

Impact of Vitamin D on Osseointegration in Dental Implants: A Systematic Review of Human Studies

Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria and Definitions
2.3. Data Collection Process
2.4. Quality Assessment
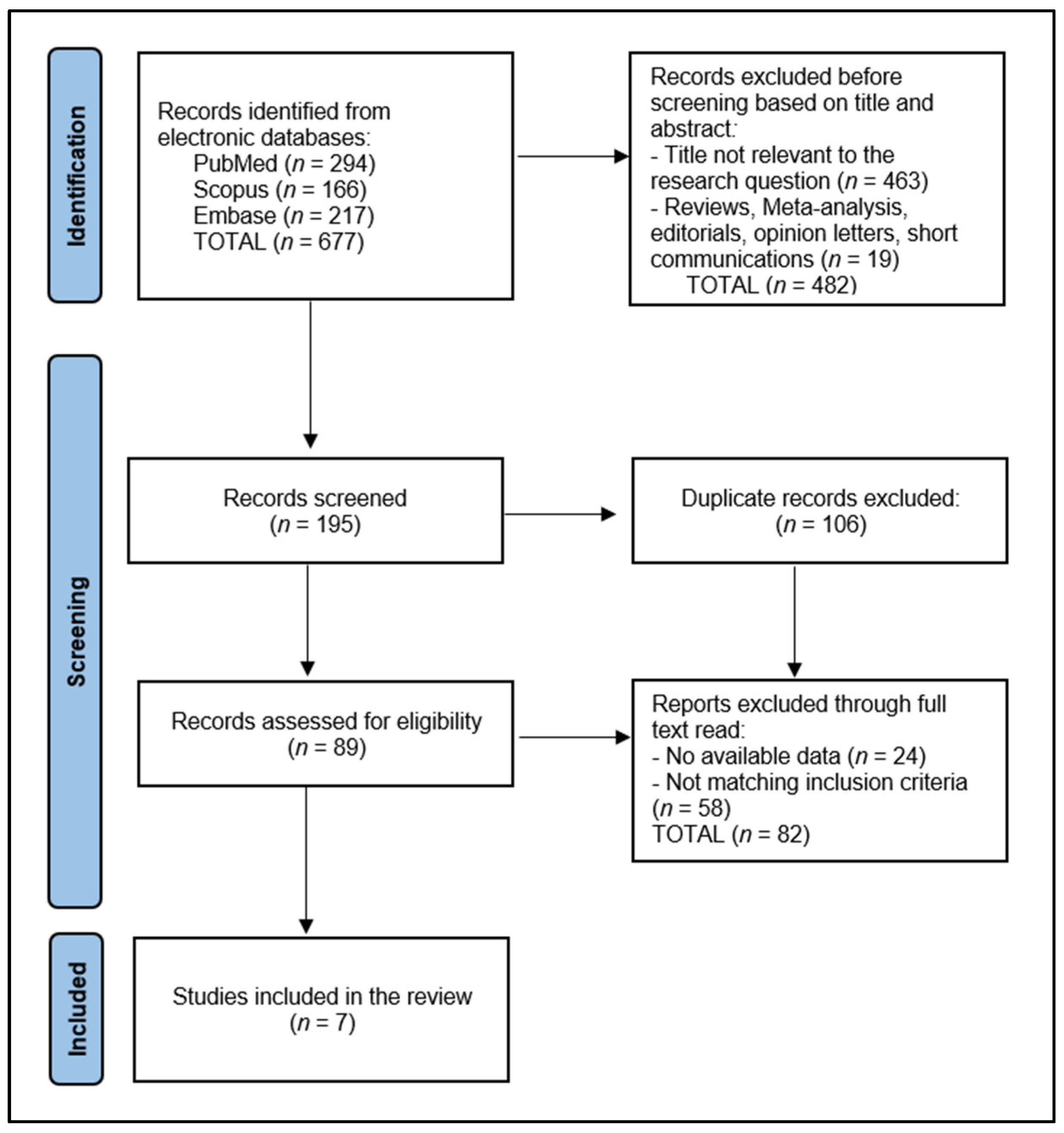
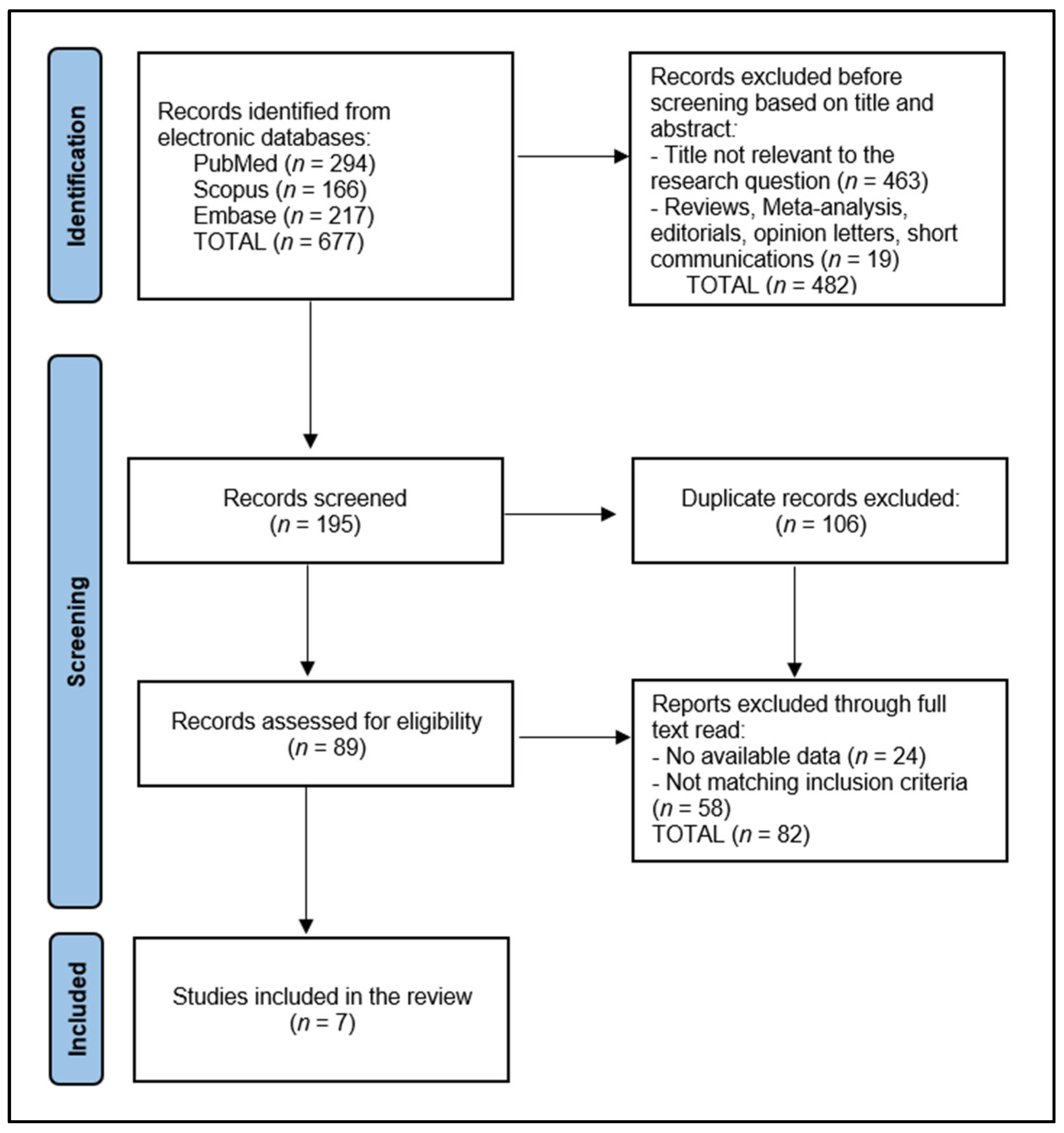
3. Results
3.1. Study Characteristics
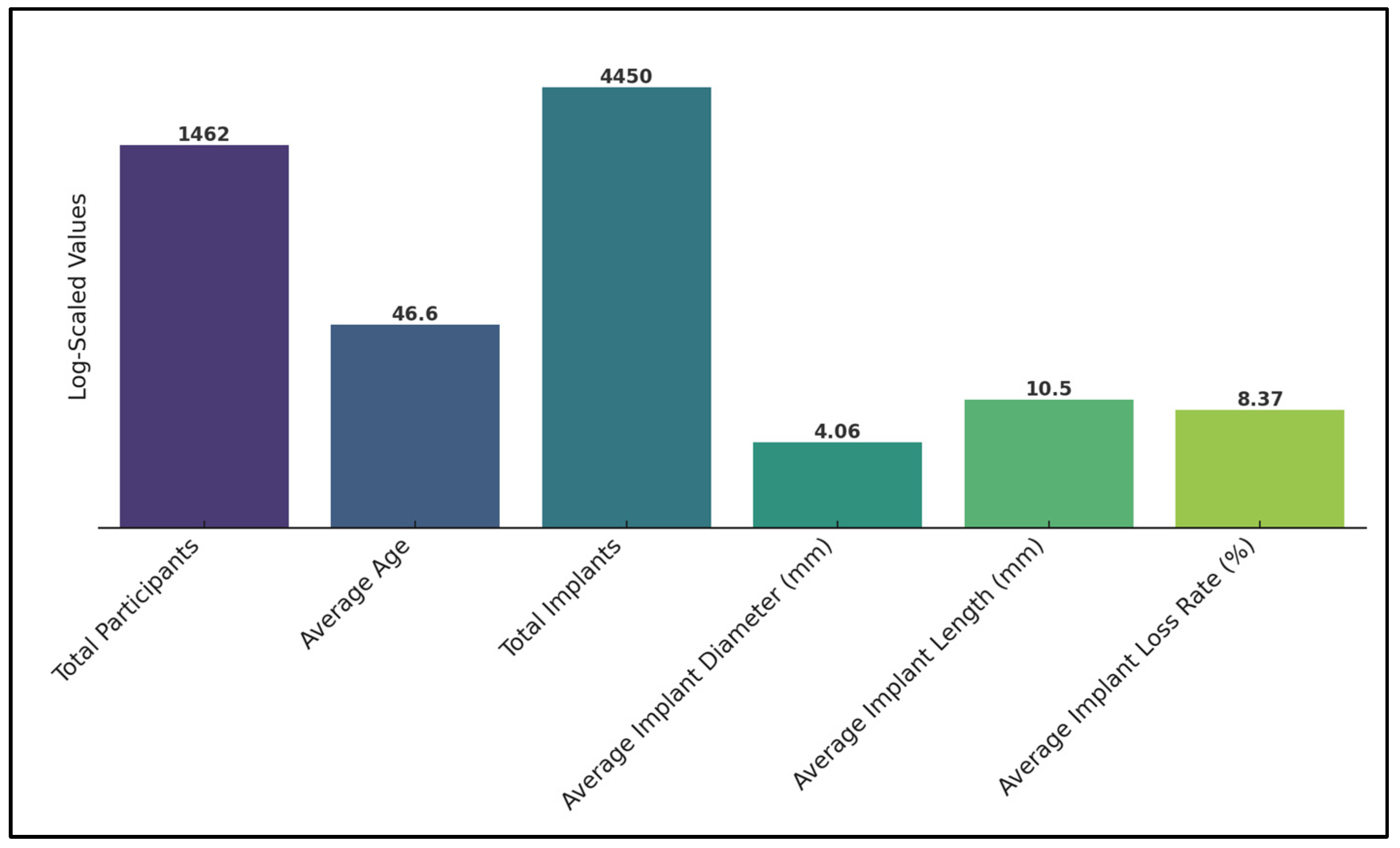
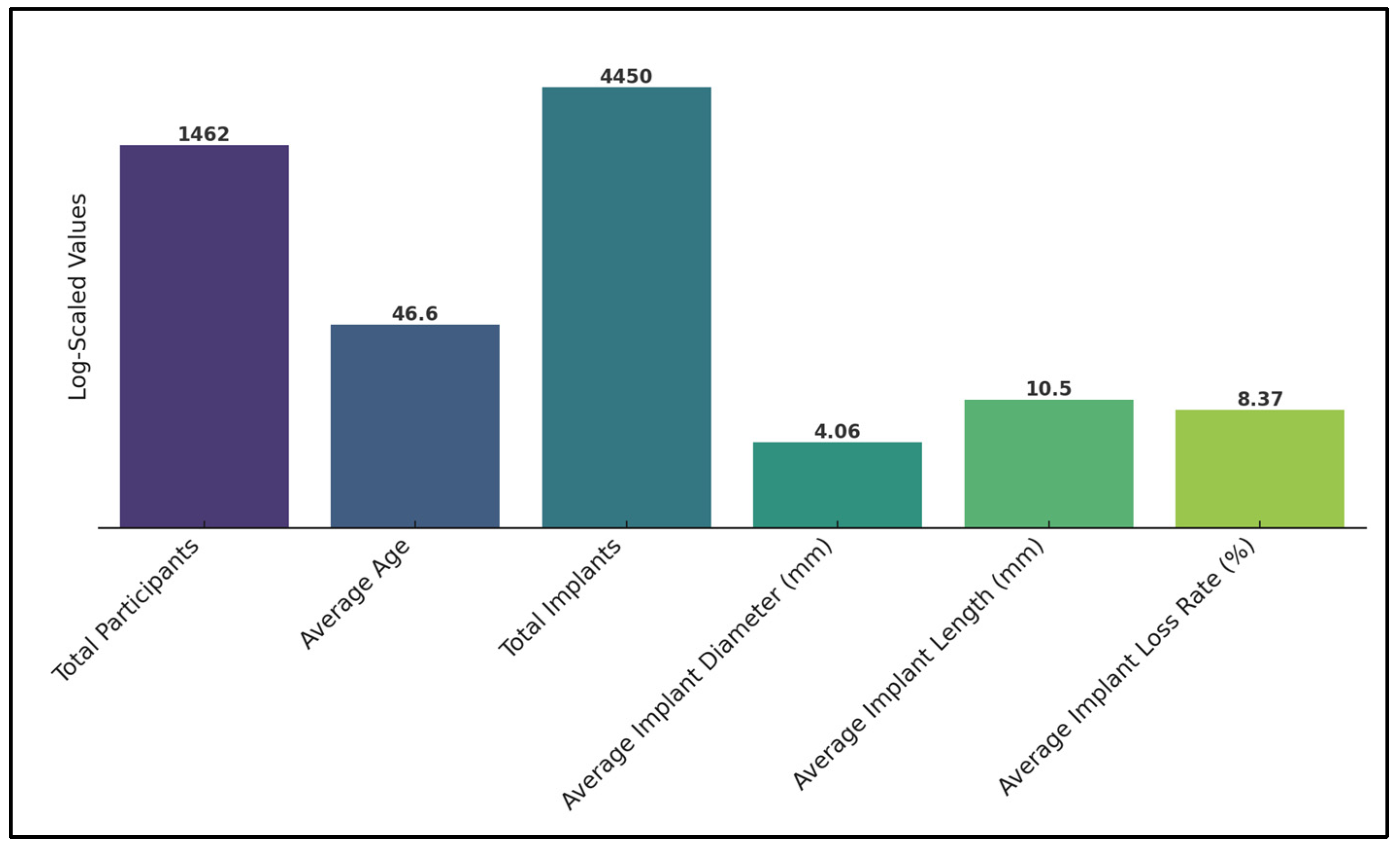
3.2. Participants’ Characteristics
3.3. Implant Assessment
3.4. Outcomes
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Levin, L.; Pathael, S.; Dolev, E.; Schwartz-Arad, D. Aesthetic versus surgical success of single dental implants: 1- to 9-year follow-up. Pract. Proced. Aesthet. Dent. 2005, 17, 533–538; quiz 540, 566. [Google Scholar] [PubMed]
- Forna, N.; Agop-Forna, D. Esthetic aspects in implant-prosthetic rehabilitation. Med. Pharm. Rep. 2019, 92 (Suppl. S3), S6–S13. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Kim, J.; Jeong, S.C.; Kim, M.; Kim, C.; Park, D. Stress Distribution Analysis of Threaded Implants for Digital Dentistry. Int. J. Environ. Res. Public Health 2022, 19, 12674. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, H.S.; Jansen, J.A. The development and future of dental implants. Dent. Mater. J. 2020, 39, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Elani, H.W.; Starr, J.R.; Da Silva, J.D.; Gallucci, G.O. Trends in Dental Implant Use in the U.S., 1999–2016, and Projections to 2026. J. Dent. Res. 2018, 97, 1424–1430. [Google Scholar] [CrossRef]
- Srinivasan, M.; Meyer, S.; Mombelli, A.; Müller, F. Dental implants in the elderly population: A systematic review and meta-analysis. Clin. Oral. Implants Res. 2017, 28, 920–930. [Google Scholar] [CrossRef] [PubMed]
