
Efficacy of 1-Kestose Supplementation in Patients with Pancreatic Ductal Adenocarcinoma: A Randomized Controlled Pilot Study
 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Randomization and Masking
2.3. Procedures
2.4. Preparation of Fecal Samples
2.5. Analysis of the Fecal Microbiome
2.6. Bioelectrical Impedance Analysis
2.7. Statistical Analysis
3. Results
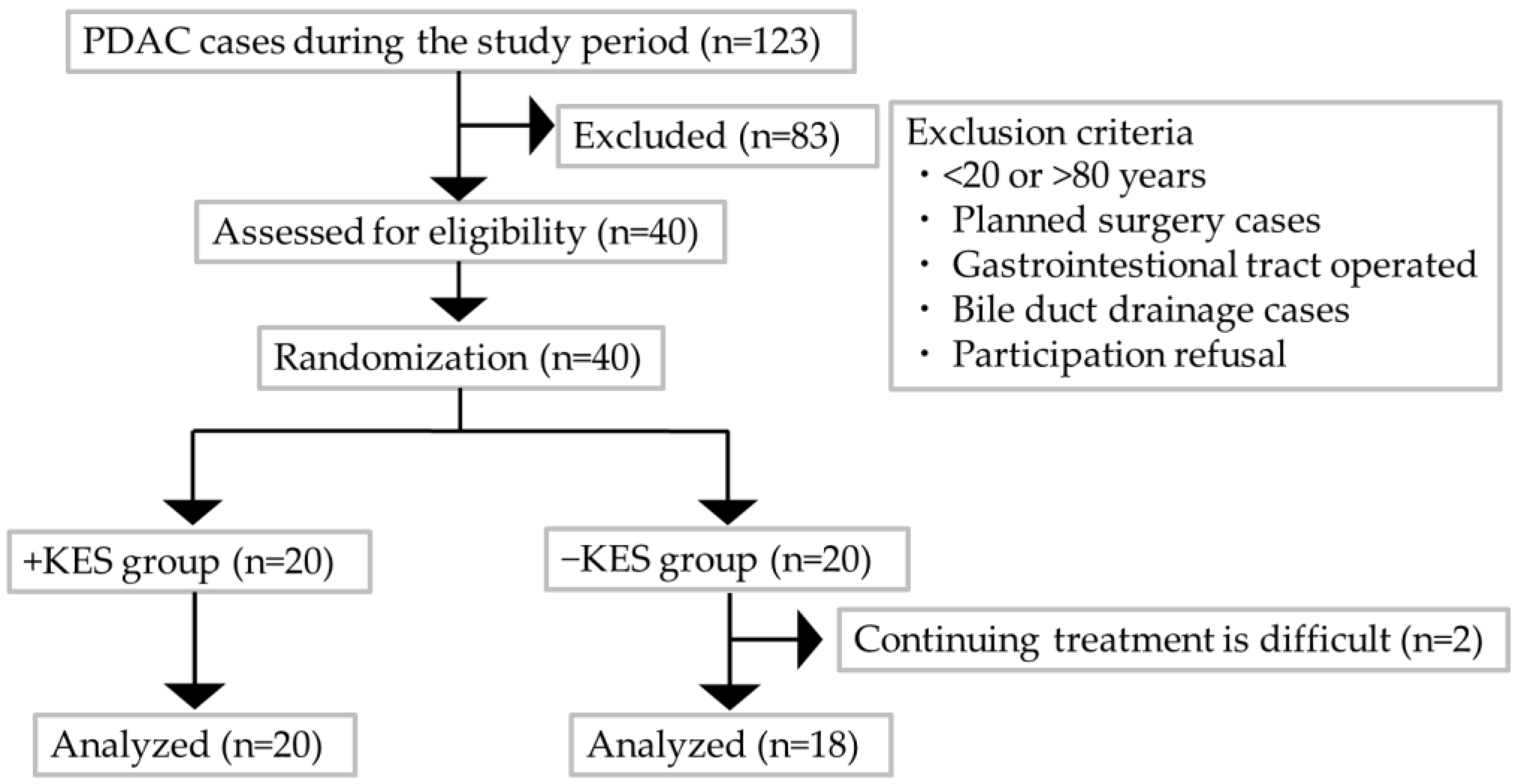
3.1. Participant Selection and Clinical Characteristics
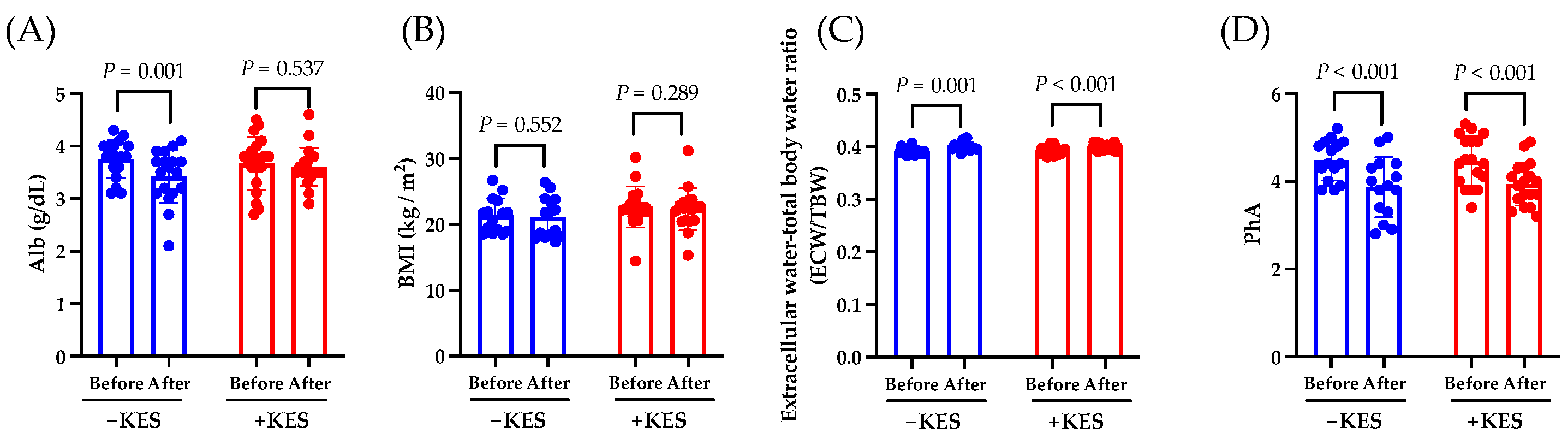
3.2. Endpoints
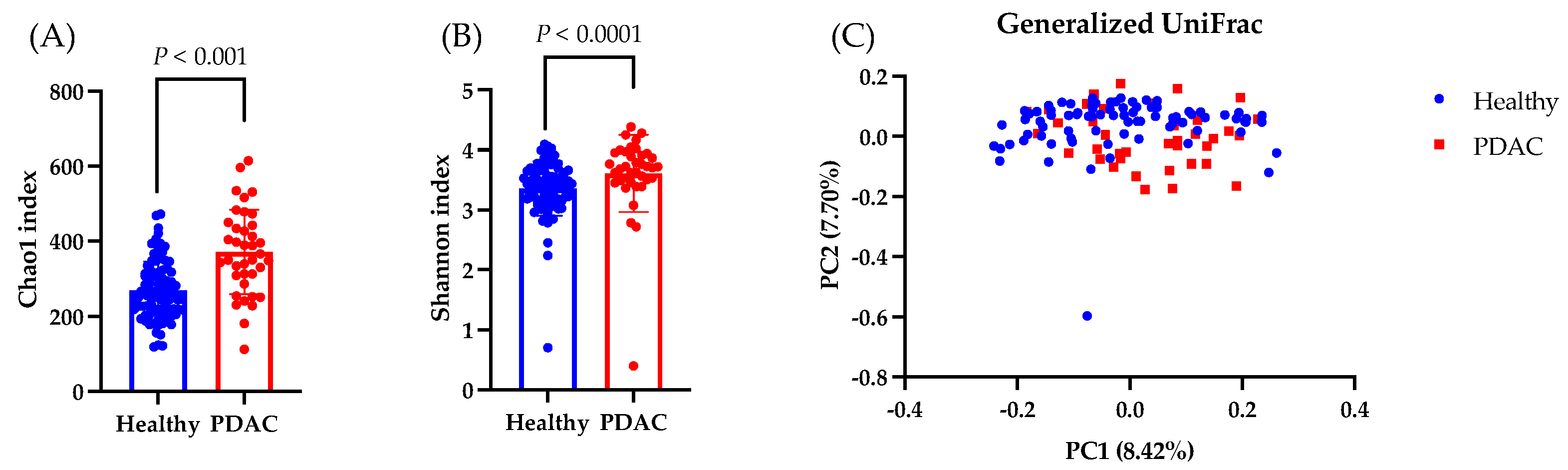
3.3. Fecal Microbiome
3.4. Safety Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collisson, E.A.; Bailey, P.; Chang, D.K.; Biankin, A.V. Molecular subtypes of pancreatic cancer. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020. [Google Scholar] [CrossRef] [PubMed]
- Kolbeinsson, H.M.; Chandana, S.; Wright, G.P.; Chung, M. Pancreatic cancer: A review of current treatment and novel therapies. J. Investig. Surg. 2023, 36, 2129884. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of pancreatic cancer: Global trends, etiology and risk factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Santos, I.; Mendes, L.; Mansinho, H.; Santos, C.A. Nutritional status and functional status of the pancreatic cancer patients and the impact of adjacent symptoms. Clin. Nutr. 2021, 40, 5486–5493. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Raghavan, S.; Winter, P.S.; Navia, A.W.; Williams, H.L.; DenAdel, A.; Lowder, K.E.; Galvez-Reyes, J.; Kalekar, R.L.; Mulugeta, N.; Kapner, K.S.; et al. Microenvironment drives cell state, plasticity, and drug response in pancreatic cancer. Cell 2021, 184, 6119–6137.e26. [Google Scholar] [CrossRef]
- Aung, K.L.; Fischer, S.E.; Denroche, R.E.; Jang, G.H.; Dodd, A.; Creighton, S.; Southwood, B.; Liang, S.B.; Chadwick, D.; Zhang, A.; et al. Genomics-driven precision medicine for advanced pancreatic cancer: Early results from the COMPASS Trial. Clin. Cancer Res. 2018, 24, 1344–1354. [Google Scholar] [CrossRef]
- Half, E.; Keren, N.; Reshef, L.; Dorfman, T.; Lachter, I.; Kluger, Y.; Reshef, N.; Knobler, H.; Maor, Y.; Stein, A.; et al. Fecal microbiome signatures of pancreatic cancer patients. Sci. Rep. 2019, 9, 16801. [Google Scholar] [CrossRef]
