5.09 ± 0.7 | 5.31 ± 0.8 | 5.44 ± 0.7 | 5.47 ± 0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña-Jorquera, H.; Martínez-Flores, R.; Espinoza-Puelles, J.P.; López-Gil, J.F.; Ferrari, G.; Zapata-Lamana, R.; Lofrano-Prado, M.C.; Landaeta-Díaz, L.; Cigarroa, I.; Durán-Agüero, S.; et al. Adolescents with a Favorable Mediterranean-Style-Based Pattern Show Higher Cognitive and Academic Achievement: A Cluster Analysis—The Cogni-Action Project. Nutrients 2024, 16, 608. https://doi.org/10.3390/nu16050608
Peña-Jorquera H, Martínez-Flores R, Espinoza-Puelles JP, López-Gil JF, Ferrari G, Zapata-Lamana R, Lofrano-Prado MC, Landaeta-Díaz L, Cigarroa I, Durán-Agüero S, et al. Adolescents with a Favorable Mediterranean-Style-Based Pattern Show Higher Cognitive and Academic Achievement: A Cluster Analysis—The Cogni-Action Project. Nutrients. 2024; 16(5):608. https://doi.org/10.3390/nu16050608
Chicago/Turabian StylePeña-Jorquera, Humberto, Ricardo Martínez-Flores, Juan Pablo Espinoza-Puelles, José Francisco López-Gil, Gerson Ferrari, Rafael Zapata-Lamana, Mara Cristina Lofrano-Prado, Leslie Landaeta-Díaz, Igor Cigarroa, Samuel Durán-Agüero, and et al. 2024. "Adolescents with a Favorable Mediterranean-Style-Based Pattern Show Higher Cognitive and Academic Achievement: A Cluster Analysis—The Cogni-Action Project" Nutrients 16, no. 5: 608. https://doi.org/10.3390/nu16050608
APA StylePeña-Jorquera, H., Martínez-Flores, R., Espinoza-Puelles, J. P., López-Gil, J. F., Ferrari, G., Zapata-Lamana, R., Lofrano-Prado, M. C., Landaeta-Díaz, L., Cigarroa, I., Durán-Agüero, S., & Cristi-Montero, C. (2024). Adolescents with a Favorable Mediterranean-Style-Based Pattern Show Higher Cognitive and Academic Achievement: A Cluster Analysis—The Cogni-Action Project. Nutrients, 16(5), 608. https://doi.org/10.3390/nu16050608