
Identification of Factors on Blood Selenium Levels in the US Adults: A Cross-Sectional Study


Abstract
1. Introduction
2. Materials and Methods
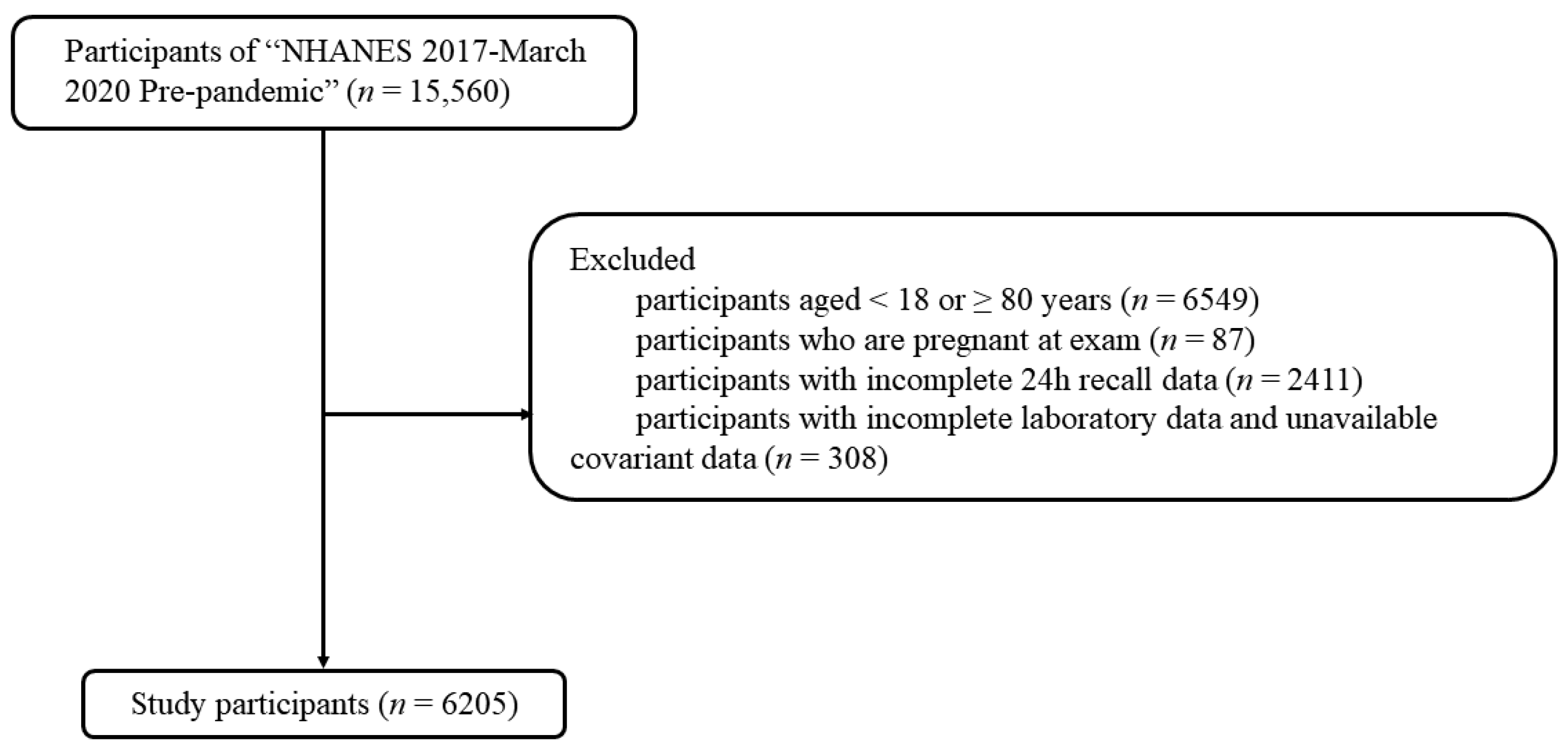
2.1. Study Design and Participants
2.2. Dietary and Supplemental Se Intakes, and Blood Se Concentration
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics for Blood Se Concentration
3.2. Comparison of Se Intake and Se Level between Different Groups of Factors
3.3. Association between Factors and Blood Se Concentration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bai, Y.Z.; Zhang, S.Q. Do selenium-enriched foods provide cognitive benefit? Metab. Brain Dis. 2023, 38, 1501–1502. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Li, B.; Li, S.; Song, Z.; Kong, F.; Zhang, X. Selenium in Wheat from Farming to Food. J. Agric. Food Chem. 2021, 69, 15458–15467. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.Z.; Zhang, S.Q. Evidence-based proposal for lowering Chinese tolerable upper intake level for selenium. Nutr. Res. 2024, 123, 53–54. [Google Scholar] [CrossRef]
- Jain, R.B.; Choi, Y.S. Normal reference ranges for and variability in the levels of blood manganese and selenium by gender, age, and race/ethnicity for general U.S. population. J. Trace Elem. Med. Biol. 2015, 30, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.Q.; Shen, S.; Zhang, Y. Comparison of Bioavailability, Pharmacokinetics, and Biotransformation of Selenium-Enriched Yeast and Sodium Selenite in Rats Using Plasma Selenium and Selenomethionine. Biol. Trace Elem. Res. 2020, 196, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Liu, K.; Sun, X.; Qin, S.; Wu, M.; Qin, L.; Wang, Y.; Li, Z.; Zhong, X.; Wei, X. A cross-sectional study of blood selenium concentration and cognitive function in elderly Americans: National Health and Nutrition Examination Survey 2011–2014. Ann. Hum. Biol. 2020, 47, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Panel on Dietary Antioxidants and Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; Institute of Medicine, The National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Swanson, C.A.; Longnecker, M.P.; Veillon, C.; Howe, M.; Levander, O.A.; Taylor, P.R.; McAdam, P.A.; Brown, C.C.; Stampfer, M.J.; Willett, W.C. Selenium intake, age, gender, and smoking in relation to indices of selenium status of adults residing in a seleniferous area. Am. J. Clin. Nutr. 1990, 52, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.M.; Wei, H.J.; Yang, C.L.; Xing, J.; Qiao, C.H.; Feng, Y.M.; Liu, J.; Liu, Z.; Wu, Q.; Liu, Y.X.; et