- Ren, Z.; Jiang, J.; Xie, H.; Li, A.; Lu, H.; Xu, S.; Zhou, L.; Zhang, H.; Cui, G.; Chen, X.; et al. Gut microbial profile analysis by MiSeq sequencing of pancreatic carcinoma patients in China. Oncotarget 2017, 8, 95176–95191. [Google Scholar] [CrossRef]
- Hashimoto, S.; Tochio, T.; Funasaka, K.; Funahashi, K.; Hartanto, T.; Togashi, Y.; Saito, M.; Nishimoto, Y.; Yoshinori, M.; Nakaoka, K.; et al. Changes in intestinal bacteria and imbalances of metabolites induced in the intestines of pancreatic ductal adenocarcinoma patients in a Japanese population: A preliminary result. Scand. J. Gastroenterol. 2023, 58, 193–198. [Google Scholar] [CrossRef]
- Smith, P.M.; Howitt, M.R.; Panikov, N.; Michaud, M.; Gallini, C.A.; Bohlooly-Y, M.; Glickman, J.N.; Garrett, W.S. The microbial metabolites, short-chain fatty acids, regulate colonic Treg cell homeostasis. Science 2013, 341, 569–573. [Google Scholar] [CrossRef]
- Carbone, D.; De Franco, M.; Pecoraro, C.; Bassani, D.; Pavan, M.; Cascioferro, S.; Parrino, B.; Cirrincione, G.; Dall’Acqua, S.; Sut, S.; et al. Structural Manipulations of Marine Natural Products Inspire a New Library of 3-Amino-1,2,4-Triazine PDK Inhibitors Endowed with Antitumor Activity in Pancreatic Ductal Adenocarcinoma. Mar. Drugs 2023, 21, 288. [Google Scholar] [CrossRef]
- Schepis, T.; De Lucia, S.S.; Pellegrino, A.; Del Gaudio, A.; Maresca, R.; Coppola, G.; Chiappetta, M.F.; Gasbarrini, A.; Franceschi, F.; Candelli, M.; et al. State-of-the-Art and Upcoming Innovations in Pancreatic Cancer Care: A Step Forward to Precision Medicine. Cancers 2023, 15, 3423. [Google Scholar] [CrossRef]
- Randazzo, O.; Papini, F.; Mantini, G.; Gregori, A.; Parrino, B.; Liu, D.S.K.; Cascioferro, S.; Carbone, D.; Peters, G.J.; Frampton, A.E.; et al. “Open Sesame?”: Biomarker Status of the Human Equilibrative Nucleoside Transporter-1 and Molecular Mechanisms Influencing its Expression and Activity in the Uptake and Cytotoxicity of Gemcitabine in Pancreatic Cancer. Cancers 2020, 12, 3206. [Google Scholar] [CrossRef] [PubMed]
