
The Combined Effects of High-Intensity Interval Exercise Training and Dietary Supplementation on Reduction of Body Fat in Adults with Overweight and Obesity: A Systematic Review






Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Literature Search
2.4. Methodological Quality of the Included Studies (Risk of Bias)
3. Results
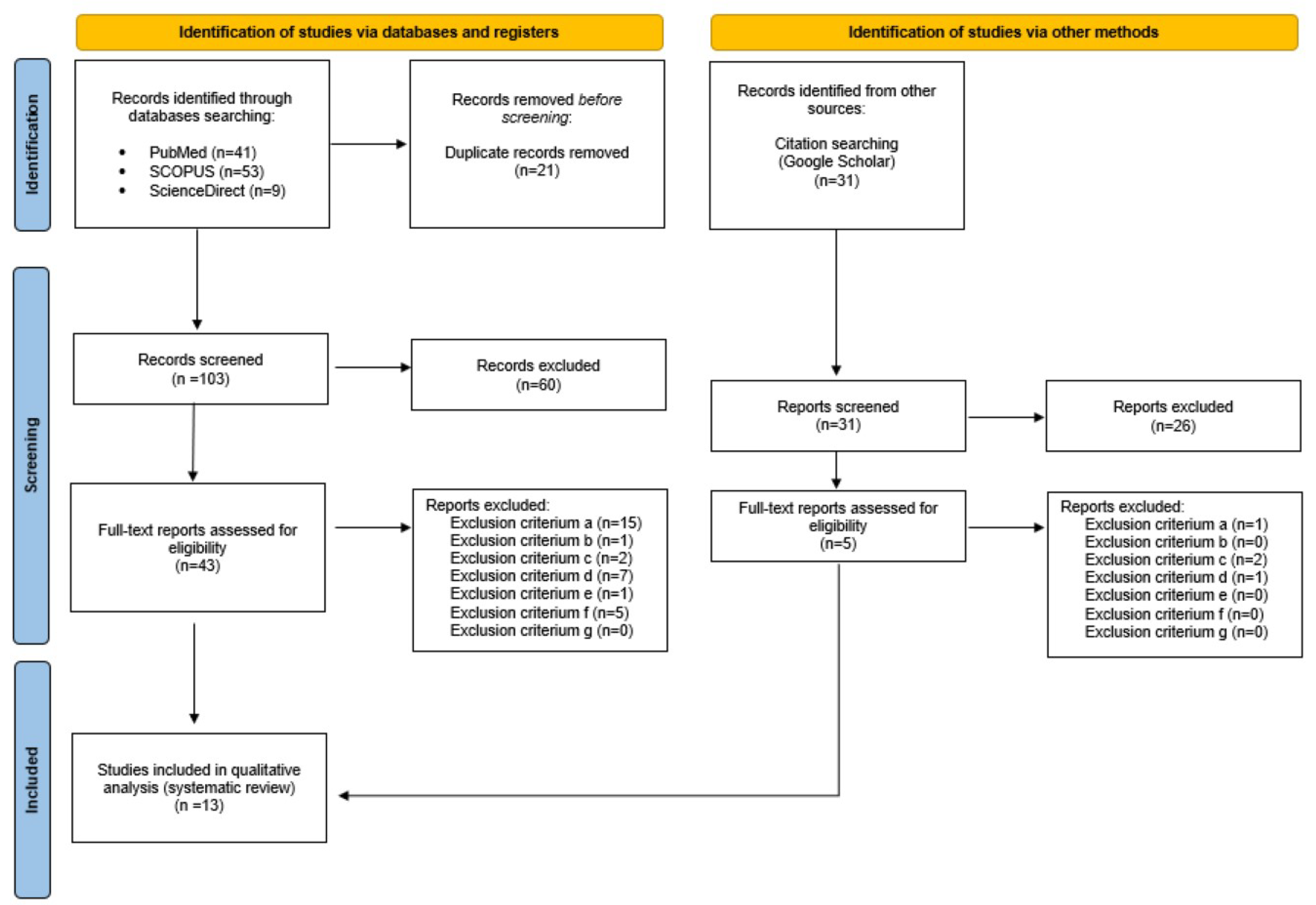
3.1. Study Selection
3.2. Study Characteristics
4. Discussion
4.1. Effects of HIIT Combined with Supplementation on BF
4.1.1. HIIT: The Most Popular Protocol
4.1.2. HIIT: Other Protocols
4.1.3. DS: Type and Dose Effect on BF
4.1.4. HIIT + DS: Sex-Based Differences in BF Responses
4.2. Effects of HIIT Combined with Supplementation on Metabolic Markers
4.2.1. Adipokines and Insulin
Adipokines
Insulin
4.2.2. Aerobic Capacity
5. Limitations and Strengths
6. Conclusions
- In general, HIIT combined with DS seems to induce the reduction of BF mass and improve metabolic health in adults with overweight and obesity; however, its effectiveness is related to several variables, including sex, type and dose of DS and HIIT protocol;
- The 40-m shuttle run test could be recommended as an effective form of HIIT for targeting overweight and obesity;
- It is difficult to point out the best type of DS for the reduction of BF in population with overweight and obesity; however, green tea seems to be effective.
