
Healthy Lifestyle, Metabolic Signature, and Risk of Cardiovascular Diseases: A Population-Based Study




Highlights
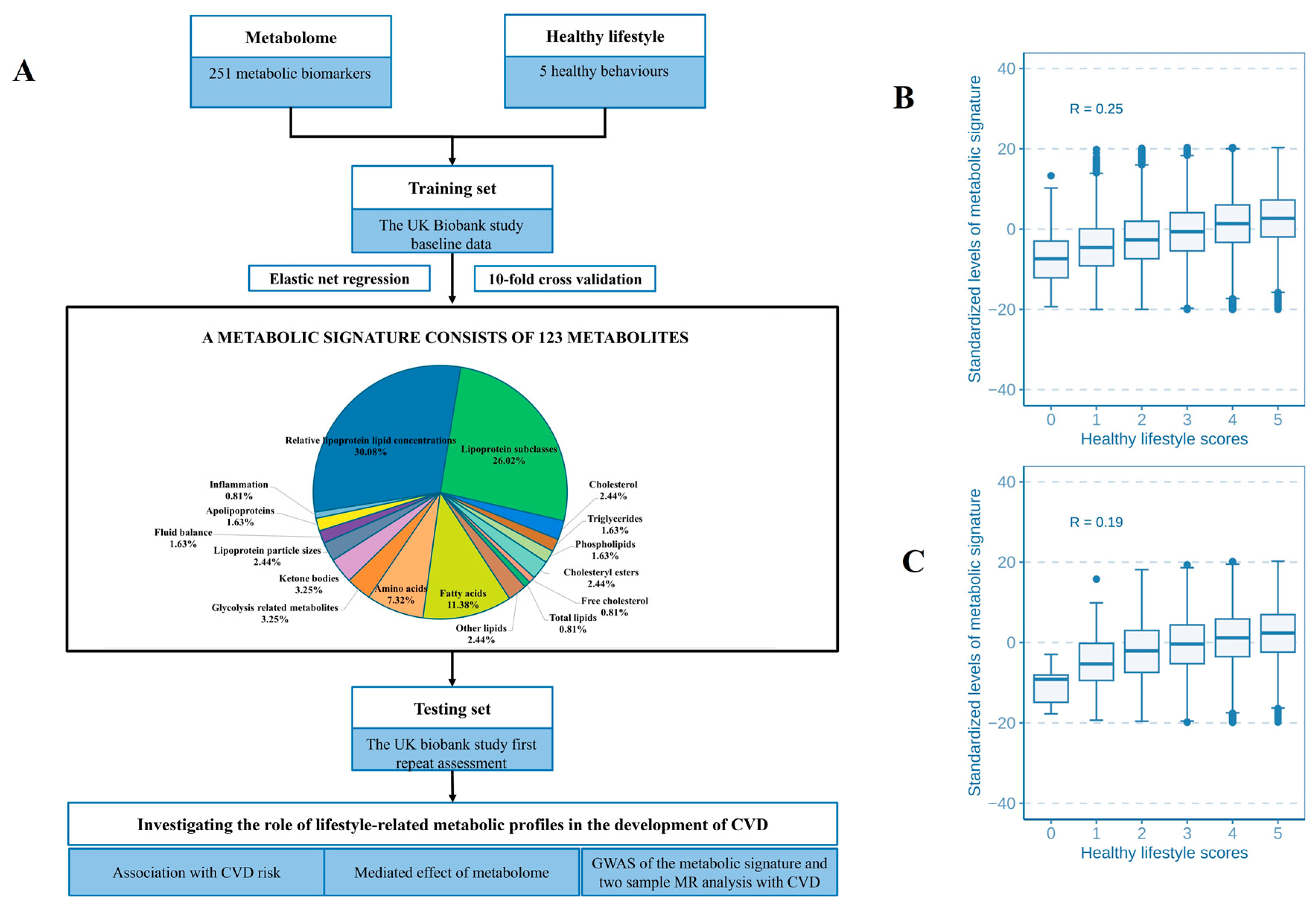
- Our study identified 123 metabolites in order to establish the metabolic signature to reflect healthy lifestyle.
- A healthy lifestyle-related metabolic signature could potentially reduce the risk of CVD.
- Healthy lifestyle–CVD association could be mediated by the metabolic signature, and its proportion was 20%.