- Raikar, S.; Talukdar, P.; Kumari, S.; Panda, S.K.; Oommen, V.M.; Prasad, A. Factors Affecting the Survival Rate of Dental Implants: A Retrospective Study. J. Int. Soc. Prev. Community Dent. 2017, 7, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Beschnidt, S.M.; Cacaci, C.; Dedeoglu, K.; Hildebrand, D.; Hulla, H.; Iglhaut, G.; Krennmair, G.; Schlee, M.; Sipos, P.; Stricker, A.; et al. Implant success and survival rates in daily dental practice: 5-year results of a non-interventional study using CAMLOG SCREW-LINE implants with or without platform-switching abutments. Int. J. Implant. Dent. 2018, 4, 33. [Google Scholar] [CrossRef]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef]
- Kochar, S.P.; Reche, A.; Paul, P. The Etiology and Management of Dental Implant Failure: A Review. Cureus 2022, 14, e30455. [Google Scholar] [CrossRef]
- Do, T.A.; Le, H.S.; Shen, Y.W.; Huang, H.L.; Fuh, L.J. Risk Factors related to Late Failure of Dental Implant-A Systematic Review of Recent Studies. Int. J. Environ. Res. Public Health 2020, 17, 3931. [Google Scholar] [CrossRef] [PubMed]
- Pandey, C.; Rokaya, D.; Bhattarai, B.P. Contemporary Concepts in Osseointegration of Dental Implants: A Review. Biomed. Res. Int. 2022, 2022, 6170452. [Google Scholar] [CrossRef] [PubMed]
- Nastri, L.; Moretti, A.; Migliaccio, S.; Paoletta, M.; Annunziata, M.; Liguori, S.; Toro, G.; Bianco, M.; Cecoro, G.; Guida, L.; et al. Do Dietary Supplements and Nutraceuticals Have Effects on Dental Implant Osseointegration? A Scoping Review. Nutrients 2020, 12, 268. [Google Scholar] [CrossRef] [PubMed]
- Muresan, G.C.; Hedesiu, M.; Lucaciu, O.; Boca, S.; Petrescu, N. Effect of Vitamin D on Bone Regeneration: A Review. Medicina 2022, 58, 1337. [Google Scholar] [CrossRef] [PubMed]