- HIIT seems to be effective in reducing insulin resistance and does not seem to require being combined with DS;
- HIIT combined with DS green tea, ginger, astaxanthin or spinach-derived thylakoid may be more effective in improving aerobic capacity of adults with overweight and obesity than HIIT alone;
- Although combining HIIT with dietary supplementation seems to improve body composition, metabolic health and aerobic capacity in adults with overweight and obesity to a greater extent than HIIT alone, but it does not seem to be necessary to combine these two interventions.
7. Practical Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, 1–253. [Google Scholar]
- World Health Organization. WHO European Regional Obesity Report 2022; WHO Regional Office for Europe: Copenhagen, Denmark, 2022; Available online: https://iris.who.int/bitstream/handle/10665/353747/9789289057738-eng.pdf (accessed on 14 December 2023).
- World Health Organization. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 6 January 2024).
- Boutari, C.; Mantzoros, C.S. A 2022 update on the epidemiology of obesity and a call to action: As its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism 2022, 133, 155217. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef]
- Leitner, D.R.; Frühbeck, G.; Yumuk, V.; Schindler, K.; Micic, D.; Woodward, E.; Toplak, H. Obesity and Type 2 Diabetes: Two Diseases with a Need for Combined Treatment Strategies—EASO Can Lead the Way. Obes. Facts 2017, 10, 483–492. [Google Scholar] [CrossRef]
- Alford, S.; Patel, D.; Perakakis, N.; Mantzoros, C.S. Obesity as a Risk Factor for Alzheimer’s Disease: Weighing the Evidence. Obes. Rev. 2018, 19, 269–280. [Google Scholar] [CrossRef]
- Jung, U.J.; Choi, M.-S. Obesity and Its Metabolic Complications: The Role of Adipokines and the Relationship between Obesity, Inflammation, Insulin Resistance, Dyslipidemia and Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2014, 15, 6184–6223. [Google Scholar] [CrossRef]
- Zhang, X.; Ha, S.; Lau, H.C.-H.; Yu, J. Excess Body Weight: Novel Insights into Its Roles in Obesity Comorbidities. Semin. Cancer Biol. 2023, 92, 16–27. [Google Scholar] [CrossRef]
- Cani, P.D.; Van Hul, M.; Lefort, C.; Depommier, C.; Rastelli, M.; Everard, A. Microbial Regulation of Organismal Energy Homeostasis. Nat. Metab. 2019, 1, 34–46. [Google Scholar] [CrossRef]
- Lumeng, C.N.; Bodzin, J.L.; Saltiel, A.R. Obesity Induces a Phenotypic Switch in Adipose Tissue Macrophage Polarization. J. Clin. Investig. 2007, 117, 175–184. [Google Scholar] [CrossRef]
- Hall, K.D.; Farooqi, I.S.; Friedman, J.M.; Klein, S.; Loos, R.J.F.; Mangelsdorf, D.J.; O’Rahilly, S.; Ravussin, E.; Redman, L.M.; Ryan, D.H.; et al. The Energy Balance Model of Obesity: Beyond Calories in, Calories Out. Am. J. Clin. Nutr. 2022, 115, 1243–1254. [Google Scholar] [CrossRef]
- Ludwig, D.S.; Ebbeling, C.B. The Carbohydrate-Insulin Model of Obesity: Beyond ‘Calories In, Calories Out’. JAMA Intern. Med. 2018, 178, 1098–1103. [Google Scholar] [CrossRef]
- Wali, J.A.; Ni, D.; Facey, H.J.W.; Dodgson, T.; Pulpitel, T.J.; Senior, A.M.; Raubenheimer, D.; Macia, L.; Simpson, S.J. Determining the Metabolic Effects of Dietary Fat, Sugars and Fat-Sugar Interaction Using Nutritional Geometry in a Dietary Challenge Study with Male Mice. Nat. Commun. 2023, 14, 4409. [Google Scholar] [CrossRef]
- Hall, K.D.; Kahan, S. Maintenance of Lost Weight and Long-Term Management of Obesity. Med. Clin. N. Am. 2018, 102, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Mann, T.; Tomiyama, A.J.; Westling, E.; Lew, A.M.; Samuels, B.; Chatman, J. Medicare’s search for effective obesity treatments: Diets are not the answer. Am. Psychol. 2007, 62, 220–233. [Google Scholar] [CrossRef]
- National Institutes of Health, Office of Dietary Supplements. Background Information: Dietary Supplements; National Institutes of Health, Office of Dietary Supplements: Bethesda, MD, USA, 2011. Available online: https://ods.od.nih.gov/factsheets/DietarySupplements-HealthProfessional/ (accessed on 7 January 2024).