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Construction of the Healthy Lifestyle Score
2.3. Assessment of CVD and Follow-Up
2.4. Assessment of Covariates
2.5. Measurement of Metabolic Biomarkers
2.6. Genotyping and Imputation
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
3.2. Identification of the Metabolic Signature Related to Healthy Lifestyle
3.3. Associations of Healthy Lifestyle with the Risk of CVD
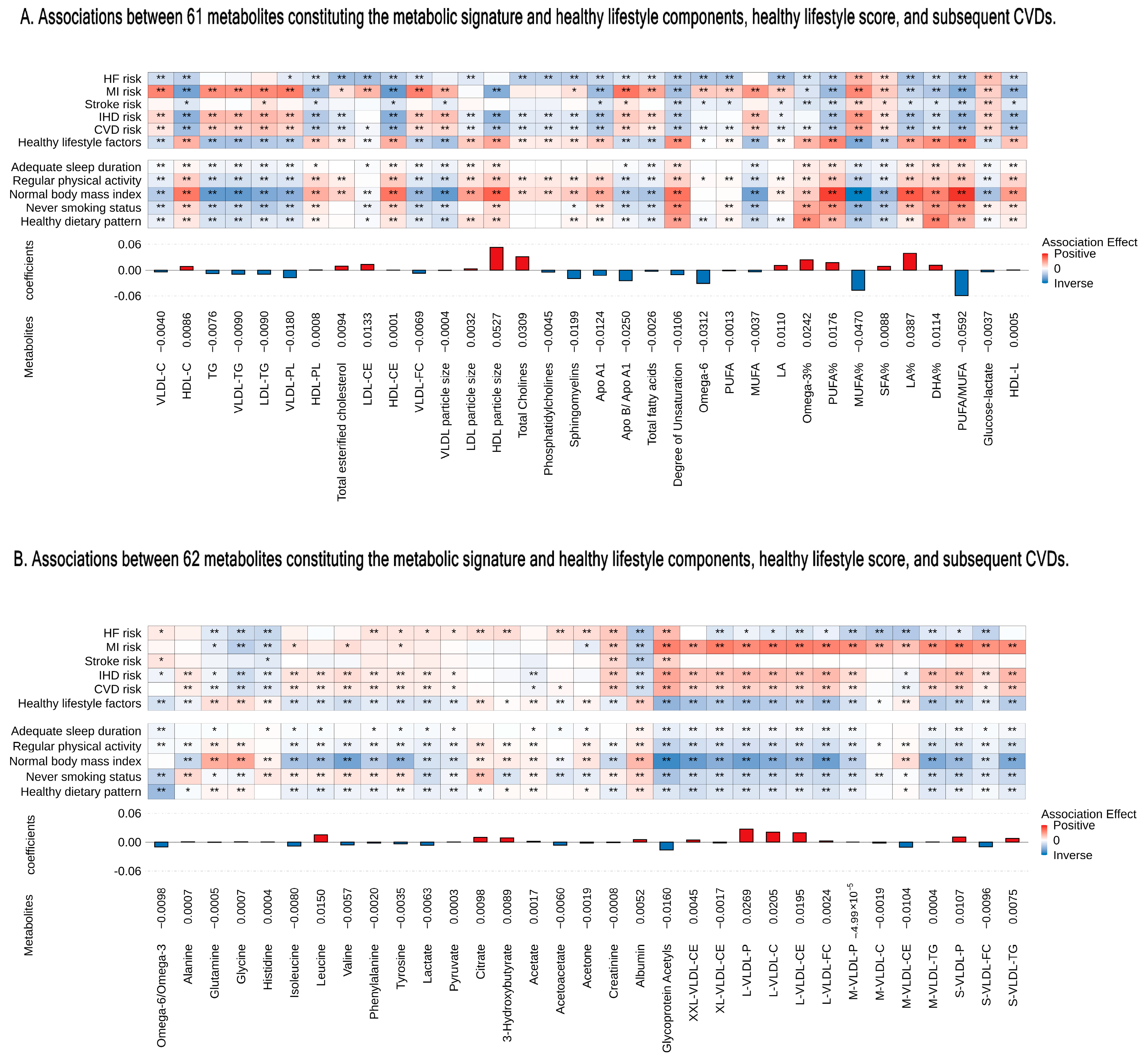
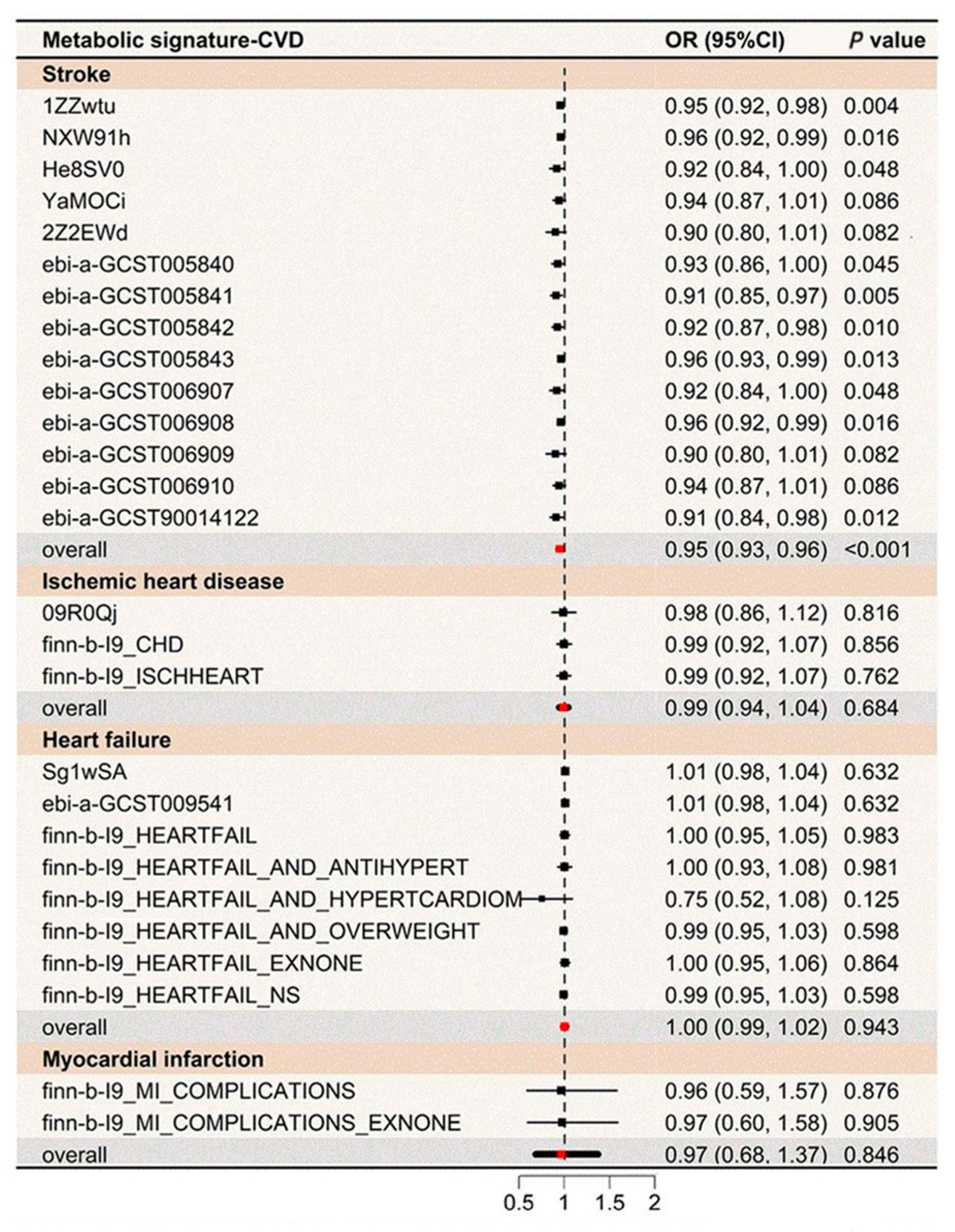
3.4. Associations of the Metabolites, Metabolic Signature, and Metabolic Pathways with the Risk of CVD
3.5. Sensitivity Analysis
4. Discussion
4.1. Overview of Results
4.2. Comparison with Previous Literature
4.3. Strengths and Limitations
4.4. Implications for Public Health
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Zwack, C.C.; Haghani, M.; Hollings, M.; Zhang, L.; Gauci, S.; Gallagher, R.; Redfern, J. The evolution of digital health technologies in cardiovascular disease research. NPJ Digit. Med. 2023, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Miedema, M.D.; Petrone, A.; Shikany, J.M.; Greenland, P.; Lewis, C.E.; Pletcher, M.J.; Gaziano, J.M.; Djousse, L. Association of Fruit and Vegetable Consumption During Early Adulthood With the Prevalence of Coronary Artery Calcium After 20 Years of Follow-Up: The Coronary Artery Risk Development in Young Adults (CARDIA) Study. Circulation 2015, 132, 1990–1998. [Google Scholar] [CrossRef] [PubMed]
- Grueter, C.E. Mediator complex dependent regulation of cardiac development and disease. Genom. Proteom. Bioinform. 2013, 11, 151–157. [Google Scholar] [CrossRef]
- Fan, M.; Sun, D.; Zhou, T.; Heianza, Y.; Lv, J.; Li, L.; Qi, L. Sleep patterns, genetic susceptibility, and incident cardiovascular disease: A prospective study of 385 292 UK biobank participants. Eur. Heart J. 2020, 41, 1182–1189. [Google Scholar] [CrossRef]
- Chudasama, Y.V.; Khunti, K.; Gillies, C.L.; Dhalwani, N.N.; Davies, M.J.; Yates, T.; Zaccardi, F. Healthy lifestyle and life expectancy in people with multimorbidity in the UK Biobank: A longitudinal cohort study. PLoS Med. 2020, 17, e1003332. [Google Scholar] [CrossRef]
- Seow, W.J.; Shu, X.O.; Nicholson, J.K.; Holmes, E.; Walker, D.I.; Hu, W.; Cai, Q.; Gao, Y.T.; Xiang, Y.B.; Moore, S.C.; et al. Association of Untargeted Urinary Metabolomics and Lung Cancer Risk Among Never-Smoking Women in China. JAMA Netw. Open 2019, 2, e1911970. [Google Scholar] [CrossRef]