- Sundar, R.; Bhagavandas Rai, A.; Naveen Kumar, J.; Devang Divakar, D. The role of Vitamin D as an adjunct for bone regeneration: A systematic review of literature. Saudi Dent. J. 2023, 35, 220–232. [Google Scholar] [CrossRef]
- Kweder, H.; Eidi, H. Vitamin D deficiency in elderly: Risk factors and drugs impact on vitamin D status. Avicenna J. Med. 2018, 8, 139–146. [Google Scholar] [CrossRef]
- Werny, J.G.; Sagheb, K.; Diaz, L.; Kämmerer, P.W.; Al-Nawas, B.; Schiegnitz, E. Does vitamin D have an effect on osseointegration of dental implants? A systematic review. Int. J. Implant. Dent. 2022, 8, 16. [Google Scholar] [CrossRef]
- Schiavo, J.H. PROSPERO: An International Register of Systematic Review Protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef]
- Jayesh, R.S.; Dhinakarsamy, V. Osseointegration. J. Pharm. Bioallied Sci. 2015, 7 (Suppl. S1), S226–S229. [Google Scholar] [CrossRef]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef]
- Alvim-Pereira, F.; Montes, C.C.; Thomé, G.; Olandoski, M.; Trevilatto, P.C. Analysis of association of clinical aspects and vitamin D receptor gene polymorphism with dental implant loss. Clin. Oral Implant. Res. 2008, 19, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, D.; Mancini, M. Bimaxillary full arch fixed dental implant supported treatment for a patient with renal failure and secondary hyperparathyroidism and osteodystrophy. J. Oral Implantol. 2015, 41, e36–e43. [Google Scholar] [CrossRef]
- Bryce, G.; MacBeth, N. Vitamin D deficiency as a suspected causative factor in the failure of an immediately placed dental implant: A case report. J. R. Nav. Med. Serv. 2014, 100, 328–332. [Google Scholar] [CrossRef]
- Fretwurst, T.; Grunert, S.; Woelber, J.P.; Nelson, K.; Semper-Hogg, W. Vitamin D deficiency in early implant failure: Two case reports. Int. J. Implant. Dent. 2016, 2, 24. [Google Scholar] [CrossRef] [PubMed]
