
An Intensive Culinary Intervention Programme to Promote Healthy Ageing: The SUKALMENA-InAge Feasibility Pilot Study
 , , , , and
, , , , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design
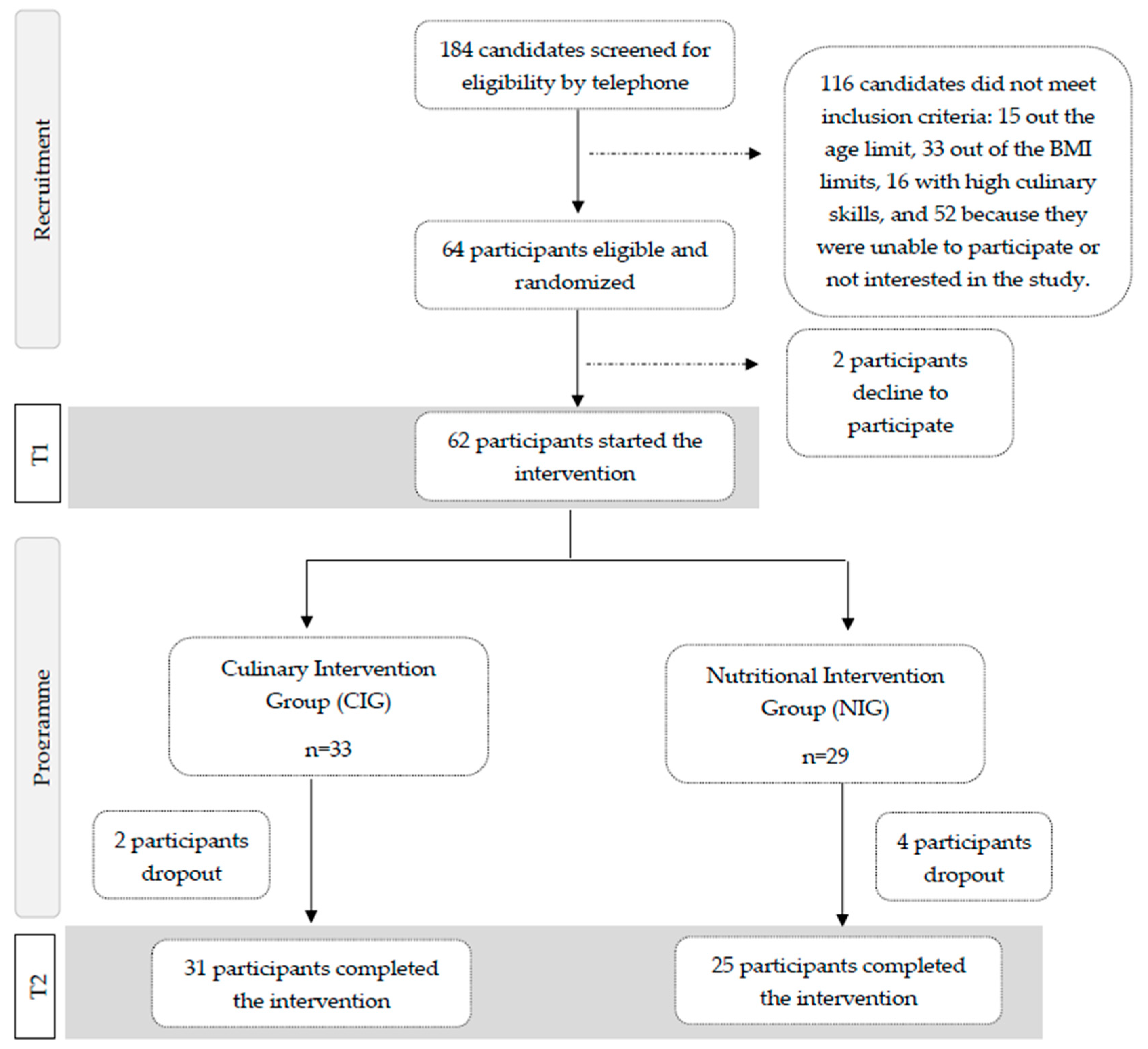
2.2. Sample Recruitment and Selection
2.3. Intervention and Control Conditions
2.4. Outcomes Assessed
2.4.1. Primary Outcome
2.4.2. Secondary Outcomes
- Dietary outcomes
- Cooking-related outcomes
- Health and biological outcomes
2.5. Other Measurements
2.6. Statistical Analysis
3. Results
3.1. Dietary Outcomes
3.2. Cooking-Related Outcomes
3.3. Health and Biological Outcomes
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kirkwood, T.B.L. Why and How Are We Living Longer? Exp. Physiol. 2017, 102, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Shlisky, J.; Bloom, D.E.; Beaudreault, A.R.; Tucker, K.L.; Keller, H.H.; Freund-Levi, Y.; Fielding, R.A.; Cheng, F.W.; Jensen, G.L.; Wu, D.; et al. Nutritional Considerations for Healthy Aging and Reduction in Age-Related Chronic Disease. Adv. Nutr. 2017, 8, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Ruthsatz, M.; Candeias, V. Non-Communicable Disease Prevention, Nutrition and Aging. Acta Biomed. 2020, 91, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) Approach to Healthy Ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.; White, M.; Brown, H.; Wrieden, W.; Kwasnicka, D.; Halligan, J.; Robalino, S.; Adams, J. Health and Social Determinants and Outcomes of Home Cooking: A Systematic Review of Observational Studies. Appetite 2017, 111, 116–134. [Google Scholar] [CrossRef]
- Mauriello, L.M.; Artz, K. Culinary Medicine: Bringing Healthcare into the Kitchen. Am. J. Health Promot. 2019, 33, 825–829. [Google Scholar] [CrossRef]
- Eisenberg, D.M.; Pacheco, L.S.; McClure, A.C.; McWhorter, J.W.; Janisch, K.; Massa, J. Perspective: Teaching Kitchens: Conceptual Origins, Applications and Potential for Impact within Food Is Medicine Research. Nutrients 2023, 15, 2859. [Google Scholar] [CrossRef] [PubMed]
- Domper, J.; Gayoso, L.; Goni, L.; Victor de la, O.; Etxeberria, U.; Ruiz-Canela, M. Culinary Medicine and Healthy Ageing: A Comprehensive Review. Nutr. Res. Rev. 2023, 23, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Roman, G.; Evan Jackson, R.; Ghadia, R.; Roman, A.; Reis, J. Mediterranean Diet: The Role of Long-Chain ω-3 Fatty Acids in Fish; Polyphenols in Fruits, Vegetables, Cereals, Coffee, Tea, Cacao and Wine; Probiotics and Vitamins in Prevention of Stroke, Age-Related Cognitive Decline, and Alzheimer Disease. Rev. Neurol. 2019, 175, 724–741. [Google Scholar] [CrossRef]
- Rajaram, S.; Jones, J.; Lee, G.J. Plant-Based Dietary Patterns, Plant Foods, and Age-Related Cognitive Decline. Adv. Nutr. 2019, 10, 422–436. [Google Scholar] [CrossRef]
- Ganesan, K.; Sukalingam, K.; Xu, B. Impact of Consumption of Repeatedly Heated Cooking Oils on the Incidence of Various Cancers- A Critical Review. Crit. Rev. Food Sci. Nutr. 2019, 59, 488–505. [Google Scholar] [CrossRef] [PubMed]
- Perrone, A.; Giovino, A.; Benny, J.; Martinelli, F. Advanced Glycation End Products (AGEs): Biochemistry, Signaling, Analytical Methods, and Epigenetic Effects. Oxid. Med. Cell Longev. 2020, 2020, 3818196. [Google Scholar] [CrossRef] [PubMed]
