
The Effects of High-Intensity Interval Training and Moderate Alcohol Consumption on Cognitive Performance—A Multidisciplinary Intervention in Young Healthy Adults
 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design
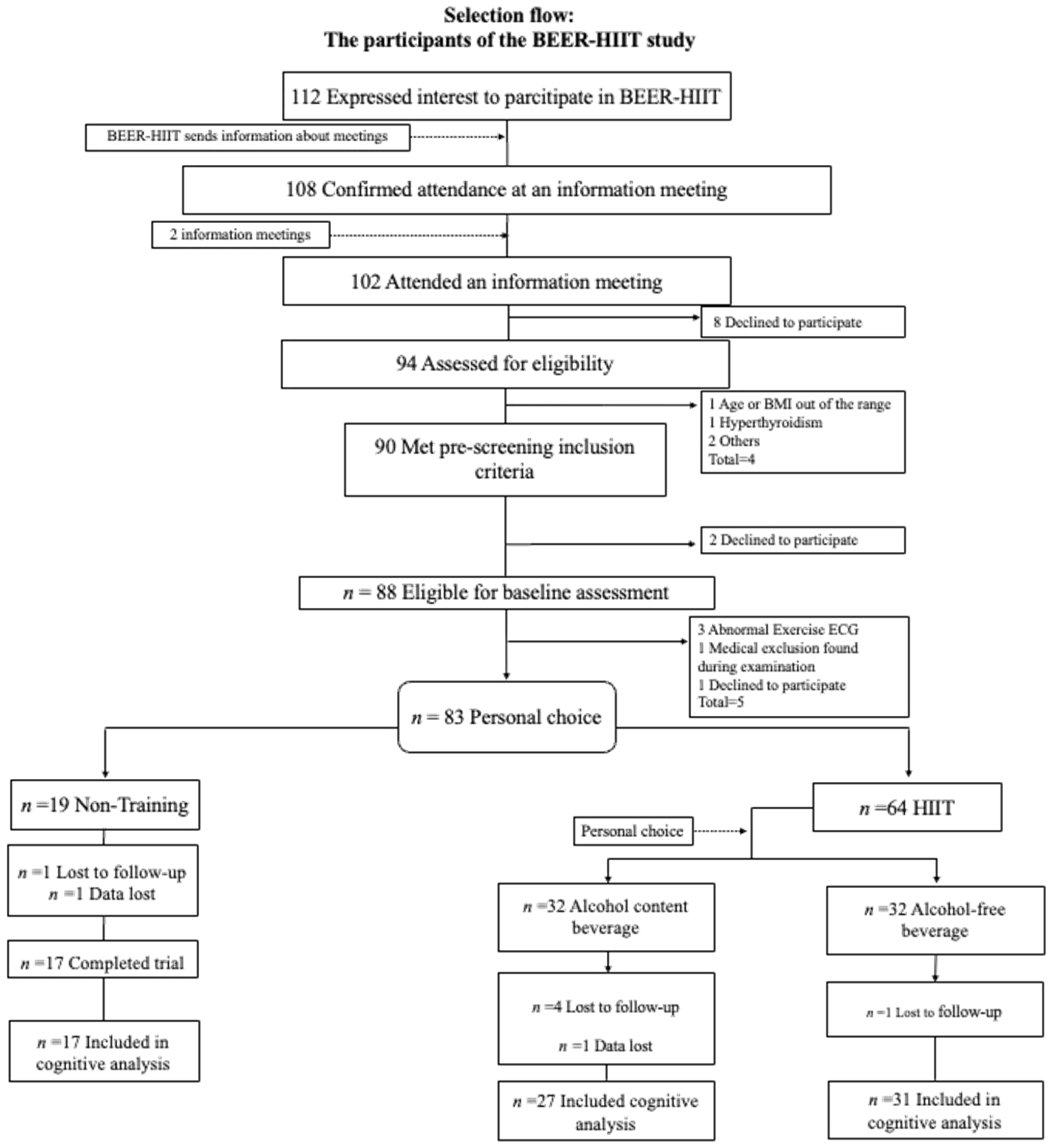
2.2. Participants
2.3. Randomization and Follow-Up
2.4. Intervention
2.5. Cognitive Function
2.6. Statistical Analyses
3. Results
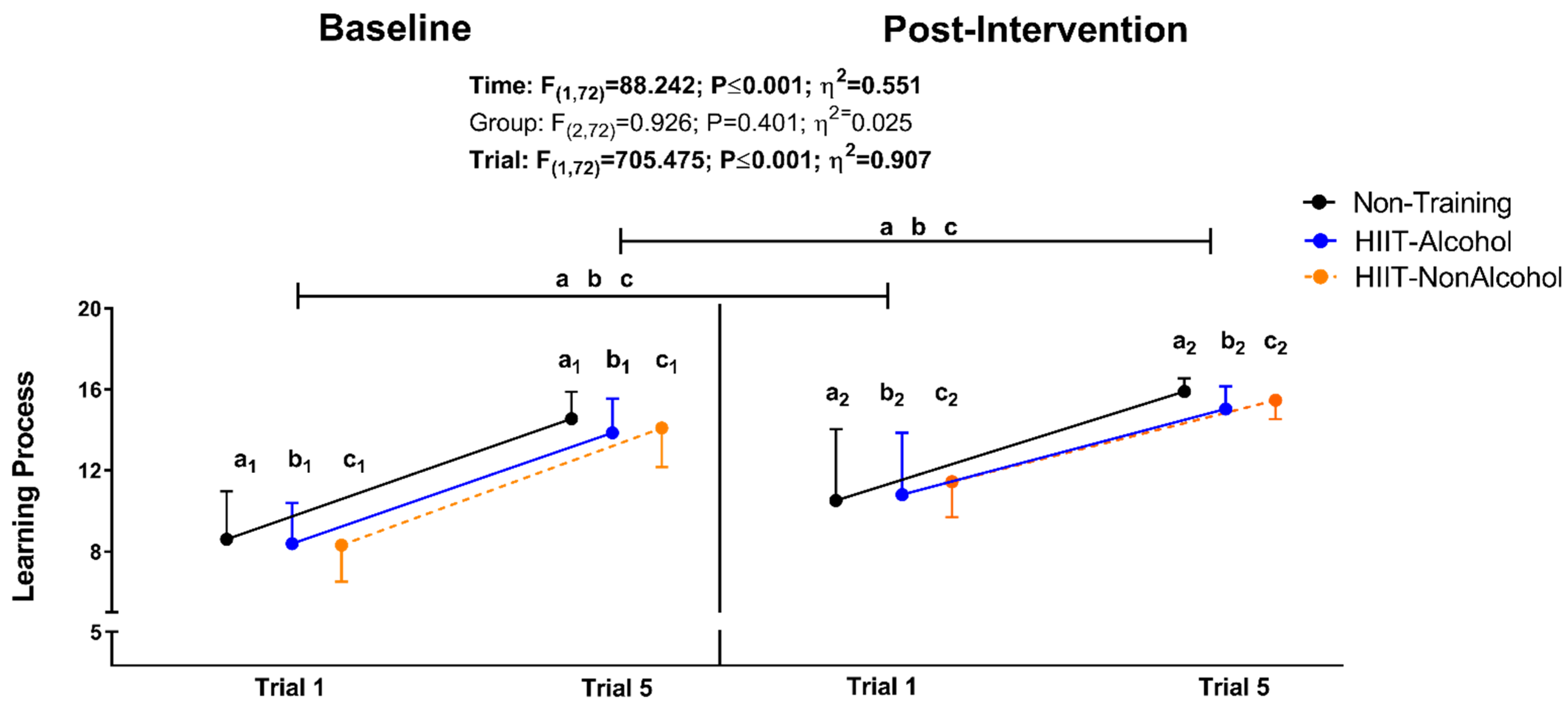