- Batsis, J.A.; Apolzan, J.W.; Bagley, P.J.; Blunt, H.B.; Divan, V.; Gill, S.; Golden, A.; Gundumraj, S.; Heymsfield, S.B.; Kahan, S.; et al. A Systematic Review of Dietary Supplements and Alternative Therapies for Weight Loss. Obesity 2021, 29, 1102–1113. [Google Scholar] [CrossRef]
- Koh, Y.S.; Asharani, P.V.; Devi, F.; Roystonn, K.; Wang, P.; Vaingankar, J.A.; Abdin, E.; Sum, C.F.; Lee, E.S.; Müller-Riemenschneider, F.; et al. A Cross-Sectional Study on the Perceived Barriers to Physical Activity and Their Associations with Domain-Specific Physical Activity and Sedentary Behaviour. BMC Public Health 2022, 22, 1051. [Google Scholar] [CrossRef]
- MacInnis, M.J.; Gibala, M.J. Physiological Adaptations to Interval Training and the Role of Exercise Intensity. J. Physiol. 2017, 595, 2915–2930. [Google Scholar] [CrossRef]
- DiPietro, L.; Dziura, J.; Yeckel, C.W.; Neufer, P.D. Exercise and Improved Insulin Sensitivity in Older Women: Evidence of the Enduring Benefits of Higher Intensity Training. J. Appl. Physiol. 2006, 100, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Whyte, L.J.; Gill, J.M.R.; Cathcart, A.J. Effect of 2 Weeks of Sprint Interval Training on Health-Related Outcomes in Sedentary Overweight/Obese Men. Metabolism 2010, 59, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Amundsen, B.H.; Rognmo, Ø.; Hatlen-Rebhan, G.; Slørdahl, S.A. High-Intensity Aerobic Exercise Improves Diastolic Function in Coronary Artery Disease. Scand. Cardiovasc. J. 2008, 42, 110–117. [Google Scholar] [CrossRef]
- Hall, B.; Żebrowska, A.; Sikora, M.; Siatkowski, S.; Robins, A. The Effect of High-Intensity Interval Exercise on Short-Term Glycaemic Control, Serum Level of Key Mediator in Hypoxia and Pro-Inflammatory Cytokines in Patients with Type 1 Diabetes-An Exploratory Case Study. Nutrients 2023, 15, 3749. [Google Scholar] [CrossRef] [PubMed]
- Bacon, A.P.; Carter, R.E.; Ogle, E.A.; Joyner, M.J. VO2max Trainability and High Intensity Interval Training in Humans: A Meta-Analysis. PLoS ONE 2013, 8, e73182. [Google Scholar] [CrossRef] [PubMed]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.; van den Berg, R.; Ward, R.E.; Keech, A. The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Body Composition in Overweight and Obese Adults: A Systematic Review and Meta-Analysis. Obes. Rev. 2017, 18, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, B.J.; Tucker, W.J.; Bhammar, D.M.; Ryder, J.R.; Sweazea, K.L.; Gaesser, G.A. Effects of High-Intensity Interval Training and Moderate-Intensity Continuous Training on Endothelial Function and Cardiometabolic Risk Markers in Obese Adults. J. Appl. Physiol. 2016, 121, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Colpitts, B.H.; Rioux, B.V.; Eadie, A.L.; Brunt, K.R.; Sénéchal, M. Irisin response to acute moderate intensity exercise and high intensity interval training in youth of different obesity statuses: A randomized crossover trial. Physiol. Rep. 2022, 10, e15198. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological Quality (Risk of Bias) Assessment Tools for Primary and Secondary Medical Studies: What Are They and Which Is Better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Dunn, S.L.; Siu, W.; Freund, J.; Boutcher, S.H. The Effect of a Lifestyle Intervention on Metabolic Health in Young Women. Diabetes Metab. Syndr. Obes. 2014, 7, 437–444. [Google Scholar] [CrossRef]
- Nayebifar, S.; Afzalpour, M.E.; Kazemi, T.; Eivary, S.H.A.; Mogharnasi, M. The Effect of a 10-Week High-Intensity Interval Training and Ginger Consumption on Inflammatory Indices Contributing to Atherosclerosis in Overweight Women. J. Res. Med. Sci. 2016, 21, 116. [Google Scholar] [CrossRef]
- Afzalpour, M.E.; Ghasemi, E.; Zarban, A. Effects of 10 Weeks of High Intensity Interval Training and Green Tea Supplementation on Serum Levels of Sirtuin-1 and Peroxisome Proliferator-Activated Receptor Gamma Co-Activator 1-Alpha in Overweight Women. Sci. Sports 2017, 32, 82–90. [Google Scholar] [CrossRef]