al. Selenium intake and metabolic balance of 10 men from a low selenium area of China. Am. J. Clin. Nutr. 1985, 42, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Alfthan, G.; Eurola, M.; Ekholm, P.; Venäläinen, E.R.; Root, T.; Korkalainen, K.; Hartikainen, H.; Salminen, P.; Hietaniemi, V.; Aspila, P.; et al. Effects of nationwide addition of selenium to fertilizers on foods, and animal and human health in Finland: From deficiency to optimal selenium status of the population. J. Trace Elem. Med. Biol. 2015, 31, 142–147. [Google Scholar] [CrossRef]
- Turck, D.; Bohn, T.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Peláez, C.; et al. Scientific opinion on the tolerable upper intake level for selenium. Efsa J. 2023, 21, e07704. [Google Scholar]
- Zhang, S.Q.; Bai, Y.Z. Strategies for enhancing beneficial effects of selenium on cognitive function. Metab. Brain Dis. 2023, 38, 1857–1858. [Google Scholar] [CrossRef] [PubMed]
- Naderi, M.; Puar, P.; Zonouzi-Marand, M.; Chivers, D.P.; Niyogi, S.; Kwong, R.W.M. A comprehensive review on the neuropathophysiology of selenium. Sci. Total Environ. 2021, 767, 144329. [Google Scholar] [CrossRef]
- Adams, W.J.; Duguay, A. Selenium-mercury interactions and relationship to aquatic toxicity: A review. Integr. Environ. Assess. Manag. 2024; preprint. [Google Scholar] [CrossRef]
- Tian, C.; Qiu, Y.; Zhao, Y.; Fu, L.; Xia, D.; Ying, J. Selenium protects against Pb-induced renal oxidative injury in weaning rats and human renal tubular epithelial cells through activating NRF2. J. Trace Elem. Med. Biol. 2024, 83, 127420. [Google Scholar] [CrossRef]
- Pei, J.; Yan, L.; Wu, Y.; Zhang, X.; Jia, H.; Li, H. Association between low blood selenium concentrations and poor hand grip strength in United States adults participating in NHANES (2011–2014). Appl. Physiol. Nutr. Metab. 2023, 48, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.F.; Chan, H.M. Factors associated with the blood and urinary selenium concentrations in the Canadian population: Results of the Canadian Health Measures Survey (2007–2011). Int. J. Hyg. Environ. Health 2018, 221, 1023–1031. [Google Scholar] [CrossRef]
- Seale, L.A.; Ogawa-Wong, A.N.; Berry, M.J. Sexual dimorphism in selenium metabolism and selenoproteins. Free Radic Biol. Med. 2018, 127, 198–205. [Google Scholar] [CrossRef]
- McAdam, P.A.; Smith, D.K.; Feldman, E.B.; Hames, C. Effect of age, sex, and race on selenium status of healthy residents of Augusta, Georgia. Biol. Trace Elem. Res. 1984, 6, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Dickson, R.C.; Tomlinson, R.H. Selenium in blood and human tissues. Clin. Chim. Acta 1967, 16, 311–321. [Google Scholar] [CrossRef]