- Zhang, J.; Fang, X.Y.; Leng, R.; Chen, H.F.; Qian, T.T.; Cai, Y.Y.; Zhang, X.H.; Wang, Y.Y.; Mu, M.; Tao, X.R.; et al. Metabolic Signature of Healthy Lifestyle and Risk of Rheumatoid Arthritis: Observational and Mendelian Randomization Study. Am. J. Clin. Nutr. 2023, 118, 183–193. [Google Scholar] [CrossRef]
- Tian, F.; Wang, Y.; Qian, Z.; Ran, S.; Zhang, Z.; Wang, C.; McMillin, S.E.; Chavan, N.R.; Lin, H. Plasma metabolomic signature of healthy lifestyle, structural brain reserve and risk of dementia. Brain 2024, awae257. [Google Scholar] [CrossRef]
- Rout, M.; Vaughan, A.; Blair, A.; Stavrakis, S.; Sidorov, E.V.; Sanghera, D.K. Discovery and validation of circulating stroke metabolites by NMR-based analyses using patients from the MISS and UK Biobank. Neurochem. Int. 2023, 169, 105588. [Google Scholar] [CrossRef]
- Delgado-Velandia, M.; Gonzalez-Marrachelli, V.; Domingo-Relloso, A.; Galvez-Fernandez, M.; Grau-Perez, M.; Olmedo, P.; Galan, I.; Rodriguez-Artalejo, F.; Amigo, N.; Briongos-Figuero, L.; et al. Healthy lifestyle, metabolomics and incident type 2 diabetes in a population-based cohort from Spain. Int. J. Behav. Nutr. Phys. Act. 2022, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Si, J.; Li, J.; Yu, C.; Guo, Y.; Bian, Z.; Millwood, I.; Yang, L.; Walters, R.; Chen, Y.; Du, H.; et al. Improved lipidomic profile mediates the effects of adherence to healthy lifestyles on coronary heart disease. eLife 2021, 10, e60999. [Google Scholar] [CrossRef] [PubMed]
- Aleksandrova, K.; Koelman, L.; Rodrigues, C.E. Dietary patterns and biomarkers of oxidative stress and inflammation: A systematic review of observational and intervention studies. Redox Biol. 2021, 42, 101869. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Butterworth, A.S.; Burgess, S. Mendelian randomization for cardiovascular diseases: Principles and applications. Eur. Heart J. 2023, 44, 4913–4924. [Google Scholar] [CrossRef]
- Rutten-Jacobs, L.C.; Larsson, S.C.; Malik, R.; Rannikmae, K.; MEGASTROKE Consortium; International Stroke Genetics Consortium; Sudlow, C.L.; Dichgans, M.; Markus, H.S.; Traylor, M. Genetic risk, incident stroke, and the benefits of adhering to a healthy lifestyle: Cohort study of 306 473 UK Biobank participants. BMJ 2018, 363, k4168. [Google Scholar] [CrossRef]
- Embling, R.; Price, M.J.; Lee, M.D.; Jones, A.; Wilkinson, L.L. Associations between dietary variety, portion size and body weight: Prospective evidence from UK Biobank participants. Br. J. Nutr. 2023, 130, 1267–1277. [Google Scholar] [CrossRef]