- Lithgow, H.M.; Florida-James, G.; Leggate, M. The Combined Effect of High-intensity Intermittent Training and Vitamin D Supplementation on Glycemic Control in Overweight and Obese Adults. Physiol. Rep. 2018, 6, e13684. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, E.; Nayebifar, S. Benefits of 10 Weeks of High-Intensity Interval Training and Green Tea Supplementation on Cardiovascular Risk Factors and VO2max in Overweight Women. J. Res. Med. Sci. 2019, 24, 79. [Google Scholar] [CrossRef] [PubMed]
- Saghebjoo, M.; Farrokhi-Fard, M.; Hedayati, M.; Sadeghi-Tabas, S. The Effect of High-Intensity Interval Training and L-Arginine Supplementation on the Serum Levels of Adiponectin and Lipid Profile in Overweight and Obese Young Men. Obes. Med. 2019, 16, 100139. [Google Scholar] [CrossRef]
- Ghasemi, E.; Afzalpour, M.E.; Nayebifar, S. Combined High-Intensity Interval Training and Green Tea Supplementation Enhance Metabolic and Antioxidant Status in Response to Acute Exercise in Overweight Women. J. Physiol. Sci. 2020, 70, 31. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, K.R.; Greenwalt, C.E.; Saylor, H.E.; Gould, L.M.; Harrison, C.H.; Brewer, G.J.; Blue, M.N.M.; Ferrando, A.A.; Huffman, K.M.; Mayer-Davis, E.J.; et al. High-Intensity Interval Training and Essential Amino Acid Supplementation: Effects on Muscle Characteristics and Whole-Body Protein Turnover. Physiol. Rep. 2021, 9, e14655. [Google Scholar] [CrossRef] [PubMed]
- Nobari, H.; Gandomani, E.E.; Reisi, J.; Vahabidelshad, R.; Suzuki, K.; Volpe, S.L.; Pérez-Gómez, J. Effects of 8 Weeks of High-Intensity Interval Training and Spirulina Supplementation on Immunoglobin Levels, Cardio-Respiratory Fitness, and Body Composition of Overweight and Obese Women. Biology 2022, 11, 196. [Google Scholar] [CrossRef]
- Sheikholeslami-Vatani, D.; Rostamzadeh, N. Changes in Appetite-Dependent Hormones and Body Composition After 8 Weeks of High-Intensity Interval Training and Vitamin D Supplementation in Sedentary Overweight Men. Front. Nutr. 2022, 9, 827630. [Google Scholar] [CrossRef]
- Saeidi, A.; Nouri-Habashi, A.; Razi, O.; Ataeinosrat, A.; Rahmani, H.; Mollabashi, S.S.; Bagherzadeh-Rahmani, B.; Aghdam, S.M.; Khalajzadeh, L.; Al Kiyumi, M.H.; et al. Astaxanthin Supplemented with High-Intensity Functional Training Decreases Adipokines Levels and Cardiovascular Risk Factors in Men with Obesity. Nutrients 2023, 15, 286. [Google Scholar] [CrossRef]
- Saeidi, A.; Saei, M.A.; Mohammadi, B.; Zarei, H.R.A.; Vafaei, M.; Mohammadi, A.S.; Barati, M.; Montazer, M.; Razi, O.; Kiyumi, M.H.A.; et al. Supplementation with Spinach-Derived Thylakoid Augments the Benefits of High Intensity Training on Adipokines, Insulin Resistance and Lipid Profiles in Males with Obesity. Front. Endocrinol. 2023, 14, 1141796. [Google Scholar] [CrossRef]
- Youssef, L.; Durand, S.; Aprahamian, F.; Lefevre, D.; Bourgin, M.; Maiuri, M.C.; Dulac, M.; Hajj-Boutros, G.; Marcangeli, V.; Buckinx, F.; et al. Serum metabolomic adaptations following a 12-week high-intensity interval training combined to citrulline supplementation in obese older adults. Eur. J. Sport Sci. 2023, 23, 2157–2169. [Google Scholar] [CrossRef] [PubMed]
- Haizlip, K.M.; Harrison, B.C.; Leinwand, L.A. Sex-Based Differences in Skeletal Muscle Kinetics and Fiber-Type Composition. Physiology 2015, 30, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Fasshauer, M.; Blüher, M. Adipokines in Health and Disease. Trends Pharmacol. Sci. 2015, 36, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Sierawska, O.; Niedźwiedzka-Rystwej, P. Adipokines as Potential Biomarkers for Type 2 Diabetes Mellitus in Cats. Front. Immunol. 2022, 13, 950049. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Redondo-Flórez, L.; Beltrán-Velasco, A.I.; Martín-Rodríguez, A.; Martínez-Guardado, I.; Navarro-Jiménez, E.; Laborde-Cárdenas, C.C.; Tornero-Aguilera, J.F. The Role of Adipokines in Health and Disease. Biomedicines 2023, 11, 1290. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Hassan-Zadeh, V. IL-6 Signalling Pathways and the Development of Type 2 Diabetes. Inflammopharmacology 2018, 26, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Pessin, J.E.; Saltiel, A.R. Signaling Pathways in Insulin Action: Molecular Targets of Insulin Resistance. J. Clin. Investig. 2000, 106, 165–169. [Google Scholar] [CrossRef]