- Mangano Guido, F.; Ghertasi Oskouei, S.; Paz, A.; Mangano, N.; Mangano, C. Low serum vitamin D and early dental implant failure: Is there a connection? A retrospective clinical study on 1740 implants placed in 885 patients. J. Dent. Res. Dent. Clin. Dent. Prospects 2018, 12, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Pereira, T.M.; Alvim-Pereira, F.; Alvim-Pereira, C.C.; Ignácio, S.A.; de Souza, C.M.; Trevilatto, P.C. A complete physical mapping of the VDR gene for dental implant loss: A pilot study. Clin. Oral Implant. Res. 2019, 13529. [Google Scholar] [CrossRef]
- Kwiatek, J.; Jaroń, A.; Trybek, G. Impact of the 25-Hydroxycholecalciferol Concentration and Vitamin D Deficiency Treatment on Changes in the Bone Level at the Implant Site during the Process of Osseointegration: A Prospective, Randomized, Controlled Clinical Trial. J. Clin. Med. 2021, 10, 526. [Google Scholar] [CrossRef]
- Banjabi, A.A.; Al-Ghafari, A.B.; Kumosani, T.A.; Kannan, K.; Fallatah, S.M. Genetic influence of vitamin D receptor gene polymorphisms on osteoporosis risk. Int. J. Health Sci. 2020, 14, 22–28. [Google Scholar]
- Marozik, P.; Rudenka, A.; Kobets, K.; Rudenka, E. Vitamin D Status, Bone Mineral Density, and VDR Gene Polymorphism in a Cohort of Belarusian Postmenopausal Women. Nutrients 2021, 13, 837. [Google Scholar] [CrossRef]
- Mustapha, A.D.; Salame, Z.; Chrcanovic, B.R. Smoking and Dental Implants: A Systematic Review and Meta-Analysis. Medicina 2021, 58, 39. [Google Scholar] [CrossRef]