- Fernández-Banares, F.; Dolz, C.; Mingorance, M.D.; Cabré, E.; Lachica, M.; Abad-Lacruz, A.; Gil, A.; Esteve, M.; Giné, J.J.; Gassull, M.A. Low serum selenium concentration in a healthy population resident in Catalunya: A preliminary report. Eur. J. Clin. Nutr. 1990, 44, 225–229. [Google Scholar]
- Zhang, S.Q. Selenium and cognitive function. Metab. Brain Dis. 2023, 38, 221–222. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, S.; Baral, B.K.; Feng, D.; Sy, F.S.; Rodriguez, R. Is selenium intake associated with the presence of depressive symptoms among US adults? Findings from National Health and Nutrition Examination Survey (NHANES) 2011–2014. Nutrition 2019, 62, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Niskar, A.S.; Paschal, D.C.; Kieszak, S.M.; Flegal, K.M.; Bowman, B.; Gunter, E.W.; Pirkle, J.L.; Rubin, C.; Sampson, E.J.; McGeehin, M. Serum selenium levels in the US population: Third National Health and Nutrition Examination Survey, 1988–1994. Biol. Trace Elem. Res. 2003, 91, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Alasfar, F.; Ben-Nakhi, M.; Khoursheed, M.; Kehinde, E.O.; Alsaleh, M. Selenium is significantly depleted among morbidly obese female patients seeking bariatric surgery. Obes. Surg. 2011, 21, 1710–1713. [Google Scholar] [CrossRef]
- Korpela, H.; Kumpulainen, J.; Luoma, P.V.; Arranto, A.J.; Sotaniemi, E.A. Decreased serum selenium in alcoholics as related to liver structure and function. Am. J. Clin. Nutr. 1985, 42, 147–151. [Google Scholar] [CrossRef]

{kind=link}
| Overall n | Blood Se Concentration (μg/L) | |||||
|---|---|---|---|---|---|---|
| Weighted % (95% CI) | Q1 (85.15–169.34) | Q2 (169.35–183.94) | Q3 (183.95–200.76) | Q4 (200.77–526.40) | p-Value | |
| Characteristic | n | |||||
| Weighted% (95% CI) | ||||||
| 6205 | 1551 | 1552 | 1551 | 1551 | ||
| 21.3 (18.3, 24.3) | 24.4 (22.8, 25.9) | 27.1 (24.4, 29.7) | 27.2 (24.4, 30.0) | |||
| Gender | <0.05 | |||||
| Male | 2988 | 655 | 728 | 768 | 837 | |
| 48.7 (46.3, 51.0) | 19.2 (15.6, 22.7) | 22.9 (20.2, 25.7) | 26.5 (22.5, 30.5) | 31.4 (27.7, 35.1) | ||
| Female | 3217 | 896 | 824 | 783 | 714 | |
| 51.3 (49.0, 53.6) | 23.4 (20.0, 26.8) | 25.7 (23.2, 28.2) | 27.6 (24.9, 30.3) | 23.3 (20.0, 26.5) | ||
| Age | 0.14 | |||||
| 18–39 | 2134 | 531 | 553 | 538 | 512 | |
| 38.9 (36.0, 41.8) | 19.9 (15.7, 24.2) | 27.2 (23.7, 30.8) | 26.7 (23.5, 29.8) | 26.2 (23.1, 29.3) | ||
| 40–59 | 2118 | 492 | 523 | 553 | 512 | |