3.1. Intervention Effects of an HIIT Program on Cognitive Function
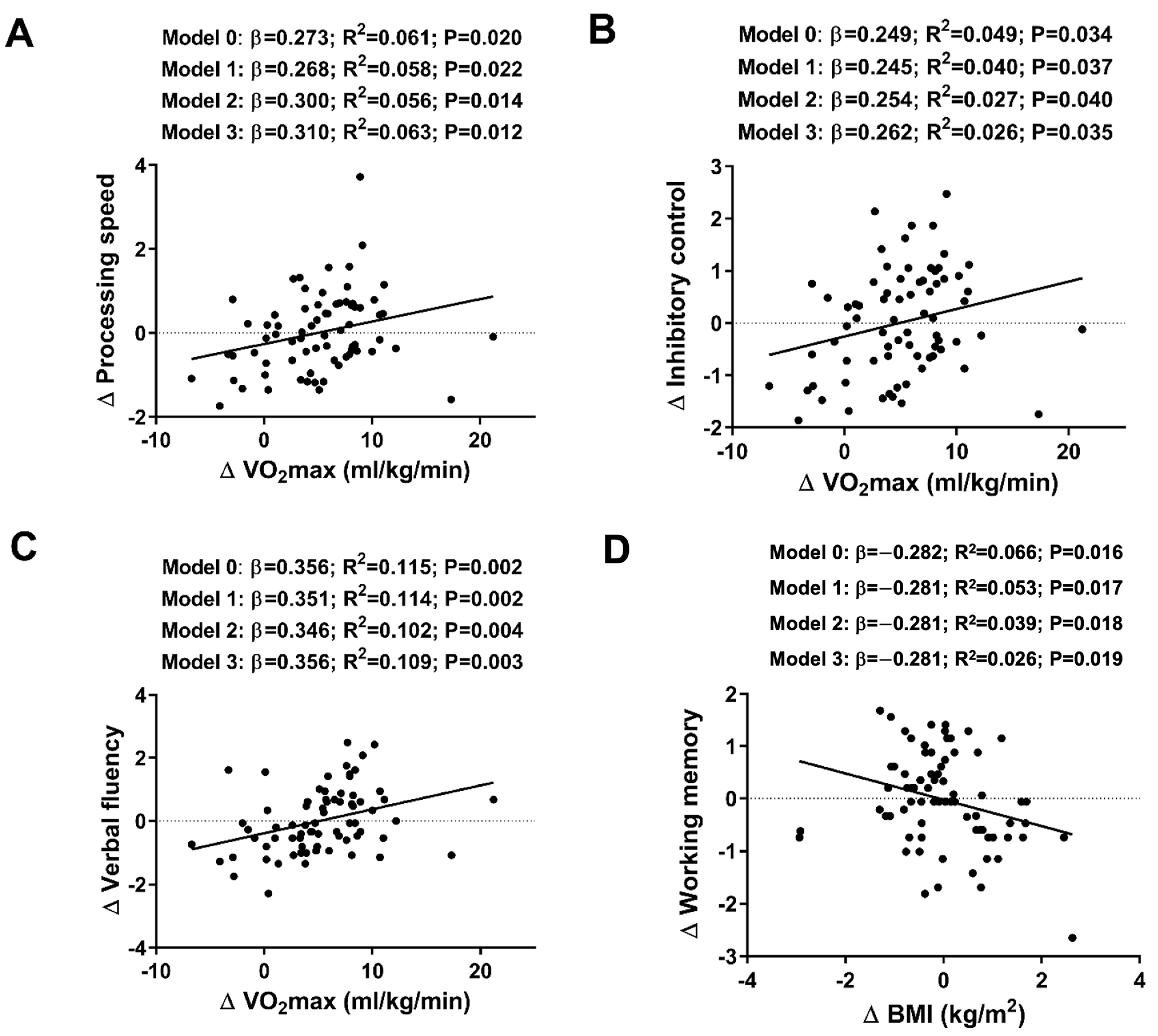
3.2. Are Exercise-Induced Changes in Cognitive Function Explained by Those Obtained in Physical Fitness and Body Composition after the Intervention?
4. Discussion
4.1. Intervention Effects of an HIIT Program on Cognitive Function
4.2. Are Exercise-Induced Changes in Cognitive Function Explained by Those Obtained in Physical Fitness and Body Composition after the Intervention?