- Drago, C.J. Rates of osseointegration of dental implants with regard to anatomical location. J. Prosthodont. 1992, 1, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yu, T.; Yang, X.; Li, F.; Ma, L.; Yang, Y. Vitamin D3 and insulin combined treatment promotes titanium implant osseointegration in diabetes mellitus rats. Bone 2013, 52, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Li, Y.; Wang, X.; Shui, X.; Hu, J. 1,25Dihydroxy vitamin D(3) improves titanium implant osseointegration in osteoporotic rats. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114 (Suppl. S5), S174–S178. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, S.P.; Casarin, R.C.; Ribeiro, F.V.; Cirano, F.R.; Rovaris, K.; Haiter, F. Impact of micronutrients supplementation on bone repair around implants: MicroCT and counter-torque analysis in rats. J. Appl. Oral Sci. 2016, 24, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. The ongoing D-lemma of vitamin D supplementation for nonskeletal health and bone health. Curr. Opin. Endocrinol. Diab. Obes. 2019, 26, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Burt, L.A.; Billington, E.O.; Rose, M.S.; Raymond, D.A.; Hanley, D.A.; Boyd, S.K. Effect of high-dose vitamin D supplementation on volumetric bone density and bone strength: A randomized clinical trial. JAMA 2019, 322, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Akhavan, A.; Noroozi, Z.; Shafiei, A.A.; Haghighat, A.; Jahanshahi, G.R.; Mousavi, S.B. The effect of vitamin D supplementation on bone formation around titanium implants in diabetic rats. Dent. Res. J. 2012, 9, 582–587. [Google Scholar] [CrossRef]
- Nakamura, Y.; Hayashi, K.; Abu-Ali, S.; Naito, M.; Fotovati, A. Effect of preoperative combined treatment with alendronate and calcitriol on fixation of hydroxyapatite-coated implants in ovariectomized rats. J. Bone Jt. Surg. Am. 2008, 90, 824–832. [Google Scholar] [CrossRef]