- Stolicyn, A.; Lyall, L.M.; Lyall, D.M.; Høier, N.; Adams, M.J.; Shen, X.; Cole, J.H.; McIntosh, A.M.; Whalley, H.C.; Smith, D.J. Comprehensive Assessment of Sleep Duration, Insomnia and Brain Structure within the UK Biobank Cohort. Sleep 2023, 47, zsad274. [Google Scholar] [CrossRef]
- Caleyachetty, R.; Littlejohns, T.; Lacey, B.; Bešević, J.; Conroy, M.; Collins, R.; Allen, N. United Kingdom Biobank (UK Biobank): JACC Focus Seminar 6/8. J. Am. Coll. Cardiol. 2021, 78, 56–65. [Google Scholar] [CrossRef]
- Fry, A.; Littlejohns, T.J.; Sudlow, C.; Doherty, N.; Adamska, L.; Sprosen, T.; Collins, R.; Allen, N.E. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants With Those of the General Population. Am. J. Epidemiol. 2017, 186, 1026–1034. [Google Scholar] [CrossRef]
- Ye, J.; Wen, Y.; Sun, X.; Chu, X.; Li, P.; Cheng, B.; Cheng, S.; Liu, L.; Zhang, L.; Ma, M.; et al. Socioeconomic Deprivation Index Is Associated With Psychiatric Disorders: An Observational and Genome-wide Gene-by-Environment Interaction Analysis in the UK Biobank Cohort. Biol. Psychiatry 2021, 89, 888–895. [Google Scholar] [CrossRef]
- Smith, C.J.; Sinnott-Armstrong, N.; Cichońska, A.; Julkunen, H.; Fauman, E.B.; Würtz, P.; Pritchard, J.K. Integrative analysis of metabolite GWAS illuminates the molecular basis of pleiotropy and genetic correlation. eLife 2022, 11, e79348. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Guasch-Ferre, M.; Chung, W.; Ruiz-Canela, M.; Toledo, E.; Corella, D.; Bhupathiraju, S.N.; Tobias, D.K.; Tabung, F.K.; Hu, J.; et al. The Mediterranean diet, plasma metabolome, and cardiovascular disease risk. Eur. Heart J. 2020, 41, 2645–2656. [Google Scholar] [CrossRef] [PubMed]
- Julkunen, H.; Cichońska, A.; Slagboom, P.E.; Würtz, P. Metabolic biomarker profiling for identification of susceptibility to severe pneumonia and COVID-19 in the general population. eLife 2021, 10, e63033. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Z.; Dong, X.; Jia, J.; Liu, Z.; Huang, T.; Qi, L. Sleep patterns, plasma metabolome and risk of incident type 2 diabetes. J. Clin. Endocrinol. Metab. 2023, 108, e1034–e1043. [Google Scholar] [CrossRef]
- Engebretsen, S.; Bohlin, J. Statistical predictions with glmnet. Clin. Epigenet. 2019, 11, 123. [Google Scholar] [CrossRef]
- Ko, N.Y.; Hong, S.; Winn, R.A.; Calip, G.S. Association of Insurance Status and Racial Disparities With the Detection of Early-Stage Breast Cancer. JAMA Oncol. 2020, 6, 385–392. [Google Scholar] [CrossRef]