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Models | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Analysis of Covariance | |||||||||
| F | p Value | η2 | F | p Value | η2 | F | p Value | η2 | |
| Memory | |||||||||
| Immediate memory | 0.767 | 0.468 | 0.021 | 0.790 | 0.458 | 0.022 | 0.718 | 0.491 | 0.020 |
| Short-term memory | 0.350 | 0.706 | 0.010 | 0.768 | 0.468 | 0.021 | 0.633 | 0.534 | 0.018 |
| Delay memory | 1.108 | 0.336 | 0.031 | 1.816 | 0.170 | 0.049 | 1.689 | 0.192 | 0.046 |
| Recognition (tc) | 2.438 | 0.095 | 0.065 | 1.887 | 0.160 | 0.051 | 1.724 | 0.186 | 0.047 |
| Recognition (id) | 0.837 | 0.437 | 0.023 | 1.653 | 0.199 | 0.045 | 1.335 | 0.270 | 0.037 |
| Composite score | 0.749 | 0.477 | 0.021 | 1.292 | 0.281 | 0.036 | 1.051 | 0.355 | 0.029 |
| Working Memory | |||||||||
| Direct Score | 0.084 | 0.919 | 0.002 | 0.105 | 0.901 | 0.003 | 0.064 | 0.938 | 0.002 |
| Processing Score | 0.498 | 0.610 | 0.014 | 0.501 | 0.608 | 0.014 | 0.430 | 0.652 | 0.012 |
| Composite score | 0.140 | 0.870 | 0.004 | 0.162 | 0.851 | 0.005 | 0.111 | 0.895 | 0.003 |
| Processing Speed | |||||||||
| Total productivity | 0.502 | 0.608 | 0.014 | 0.645 | 0.528 | 0.018 | 0.724 | 0.489 | 0.020 |
| Correct work | 0.304 | 0.739 | 0.009 | 0.570 | 0.569 | 0.016 | 0.630 | 0.536 | 0.018 |
| Concentration Index | 0.371 | 0.691 | 0.011 | 0.480 | 0.621 | 0.014 | 0.763 | 0.470 | 0.021 |
| Composite score | 0.413 | 0.663 | 0.012 | 0.637 | 0.532 | 0.018 | 0.783 | 0.461 | 0.022 |
| Inhibitory Control | |||||||||
| Omissions | 1.109 | 0.335 | 0.031 | 1.397 | 0.254 | 0.038 | 1.330 | 0.271 | 0.037 |
| Total Effectiveness | 0.406 | 0.668 | 0.011 | 0.643 | 0.529 | 0.018 | 0.603 | 0.550 | 0.017 |
| Verbal Fluency | |||||||||
| Total Phonologic | 0.771 | 0.467 | 0.022 | 1.020 | 0.366 | 0.028 | 0.691 | 0.504 | 0.019 |
| Total Semantic | 2.098 | 0.130 | 0.057 | 2.450 | 0.094 | 0.065 | 2.459 | 0.093 | 0.066 |
| Total Score | 1.067 | 0.350 | 0.030 | 1.237 | 0.296 | 0.034 | 0.886 | 0.417 | 0.025 |
Appendix B
| VO2max (mL/min) | VO2max (mL/kg/min) | Hand Grip Strength | Hand Grip Strength/Weight | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | R2 | p | β | R2 | p | β | R2 | p | β | R2 | p | |
| Memory | ||||||||||||
| Model 0 | 0.135 | 0.004 | 0.256 | 0.102 | 0.004 | 0.390 | 0.018 | −0.014 | 0.880 | −0.010 | −0.014 | 0.932 |
| Model 1 | 0.133 | −0.007 | 0.263 | 0.100 | −0.015 | 0.405 | 0.016 | −0.023 | 0.892 | −0.015 | −0.024 | 0.899 |
| Model 2 | 0.063 | 0.018 | 0.612 | 0.039 | 0.015 | 0.705 | 0.000 | 0.023 | 0.999 | −0.011 | 0.022 | 0.924 |
| Model 3 | 0.055 | 0.015 | 0.662 | 0.031 | 0.013 | 0.708 | −0.015 | 0.021 | 0.897 | −0.034 | 0.021 | 0.777 |
| Working Memory | ||||||||||||
| Model 0 | −0.122 | 0.001 | 0.302 | −0.021 | −0.014 | 0.863 | −0.174 | 0.017 | 0.138 | −0.066 | −0.010 | 0.579 |
| Model 1 | −0.123 | −0.012 | 0.303 | −0.022 | −0.027 | 0.854 | −0.175 | 0.004 | 0.139 | −0.068 | −0.024 | 0.571 |
| Model 2 | −0.146 | −0.023 | 0.254 | −0.029 | −0.041 | 0.817 | −0.176 | −0.010 | 0.140 | −0.069 | −0.039 | 0.573 |
| Model 3 | −0.149 | −0.036 | 0.249 | −0.031 | −0.056 | 0.806 | −0.185 | −0.020 | 0.127 | −0.081 | −0.050 | 0.515 |
| Processing Speed | ||||||||||||
| Model 0 | 0.198 | 0.025 | 0.094 | 0.273 | 0.061 | 0.020 | −0.034 | −0.013 | 0.775 | −0.047 | −0.012 | 0.693 |
| Model 1 | 0.195 | 0.023 | 0.098 | 0.268 | 0.058 | 0.022 | −0.037 | −0.012 | 0.755 | −0.056 | −0.012 | 0.641 |
| Model 2 | 0.233 | 0.020 | 0.065 | 0.300 | 0.056 | 0.014 | −0.037 | −0.027 | 0.758 | −0.056 | −0.026 | 0.642 |
| Model 3 | 0.244 | 0.026 | 0.054 | 0.301 | 0.063 | 0.012 | −0.020 | −0.025 | 0.871 | −0.033 | −0.028 | 0.790 |
| Inhibitory Control | ||||||||||||
| Model 0 | 0.176 | 0.017 | 0.137 | 0.249 | 0.049 | 0.034 | −0.006 | −0.014 | 0.960 | −0.004 | −0.014 | 0.971 |
| Model 1 | 0.174 | 0.010 | 0.141 | 0.245 | 0.040 | 0.037 | −0.008 | −0.019 | 0.944 | −0.011 | −0.021 | 0.927 |
| Model 2 | 0.182 | −0.004 | 0.153 | 0.254 | 0.027 | 0.040 | −0.013 | −0.030 | 0.916 | −0.010 | −0.033 | 0.933 |
| Model 3 | 0.190 | −0.007 | 0.137 | 0.262 | 0.026 | 0.035 | 0.001 | −0.034 | 0.991 | 0.010 | −0.038 | 0.936 |
| Verbal Fluency | ||||||||||||