- Sohouli, M.H.; Fatahi, S.; Sharifi-Zahabi, E.; Santos, H.O.; Tripathi, N.; Lari, A.; Pourrajab, B.; Kord-Varkaneh, H.; Găman, M.A.; Shidfar, F. The Impact of Low Advanced Glycation End Products Diet on Metabolic Risk Factors: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv. Nut. 2021, 12, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Wang, Y.; Fu, L. Dietary Advanced Glycation End-Products: Perspectives Linking Food Processing with Health Implications. Compr. Rev. Food Sci. Food Saf. 2020, 19, 2559–2587. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, J.; del Castillo, M.D.; de la Maza, M.P.; Filip, R.; Gugliucci, A.; Luevano-Contreras, C.; Macías-Cervantes, M.H.; Markowicz Bastos, D.H.; Medrano, A.; Menini, T.; et al. Dietary Advanced Glycation End Products and Their Role in Health and Disease. Adv. Nutr. 2015, 6, 461–473. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Lin, X.; Bu, C.; Zhang, X. Role of Advanced Glycation End Products in Mobility and Considerations in Possible Dietary and Nutritional Intervention Strategies. Nutr. Metab. 2018, 15, 72. [Google Scholar] [CrossRef] [PubMed]
- Gayoso, L.; Goni, L.; de la O, V.; Domper, J.; Razquin, C.; Ruiz-Canela, M.; Etxeberria, U. An Intensive Culinary Intervention Programme to Empower Type 2 Diabetic Patients in Cooking Skills: The SUKALMENA Pilot Study. Int. J. Gastron. Food Sci. 2023, 32, 100721. [Google Scholar] [CrossRef]
- Arain, M.; Campbell, M.J.; Cooper, C.L.; Lancaster, G.A. What Is a Pilot or Feasibility Study? A Review of Current Practice and Editorial Policy. BMC Med. Res. Methodol. 2010, 10, 67. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, A.; Tovar, J.; Johansson, M.; Radeborg, K.; Björck, I. A Diet Based on Multiple Functional Concepts Improves Cognitive Performance in Healthy Subjects. Nutr. Metab. 2013, 10, 49. [Google Scholar] [CrossRef]
- De Courten, B.; De Courten, M.P.J.; Soldatos, G.; Dougherty, S.L.; Straznicky, N.; Schlaich, M.; Sourris, K.C.; Chand, V.; Scheijen, J.L.J.M.; Kingwell, B.A.; et al. Diet Low in Advanced Glycation End Products Increases Insulin Sensitivity in Healthy Overweight Individuals: A Double-Blind, Randomized, Crossover Trial. Am. J. Clin. Nutr. 2016, 103, 1426–1433. [Google Scholar] [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- De La Fuente-Arrillaga, C.; Vzquez Ruiz, Z.; Bes-Rastrollo, M.; Sampson, L.; Martinez-González, M.A. Reproducibility of an FFQ Validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Martin-moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and Validation of a Food Frequency Questionnaire in Spain Downloaded From. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Moreiras, O.; Carvajal, Á.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos, 7th ed.; Piramide: Madrid, Spain, 2003; Volume 1, ISBN 978-84-368-3947-0. [Google Scholar]
- Mataix Verdú, J.; García Diz, L.; Mañas Almendros, M.; Martínez de Victoria, E.; Llopis González, J. Tabla de Composición de Alimentos (Food Composition Tables), 4th ed.; Editorial Universidad de Granada: Granada, Spain, 2003; Volume 1, ISBN 84-338-3050-3. [Google Scholar]