- Carbone, D.; Pecoraro, C.; Panzeca, G.; Xu, G.; Roeten, M.S.F.; Cascioferro, S.; Giovannetti, E.; Diana, P.; Parrino, B. 1,3,4-Oxadiazole and 1,3,4-Thiadiazole Nortopsentin Derivatives against Pancreatic Ductal Adenocarcinoma: Synthesis, Cytotoxic Activity, and Inhibition of CDK1. Mar. Drugs 2023, 21, 412. [Google Scholar] [CrossRef] [PubMed]
- Ose, R.; Hirano, K.; Maeno, S.; Nakagawa, J.; Salminen, S.; Tochio, T.; Endo, A. The ability of human intestinal anaerobes to metabolize different oligosaccharides: Novel means for microbiota modulation. Anaerobe 2018, 51, 110–119. [Google Scholar] [CrossRef]
- Ikegami, S.; Nakamura, M.; Honda, T.; Yamamura, T.; Maeda, K.; Sawada, T.; Ishikawa, E.; Yamamoto, K.; Furune, S.; Ishikawa, T.; et al. Efficacy of 1-kestose supplementation in patients with mild to moderate ulcerative colitis: A randomised, double-blind, placebo-controlled pilot study. Aliment. Pharmacol. Ther. 2023, 57, 1249–1257. [Google Scholar] [CrossRef]
- Tominaga, K.; Tsuchiya, A.; Nakano, O.; Kuroki, Y.; Oka, K.; Minemura, A.; Matsumoto, A.; Takahashi, M.; Kadota, Y.; Tochio, T.; et al. Increase in muscle mass associated with the prebiotic effects of 1-kestose in super-elderly patients with sarcopenia. Biosci. Microbiota Food Health 2021, 40, 150–155. [Google Scholar] [CrossRef]
- Ozaka, M.; Ishii, H.; Sato, T.; Ueno, M.; Ikeda, M.; Uesugi, K.; Sata, N.; Miyashita, K.; Mizuno, N.; Tsuji, K.; et al. A phase II study of modified FOLFIRINOX for chemotherapy-naïve patients with metastatic pancreatic cancer. Cancer Chemother. Pharmacol. 2018, 81, 1017–1023. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glöckner, F.O. Evaluation of general 16S ribosomal RNA gene PCR primers for classical and next-generation sequencing-based diversity studies. Nucleic Acids Res. 2013, 41, e1. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, H.W.; Mustafa, B.; Lee, H.I.; Kwon, H.W. The relationships between microbiome diversity and epidemiology in domestic species of malaria-mediated mosquitoes of Korea. Sci. Rep. 2023, 13, 9081. [Google Scholar] [CrossRef] [PubMed]