| Model 0 | 0.313 | 0.085 | 0.007 | 0.356 | 0.115 | 0.002 | 0.077 | −0.008 | 0.514 | 0.072 | −0.009 | 0.547 |
| Model 1 | 0.311 | 0.087 | 0.007 | 0.351 | 0.114 | 0.002 | 0.074 | −0.008 | 0.532 | 0.064 | −0.011 | 0.595 |
| Model 2 | 0.308 | 0.074 | 0.013 | 0.346 | 0.102 | 0.004 | 0.069 | −0.016 | 0.563 | 0.065 | −0.024 | 0.593 |
| Model 3 | 0.319 | 0.080 | 0.010 | 0.356 | 0.109 | 0.003 | 0.084 | −0.018 | 0.484 | 0.084 | −0.030 | 0.499 |
Appendix C
| BMI | FMI | LMI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | R2 | p | β | R2 | p | β | R2 | p | |
| Memory | |||||||||
| Model 0 | 0.004 | −0.014 | 0.970 | 0.136 | 0.005 | 0.251 | −0.125 | 0.002 | 0.293 |
| Model 1 | 0.008 | −0.024 | 0.945 | 0.133 | −0.006 | 0.263 | −0.118 | −0.010 | 0.327 |
| Model 2 | 0.002 | 0.026 | 0.988 | 0.136 | 0.046 | 0.241 | −0.130 | 0.044 | 0.266 |
| Model 3 | 0.003 | 0.023 | 0.978 | 0.139 | 0.043 | 0.234 | −0.138 | 0.042 | 0.243 |
| Working Memory | |||||||||
| Model 0 | −0.282 | 0.066 | 0.016 | −0.213 | 0.032 | 0.070 | −0.059 | −0.011 | 0.619 |
| Model 1 | −0.281 | 0.053 | 0.017 | −0.215 | 0.019 | 0.070 | −0.057 | −0.025 | 0.637 |
| Model 2 | −0.281 | 0.039 | 0.018 | −0.215 | 0.005 | 0.072 | −0.057 | −0.040 | 0.639 |
| Model 3 | −0.281 | 0.026 | 0.019 | −0.214 | −0.008 | 0.075 | −0.060 | −0.053 | 0.626 |
| Processing Speed | |||||||||
| Model 0 | 0.112 | −0.001 | 0.344 | 0.058 | −0.011 | 0.626 | 0.038 | −0.013 | 0.749 |
| Model 1 | 0.119 | 0.000 | 0.316 | 0.053 | −0.012 | 0.657 | 0.054 | −0.012 | 0.652 |
| Model 2 | 0.120 | −0.014 | 0.318 | 0.053 | −0.026 | 0.660 | 0.055 | −0.026 | 0.648 |
| Model 3 | 0.118 | −0.014 | 0.324 | 0.050 | −0.026 | 0.677 | 0.063 | −0.025 | 0.602 |
| Inhibitory Control | |||||||||
| Model 0 | 0.065 | −0.010 | 0.587 | 0.050 | −0.012 | 0.672 | 0.031 | −0.013 | 0.791 |
| Model 1 | 0.070 | −0.015 | 0.559 | 0.047 | −0.018 | 0.697 | 0.044 | −0.018 | 0.715 |
| Model 2 | 0.069 | −0.028 | 0.569 | 0.047 | −0.030 | 0.695 | 0.042 | −0.031 | 0.732 |
| Model 3 | 0.067 | −0.034 | 0.577 | 0.045 | −0.036 | 0.710 | 0.048 | −0.036 | 0.694 |
| Verbal Fluency | |||||||||
| Model 0 | 0.185 | 0.021 | 0.118 | 0.190 | 0.022 | 0.108 | −0.090 | −0.006 | 0.450 |
| Model 1 | 0.192 | 0.023 | 0.105 | 0.185 | 0.021 | 0.118 | −0.076 | −0.009 | 0.527 |
| Model 2 | 0.190 | 0.012 | 0.109 | 0.186 | 0.011 | 0.118 | −0.079 | −0.019 | 0.512 |
| Model 3 | 0.189 | 0.006 | 0.113 | 0.183 | 0.004 | 0.124 | −0.073 | −0.026 | 0.545 |
References
- Erickson, K.I.; Hillman, C.; Stillman, C.M.; Ballard, R.M.; Bloodgood, B.; Conroy, D.E.; Macko, R.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E. Physical Activity, Cognition, and Brain Outcomes: A Review of the 2018 Physical Activity Guidelines. Med. Sci. Sports Exerc. 2019, 51, 1242–1251. [Google Scholar] [CrossRef]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be Smart, Exercise Your Heart: Exercise Effects on Brain and Cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Stillman, C.M.; Esteban-Cornejo, I.; Brown, B.; Bender, C.M.; Erickson, K.I. Effects of Exercise on Brain and Cognition Across Age Groups and Health States. Trends Neurosci. 2020, 43, 533–543. [Google Scholar] [CrossRef]
- Erickson, K.I.; Gildengers, A.G.; Butters, M.A. Physical Activity and Brain Plasticity in Late Adulthood. Dialogues Clin. Neurosci. 2013, 15, 99–108. [Google Scholar] [CrossRef]
- Stroth, S.; Hille, K.; Spitzer, M.; Reinhardt, R. Aerobic Endurance Exercise Benefits Memory and Affect in Young Adults. Neuropsychol. Rehabil. 2009, 19, 223–243. [Google Scholar] [CrossRef]
- Pereira, A.C.; Huddleston, D.E.; Brickman, A.M.; Sosunov, A.A.; Hen, R.; McKhann, G.M.; Sloan, R.; Gage, F.H.; Brown, T.R.; Small, S.A. An in Vivo Correlate of Exercise-Induced Neurogenesis in the Adult Dentate Gyrus. Proc. Natl. Acad. Sci. USA 2007, 104, 5638–5643. [Google Scholar] [CrossRef]
- Mekari, S.; Neyedli, H.F.; Fraser, S.; O’brien, M.W.; Martins, R.; Evans, K.; Earle, M.; Aucoin, R.; Chiekwe, J.; Hollohan, Q.; et al. High-Intensity Interval Training Improves Cognitive Flexibility in Older Adults. Brain Sci. 2020, 10, 796. [Google Scholar] [CrossRef]