- Goni, L.; Gil, M.; de la O, V.; Martínez-González, M.Á.; Eisenberg, D.M.; Pueyo-Garrigues, M.; Vasilj, M.; Gayoso, L.; Etxeberria, U.; Ruiz-Canela, M. Development and Validation of a New Home Cooking Frequency Questionnaire: A Pilot Study. Nutrients 2022, 14, 1136. [Google Scholar] [CrossRef] [PubMed]
- Vasilj, M.; Goni, L.; Gayoso, L.; Razquin, C.; Sesma, T.; Etxeberria, U.; Ruiz-Canela, M. Correlation between Serum Advanced Glycation End Products and Dietary Intake of Advanced Glycation End Products Estimated from Home Cooking and Food Frequency Questionnaires. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Condrasky, M.D.; Williams, J.E.; Catalano, P.M.; Griffin, S.F. Development of Psychosocial Scales for Evaluating the Impact of a Culinary Nutrition Education Program on Cooking and Healthful Eating. J. Nutr. Educ. Behav. 2011, 43, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Vrhovnik, L. A Pilot Study for the Development of a Food Skills Survey Tool. Master’s Thesis, Queen’s University, Kingston, ON, Canada, 2012. [Google Scholar]
- Matthews, D.R.; Hosker, J.R.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Fl-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Arshi, B.; Chen, J.; Ikram, M.A.; Zillikens, M.C.; Kavousi, M. Advanced Glycation End-Products, Cardiac Function and Heart Failure in the General Population: The Rotterdam Study. Diabetologia 2023, 66, 472–481. [Google Scholar] [CrossRef]
- Van Waateringe, R.P.; Fokkens, B.T.; Slagter, S.N.; Van der Klauw, M.M.; Van Vliet-Ostaptchouk, J.V.; Graaff, R.; Paterson, A.D.; Smit, A.J.; Lutgers, H.L.; Wolffenbuttel, B.H.R. Skin Autofluorescence Predicts Incident Type 2 Diabetes, Cardiovascular Disease and Mortality in the General Population. Diabetologia 2019, 62, 269–280. [Google Scholar] [CrossRef]
- McGowan, L.; Pot, G.K.; Stephen, A.M.; Lavelle, F.; Spence, M.; Raats, M.; Hollywood, L.; McDowell, D.; McCloat, A.; Mooney, E.; et al. The Influence of Socio-Demographic, Psychological and Knowledge-Related Variables alongside Perceived Cooking and Food Skills Abilities in the Prediction of Diet Quality in Adults: A Nationally Representative Cross-Sectional Study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 111. [Google Scholar] [CrossRef]
- Garcia, A.L.; Reardon, R.; Mcdonald, M.; Vargas-Garcia, E.J. Community Interventions to Improve Cooking Skills and Their Effects on Confidence and Eating Behaviour. Curr. Nutr. Rep. 2016, 5, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Lo, B.K.; Loui, C.; Folta, S.C.; Flickinger, A.; Connor, L.M.; Liu, E.; Megiel, S.; Seguin, R.A. Self-Efficacy and Cooking Confidence Are Associated with Fruit and Vegetable Intake in a Cross-Sectional Study with Rural Women. Eat. Behav. 2019, 33, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Hasan, B.; Thompson, W.G.; Almasri, J.; Wang, Z.; Lakis, S.; Prokop, L.J.; Hensrud, D.D.; Frie, K.S.; Wirtz, M.J.; Murad, A.L.; et al. The Effect of Culinary Interventions (Cooking Classes) on Dietary Intake and Behavioral Change: A Systematic Review and Evidence Map. BMC Nutr. 2019, 5, 29. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, J.A.; Ishikawa, Y.; Hosokawa, C.; Janisch, K.; Massa, J.; Eisenberg, D.M. Gender Differences in Global Estimates of Cooking Frequency Prior to COVID-19. Appetite 2021, 161, 105117. [Google Scholar] [CrossRef] [PubMed]