- Kwon, H.; Pessin, J.E. Adipokines Mediate Inflammation and Insulin Resistance. Front. Endocrinol. 2013, 4, 71. [Google Scholar] [CrossRef]
- Reaven, G.M. Compensatory Hyperinsulinemia and the Development of an Atherogenic Lipoprotein Profile: The Price Paid to Maintain Glucose Homeostasis in Insulin-Resistant Individuals. Endocrinol. Metab. Clin. N. Am. 2005, 34, 49–62. [Google Scholar] [CrossRef]
- Henry, S.L.; Bensley, J.G.; Wood-Bradley, R.J.; Cullen-McEwen, L.A.; Bertram, J.F.; Armitage, J.A. White Adipocytes: More than Just Fat Depots. Int. J. Biochem. Cell Biol. 2012, 44, 435–440. [Google Scholar] [CrossRef]
- Grases-Pintó, B.; Abril-Gil, M.; Castell, M.; Rodríguez-Lagunas, M.J.; Burleigh, S.; Fåk Hållenius, F.; Prykhodko, O.; Pérez-Cano, F.J.; Franch, À. Influence of Leptin and Adiponectin Supplementation on Intraepithelial Lymphocyte and Microbiota Composition in Suckling Rats. Front. Immunol. 2019, 10, 2369. [Google Scholar] [CrossRef]
- Friedman, J.M. Leptin and the Endocrine Control of Energy Balance. Nat. Metab. 2019, 1, 754–764. [Google Scholar] [CrossRef]
- Feito, Y.; Burrows, E.K.; Tabb, L.P. A 4-Year Analysis of the Incidence of Injuries Among CrossFit-Trained Participants. Orthop. J. Sports Med. 2018, 6, 2325967118803100. [Google Scholar] [CrossRef]
- McPherron, A.C.; Lawler, A.M.; Lee, S.J. Regulation of Skeletal Muscle Mass in Mice by a New TGF-Beta Superfamily Member. Nature 1997, 387, 83–90. [Google Scholar] [CrossRef]
- Schuelke, M.; Wagner, K.R.; Stolz, L.E.; Hubner, C.; Riebel, T.; Komen, W.; Braun, T.; Tobin, J.F.; Lee, S.J. Myostatin mutation associated with gross muscle hypertrophy in a child. N. Engl. J. Med. 2004, 350, 2682–2688. [Google Scholar] [CrossRef] [PubMed]
- Seldin, M.M.; Tan, S.Y.; Wong, G.W. Metabolic Function of the CTRP Family of Hormones. Rev. Endocr. Metab. Disord. 2014, 15, 111–123. [Google Scholar] [CrossRef]
- Guo, T.; Jou, W.; Chanturiya, T.; Portas, J.; Gavrilova, O.; McPherron, A.C. Myostatin Inhibition in Muscle, but Not Adipose Tissue, Decreases Fat Mass and Improves Insulin Sensitivity. PLoS ONE 2009, 4, e4937. [Google Scholar] [CrossRef]
- Pietiläinen, K.H.; Kaprio, J.; Borg, P.; Plasqui, G.; Yki-Järvinen, H.; Kujala, U.M.; Rose, R.J.; Westerterp, K.R.; Rissanen, A. Physical Inactivity and Obesity: A Vicious Circle. Obesity 2008, 16, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Setty, P.; Padmanabha, B.; Doddamani, B. Correlation between Obesity and Cardio Respiratory Fitness. Int. J. Med. Sci. Public Health 2013, 2, 298–302. [Google Scholar] [CrossRef]
- Cantó, C.; Auwerx, J. PGC-1alpha, SIRT1 and AMPK, an energy sensing network that controls energy expenditure. Curr. Opin. Lipidol. 2009, 20, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Rech, C.C.; de Camargo, E.M.; de Paula Almeida, M.; dos Santos Bronoski, R.; Okuno, N.M.; Reis, R.S. Barriers for physical activity in overweight adults. Rev. Bras. Atividade Fís. Saúde 2016, 21, 272–279. [Google Scholar] [CrossRef]
- Ambati, R.R.; Siew Moi, P.; Ravi, S.; Aswathanarayana, R.G. Astaxanthin: Sources, Extraction, Stability, Biological Activities and Its Commercial Applications—A Review. Mar. Drugs 2014, 12, 128–152. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, M.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Author | Risk of Bias Judgement | |||||
|---|---|---|---|---|---|---|
| Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | Overall Risk of Bias | |
| Dunn et al. [32] | LOW | LOW | LOW | LOW | LOW | LOW |
| Nayebifar et al. [33] | LOW | SOME CONCERNS | LOW | LOW | LOW | SOME CONCERNS |
| Lithgow et al. [34] | LOW | LOW | LOW | LOW | LOW | LOW |