- Gormley, M.; Dudding, T.; Kachuri, L.; Burrows, K.; Chong, A.H.W.; Martin, R.M.; Thomas, S.J.; Tyrrell, J.; Ness, A.R.; Brennan, P.; et al. Investigating the effect of sexual behaviour on oropharyngeal cancer risk: A methodological assessment of Mendelian randomization. BMC Med. 2022, 20, 40. [Google Scholar] [CrossRef]
- Miller, I.J.; Peters, S.R.; Overmyer, K.A.; Paulson, B.R.; Westphall, M.S.; Coon, J.J. Real-time health monitoring through urine metabolomics. NPJ Digit. Med. 2019, 2, 109. [Google Scholar] [CrossRef]
- Pang, Y.; Kartsonaki, C.; Turnbull, I.; Guo, Y.; Yang, L.; Bian, Z.; Chen, Y.; Millwood, I.Y.; Bragg, F.; Gong, W.; et al. Metabolic and lifestyle risk factors for acute pancreatitis in Chinese adults: A prospective cohort study of 0.5 million people. PLoS Med. 2018, 15, e1002618. [Google Scholar] [CrossRef]
- Shah, R.V.; Steffen, L.M.; Nayor, M.; Reis, J.P.; Jacobs, D.R.; Allen, N.B.; Lloyd-Jones, D.; Meyer, K.; Cole, J.; Piaggi, P.; et al. Dietary metabolic signatures and cardiometabolic risk. Eur. Heart J. 2023, 44, 557–569. [Google Scholar] [CrossRef]
- Lu, Q.; Chen, J.; Li, R.; Wang, Y.; Tu, Z.; Geng, T.; Liu, L.; Pan, A.; Liu, G. Healthy lifestyle, plasma metabolites, and risk of cardiovascular disease among individuals with diabetes. Atherosclerosis 2023, 367, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Rios, S.; García-Gavilán, J.F.; Babio, N.; Paz-Graniel, I.; Ruiz-Canela, M.; Liang, L.; Clish, C.B.; Toledo, E.; Corella, D.; Estruch, R.; et al. Plasma metabolite profiles associated with the World Cancer Research Fund/American Institute for Cancer Research lifestyle score and future risk of cardiovascular disease and type 2 diabetes. Cardiovasc. Diabetol. 2023, 22, 252. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.B.; Chen, C.; Pan, X.F.; Guo, J.; Li, Y.; Franco, O.H.; Liu, G.; Pan, A. Associations of healthy lifestyle and socioeconomic status with mortality and incident cardiovascular disease: Two prospective cohort studies. BMJ 2021, 373, n604. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Chu, M.; Fu, Z.; Liu, Q.; Liang, J.; Xu, J.; Weng, Z.; Chen, X.; Xu, C.; Gu, A. The Association of Metabolomic Profiles of a Healthy Lifestyle with Heart Failure Risk in a Prospective Study. Nutrients 2023, 15, 2934. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Colaco, K.; Lee, K.A.; Akhtari, S.; Winer, R.; Welsh, P.; Sattar, N.; McInnes, I.B.; Chandran, V.; Harvey, P.; Cook, R.J.; et al. Targeted metabolomic profiling and prediction of cardiovascular events: A prospective study of patients with psoriatic arthritis and psoriasis. Ann. Rheum. Dis. 2021, 80, 1429–1435. [Google Scholar] [CrossRef]