- Aranceta, J.; Rodrigo, C.P.; Eguileor, I.; Marzana, I.; de Galdeano, L.G.; de Buruaga, J.S. Food Consumption Patterns in the Adult Population of the Basque Country (EINUT-I). Public Health Nutr. 1998, 1, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Ramos, E.; Tomaino, L.; Sánchez-Villegas, A.; Ribas-Barba, L.; Gómez, S.F.; Wärnberg, J.; Osés, M.; González-Gross, M.; Gusi, N.; Aznar, S.; et al. Trends in Adherence to the Mediterranean Diet in Spanish Children and Adolescents across Two Decades. Nutrients 2023, 15, 2348. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Martínez, R.; Mafla-España, M.A.; Cauli, O. Mediterranean Diet Adherence in Community-Dwelling Older Adults in Spain: Social Determinants Related to the Family. Nutrients 2022, 14, 5141. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; Simonetta, I.; Daidone, M.; Mogavero, A.; Ortello, A.; Pinto, A. Metabolic and Vascular Effect of the Mediterranean Diet. Int. J. Mol. Sci. 2019, 20, 4716. [Google Scholar] [CrossRef] [PubMed]
- Di Rosa, C.; Lattanzi, G.; Spiezia, C.; Imperia, E.; Piccirilli, S.; Beato, I.; Gaspa, G.; Micheli, V.; De Joannon, F.; Vallecorsa, N.; et al. Mediterranean Diet versus Very Low-Calorie Ketogenic Diet: Effects of Reaching 5% Body Weight Loss on Body Composition in Subjects with Overweight and with Obesity—A Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 13040. [Google Scholar] [CrossRef]
- Alpaugh, M.; Pope, L.; Trubek, A.; Skelly, J.; Harvey, J. Cooking as a Health Behavior: Examining the Role of Cooking Classes in a Weight Loss Intervention. Nutrients 2020, 12, 3669. [Google Scholar] [CrossRef]
- Baden, M.Y.; Kato, S.; Niki, A.; Hara, T.; Ozawa, H.; Ishibashi, C.; Hosokawa, Y.; Fujita, Y.; Fujishima, Y.; Nishizawa, H.; et al. Feasibility Pilot Study of a Japanese Teaching Kitchen Program. Front. Public. Health 2023, 11, 1258434. [Google Scholar] [CrossRef] [PubMed]
- Crosby, L.; Rembert, E.; Levin, S.; Green, A.; Ali, Z.; Jardine, M.; Nguyen, M.; Elliott, P.; Goldstein, D.; Freeman, A.; et al. Changes in Food and Nutrient Intake and Diet Quality on a Low-Fat Vegan Diet Are Associated with Changes in Body Weight, Body Composition, and Insulin Sensitivity in Overweight Adults: A Randomized Clinical Trial. J. Acad. Nutr. Diet. 2022, 122, 1922–1939. [Google Scholar] [CrossRef] [PubMed]
- Karpińska, E.; Moskwa, J.; Puścion-Jakubik, A.; Naliwajko, S.K.; Soroczyńska, J.; Markiewicz-Żukowska, R.; Socha, K. Body Composition of Young Women and The Consumption of Selected Nutrients. Nutrients 2023, 15, 129. [Google Scholar] [CrossRef] [PubMed]