- Venckunas, T.; Snieckus, A.; Trinkunas, E.; Baranauskiene, N.; Solianik, R.; Juodsnukis, A.; Streckis, V.; Kamandulis, S. Interval Running Training Improves Cognitive Flexibility and Aerobic Power of Young Healthy Adults. J. Strength. Cond. Res. 2016, 30, 2114–2121. [Google Scholar] [CrossRef]
- Alves, C.R.R.; Tessaro, V.H.; Teixeira, L.A.C.; Murakava, K.; Roschel, H.; Gualano, B.; Takito, M.Y. Influence of Acute High-Intensity Aerobic Interval Exercise Bout on Selective Attention and Short-Term Memory Tasks. Percept. Mot. Skills 2014, 118, 63–72. [Google Scholar] [CrossRef]
- Tomporowski, P.D.; Pesce, C. Exercise, Sports, and Performance Arts Benefit Cognition via a Common Process. Psychol. Bull. 2019, 145, 929–951. [Google Scholar] [CrossRef]
- De Gaetano, G.; Costanzo, S.; Di Castelnuovo, A.; Badimon, L.; Bejko, D.; Alkerwi, A.; Chiva-Blanch, G.; Estruch, R.; La Vecchia, C.; Panico, S.; et al. Effects of Moderate Beer Consumption on Health and Disease: A Consensus Document. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 443–467. [Google Scholar] [CrossRef]
- Maughan, R.J. Alcohol and Football. In Nutrition and Football: The FIFA/FMARC Consensus on Sports Nutrition; Routledge: London, UK, 2006; pp. 121–133. [Google Scholar] [CrossRef]
- Zhou, J.; Heim, D. Sports and Spirits: A Systematic Qualitative Review of Emergent Theories for Student-Athlete Drinking. Alcohol Alcohol. 2014, 49, 604–617. [Google Scholar] [CrossRef]
- Bill, F.; Foundation, M.G. Articles Alcohol Use and Burden for 195 Countries and Territories, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef]
- Mehlig, K.; Skoog, I.; Guo, X.; Schutze, M.; Gustafson, D.; Waern, M.; Ostling, S.; Bjorkelund, C.; Lissner, L. Alcoholic Beverages and Incidence of Dementia: 34-Year Follow-up of the Prospective Population Study of Women in Goteborg. Am. J. Epidemiol. 2007, 167, 684–691. [Google Scholar] [CrossRef]
- Hebert, L.E.; Scherr, P.A.; Beckett, L.A.; Albert, M.S.; Rosner, B.; Talor, J.O.; Evans, D.A. Relation of Smoking and Low-to-Moderate Alcohol Consumption to Change in Cognitive Function: A Longitudinal Study in a Defined Community of Older Persons. Am. J. Epidemiol. 1993, 137, 881–891. [Google Scholar] [CrossRef]
- Elwood, P.C.; Gallacher, J.E.J.; Hopkinson, C.A.; Pickering, J.; Rabbitt, P.; Stollery, B.; Brayne, C.; Huppert, F.A.; Bayer, A. Smelting, Drinking, and Other Life Style Factors and Cognitive Function in Men in the Caerphilly Cohort. J. Epidemiol. Community Health (1978) 1999, 53, 9–14. [Google Scholar] [CrossRef]
- Zhang, R.; Shen, L.; Miles, T.; Shen, Y.; Cordero, J.; Qi, Y.; Liang, L.; Li, C. Association of Low to Moderate Alcohol Drinking with Cognitive Functions from Middle to Older Age Among US Adults. JAMA Netw. Open 2020, 3, e207922. [Google Scholar] [CrossRef]
- Ganguli, M.; Vander Bilt, J.; Saxton, J.A.; Shen, C.; Dodge, H.H. Alcohol Consumption and Cognitive Function in Late Life: A Longitudinal Community Study. Neurology 2005, 65, 1210–1217. [Google Scholar] [CrossRef]
- Samuelson, G. Global Strategy on Diet, Physical Activity and Health. Scand. J. Nutr. 2004, 48, 57. [Google Scholar] [CrossRef]
- Gunnar, A.V. Borg Psychophysical Bases of Perceived Exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar]
- Gillach, M.C.; Sallis, J.F.; Buono, M.J.; Patterson, P.; Nader, P.R. The Relationship Between Perceived Exertion and Heart Rate in Children and Adults. Pediatr. Exerc. Sci. 1989, 1, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Lamb, K.L. Children’s Ratings of Effort during Cycle Ergometry: An Examination of the Validity of Two Effort Rating Scales. Pediatr. Exerc. Sci. 1995, 7, 407–421. [Google Scholar] [CrossRef]
- Molina-Hidalgo, C.; De-la-O, A.; Jurado-Fasoli LAmaro-Gahete, F.J.; Catena, A.; Castillo, M. Investigating the Alcohol Effects on the Response to Strenuous Exercise Training: Protocol for a Multidisciplinary Intervention Study in Young Healthy Adults—The BEER-HIIT Study. Subst. Use Addict. J. 2024. [Google Scholar] [CrossRef] [PubMed]