- Fu, Z.; Liu, Q.; Liang, J.; Weng, Z.; Li, W.; Xu, J.; Zhang, X.; Xu, C.; Gu, A. Association between NMR metabolomic signatures of healthy lifestyle and incident coronary artery disease. Eur. J. Prev. Cardiol. 2023, 30, 243–253. [Google Scholar] [CrossRef]
- Varga, T.V.; Kurbasic, A.; Aine, M.; Eriksson, P.; Ali, A.; Hindy, G.; Gustafsson, S.; Luan, J.; Shungin, D.; Chen, Y.; et al. Novel genetic loci associated with long-term deterioration in blood lipid concentrations and coronary artery disease in European adults. Int. J. Epidemiol. 2017, 46, 1211–1222. [Google Scholar] [CrossRef]
- Swerdlow, D.I.; Holmes, M.V.; Kuchenbaecker, K.B.; Engmann, J.E.; Shah, T.; Sofat, R.; Guo, Y.; Chung, C.; Peasey, A.; Pfister, R.; et al. The interleukin-6 receptor as a target for prevention of coronary heart disease: A mendelian randomisation analysis. Lancet 2012, 379, 1214–1224. [Google Scholar] [CrossRef]
- Tessier, A.J.; Wang, F.; Liang, L.; Wittenbecher, C.; Haslam, D.E.; Eliassen, A.H.; Tobias, D.K.; Li, J.; Zeleznik, O.A.; Ascherio, A.; et al. Plasma metabolites of a healthy lifestyle in relation to mortality and longevity: Four prospective US cohort studies. Med 2024, 5, 224–238.e225. [Google Scholar] [CrossRef]
- Vincent, H.K.; Raiser, S.N.; Vincent, K.R. The aging musculoskeletal system and obesity-related considerations with exercise. Ageing Res. Rev. 2012, 11, 361–373. [Google Scholar] [CrossRef] [PubMed]
- Fiuza-Luces, C.; Santos-Lozano, A.; Joyner, M.; Carrera-Bastos, P.; Picazo, O.; Zugaza, J.L.; Izquierdo, M.; Ruilope, L.M.; Lucia, A. Exercise benefits in cardiovascular disease: Beyond attenuation of traditional risk factors. Nat. Rev. Cardiol. 2018, 15, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Gupta, S.; Faulkner, P.; Mullens, D.; Thomas, M.; Sytha, S.P.; Ivanov, I.; Cai, J.J.; Heaps, C.L.; Newell-Fugate, A.E. Single-nucleus transcriptomics of epicardial adipose tissue from female pigs reveals effects of exercise training on resident innate and adaptive immune cells. Cell Commun. Signal 2024, 22, 243. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed. Pharmacother. 2002, 56, 365–379. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (n = 161,018) | Incident CVD (n = 17,030) | No CVD (n = 143,988) | p-Value * |