- Gatto, N.M.; Martinez, L.C.; Spruijt-Metz, D.; Davis, J.N. LA Sprouts Randomized Controlled Nutrition, Cooking and Gardening Programme Reduces Obesity and Metabolic Risk in Hispanic/Latino Youth. Pediatr. Obes. 2017, 12, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Reicks, M.; Kocher, M.; Reeder, J. Impact of Cooking and Home Food Preparation Interventions among Adults: A Systematic Review (2011–2016). J. Nutr. Educ. Behav. 2018, 50, 148–172. [Google Scholar] [CrossRef] [PubMed]
- Villarini, M.; Lanari, C.; Barchiesi, L.; Casciari, E.; Tabascio, A.; Castellini, M.; Levorato, S.; Vannini, S.; Fornaciari, G.; Moretti, M.; et al. Effects of the “PreveDi” Lifestyle Modification Trial on Metabolic Syndrome. Ann. Ig 2015, 27, 595–606. [Google Scholar] [CrossRef]
- Shahar, S.; Adznam, S.N.A.; Lee, L.K.; Yusof, N.A.M.; Salleh, M.; Mohamed Sakian, N.I. A Nutrition Education Intervention for Anthropometric and Biochemical Profiles of Rural Older Malays with Metabolic Syndrome. Public Health Nurs. 2013, 30, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Murimi, M.W.; Kanyi, M.; Mupfudze, T.; Amin, M.R.; Mbogori, T.; Aldubayan, K. Factors Influencing Efficacy of Nutrition Education Interventions: A Systematic Review. J. Nutr. Educ. Behav. 2017, 49, 142–165. [Google Scholar] [CrossRef] [PubMed]
- Owusu-Addo, E.; Ofori-Asenso, R.; Batchelor, F.; Mahtani, K.; Brijnath, B. Effective Implementation Approaches for Healthy Ageing Interventions for Older People: A Rapid Review. Arch. Gerontol. Geriatr. 2021, 92, 104263. [Google Scholar] [CrossRef]
- Lopez-Moreno, J.; Quintana-Navarro, G.M.; Camargo, A.; Jimenez-Lucena, R.; Delgado-Lista, J.; Marin, C.; Tinahones, F.J.; Striker, G.E.; Roche, H.M.; Perez-Martinez, P.; et al. Dietary Fat Quantity and Quality Modifies Advanced Glycation End Products Metabolism in Patients with Metabolic Syndrome. Mol. Nutr. Food Res. 2017, 61, 1601029. [Google Scholar] [CrossRef]
- Lopez-Moreno, J.; Quintana-Navarro, G.M.; Delgado-Lista, J.; Garcia-Rios, A.; Delgado-Casado, N.; Camargo, A.; Perez-Martinez, P.; Striker, G.E.; Tinahones, F.J.; Perez-Jimenez, F.; et al. Mediterranean Diet Reduces Serum Advanced Glycation End Products and Increases Antioxidant Defenses in Elderly Adults: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2016, 64, 901–904. [Google Scholar] [CrossRef] [PubMed]
- Vlassara, H.; Cai, W.; Tripp, E.; Pyzik, R.; Yee, K.; Goldberg, L.; Tansman, L.; Chen, X.; Mani, V.; Fayad, Z.A.; et al. Oral AGE Restriction Ameliorates Insulin Resistance in Obese Individuals with the Metabolic Syndrome: A Randomised Controlled Trial. Diabetologia 2016, 59, 2181–2192. [Google Scholar] [CrossRef] [PubMed]
- Lotan, R.; Ganmore, I.; Shelly, S.; Zacharia, M.; Uribarri, J.; Beisswenger, P.; Cai, W.; Troen, A.M.; Beeri, M.S. Long Term Dietary Restriction of Advanced Glycation End-Products (Ages) in Older Adults with Type 2 Diabetes Is Feasible and Efficacious-Results from a Pilot RCT. Nutrients 2020, 12, 3143. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Keogh, J.B.; Deo, P.; Clifton, P.M. Differential Effects of Dietary Patterns on Advanced Glycation End Products: A Randomized Crossover Study. Nutrients 2020, 12, 1767. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Effects of Two Different Dietary Patterns on Inflammatory Markers, Advanced Glycation End Products and Lipids in Subjects without Type 2 Diabetes: A Randomised Crossover Study. Nutrients 2017, 9, 336. [Google Scholar] [CrossRef] [PubMed]