- Capurso, G.; Pecorelli, N.; Burini, A.; Orsi, G.; Palumbo, D.; Macchini, M.; Mele, R.; de Cobelli, F.; Falconi, M.; Arcidiacono, P.G.; et al. The impact of nutritional status on pancreatic cancer therapy. Expert. Rev. Anticancer Ther. 2022, 22, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Yamada, D.; Eguchi, H.; Asaoka, T.; Tomihara, H.; Noda, T.; Wada, H.; Kawamoto, K.; Gotoh, K.; Takeda, Y.; Tanemura, M.; et al. The basal nutritional state of PDAC patients is the dominant factor for completing adjuvant chemotherapy. Surg. Today 2017, 47, 1361–1371. [Google Scholar] [CrossRef]
- Tozuka, Y.; Ueno, M.; Kobayashi, S.; Morimoto, M.; Fukushima, T.; Sano, Y.; Kawano, K.; Hanaoka, A.; Tezuka, S.; Asama, H.; et al. Prognostic significance of sarcopenia as determined by bioelectrical impedance analysis in patients with advanced pancreatic cancer receiving gemcitabine plus nab-paclitaxel: A retrospective study. Oncol. Lett. 2022, 24, 375. [Google Scholar] [CrossRef]
- Rom, H.; Tamir, S.; Van Vugt, J.L.A.; Berger, Y.; Perl, G.; Morgenstern, S.; Tovar, A.; Brenner, B.; Benchimol, D.; Kashtan, H.; et al. Sarcopenia as a predictor of survival in patients with pancreatic adenocarcinoma after pancreatectomy. Ann. Surg. Oncol. 2022, 29, 1553–1563. [Google Scholar] [CrossRef]
- Gupta, D.; Lis, C.G.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Lammersfeld, C.A. Bioelectrical impedance phase angle as a prognostic indicator in advanced pancreatic cancer. Br. J. Nutr. 2004, 92, 957–962. [Google Scholar] [CrossRef]
- Don, B.R.; Kaysen, G. Serum albumin: Relationship to inflammation and nutrition. Semin. Dial. 2004, 17, 432–437. [Google Scholar] [CrossRef]
- van Wijk, L.; de Klein, G.W.; Kanters, M.A.; Patijn, G.A.; Klaase, J.M. The ultimate preoperative C-reactive protein-to-albumin ratio is a prognostic factor for survival after pancreatic cancer resection. Eur. J. Med. Res. 2020, 25, 46. [Google Scholar] [CrossRef] [PubMed]
- Zahorec, R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl. Lek. Listy 2021, 122, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Wang, W.J.; Zhi, Q.; Shen, M.; Jiang, M.; Bian, X.; Gong, F.R.; Zhou, C.; Lian, L.; Wu, M.Y.; et al. Neutrophil/lymphocyte ratio is a more sensitive systemic inflammatory response biomarker than platelet/lymphocyte ratio in the prognosis evaluation of unresectable pancreatic cancer. Oncotarget 2017, 8, 88835–88844. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wei, Q.; Fan, J.; Cheng, S.; Ding, W.; Hua, Z. Prognostic role of the neutrophil-to-lymphocyte ratio in pancreatic cancer: A meta-analysis containing 8252 patients. Clin. Chim. Acta 2018, 479, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Li, M.X.; Liu, X.M.; Zhang, X.F.; Zhang, J.F.; Wang, W.L.; Zhu, Y.; Dong, J.; Cheng, J.W.; Liu, Z.W.; Ma, L.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in colorectal cancer: A systematic review and meta-analysis. Int. J. Cancer 2014, 134, 2403–2413. [Google Scholar] [CrossRef]
- Zhao, Q.T.; Yang, Y.; Xu, S.; Zhang, X.P.; Wang, H.E.; Zhang, H.; Wang, Z.K.; Yuan, Z.; Duan, G.C. Prognostic role of neutrophil to lymphocyte ratio in lung cancers: A meta-analysis including 7,054 patients. Onco Targets Ther. 2015, 8, 2731–2738. [Google Scholar] [CrossRef]
- Xin-Ji, Z.; Yong-Gang, L.; Xiao-Jun, S.; Xiao-Wu, C.; Dong, Z.; Da-Jian, Z. The prognostic role of neutrophils to lymphocytes ratio and platelet count in gastric cancer: A meta-analysis. Int. J. Surg. 2015, 21, 84–91. [Google Scholar] [CrossRef]
- Yodying, H.; Matsuda, A.; Miyashita, M.; Matsumoto, S.; Sakurazawa, N.; Yamada, M.; Uchida, E. Prognostic significance of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in oncologic outcomes of esophageal cancer: A systematic review and meta-analysis. Ann. Surg. Oncol. 2016, 23, 646–654. [Google Scholar] [CrossRef]
- Liu, Z.; Jin, K.; Guo, M.; Long, J.; Liu, L.; Liu, C.; Xu, J.; Ni, Q.; Luo, G.; Yu, X. Prognostic value of the CRP/Alb ratio, a novel inflammation-based score in pancreatic cancer. Ann. Surg. Oncol. 2017, 24, 561–568. [Google Scholar] [CrossRef]
- Haruki, K.; Shiba, H.; Shirai, Y.; Horiuchi, T.; Iwase, R.; Fujiwara, Y.; Furukawa, K.; Misawa, T.; Yanaga, K. The C-reactive Protein to Albumin Ratio Predicts Long-Term Outcomes in patients with pancreatic cancer after pancreatic resection. World J. Surg. 2016, 40, 2254–2260. [Google Scholar] [CrossRef]
- Al Bander, Z.; Nitert, M.D.; Mousa, A.; Naderpoor, N. The gut microbiota and inflammation: An overview. Int. J. Environ. Res. Public Health 2020, 17, 7618. [Google Scholar] [CrossRef]