|---|---|---|---|---|
| Age, years | 56.00 (8.02) | 60.23 (6.88) | 55.50 (8.00) | <0.001 |
| Male | 74,885 (46.51) | 10,469 (61.47) | 64,416 (44.74) | <0.001 |
| Townsend deprivation index | −1.66 (2.89) | −1.41 (3.03) | −1.69 (2.87) | <0.001 |
| Education level | <0.001 | |||
| Any school degree | 62,998 (39.12) | 6072 (35.65) | 56,926 (39.54) | |
| College education | 58,263 (36.18) | 4727 (27.76) | 53,536 (37.18) | |
| Other education | 29,632 (18.40) | 4794 (28.15) | 24,838 (17.25) | |
| Vocational qualification | 10,125 (6.29) | 1437 (8.44) | 8688 (6.03) | |
| Metabolic signature score | 0.62 (7.16) | −1.62 (7.37) | 0.88 (7.09) | <0.001 |
| Metabolic signature level | <0.001 | |||
| Unfavorable | 49,589 (30.80) | 7324 (43.01) | 42,265 (29.35) | |
| Moderate | 54,716 (33.98) | 5451 (32.01) | 49,265 (34.21) | |
| Favorable | 56,713 (35.22) | 4255 (24.99) | 52,458 (36.43) | |
| Healthy lifestyle score | 3.76 (1.02) | 3.55 (1.09) | 3.78 (1.01) | <0.001 |
| Healthy lifestyle components | ||||
| Healthy diet | 131,573 (81.71) | 13,527 (81.15) | 118,046 (83.14) | <0.001 |
| No current smokers | 145,564 (90.40) | 14,811 (86.97) | 130,753 (90.81) | <0.001 |
| Body mass index < 30 kg/m2 | 123,265 (76.75) | 11,524 (67.95) | 111,741 (77.79) | <0.001 |
| Regular physical activity | 85,429 (53.06) | 8662 (50.86) | 76,767 (53.31) | <0.001 |
| Adequate sleep duration | 118,796 (75.81) | 11,875 (72.30) | 106,921 (76.22) | <0.001 |
| Prevalent depression status | 5161 (3.21) | 531 (3.12) | 4630 (3.22) | 0.509 |
| Traditional risk factors | ||||
| Obesity | 37,345 (23.25) | 5436 (32.05) | 31,909 (22.21) | <0.001 |
| Hypertension | 109,887 (68.25) | 14,262 (83.75) | 95,625 (66.41) | <0.001 |
| Diabetes | 6589 (4.09) | 1597 (9.38) | 4992 (3.47) | <0.001 |
| Dyslipidemia | 20,823 (12.93) | 4422 (25.97) | 16,401 (11.39) | <0.001 |
| Analysis Model | No. of Events | Healthy Lifestyle Score * | Metabolic Signature † | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| CVD | |||||
| Age- and sex-adjusted model | 17,030 | 0.79 (0.78, 0.80) | <0.001 | 0.78 (0.76, 0.79) | <0.001 |
| Multivariable-adjusted model ‡ | 17,030 | 0.81 (0.80, 0.83) | <0.001 | 0.79 (0.78, 0.81) | <0.001 |
| Multivariable-adjusted + mutual adjustment § | 17,030 | 0.85 (0.84, 0.86) | <0.001 | 0.83 (0.81, 0.84) | <0.001 |
| IHD | |||||