- Jurado-Fasoli, L.; Amaro-Gahete, F.J.; De-la-O, A.; Gutiérrez, Á.; Castillo, M.J. Alcohol Consumption and S-Klotho Plasma Levels in Sedentary Healthy Middle-Aged Adults: A Cross Sectional Study. Drug Alcohol. Depend. 2019, 194, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Poli, A.; Marangoni, F.; Avogaro, A.; Barba, G.; Bellentani, S.; Bucci, M.; Cambieri, R.; Catapano, A.L.; Costanzo, S.; Cricelli, C.; et al. Moderate Alcohol Use and Health: A Consensus Document. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 487–504. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Comber, D.L.; Estabrooks, P.A.; Savla, J.; Davy, B.M. The Beverage Intake Questionnaire: Determining Initial Validity and Reliability. J. Am. Diet. Assoc. 2010, 110, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Nissensohn, M.; López-Ufano, M.; Castro-Quezada, I.; et Serra-Majem, L. Valoración de La Ingesta de Bebidas y Del Estado de Hidratación. Span. J. Community Nutr. 2002, 21, 58–65. [Google Scholar]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Benedet, M.; Alejandre, M. TAVEC: Test de Aprendizaje Verbal España-Complutense; Tea: Madrid, Spain, 1998; ISBN 8471745291. [Google Scholar]
- Weschler, D. Wechsler Adult Intelligence Scale, 4th ed.; Statistics Solutions: Clearwater, FL, USA, 2008. [Google Scholar] [CrossRef]
- Bates, M.E.; Lemay, E.P. The D2 Test of Attention: Construct Validity and Extensions in Scoring Techniques. J. Int. Neuropsychol. Soc. 2004, 10, 392–400. [Google Scholar] [CrossRef]
- Olabarrieta-Landa, L.; Torre, E.L.; López-Mugartza, J.C.; Bialystok, E.; Arango-Lasprilla, J.C. Verbal Fluency Tests: Developing a New Model of Administration and Scoring for Spanish Language. NeuroRehabilitation 2017, 41, 539–565. [Google Scholar] [CrossRef]
- Molina-Hidalgo, C.; De-Lao, A.; Jurado-Fasoli, L.; Amaro-Gahete, F.J.; Castillo, M.J. Beer or Ethanol Effects on the Body Composition Response to High-Intensity Interval Training. The BEER-HIIT Study. Nutrients 2019, 11, 909. [Google Scholar] [CrossRef] [PubMed]
- Molina-Hidalgo, C.; De-La-O, A.; Dote-Montero, M.; Amaro-Gahete, F.J.; Castillo, M.J. Influence of Daily Beer or Ethanol Consumption on Physical Fitness in Response to a High-Intensity Interval Training Program. The BEER-HIIT Study. J. Int. Soc. Sports Nutr. 2020, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, M.L.; Chinchilli, V.M. Including Multiple Imputation in a Sensitivity Analysis for Clinical Trials with Treatment Failures. Contemp. Clin. Trials 2007, 28, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Reljic, D.; Lampe, D.; Wolf, F.; Zopf, Y.; Herrmann, H.J.; Fischer, J. Prevalence and Predictors of Dropout from High-intensity Interval Training in Sedentary Individuals: A Meta-analysis. Scand. J. Med. Sci. Sports 2019, 29, 1288–1304. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Donofry, S.D.; Sewell, K.R.; Brown, B.M.; Stillman, C.M. Cognitive Aging and the Promise of Physical Activity. Annu. Rev. Clin. Psychol. 2022, 18, 417–442. [Google Scholar] [CrossRef]
- Winter, B.; Breitenstein, C.; Mooren, F.C.; Voelker, K.; Fobker, M.; Lechtermann, A.; Krueger, K.; Fromme, A.; Korsukewitz, C.; Floel, A.; et al. High Impact Running Improves Learning. Neurobiol. Learn. Mem. 2007, 87, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Coetsee, C.; Terblanche, E. The Effect of Three Different Exercise Training Modalities on Cognitive and Physical Function in a Healthy Older Population. Eur. Rev. Aging Phys. Act. 2017, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Topiwala, A.; Allan, C.L.; Valkanova, V.; Zsoldos, E.; Filippini, N.; Sexton, C.; Mahmood, A.; Fooks, P.; Singh-Manoux, A.; Mackay, C.E.; et al. Moderate Alcohol Consumption as Risk Factor for Adverse Brain Outcomes and Cognitive Decline: Longitudinal Cohort Study. BMJ 2017, 357, j2353. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Room, R.; Graham, K.; Monteiro, M.; Gmel, G.; Sempos, C.T. The Relationship of Average Volume of Alcohol Consumption and Patterns of Drinking to Burden of Disease: An Overview. Addiction 2003, 98, 1209–1228. [Google Scholar] [CrossRef]
- Cox, E.P.; O’Dwyer, N.; Cook, R.; Vetter, M.; Cheng, H.L.; Rooney, K.; O’Connor, H. Relationship between Physical Activity and Cognitive Function in Apparently Healthy Young to Middle-Aged Adults: A Systematic Review. J. Sci. Med. Sport. 2016, 19, 616–628. [Google Scholar] [CrossRef]