- Luo, W.; Cao, Z.; Qiu, J.; Liu, Y.; Zheng, L.; Zhang, T. Novel discoveries targeting pathogenic gut microbes and new therapies in pancreatic cancer: Does pathogenic E. coli infection cause pancreatic cancer progression modulated by TUBB/Rho/ROCK signaling pathway? A bioinformatic analysis. BioMed Res. Int. 2020, 2020, 2340124. [Google Scholar] [CrossRef]
- Li, R.; Hu, Y.; Hou, S. An exploration of oral-gut pathogens mediating immune escape of pancreatic cancer via miR-21/PTEN axis. Front. Microbiol. 2022, 13, 928846. [Google Scholar] [CrossRef]
- Di Carlo, P.; Serra, N.; D’Arpa, F.; Agrusa, A.; Gulotta, G.; Fasciana, T.; Rodolico, V.; Giammanco, A.; Sergi, C. The microbiota of the bilio-pancreatic system: A cohort, STROBE-compliant study. Infect. Drug Resist. 2019, 12, 1513–1527. [Google Scholar] [CrossRef] [PubMed]
- Moshkovskaya, M.; Vakhrusheva, T.; Rakitina, D.; Baykova, J.; Panasenko, O.; Basyreva, L.; Gusev, S.; Gusev, A.; Mikhalchik, E.; Smolina, N.; et al. Neutrophil activation by Escherichia coli isolates from human intestine: Effects of bacterial hydroperoxidase activity and surface hydrophobicity. FEBS Open Bio 2020, 10, 414–426. [Google Scholar] [CrossRef] [PubMed]
- Klapproth, J.M.; Scaletsky, I.C.; McNamara, B.P.; Lai, L.C.; Malstrom, C.; James, S.P.; Donnenberg, M.S. A large toxin from pathogenic Escherichia coli strains that inhibits lymphocyte activation. Infect. Immun. 2000, 68, 2148–2155. [Google Scholar] [CrossRef] [PubMed]
- McNamara, B.P.; Koutsouris, A.; O’Connell, C.B.; Nougayréde, J.P.; Donnenberg, M.S.; Hecht, G. Translocated EspF protein from enteropathogenic Escherichia coli disrupts host intestinal barrier function. J. Clin. Investig. 2001, 107, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Tochio, T.; Kadota, Y.; Tanaka, T.; Koga, Y. 1-Kestose, the smallest fructooligosaccharide component, which efficiently stimulates Faecalibacterium prausnitzii as well as Bifidobacteria in humans. Foods 2018, 7, 140. [Google Scholar] [CrossRef]
- Watanabe, A.; Kadota, Y.; Kamio, R.; Tochio, T.; Endo, A.; Shimomura, Y.; Kitaura, Y. 1-Kestose supplementation mitigates the progressive deterioration of glucose metabolism in type 2 diabetes OLETF rats. Sci. Rep. 2020, 10, 15674. [Google Scholar] [CrossRef]