| 34.8 (32.4, 37.1) | 21.9 (17.8, 26.1) | 21.5 (19.2, 23.9) | 29.2 (25.7, 32.6) | 26.2 (23.1, 29.3) | ||
| 60–79 | 1953 | 528 | 476 | 460 | 489 | |
| 26.3 (23.1, 29.6) | 22.6 (19.3, 25.9) | 23.9 (20.3, 27.5) | 24.9 (20.8, 29.0) | 28.6 (23.6, 33.7) | ||
| Race | <0.05 | |||||
| Mexican American | 750 | 136 | 206 | 206 | 202 | |
| 8.8 (6.1, 11.5) | 17.1 (12.7, 21.5) | 27.2 (22.1, 32.3) | 27.0 (20.2, 33.9) | 28.7 (22.9, 34.4) | ||
| Other Hispanic | 647 | 181 | 171 | 145 | 150 | |
| 8.0 (6.3, 9.7) | 27.4 (23.8, 31.1) | 25.3 (20.5, 30.2) | 26.5 (19.9, 33.2) | 20.7 (15.9, 25.5) | ||
| Non-Hispanic White | 2121 | 481 | 512 | 587 | 541 | |
| 61.8 (56.3, 67.4) | 20.3 (16.3, 24.4) | 24.1 (22.0, 26.1) | 28.0 (23.9, 32.0) | 27.6 (23.7, 31.5) | ||
| Non-Hispanic Black | 1734 | 562 | 467 | 358 | 347 | |
| 11.4 (8.3, 14.4) | 27.4 (23.0, 31.8) | 27.0 (23.8, 30.1) | 22.7 (19.4, 25.9) | 23.0 (17.9, 28.0) | ||
| Other Race | 953 | 191 | 196 | 255 | 311 | |
| 10.0 (8.1, 11.9) | 19.5 (15.3, 23.7) | 20.1 (15.0, 25.1) | 26.8 (23.9, 29.8) | 33.6 (28.0, 39.2) | ||
| Education | <0.05 | |||||
| <High school | 940 | 266 | 243 | 219 | 212 | |
| 9.2 (8.0, 10.4) | 28.0 (23.2, 32.9) | 25.1 (20.4, 29.8) | 24.1 (18.5, 29.6) | 22.9 (17.2, 28.5) | ||
| High school | 1391 | 388 | 361 | 311 | 331 | |
| 26.8 (24.3, 29.3) | 24.3 (19.8, 28.8) | 26.4 (22.4, 30.5) | 23.0 (18.6, 27.4) | 26.3 (21.8, 30.7) | ||
| >High school | 3577 | 841 | 863 | 950 | 923 | |
| 64.0 (61.0, 67.0) | 19.4 (15.9, 22.9) | 23.3 (21.6, 25.0) | 29.3 (26.4, 32.2) | 28.0 (24.5, 31.6) | ||
| PIR | 0.22 | |||||
| <1.3 | 1585 | 485 | 385 | 380 | 335 | |
| 19.7 (17.5, 21.8) | 25.1 (21.5, 28.8) | 21.9 (19.2, 24.6) | 28.6 (24.9, 32.4) | 24.3 (19.9, 28.7) | ||
| 1.3–4.0 | 2378 | 548 | 589 | 591 | 650 | |
| 39.4 (35.7, 43.1) | 20.1 (16.3, 23.9) | 24.4 (21.8, 27.0) | 26.3 (23.0, 29.6) | 29.2 (25.1, 33.3) | ||
| >4.0 | 1520 | 332 | 379 | 414 | 395 | |
| 40.9 (37.2, 44.7) | 20.1 (15.9, 24.3) | 24.8 (21.7, 27.9) | 28.1 (23.2, 33.0) | 27.0 (22.6, 31,4) | ||
| BMI | 0.64 | |||||
| <18.5 | 93 | 29 | 25 | 10 | 19 | |
| 1.3 (0.8, 1.8) | 30.0 (15.2, 44.8) | 28.3 (11.2, 45.4) | 20.1 (6.7, 33.5) | 21.7 (6.6, 36.7) | ||
| 18.5–25.0 | 1459 | 404 | 369 | 366 | 320 | |
| 24.8 (22.5, 27.0) | 23.1 (18.7, 27.5) | 25.1 (21.9, 28.2) | 26.5 (21.8, 31.2) | 25.3 (21.1, 29.6) | ||
| 25.0–30.0 | 1863 | 410 | 461 | 463 | 529 | |
| 31.4 (29.2, 33.7) | 19.5 (15.8, 23.3) | 24.7 (22.2, 27.3) | 26.1 (20.5, 31.7) | 29.6 (25.0, 34.3) | ||
| ≥30.0 | 2742 | 686 | 688 | 693 | 675 | |
| 42.5 (39.5, 45.5) | 21.2 (17.4, 24.9) | 23.6 (21.6, 25.7) | 28.4 (24.4, 32.3) | 26.8 (23.2, 30.4) | ||