- Dvorak, G.; Fügl, A.; Watzek, G.; Tangl, S.; Pokorny, P.; Gruber, R. Impact of dietary vitamin D on osseointegration in the ovariectomized rat. Clin. Oral Implant. Res. 2012, 23, 1308–1313. [Google Scholar] [CrossRef]
- Fretwurst, T.; Wölber, J.P.; Nelson, K. Vitamin D zur implantation—Ist ein Screening mit Substitution sinnvoll? Quintessenz Zahnmed. 2020, 71, 504–510. [Google Scholar]
- Shahram, G.; Karl, U.V.; Al-Maawi, S. Vitamin D als schlüsselelement für immunabwehr und regeneration. Implantol. J. 2020, 9, 16–22. [Google Scholar]

{kind=link}
{kind=link}
| Study and Author | Country | Study Year | Study Design | Quality of Evidence |
|---|---|---|---|---|
| Alvim-Pereira et al. [21] | Brazil | 2008 | Case-Control | Medium |
| Flanagan et al. [22] | USA | 2013 | Case Report | Low |
| Bryce et al. [23] | United Kingdom | 2014 | Case Report | Low |
| Fretwurst et al. [24] | Germany | 2016 | Case Series | Low |
| Mangano et al. [25] | Italy | 2018 | Retrospective Cohort | Medium |
| Pereira et al. [26] | Brazil | 2019 | Case-Control | Medium |
| Kwiatek et al. [27] | Poland | 2021 | Randomized Trial | High |
| Study Number | Number of Individuals | Study Groups | Age (Years) | Sex (Male) |
|---|---|---|---|---|
| Alvim-Pereira et al. [21] | 207 | 137 with dental implants vs. 70 without implants | 51.6 years vs. 52.8 years | 36.5% with implants vs. 40.0% without |
| Flanagan et al. [22] | 1 | NR | 34 years | 1 Male |
| Bryce et al. [23] | 1 | NR | 29 years | 1 Male |
| Fretwurst et al. [24] | 2 | NR | 48 years vs. 51 years | 2 Male |
| Mangano et al. [25] | 885 | 850 successful implants vs. 35 early failures | 57.3 years | 51.5% |
| Pereira et al. [26] | 244 | 81 with Vitamin D receptor mutation vs. 163 controls | 51.9 years | 33.6% |