- Sivan, A.; Corrales, L.; Hubert, N.; Williams, J.B.; Aquino-Michaels, K.; Earley, Z.M.; Benyamin, F.W.; Lei, Y.M.; Jabri, B.; Alegre, M.L.; et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science 2015, 350, 1084–1089. [Google Scholar] [CrossRef]
- Krajmalnik-Brown, R.; Ilhan, Z.E.; Kang, D.W.; DiBaise, J.K. Effects of gut microbes on nutrient absorption and energy regulation. Nutr. Clin. Pract. 2012, 27, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.; Tochio, T.; Kadota, Y.; Takahashi, M.; Kitaura, Y.; Ishikawa, H.; Yasutake, T.; Nakano, M.; Shinohara, H.; Kudo, T.; et al. Supplementation of 1-Kestose Modulates the Gut Microbiota Composition to Ameliorate Glucose Metabolism in Obesity-Prone Hosts. Nutrients 2021, 13, 2983. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | −KES | +KES | p Value |
|---|---|---|---|
| Sex (male/female) | 8/10 | 10/10 | 0.757 |
| ECOG (0/1) | 16/2 | 18/2 | >0.999 |
| Stage (III/IV) | 9/9 | 10/10 | >0.999 |
| Age at entry, mean ± SD | 67.50 ± 9.40 | 68.95 ± 9.34 | 0.637 |
| BMI (kg/m2), mean ± SD | 21.37 ± 2.59 | 22.68 ± 3.14 | 0.069 |
| Extracellular water–total body water ratio (ECW/TBW), mean ± SD | 0.39 ± 0.01 | 0.39 ± 0.01 | 0.512 |
| PhA, mean ± SD | 4.48 ± 0.46 | 4.46 ± 0.57 | 0.922 |
| Alb (g/dL), mean ± SD | 3.76 ± 0.36 | 3.67 ± 0.50 | 0.525 |
| CRP (mg/dL), mean ± SD | 0.62 ± 1.33 | 1.43 ± 1.88 | 0.080 |
| Neutrophil (%), mean ± SD | 68.29 ± 10.15 | 69.48 ± 12.34 | 0.767 |
| Lymphocytes (%), mean ± SD | 23.31 ± 8.88 | 21.38 ± 9.13 | 0.857 |
| NLR, mean ± SD | 3.48 ± 1.73 | 5.28 ± 7.17 | 0.989 |
| CA19-9 (Log10(CA19-9)), mean ± SD | 2.89 ± 1.66 | 2.81 ± 1.31 | 0.874 |
| Characteristic | −KES | +KES |
|---|---|---|
| Complete response | 0 | 0 |
| Partial response | 11 (61%) | 14 (70%) |
| Stable disease | 4 (22%) | 5 (25%) |
| Progressive disease | 3 (17%) | 1 (5%) |
| Taxon Name | LDA Effect Size | p Value | Taxonomic Relative Abundance | |
|---|---|---|---|---|
| Healthy | PDAC | |||
| Escherichia coli group | 4.228 | 0.013 | 0.741 | 3.765 |
| Blautia wexlerae | 4.207 | 0.001 | 6.002 | 2.968 |
| Streptococcus salivarius group | 4.176 | 0.001 | 0.499 | 3.547 |