| Smoking status | 0.32 | |||||
| Every day | 866 | 264 | 215 | 203 | 184 | |
| 30.5 (27.6, 33.5) | 24.9 (20.5, 29.2) | 26.6 (21.5, 31.8) | 26.1 (21.9, 30.4) | 22.3 (16.8, 27.9) | ||
| Somedays | 260 | 73 | 71 | 57 | 59 | |
| 10.1 (7.6, 12.6) | 19.3 (10.4, 28.3) | 32.2 (19.0, 45.4) | 25.7 (16.0, 35.4) | 22.7 (12.2, 33.2) | ||
| Not at all | 1384 | 328 | 334 | 343 | 379 | |
| 59.3 (55.5, 63.2) | 21.5 (16.7, 26.3) | 23.7 (19.4, 28.0) | 25.2 (21.1, 29.3) | 29.6 (24.5, 34.7) | ||
| Alcohol use | 0.68 | |||||
| Yes | 840 | 241 | 192 | 218 | 189 | |
| 14.3 (12.6, 16.0) | 21.9 (17.2, 26.6) | 21.9 (17.9, 25.9) | 28.9 (21.9, 35.8) | 27.3 (20.6, 34.1) | ||
| No | 4672 | 1128 | 1202 | 1165 | 1177 | |
| Dietary Se (μg/d) | 0.52 | |||||
| 6.70–73.84 | 1551 | 422 | 381 | 361 | 387 | |
| 22.8 (20.8, 24.8) | 20.5 (17.3, 23.7) | 25.5 (22.8, 28.1) | 27.7 (23.5, 31.9) | 26.4 (22.6, 30.1) | ||
| 73.85–101.29 | 1551 | 417 | 384 | 386 | 364 | |
| 25.4 (23.8, 27.0) | 24.9 (21.0, 28.7) | 24.3 (21.0, 27.6) | 25.8 (20.7, 30.9) | 25.0 (19.2, 30.9) | ||
| 101.30–135.74 | 1550 | 362 | 410 | 391 | 387 | |
| 26.3 (24.5, 28.0) | 19.0 (14.1, 23.9) | 24.5 (21.6, 27.3) | 28.4 (24.5, 32.2) | 28.2 (23.1, 33.2) | ||
| 135.75–780.20 | 1553 | 350 | 377 | 413 | 413 | |
| 25.6 (24.1, 27.0) | 21.0 (16.4, 25.6) | 23.4 (20.5, 26.3) | 26.4 (22.0, 30.8) | 29.2 (24.4, 34.0) | ||
| Total Se (μg/d) | 0.27 | |||||
| 6.70–77.69 | 1549 | 422 | 398 | 350 | 379 | |
| 22.2 (20.1, 24.3) | 21,6 (17.5, 25.8) | 26.3 (23.0, 29.6) | 24.5 (20.8, 28.1) | 27.6 (23.2, 31.9) | ||
| 77.70–107.64 | 1553 | 436 | 402 | 372 | 343 | |
| 25.8 (24.1, 27.5) | 24.4 (20.6, 28.2) | 25.5 (21.0, 29.9) | 26.6 (20.5, 32.8) | 23.5 (17.7, 29.4) | ||
| 107.65–147.89 | 1551 | 377 | 386 | 386 | 402 | |
| 25.8 (24.1, 27.5) | 20.8 (15.0, 26.6) | 24.5 (20.5, 28.6) | 27.5 (22.9, 32.0) | 27.2 (22.0, 32.3) | ||
| 147.90–830.20 | 1552 | 316 | 366 | 443 | 427 | |
| 26.2 (24.3, 28.0) | 18.6 (14.7, 22.5) | 21.5 (18.9, 24.2) | 29.3 (23.5, 35.1) | 30.6 (25.9, 35.3) | ||
| Hypertension history | ||||||
| Yes | 2252 | 583 | 546 | 535 | 588 | 0.42 |
| 31.0 (28.5, 33.6) | 21.6 (18.6, 24.6) | 22.6 (19.7, 25.5) | 26.5 (23.1, 30.0) | 29.2 (25.1, 33.4) | ||
| No | 3947 | 966 | 1006 | 1015 | 960 | |
| 68.9 (66.3, 71.5) | 21.2 (17.6, 24.8) | 25.2 (22.6, 27.8) | 27.3 (24.1, 30.5) | 26.3 (23.5, 29.1) | ||
| Diabetes history | ||||||
| Yes | 883 | 235 | 202 | 196 | 250 | 0.23 |
| 11.0 (10.1, 11.9) | 22.9 (18.8, 26.9) | 22.3 (16.4, 28.1) | 23.4 (18.9, 28.0) | 31.5 (25.6, 37.3) | ||
| No | 5144 | 1276 | 1306 | 1310 | 1252 | |