| Afzalpour et al. [35] | LOW | SOME CONCERNS | LOW | LOW | LOW | SOME CONCERNS |
| Ghasemi et al. [36] | SOME CONCERNS | SOME CONCERNS | LOW | LOW | LOW | SOME CONCERNS |
| Saghebjoo et al. [37] | LOW | LOW | LOW | LOW | LOW | LOW |
| Ghasemi et al. [38] | LOW | LOW | LOW | LOW | LOW | LOW |
| Hirsch et al. [39] | LOW | LOW | LOW | LOW | LOW | LOW |
| Nobari et al. [40] | LOW | SOME CONCERNS | LOW | LOW | LOW | SOME CONCERNS |
| Sheikholeslami-Vatani et al. [41] | LOW | LOW | LOW | LOW | LOW | LOW |
| Saeidi et al. [42] | LOW | SOME CONCERNS | LOW | LOW | LOW | SOME CONCERNS |
| Saeidi et al. [43] | LOW | LOW | LOW | LOW | LOW | LOW |
| Youssef et al. [44] | LOW | LOW | LOW | LOW | LOW | LOW |
| Author | Participants Characteristics | HIIT | Supplement | Protocol of the Intervention (HIIT + Supplement) | Intervention: Main Findings |
|---|---|---|---|---|---|
| Herbs and botanicals | |||||
| Nayebifar et al. [33] | nF = 24/age = 20–30 years SG1 (HIIT + ginger); nF = 8/age = 21.88 ± 3.4 years; BM = 74.19 ± 11.53 kg; BMI = 28.68 ± 2.60 kg/m2 SG2 (HIIT + placebo); nF = 8/age = 22.38 ± 3.24 years; BM = 72.24 ± 6.86 kg; BMI = 28.42 ± 2.4 kg/m2 SG3 (ginger); nF = 8/age = 21.63 ± 1.77 years; BM = 64.91 ± 3.6 kg; BMI = 26.06 ± 1.69 kg/m2 | A 40 m shuttle run: three times per week, 20 m of max speed/20 m recovery, repeated 10 times. | Ginger (3000 mg) or placebo (Nokhodchi flour) 30 min before each meal. | A 10-week programme of HIIT combined with 3000 mg of ginger or Nokhodchi flour supplementation in females with overweight. | HIIT+ ginger: ↓ body fat (%) ∆ ↑ VO2max (mL/kg/min). HIIT: ↑ VO2max (mL/kg/min). |
| Afzalpour et al. [34] | nP = 24 females SG1 (HIIT + ginger); nF = 8/age = 21.87 ± 3.39 years; BM = 74.19 ± 11.53 kg; BMI = 28.68 ± 2.60 kg/m2 SG2 (HIIT + placebo); nF = 8/age = 22.37 ± 3.24 years; BM = 72.24 ± 6.86 kg; BMI = 28.42 ± 2.40 kg/m2 SG3 (ginger); nF = 8/age = 21.62 ± 1.76 years; BM = 64.91 ± 3.6 kg; BMI = 26.06 ± 1.6 kg/m2 | A 30 s sprint (intensity over 90% HRmax) followed by 30 s active rest, and repeated three times per training session, three times/week. Each two weeks, one repetition was added. | Ginger (3 g per one tablet) or placebo (flour) once a day. | A 10-week programme of HIIT combined with ginger or placebo supplementation in females with overweight and obesity. | HIIT + ginger ∆: ↓ body fat (%), ↑ VO2max (mL/kg/min). |
| Ghasemi et al. [36] | nP = 30 females/age = 20–30 years; BMI ≥ 25 kg/m2 SG1 (green tea); nF = 10 SG2 (HIIT + green tea); nF = 10 SG3 (HIIT + placebo); nF = 10 | A 40-m maximal shuttle run (30 s) at an intensity of 85–95% of maximum heart rate interspersed with 30 s of active relaxation time, three times a week for 10 weeks. | Green tea (500 mg) or placebo (500 mg starch powder) three times/day. | A 10-week programme of HIIT combined with 500 mg green tea extract or placebo supplementation in females with overweight. | HIIT + green tea ∆: ↓ body fat (%). |
| Ghasemi et al. [38] | nP = 30 females/age = 20–30; BMI > 25 kg/m2 SG1 (HIIT + green tea); nF = 10/age = 22.47 ± 3.32 years, BM = 70.56 ± 6.19 kg; BMI = 27.15 ± 1.47 kg/m2 SG2 (HIIT + placebo); nF = 10/age = 23.58 ± 2.23; BM = 72.18 ± 3.51 kg; BMI = 27.32 ± 1.27 kg/m2 SG3 (green tea); nF = 10/age = 21.06 ± 2.65; BM = 73.45 ± 8.44 kg; BMI = 28.03 ± 1.04 kg/m2 | A 40-m shuttle run at 90% Hrmax (30 s) three times/week. | Green tea (1500 mg) or placebo (starch powder) tablets three times/day, 2 h after the main meals, 7 days/week. For 10 weeks. | A 10-week programme of HIIT combined with green tea (500 mg) supplementation in young, sedentary females with overweight. | HIIT + green tea ∆: ↓ body fat (%), ↓ body mass (kg), ↑ PGC-1α (pg/mL), ↑ VO2max (ml/kg/min). |
| Nobari et al. [40] | nP = 30 females/age = 25.1 ± 6.7 years; BM = 75.8 ± 8.4 kg SG1 (spirulina); nF = 10 SG2 (HIIT + spirulina); nF = 10 SG3 (HIIT + placebo); nF = 10 | An exercise of 30 s running at an intensity of 90% Hrmax, interspersed with 30 s walking, repeated 4–7 times in each session, 3 times a week. | Spirulina powder (6 g) or placebo (green colouring food dissolved in water) one tablet per day. | An 8-week programme of HIIT and spirulina powder (6 g/day) or placebo supplementation in females with overweight and obesity. | HIIT + spirulina: ↓ body mass (kg) |