| Kwiatek et al. [27] | 122 | Group 1: Vitamin D < 30 ng/mL, Group 2: Vitamin D < 30 ng/mL + supplement, Group 3: Vitamin D > 30 ng/mL | 43.8 years | 46.7% |
| Study Number | Number of Implants | Location (Mandible, Maxilla) | Implant Size (Diameter, Length) | Follow-Up |
|---|---|---|---|---|
| Alvim-Pereira et al. [21] | 1232 healthy implants, 135 lost implants | Healthy implants: 50.9% maxilla, 55.4% posterior region Lost implants: 37.5% maxilla, 64.7% posterior region | Healthy implants: diameter 3.99, length 13.16 Lost implants: diameter: 4.03, length 12.35 | 43 weeks |
| Flanagan et al. [22] | 18 | Mandible and maxilla | NR | 7 months |
| Bryce et al. [23] | 1 | Mandibular premolar | Diameter: 4.3, length 10 | 5 months |
| Fretwurst et al. [24] | 9 | Mandible | Diameter: 4.1, length 12 vs. Diameter 4.3, length 7 | NR |
| Mangano et al. [25] | 1740 | Mandible and maxilla | NR | 4 months |
| Pereira et al. [26] | 1193 | NR | NR | 250 weeks |
| Kwiatek et al. [27] | 122 | Mandible: premolars 25.8%, molars 74.2% | Diameter: 3.3–4.2, length: 8–11.5 | 6–12 weeks |
| Study Number | Vitamin D Assessment | Outcomes | Risk Factors |
|---|---|---|---|
| Alvim-Pereira et al. [21] | NR | 9.8% implant loss rate | No association between Vitamin D TaqI receptor polymorphism and implant loss. |
| Flanagan et al. [22] | Vitamin D3 supplementation, phosphate binders and calcium cinacalcet calcimimetic, 3 × dialysis/week | Successful implantation | Low serum Vitamin D levels do not pose an elevated risk for loss of dental implant if calcium levels are properly corrected in patients with IgA nephropathy. |
| Bryce et al. [23] | Severe Vitamin D deficiency | Successful implantation | Low serum Vitamin D might contribute to unsuccessful osseointegration in dental implants. |