- Sroga, G.E.; Stephen, S.J.; Wang, B.; Vashishth, D. Techniques for Advanced Glycation End Product Measurements for Diabetic Bone Disease: Pitfalls and Future Directions. Curr. Opin. Endocrinol. Diabetes Obes. 2022, 29, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, Y.; Toyoguchi, T.; Inage, K.; Fujimoto, K.; Orita, S.; Suzuki, M.; Kanamoto, H.; Abe, K.; Norimoto, M.; Umimura, T.; et al. Advanced Glycation End Products Are Associated with Sarcopenia in Older Women: Aging Marker Dynamics. J. Women Aging 2021, 33, 328–340. [Google Scholar] [CrossRef]
- Béjar, L.M.; Vázquez-Limón, E. ¿Hay Alguna Alternativa al Tradicional Cuestionario de Frecuencia de Consumo de Alimentos Para La Evaluación de La Ingesta Alimentaria Habitual? Nutr. Hosp. 2017, 34, 880–888. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week | 1 | 2 | 3 | 4 | |
|---|---|---|---|---|---|
| Classes | Mediterranean diet and healthy pantry | Gastro-healthy eating plate | Culinary techniques and AGEs | Food groups: vegetables and fruits, protein, and carbohydrates | |
| Pantry and shopping | Proportions of plate | Prevention of cooking formation of AGEs | Key aspects of each food group | ||
| Objectives | Learning organizational and planning guidelines in kitchen | Getting to know proportions of different food groups that healthy dishes should have based on “the healthy eating plate” | Getting to know AGEs and strategies to reduce these compounds in foods | Learning about different proportions of healthy eating plate | |
| Theoretical part | Gastronomic culture | Mediterranean diet and its benefits | Healthy eating plate | General information about AGEs, what they are, how they are formed, and their effect on health | Vegetables and fruits: benefits, bioactive compounds, and seasonality |
| Planning grocery shopping and its key aspects, such as how to read nutritional labels | Extra virgin olive oil: benefits and different types | Proteins: types and plant and animal protein sources | |||
| Carbohydrates: types, food sources, and how to identify whole foods | |||||
| Culinary resources | Basic equipment | Gastro-healthy eating plate | Strategies to reduce AGEs in foods | Culinary resources to prepare delicious vegetables and fruits | |
| Pantry: general preparations that boost flavour of plates | Healthy culinary techniques: blanching, boiling, poaching, sweating, grinding, pressure cooking, stewing, use of oven | Healthy culinary techniques: microwaving, papillote, steaming, salt cooking, marinating, pickling, fermenting, sprouting | Culinary resources for preparing delicious dishes based on animal and plant proteins | ||
| Healthy culinary techniques: importance of different cuts | Key culinary strategies: batch cooking | Culinary resources for preparing delicious carbohydrate-based dishes | |||
| How to use recipe books | |||||
| Cooking class | Aims | Preparation of sauces and pastas | Example of healthy eating plate and healthy dessert | Example of how to cook food using different culinary techniques to reduce formation of AGEs | Example of healthy eating plate with vegetal protein and animal protein. Marinating foods in acidic or citrus-based sauces |