- Cherup, N.; Roberson, K.; Potiaumpai, M.; Widdowson, K.; Jaghab, A.M.; Chowdhari, S.; Armitage, C.; Seeley, A.; Signorile, J. Improvements in Cognition and Associations with Measures of Aerobic Fitness and Muscular Power Following Structured Exercise. Exp. Gerontol. 2018, 112, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Colcombe, S.; Kramer, A.F. Fitness Effects on the Cognitive Function of Older Adults: A Meta-Analytic Study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Mekari, S.; Dupuy, O.; Martins, R.; Evans, K.; Kimmerly, D.S.; Fraser, S.; Neyedli, H.F. The Effects of Cardiorespiratory Fitness on Executive Function and Prefrontal Oxygenation in Older Adults. Geroscience 2019, 41, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Prickett, C.; Brennan, L.; Stolwyk, R. Examining the Relationship between Obesity and Cognitive Function: A Systematic Literature Review. Obes. Res. Clin. Pract. 2015, 9, 93–113. [Google Scholar] [CrossRef]
- Stanek, K.M.; Strain, G.; Devlin, M.; Cohen, R.; Paul, R.; Crosby, R.D.; Mitchell, J.E.; Gunstad, J. Body Mass Index and Neurocognitive Functioning Across the Adult Lifespan. Neuropsychology 2013, 27, 141. [Google Scholar] [CrossRef]
| Non-Training (n = 17) | HIIT-Alcohol (n = 27) | HIIT-NonAlcohol (n = 31) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | p Value | |||||||||
| Sex (men%/women%) | 64.7%/35.3% | 48.1%/51.8% | 54.8%/45.2% | 0.572 | ||||||
| Age | 20.2 ± 1.3 | 24.2 ± 1.5 | 24.5 ± 1.5 | 0.006 * | ||||||
| Alcohol Ingested (mL/week) | 1144.1 ± 831.9 | 696.7 ± 857.4 | 1204.5 ± 1167.3 | 0.131 | ||||||
| Educational level (%) | 0.097 | |||||||||
| Primary Education | -- | 3.7% | -- | |||||||
| Secondary Education | 47.1% | 40.7% | 22.5% | |||||||
| Vocational Education and Training | 23.5% | 18.5% | 22.5% | |||||||
| University Degree or Certificate of Higher Education | 29.5% | 37.3% | 54.8% | |||||||
| Occupational activity (%) | 0.005 * | |||||||||
| Level 1 | 100% † | 55.6% | 54.8% | |||||||
| Level 2 | -- | 18.5% | 16.1% | |||||||
| Level 3 | -- | 25.9% | 29.1% | |||||||
| Learning Process | ||||||||||
| Trial 1 | 8.8 ± 2.3 | 8.3 ± 2.0 | 8.3 ± 1.8 | 0.666 | ||||||
| Trial 2 | 11.2 ± 2.7 | 12.2 ± 2.1 | 11.4 ± 2.3 | 0.269 | ||||||
| Trial 3 | 12.9 ± 2.3 | 13.1 ± 2.2 | 12.4 ± 2.7 | 0.530 | ||||||
| Trial 4 | 14.4 ± 1.3 | 13.4 ± 2.1 | 13.4 ± 3.1 | 0.329 | ||||||
| Trail 5 | 14.5 ± 1.3 | 13.8 ± 1.7 | 14.1 ± 1.9 | 0.474 | ||||||
| Memory | ||||||||||
| Immediate memory | 61.8 ± 7.4 | 60.9 ± 7.7 | 59.6 ± 9.3 | 0.638 | ||||||
| Short-term memory | 13.6 ± 1.2 | 13.9 ± 1.8 | 12.9 ± 2.5 | 0.170 | ||||||
| Delay memory | 13.9 ± 1.4 | 14.2 ± 1.8 | 13.3 ± 2.2 | 0.224 | ||||||
| Recognition (tc) | 15.3 ± 0.9 | 15.6 ± 0.6 | 15.0 ± 1.4 | 0.115 | ||||||
| Recognition (id) | 97.7 ± 2.7 | 98.2 ± 1.9 | 96.9 ± 4.1 | 0.284 | ||||||
| Working Memory | ||||||||||
| Direct Score | 13.0 ± 1.6 | 11.8 ± 2.1 | 11.7 ± 2.5 | 0.125 | ||||||
| Processing Score | 5.8 ± 0.8 | 5.6 ± 0.9 | 5.5 ± 0.9 | 0.507 | ||||||
| Processing Speed | ||||||||||
| Total productivity | 516.6 ± 88.0 | 514.5 ± 76.5 | 510.9 ± 67.3 | 0.965 | ||||||
| Correct work | 208.7 ± 43.4 | 203.9 ± 39.0 | 200.7 ± 36.5 | 0.793 | ||||||
| Concentration Index | 208.4 ± 43.5 | 203.4 ± 39.4 | 200.0 ± 36.6 | 0.776 | ||||||
| Inhibitory Control | ||||||||||
| Total Effectiveness | 502.9 ± 86.7 | 498.3 ± 77.5 | 492.7 ± 68.1 | 0.900 | ||||||
| Verbal Fluency | ||||||||||
| Phonologic | 86.1 ± 23.2 | 88.4 ± 20.5 | 77.1 ± 15.0 | 0.069 | ||||||
| Semantic | 40.5 ± 8.0 | 40.1 ± 6.5 | 37.5 ± 8.5 | 0.315 | ||||||
| Total Score | 126.6 ± 28.0 | 128.4 ± 23.8 | 114.6 ± 19.3 | 0.057 | ||||||
| Non-Training | HIIT-Alcohol | HIIT-NonAlcohol | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-Intervention | Baseline | Post-Intervention | Baseline | Post-Intervention | Model 0 | ||||||
| Mean ± SD | ||||||||||||
| Memory | p Value | p Value | p Value | F | p Value | η2 | ||||||
| Immediate Memory | 61.82 ± 7.38 | 70.06 ± 5.85 | ≤0.001 | 60.93 ± 7.68 | 70.15 ± 5.56 | ≤0.001 | 59.55 ± 9.26 | 67.94 ± 6.87 | ≤0.001 | 0.788 | 0.459 | 0.022 |