| 86.7 (85.5, 87.9) | 21.1 (18.0, 24.3) | 24.7 (22.7, 26.7) | 27.5 (24.6, 30.3) | 26.7 (23.7, 29.7) | ||
| Stroke history | ||||||
| Yes | 272 | 92 | 61 | 59 | 60 | 0.38 |
| 3.5 (2.8, 4.3) | 24.5 (16.6, 32.3) | 19.3 (13.2, 25.3) | 30.9 (25.6, 36.2) | 25.3 (16.3, 34.4) | ||
| No | 5630 | 1402 | 1404 | 1419 | 1405 | |
| 96.4 (95.6, 97.1) | 21.4 (18.3, 24.5) | 24.5 (22.8, 26.1) | 26.9 (24.3, 29.6) | 27.2 (24.2, 30.1) | ||
| Characteristic | Se Intake (μg/d) | Differences | Blood Se Concentration (μg/L) | Differences |
|---|---|---|---|---|
| Gender | ||||
| Male | 140.1 (137.6, 142.6) | M > F (p < 0.0001) | 188.5 (187.5, 189.4) | M > F (p < 0.0001) |
| Female | 101.1 (99.5, 102.8) | 184.2 (183.3, 185.1) | ||
| Age | ||||
| 18–39 | 119.1 (116.5, 121.7) | 185.5 (184.4, 186.5) | ||
| 40–59 | 122.5 (119.7, 125.2) | 40–59 > 60–79 (p < 0.05) | 186.9 (185.8, 187.9) | |
| 60–79 | 118.0 (115.2, 120.8) | 186.5 (185.1, 187.8) | ||
| Race | ||||
| Mexican American | 125.3 (121.0, 129.6) | Mexican American > Other Hispanic (p < 0.05) | 189.0 (187.2, 190.8) | Other Race > Non-Hispanic White > Other Hispanic > Non-Hispanic Black (p < 0.05) |
| Other Hispanic | 116.4 (111.5, 121.2) | Mexican American > Non-Hispanic Black (p < 0.05) | 183.8 (181.9, 185.7) | Mexican American > Other Hispanic (p < 0.05) |
| Non-Hispanic White | 122.1 (119.4, 124.8) | Other Hispanic < Non-Hispanic White (p < 0.05) | 188.1 (186.9, 189.3) | |
| Non-Hispanic Black | 113.5 (110.7, 116.3) | Other Hispanic< Other Race (p < 0.05) | 180.9 (179.7, 182.0) | |
| Other Race | 124.9 (120.7, 129.0) | Non-Hispanic White> Non-Hispanic Black (p < 0.05) | 191.5 (189.8, 193.1) | |
| Non-Hispanic Black < Other Race (p < 0.05) | ||||
| Education | ||||
| <High school | 111.2 (107.6, 114.9) | “<High school” < “>High school” | 183.8 (182.2, 185.4) | “<High school” < “>High school” |
| High school | 116.1 (112.8, 119.4) | “High school“ < “>High school” | 184.4 (183.0, 185.8) | “High school“ < “>High school” |
| >High school | 124.4 (122.3, 126.5) | 187.5 (186.6, 188.4) | ||
| BMI | ||||
| Underweight | 117.2 (104.5, 130.0) | Overweight > Obese (p < 0.05) | 181.4 (175.5, 187.2) | Underweight < Overweight (p < 0.05) |
| Normal weight | 121.2 (117.9, 124.4) | 184.4 (183.1, 185.6) | Normal weight < Overweight (p < 0.05) | |
| Overweight | 121.7 (118.8, 124.7) | 188.8 (187.6, 190.1) | Overweight > Obese (p < 0.05) | |
| Obese | 117.9 (115.6, 120.2) | 185.9 (184.9, 186.9) | ||
| PIR | ||||
| Low | 111.4 (108.5, 114.2) | Low < Medium < High (p < 0.05) | 182.7 (181.5, 184.0) | Low < Medium (p < 0.05) |