| Age- and sex-adjusted model | 12,599 | 0.80 (0.78, 0.81) | <0.001 | 0.78 (0.76, 0.79) | <0.001 |
| Multivariable-adjusted model ‡ | 12,599 | 0.82 (0.81, 0.83) | <0.001 | 0.80 (0.78, 0.81) | <0.001 |
| Multivariable-adjusted + mutual adjustment § | 12,599 | 0.85 (0.84, 0.87) | <0.001 | 0.83 (0.81, 0.84) | <0.001 |
| Stroke | |||||
| Age- and sex-adjusted model | 2898 | 0.84 (0.81, 0.87) | <0.001 | 0.82 (0.79, 0.85) | <0.001 |
| Multivariable-adjusted model ‡ | 2898 | 0.86 (0.83, 0.89) | <0.001 | 0.84 (0.81, 0.87) | <0.001 |
| Multivariable-adjusted + mutual adjustment § | 2898 | 0.89 (0.86, 0.92) | <0.001 | 0.86 (0.83, 0.90) | <0.001 |
| MI | |||||
| Age- and sex-adjusted model | 2391 | 0.79 (0.76, 0.82) | <0.001 | 0.80 (0.76, 0.83) | <0.001 |
| Multivariable-adjusted model ‡ | 2391 | 0.81 (0.78, 0.84) | <0.001 | 0.82 (0.78, 0.85) | <0.001 |
| Multivariable-adjusted + mutual adjustment § | 2391 | 0.84 (0.81, 0.87) | <0.001 | 0.86 (0.82, 0.89) | <0.001 |
| HF | |||||
| Age- and sex-adjusted model | 4281 | 0.70 (0.68, 0.72) | <0.001 | 0.68 (0.66, 0.70) | <0.001 |
| Multivariable-adjusted model ‡ | 4281 | 0.73 (0.71, 0.75) | <0.001 | 0.70 (0.68, 0.72) | <0.001 |
| Multivariable-adjusted + mutual adjustment § | 4281 | 0.78 (0.76, 0.80) | <0.001 | 0.75 (0.72, 0.77) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Tian, F.; Qian, Z.; Ran, S.; Zhang, J.; Wang, C.; Chen, L.; Zheng, D.; Vaughn, M.G.; Tabet, M.; et al. Healthy Lifestyle, Metabolic Signature, and Risk of Cardiovascular Diseases: A Population-Based Study. Nutrients 2024, 16, 3553. https://doi.org/10.3390/nu16203553
Wang Y, Tian F, Qian Z, Ran S, Zhang J, Wang C, Chen L, Zheng D, Vaughn MG, Tabet M, et al. Healthy Lifestyle, Metabolic Signature, and Risk of Cardiovascular Diseases: A Population-Based Study. Nutrients. 2024; 16(20):3553. https://doi.org/10.3390/nu16203553
Chicago/Turabian StyleWang, Yuhua, Fei Tian, Zhengmin (Min) Qian, Shanshan Ran, Jingyi Zhang, Chongjian Wang, Lan Chen, Dashan Zheng, Michael G. Vaughn, Maya Tabet, and et al. 2024. "Healthy Lifestyle, Metabolic Signature, and Risk of Cardiovascular Diseases: A Population-Based Study" Nutrients 16, no. 20: 3553. https://doi.org/10.3390/nu16203553
APA StyleWang, Y., Tian, F., Qian, Z., Ran, S., Zhang, J., Wang, C., Chen, L., Zheng, D., Vaughn, M. G., Tabet, M., & Lin, H. (2024). Healthy Lifestyle, Metabolic Signature, and Risk of Cardiovascular Diseases: A Population-Based Study. Nutrients, 16(20), 3553. https://doi.org/10.3390/nu16203553