| Bifidobacterium adolescentis group | 4.119 | 0.044 | 3.577 | 1.185 |
| Enterococcus faecium group | 4.029 | 0.015 | 1.023 | 2.550 |
| Taxon Name | Taxonomic Relative Abundance | |||||
|---|---|---|---|---|---|---|
| −KES | +KES | |||||
| Before | After | p-Value | Before | After | p-Value | |
| Escherichia coli group | 3.74 ± 10.08 | 4.28 ± 5.98 | 0.799 | 3.78 ± 9.33 | 1.76 ± 4.08 | 0.023 |
| Blautia wexlerae | 3.08 ± 3.94 | 3.45 ± 3.68 | 0.832 | 2.87 ± 2.20 | 2.67 ± 2.73 | 0.523 |
| Streptococcus salivarius group | 3.13 ± 5.95 | 3.97 ± 6.55 | 0.417 | 3.92 ± 6.40 | 5.03 ± 5.03 | 0.368 |
| Bifidobacterium adolescentis group | 1.62 ± 3.26 | 3.02 ± 9.79 | 0.570 | 0.80 ± 2.44 | 1.53 ± 4.27 | 0.722 |
| Enterococcus faecium group | 0.02 ± 0.03 | 0.85 ± 3.10 | 0.079 | 4.83 ± 20.39 | 4.10 ± 12.90 | 0.540 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakaoka, K.; Ohno, E.; Kuramitsu, K.; Kuzuya, T.; Funasaka, K.; Tochio, T.; Fujii, T.; Takahashi, H.; Kondo, N.; Miyahara, R.; et al. Efficacy of 1-Kestose Supplementation in Patients with Pancreatic Ductal Adenocarcinoma: A Randomized Controlled Pilot Study. Nutrients 2024, 16, 2889. https://doi.org/10.3390/nu16172889
Nakaoka K, Ohno E, Kuramitsu K, Kuzuya T, Funasaka K, Tochio T, Fujii T, Takahashi H, Kondo N, Miyahara R, et al. Efficacy of 1-Kestose Supplementation in Patients with Pancreatic Ductal Adenocarcinoma: A Randomized Controlled Pilot Study. Nutrients. 2024; 16(17):2889. https://doi.org/10.3390/nu16172889
Chicago/Turabian StyleNakaoka, Kazunori, Eizaburo Ohno, Kento Kuramitsu, Teiji Kuzuya, Kohei Funasaka, Takumi Tochio, Tadashi Fujii, Hideaki Takahashi, Nobuhiro Kondo, Ryoji Miyahara, and et al. 2024. "Efficacy of 1-Kestose Supplementation in Patients with Pancreatic Ductal Adenocarcinoma: A Randomized Controlled Pilot Study" Nutrients 16, no. 17: 2889. https://doi.org/10.3390/nu16172889
APA StyleNakaoka, K., Ohno, E., Kuramitsu, K., Kuzuya, T., Funasaka, K., Tochio, T., Fujii, T., Takahashi, H., Kondo, N., Miyahara, R., Hashimoto, S., & Hirooka, Y. (2024). Efficacy of 1-Kestose Supplementation in Patients with Pancreatic Ductal Adenocarcinoma: A Randomized Controlled Pilot Study. Nutrients, 16(17), 2889. https://doi.org/10.3390/nu16172889