| Medium | 120.3 (117.8, 122.7) | 187.7 (186.6, 188.3) | Low < High (p < 0.05) | |
| High | 128.2 (124.7, 131.6) | 188.4 (187.0, 189.7) | ||
| Smoking status | ||||
| Every day | 115.2 (111.2, 119.2) | Every day < Somedays (p < 0.05) | 182.1 (180.4, 183.7) | Every day < Not at all (p < 0.05) |
| Somedays | 127.5 (119.0, 135.9) | Every day < Not at all (p < 0.05) | 183.3 (180.3, 186.2) | Somedays< Not at all (p < 0.05) |
| Not at all | 125.6 (122.1, 129.1) | 187.8 (186.4, 189.3) | ||
| Alcohol use | ||||
| Yes | 131.9 (127.4, 136.4) | Yes > No (p < 0.0001) | 183.9 (182.0, 185.7) | Yes < No (p < 0.05) |
| No | 119.6 (117.9, 121.4) | 186.5 (185.7, 187.2) |
| Factors | β (95% CI) | p-Value |
|---|---|---|
| Dietary Se (μg/day) | 0.03 (0.01, 0.04) | <0.05 |
| Total Se (μg/day) | 0.05 (0.04, 0.07) | <0.001 |
| Female (vs. male) | −2.66 (−5.26, −0.06) | <0.05 |
| Age (y) | 0.03 (−0.06, 0.11) | 0.52 |
| Race (vs. other race) | ||
| Mexican American | −1.14 (−5.64, 3.36) | 0.61 |
| Other Hispanic | −6.59 (−11.2, −1.97) | <0.05 |
| Non-Hispanic White | −1.98 (−5.16, 1.20) | 0.21 |
| Non-Hispanic Black | −6.65 (−10.8, 2.51) | <0.05 |
| Educational status (vs. <high school) | ||
| High school | −0.51 (−3.93, 2.91) | 0.76 |
| >High school | 2.73 (−0.94, 6.40) | 0.14 |
| PIR (vs. low) | ||
| Medium | 1.49 (−0.84, 3.83) | 0.20 |
| High | 0.07 (−2.56, 2.70) | 0.96 |
| BMI (vs. underweight) | ||
| Normal weight | 5.76 (−0.65, 12.17) | 0.08 |
| Overweight | 8.52 (2.25, 14.79) | <0.05 |
| Obese | 7.33 (1.17, 13.49) | <0.05 |
| Smoking status (vs. not at all) | ||
| Everyday | −2.65 (−6.12, 0.81) | 0.13 |
| Somedays | −3.44 (−9.54, 2.66) | 0.26 |
| Alcohol use (vs. yes) | 1.59 (−0.97, 4.16) | 0.21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bai, Y.-Z.; Gao, Y.-X.; Zhang, S.-Q. Identification of Factors on Blood Selenium Levels in the US Adults: A Cross-Sectional Study. Nutrients 2024, 16, 1734. https://doi.org/10.3390/nu16111734
Bai Y-Z, Gao Y-X, Zhang S-Q. Identification of Factors on Blood Selenium Levels in the US Adults: A Cross-Sectional Study. Nutrients. 2024; 16(11):1734. https://doi.org/10.3390/nu16111734
Chicago/Turabian StyleBai, Ya-Zhi, Yi-Xiong Gao, and Shuang-Qing Zhang. 2024. "Identification of Factors on Blood Selenium Levels in the US Adults: A Cross-Sectional Study" Nutrients 16, no. 11: 1734. https://doi.org/10.3390/nu16111734
APA StyleBai, Y.-Z., Gao, Y.-X., & Zhang, S.-Q. (2024). Identification of Factors on Blood Selenium Levels in the US Adults: A Cross-Sectional Study. Nutrients, 16(11), 1734. https://doi.org/10.3390/nu16111734