| Short-Term Memory | 13.59 ± 1.23 | 15.29 ± 0.85 | ≤0.001 | 13.85 ± 1.81 | 14.89 ± 1.58 | 0.004 | 12.87 ± 2.47 | 14.77 ± 1.45 | ≤0.001 | 0.850 | 0.432 | 0.023 |
| Delay Memory | 13.88 ± 1.41 | 15.47 ± 0.62 | ≤0.001 | 14.15 ± 1.83 | 14.93 ± 1.62 | 0.0014 | 13.29 ± 2.18 | 15.00 ± 1.13 | ≤0.001 | 2.043 | 0.137 | 0.054 |
| Recognition (tc) | 15.29 ± 0.92 | 16.00 ± 0.00 | 0.005 | 15.56 ± 0.64 | 15.89 ± 0.32 | 0.105 | 14.97 ± 1.38 | 15.68 ± 0.70 | ≤0.001 | 1.956 | 0.149 | 0.052 |
| Recognition (id) | 97.73 ± 2.67 | 99.60 ± 0.89 | 0.014 | 98.23 ± 1.93 | 98.82 ± 1.93 | 0.321 | 96.92 ± 4.09 | 99.12 ± 1.73 | ≤0.001 | 1.632 | 0.203 | 0.044 |
| Composite score | 0.082 ± 0.204 | 0.277 ± 0.174 | 0.315 | 0.195 ± 0.162 | −0.002 ± 0.162 | 0.201 | −0.219 ± 0.151 | −0.125 ± 0.129 | 0.513 | 1.462 | 0.239 | 0.040 |
| Working Memory | ||||||||||||
| Direct Score | 13.00 ± 1.62 | 13.06 ± 3.47 | 0.928 | 11.78 ± 2.08 | 11.96 ± 3.11 | 0.722 | 11.74 ± 2.49 | 11.77 ± 2.97 | 0.947 | 0.116 | 0.891 | 0.003 |
| Processing Score | 5.82 ± 0.81 | 5.88 ± 1.27 | 0.845 | 5.63 ± 0.88 | 5.41 ± 1.12 | 0.354 | 5.52 ± 0.89 | 5.32 ± 1.49 | 0.387 | 0.574 | 0.566 | 0.016 |
| Composite score | 0.349 ± 0.820 | 0.307 ± 1.020 | 0.852 | −0.042 ± 0.186 | −0.050 ± 0.183 | 0.966 | −0.117 ± 0.173 | −0.113 ± 0.171 | 0.982 | 0.187 | 0.830 | 0.005 |
| Processing Speed | ||||||||||||
| Total productivity | 516.59 ± 87.93 | 576.59 ± 72.84 | ≤0.001 | 514.52 ± 76.49 | 566.07 ± 67.83 | ≤0.001 | 510.87 ± 67.316 | 571.87 ± 52.41 | ≤0.001 | 0.691 | 0.504 | 0.019 |
| Correct work | 208.71 ± 43.44 | 244.82 ± 39.72 | ≤0.001 | 203.85 ± 39.04 | 235.15 ± 36.43 | ≤0.001 | 200.68 ± 36.54 | 237.29 ± 39.76 | ≤0.001 | 0.530 | 0.591 | 0.015 |
| Concentration Index | 208.41 ± 43.46 | 242.94 ± 41.62 | ≤0.001 | 203.44 ± 39.37 | 234.85 ± 36.50 | ≤0.001 | 200.00 ± 36.58 | 236.94 ± 39.72 | ≤0.001 | 0.442 | 0.644 | 0.012 |
| Composite score | 0.102 ± 0.245 | 0.136 ± 0.240 | 0.783 | 0.007 ± 0.194 | −0.075 ± 0.180 | 0.399 | −0.067 ± 0.181 | −0.007 ± 0.178 | 0.516 | 0.618 | 0.542 | 0.017 |
| Inhibitory Control | ||||||||||||
| Total Effectiveness | 502.82 ± 86.61 | 565.18 ± 74.533 | ≤0.001 | 498.26 ± 77.45 | 552.22 ± 66.00 | ≤0.001 | 492.61 ± 68.01 | 554.87 ± 55.62 | ≤0.001 | 0.713 | 0.494 | 0.020 |
| Verbal Fluency | ||||||||||||
| Phonologic | 86.12 ± 23.15 | 95.71 ± 24.51 | 0.003 | 88.37 ± 20.55 | 96.89 ± 16.70 | ≤0.001 | 77.10 ± 14.93 | 84.42 ± 17.16 | 0.002 | 0.964 | 0.386 | 0.026 |
| Semantic | 40.47 ± 8.02 | 39.88 ± 10.78 | 0.705 | 40.11 ± 6.47 | 42.37 ± 6.03 | 0.070 | 37.48 ± 8.55 | 37.48 ± 6.74 | 1.000 | 2.364 | 0.101 | 0.062 |
| Total Verbal Fluency | 126.59 ± 27.97 | 135.59 ± 33.55 | 0.016 | 128.41 ± 23.76 | 139.26 ± 21.09 | ≤0.001 | 114.58 ± 19.25 | 121.90 ± 20.06 | 0.008 | 1.103 | 0.338 | 0.030 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-Hidalgo, C.; Amaro-Gahete, F.J.; Peven, J.C.; Erickson, K.I.; Catena, A.; Castillo, M.J. The Effects of High-Intensity Interval Training and Moderate Alcohol Consumption on Cognitive Performance—A Multidisciplinary Intervention in Young Healthy Adults. Nutrients 2024, 16, 1680. https://doi.org/10.3390/nu16111680
Molina-Hidalgo C, Amaro-Gahete FJ, Peven JC, Erickson KI, Catena A, Castillo MJ. The Effects of High-Intensity Interval Training and Moderate Alcohol Consumption on Cognitive Performance—A Multidisciplinary Intervention in Young Healthy Adults. Nutrients. 2024; 16(11):1680. https://doi.org/10.3390/nu16111680
Chicago/Turabian StyleMolina-Hidalgo, Cristina, Francisco J. Amaro-Gahete, Jamie C. Peven, Kirk I. Erickson, Andres Catena, and Manuel J. Castillo. 2024. "The Effects of High-Intensity Interval Training and Moderate Alcohol Consumption on Cognitive Performance—A Multidisciplinary Intervention in Young Healthy Adults" Nutrients 16, no. 11: 1680. https://doi.org/10.3390/nu16111680
APA StyleMolina-Hidalgo, C., Amaro-Gahete, F. J., Peven, J. C., Erickson, K. I., Catena, A., & Castillo, M. J. (2024). The Effects of High-Intensity Interval Training and Moderate Alcohol Consumption on Cognitive Performance—A Multidisciplinary Intervention in Young Healthy Adults. Nutrients, 16(11), 1680. https://doi.org/10.3390/nu16111680