| Fretwurst et al. [24] | Vitamin D deficiency | 22.2% implant loss rate | Successful replacement after Vitamin D supplementation |
| Mangano et al. [25] | Vitamin D deficiency in 53.7% of patients; 29.5 ng/mL vs. 25.4 ng/mL in the early failure group | 3.9% implant loss rate; 11.1% among patients with severe vitamin D deficiency | Four times higher prevalence of early implant loss with low serum Vitamin D levels; higher when associated with smoking and periodontal disease. |
| Pereira et al. [26] | Vitamin D deficiency due to receptor mutation | 11.4% implant loss rate | Vitamin D allele G of rs3782905 significantly associated with poor osseointegration. |
| Kwiatek et al. [27] | Day of surgery: 23.9 ng/mL, After 6 weeks: 30.4 ng/mL, After 12 weeks: 33.1 ng/mL | NR | Significantly higher bone density in patients with Vitamin D supplementation after 12 weeks. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buzatu, B.L.R.; Buzatu, R.; Luca, M.M. Impact of Vitamin D on Osseointegration in Dental Implants: A Systematic Review of Human Studies. Nutrients 2024, 16, 209. https://doi.org/10.3390/nu16020209
Buzatu BLR, Buzatu R, Luca MM. Impact of Vitamin D on Osseointegration in Dental Implants: A Systematic Review of Human Studies. Nutrients. 2024; 16(2):209. https://doi.org/10.3390/nu16020209
Chicago/Turabian StyleBuzatu, Berivan Laura Rebeca, Roxana Buzatu, and Magda Mihaela Luca. 2024. "Impact of Vitamin D on Osseointegration in Dental Implants: A Systematic Review of Human Studies" Nutrients 16, no. 2: 209. https://doi.org/10.3390/nu16020209
APA StyleBuzatu, B. L. R., Buzatu, R., & Luca, M. M. (2024). Impact of Vitamin D on Osseointegration in Dental Implants: A Systematic Review of Human Studies. Nutrients, 16(2), 209. https://doi.org/10.3390/nu16020209