| Saeidi et al. [42] | nP = 68/age = 27.6 ± 8.4 years; BM = 94.7 ± 2.0 kg; BMI = 33.6 ± 1.4 kg/m2 SG1 (astaxanthin); nP = 15 SG2 (HIIT); nP = 15 SG3 (HIIT + astaxanthin); nP = 15 CG; nP = 15 | Crossfit sessions of 60 min consisting of 60 min/CrossFit® sessions consisting of squats, deadlift, press, jerks, barbell, dumbbell, and medicine ball cleans, pull-ups, kettlebell swings and other, three times a week. | Astaxanthin (20 mg) or placebo (20 mg raw corn starch) one tablet a day with breakfast. | A 12-week programme of 36 high-intensity-functional training Crossfit sessions lasting up to 60 combined with astaxanthin (20 mg/day) or raw corn starch supplementation in males with obesity. | HIIT + astaxanthin ∆: ↓ body fat (%), ↓ body mass (kg), ↓ BMI (kg/m2), ↓ fasting glucose (mg/dL), ↓ fasting insulin (ng/mL), ↓ myostatin, GDF-15, CTRP2 and CTRP9 (ng/mL), ↑ VO2peak (mL/kg/min). |
| Saeidi et al. [43] | nP = 68/age = 27.6 ± 8.4 years; BM = 95.7 ± 3.8 kg; BMI = 32.6 ± 2.6 kg/m2 SG1 (spinach-derived thylakoid); nP = 15 SG2 (HIIT); nP = 15 SG3 (HIIT + spinach-derived thylakoid); nP = 15 CG; nP = 15 | Crossfit sessions of 60 min consisting of 60 min/CrossFit® sessions consisting of squats, deadlift, press, jerks, barbell, dumbbell, and medicine ball cleans, pull-ups, kettlebell swings and other. | Spinach-derived thylakoid (5 g) or placebo (5 g of raw corn starch). | A 12-week programme of 36 high-intensity-functional training Crossfit sessions lasting up to 60 min combined with thylakoid-rich spinach extract or matching placebo supplementation. | HIIT + spinach-derived thylakoid ∆: ↓ body fat (%), ↓ HOMA IR, ↓ myostatin, GDF-15, CTRP2 and CTRP9 (ng/mL), ↑ fat free mass (kg), ↑ VO2peak (mL/kg/min). |
| Vitamins | |||||
| Lithgow et al. [35] | nP = 20, males and females SG1 (HIIT + vitamin D; nP = 10; nM = 8; nF = 2/age = 34 ± 9 years; BM = 96.2 ± 12.2 kg; BMI = 30.5 ± 2.2 kg/m2 SG2 (HIIT + placebo); nP = 10; nM = 6; nF = 4/age = 34 ± 10 years; BM = 97.0 ± 15.6 kg; BMI = 32.3 ± 3.1 kg/m2 | A cycle ergometer: 10 repetitions of 1 min intervals interspersed with 1 min active recovery at a power output of 50, three times a week for 6 weeks. The power output (W) of the high-intensity intervals was assigned as a workload corresponding to 100% VO2peak (sessions 1–6) to 110% VO2peak (sessions 7–12), and ultimately 120% (sessions 13–18) | Vitamin D3 (100 μg per tablet) or placebo one tablet/day with breakfast. | A 6-week programme of HIIT combined with vitamin D or placebo supplementation in males and females with overweight and obesity. | HIIT alone: ↓ waist and hip circumference (cm) HIIT + vitamin D3: ↓ fasting insulin (mU/L) ↓ fasting glucose (mmol/L) |
| Sheikholeslami-Vatani et al. [41] | nP = 48 males/age = 21.7 ± 1.4 years; BM = 86.52 ± 3.92 kg; BMI = 27.28 ± 0.76 kg/m2 SG1 (HIIT + Vitamin D3); nM = 12 SG2 (HIIT + placebo); nM = 12 SG3 (Vitamin D3); nM = 12 CG; nM = 12 | An amount of 10 × 1 min intervals cycling at 90% VO2peak separated by 1 min active recovery at 15% VO2peak from week 1 to week 4, then 10 × 1 min intervals cycling at 100% VO2peak separated by 1 min active recovery at 15% VO2peak from week 5 to week 8; 3 sessions per week. | Vitamin D3 (2000 IU) or placebo (maltodextrin) one tablet a day. | An 8-week programme of HIIT combined with vitamin D3 (2000 IU/day) or maltodextrin supplementation in males with overweight. | HIIT alone and HIIT + vitamin D3, ↓ body fat (%), ↓ BMI (kg/m2), ↓ body mass (kg), ↓ insulin (ng/dl). |
| Amino acids | |||||
| Saghebjoo et al. [37] | nP = 40 males/age = 23.9 ± 1.4; BMI = 29.6 ± 4.0 kg/m2 SG1 (HIIT + placebo); nM = 10 SG2 (L-arginine); nM = 10 SG3 (HIIT + L-arginine); nM10 SG4 (placebo); nM = 10 | A 30-s sprint interspersed with 30 s of walking, repeated 4–6 times in the first and second week, to 5 times in the third and fourth week then 6 times in the fifth and sixth week. | L-arginine (6 g/day): three capsules per day with 400 mL of water at half an hour before breakfast, 1 h before lunch, and 1 h before the last daily meal. | A 6-week programme of HIIT combined with L-arginine (6 g/day) supplementation in males with overweight and obesity. | No significant changes in %FAT, BMI, adiponectin in response to HIIT, L-arginine or HIIT + L-arginine. |
| Hirsch et al. [39] | nP = 76 males and females SG1 (HIIT); nP = 19; nM = 9; nF = 10/age = 36.74 ± 5.61; BM = 96.57 ± 17.23 kg; BMI = 31.73 ± 4.72 kg/m2 SG2 (EAA); nP = 20; nM = 10; nF = 10/age = 35.60 ± 4.95; BM = 96.66 ± 16.33 kg; BMI = 31.22 ± 4.29 kg/m2 SG3 (HIIT + EAA); nP = 19; nM = 9; nF = 10/age = 36.21 ± 6.65; BM = 91.78 ± 13.54 kg; BMI = 31.41 ± 3.36 kg/m2CG; nP = 8; nM = 4; nF = 4/age = 36.88 ± 7.45; BM = 92.20 ± 15.52 kg; BMI = 30.55 ± 3.91 kg/m2 | On a cycle ergometer: 1-min at 90% max wattage interspersed with 1-min complete rest. HIIT started with six sets of intervals and progressed by one set each week until reaching ten sets at week five; ten sets were maintained for the remainder of the 8 weeks; HIIT sets were performed 2 days/week. | Essential amino acid (EAA) (3.6 g) twice a day. | An 8-week programme of HIIT combined with EAA (3.6 g/2× day) supplementation in adults with overweight and obesity. | HIIT alone and HIIT+ EAA: ↑ thigh lean mass size (kg) |
| Youssef et al. [44] | nP = 83; BM = 81.4 ± 14.0 kg; BMI 30–40 kg/m2 SG1 (HIIT +citrulline); nP = 39 SG2 (HIIT + placebo); nP = 44 | HIIT, three times/per week; 30 min/session. | Citrulline (10 g) or placebo daily. | A 12-week HIIT combined with citrulline or placebo supplementation in adults with obesity. | HIIT + citrulline: ↓ total body fat (kg and %), ↓ android and trunk fat mass (kg), ↓ leptin (ng/mL). |
| Fatty acids | |||||
| Dunn et al. [32] | SG; nF = 15/age = 24 ± 1.0 years; BM = 73.3 ± 3.1 kg; BMI = 27.6 ± 0.8 kg/m2 CG; nF = 15/age = 22 ± 0.6 years; BM = 70.9 ± 2.9 kg; BMI = 25.7 ± 0.5 kg/m2 | A manual cycle ergometer, three times a week, 20 min of exercise: 8-s sprint, 12-s recovery. | ω-3 fatty acids (550 mg of eicosapentaenoic acid and docosahexaenoic acid per 1100 mg capsule) three capsules/day. | A 12-week programme of HIIT combined with low glycaemic Mediterranean diet (Mediet) and ω-3 supplementation in females with overweight. | HIIT+ ω-3 + Mediet: ↓ total fat mass (kg), ↓ abdominal adiposity (kg), ↓ waist circumference (cm), ↓ systolic blood pressure (mmHg), ↓ fasting plasma insulin (μIU/mL), ↓ IL-6 (pg/mL), ↖ VO2peak (ml/kg/min). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaweł, E.; Hall, B.; Siatkowski, S.; Grabowska, A.; Zwierzchowska, A. The Combined Effects of High-Intensity Interval Exercise Training and Dietary Supplementation on Reduction of Body Fat in Adults with Overweight and Obesity: A Systematic Review. Nutrients 2024, 16, 355. https://doi.org/10.3390/nu16030355
Gaweł E, Hall B, Siatkowski S, Grabowska A, Zwierzchowska A. The Combined Effects of High-Intensity Interval Exercise Training and Dietary Supplementation on Reduction of Body Fat in Adults with Overweight and Obesity: A Systematic Review. Nutrients. 2024; 16(3):355. https://doi.org/10.3390/nu16030355
Chicago/Turabian StyleGaweł, Eliza, Barbara Hall, Szymon Siatkowski, Agata Grabowska, and Anna Zwierzchowska. 2024. "The Combined Effects of High-Intensity Interval Exercise Training and Dietary Supplementation on Reduction of Body Fat in Adults with Overweight and Obesity: A Systematic Review" Nutrients 16, no. 3: 355. https://doi.org/10.3390/nu16030355
APA StyleGaweł, E., Hall, B., Siatkowski, S., Grabowska, A., & Zwierzchowska, A. (2024). The Combined Effects of High-Intensity Interval Exercise Training and Dietary Supplementation on Reduction of Body Fat in Adults with Overweight and Obesity: A Systematic Review. Nutrients, 16(3), 355. https://doi.org/10.3390/nu16030355