| Recipes | Pesto Green curry Baba ganoush Harissa pasta Asian dressing | Vegetable salmorejo and wholegrain croutons. Ceviche of fruits. | Fish (mackerel) cooked using four culinary techniques: papillote, steaming, salt cooking, and marinating before microwaving | Seasoned boiled leeks, textured soy with garlic and quinoa. Carrots and marinated chicken in papillote with pesto and millet. | |
| Within-Group Changes (95% CI) | Difference in Changes between Groups (95% CI) | ||
|---|---|---|---|
| NIG (n = 26) | CIG (n = 30) | ||
| Global confidence about cooking at home a | 5.5 (−1.4 to 12.4) | 8.3 (2.8 to 13.7) ** | 2.8 (−6.1 to 11.5) |
| Confidence in the use of specific cooking techniques and skills a | |||
| Prepare food for cooking by chopping, mixing, and stirring | −0.2 (−0.9 to 0.5) | −0.1 (−1.1 to 0.9) | 0.1 (−1.1 to 1.3) |
| Use different methods to cook foods such as boiling | −0.1 (−0.4 to 0.3) | 0.3 (−0.7 to 1.2) | 0.3 (−0.7 to 1.3) |
| Use different equipment for cooking | 0.02 (−0.5 to 0.5) | 0.3 (−0.3 to 1.0) | 0.3 (−0.5 to 1.1) |
| Preserve food | 0.1 (−0.9 to 1.0) | 1.2 (0.1 to 2.3) * | 1.1 (−0.4 to 2.5) |
| Know when your food is cooked | 0.6 (−0.3 to 1.5) | 0.6 (−0.04 to 1.2) | −0.01 (−1.1 to 1.1) |
| Handle, store, and prepare foods safely b | 0.1 (−0.6 to 0.7) | −0.2 (−1.0 to 0.5) | −0.3 (−1.3 to 0.7) |
| Cook grains, for example rice, pasta, etc. | 0.2 (−0.4 to 0.7) | 0.3 (−0.4 to 1.0) | 0.1 (−0.7 to 1.0) |
| Cook vegetables | 0.1 (−0.3 to 0.4) | 0.3 (−0.2 to 0.8) | 0.3 (−0.3 to 0.8) |
| Cook meat, fish, or poultry | −0.1 (−0.6 to 0.6) | 0.1 (−0.4 to 0.5) | 0.1 (−0.6 to 0.8) |
| Prepare a balanced meal | 0.3 (−0.5 to 1.0) | 0.8 (0.3 to 1.3) ** | 0.5 (−0.4 to 1.4) |
| Prepare more than one food item for a meal at the same time | 0.4 (−0.1 to 1.0) | 0.5 (−0.1 to 1.1) | 0.1 (−0.7 to 0.9) |
| Compare food prices to save money b | 0.4 (−0.1 to 1.6) | 0.8 (0.01 to 1.6) * | 0.4 (−1.1 to 1.8) |
| Read the nutrition information on food labels | 0.3 (−0.4 to 1.0) | 0.5 (−0.2 to 1.2) | 0.2 (−0.8 to 1.2) |
| Plan meals for the week c | 0.3 (−0.6 to 1.2) | 1.5 (0.5 to 2.5) ** | 1.2 (−0.2 to 2.5) |
| Read recipes | −0.5 (−1.2 to 0.3) | 0.4 (−0.1 to 1.0) | 0.9 (−0.03 to 1.8) |
| Use substitutions in recipes if I do not have a specific ingredient | 0.5 (−0.5 to 1.5) | 0.8 (0.1 to 1.4) * | 0.3 (−0.9 to 1.4) |
| Change recipes to make them healthier | 1.0 (0.1 to 1.8) * | 0.7 (0.2 to 1.2) ** | −0.3 (−1.3 to 0.7) |
| Use leftovers to create another meal b | 0.3 (−0.5 to 1.1) | 0.7 (0.04 to 1.3) * | 0.3 (−0.7 to 1.3) |
| Within-Group Changes (95% CI) | Difference in Changes between Groups (95% CI) | ||
|---|---|---|---|
| NIG (n = 26) | CIG (n = 30) | ||
| Global attitude about cooking at home a | 1.3 (−5.7 to 8.3) | −1.8 (−11.3 to 7.6) | −3.2 (−14.9 to 8.6) |
| Attitude in the use of specific cooking techniques and skills a | |||
| I do NOT like to cook because it takes too much time. | 0.5 (−0.2 to 1.3) | 0.5 (−0.4 to 1.4) | −0.03 (−1.2 to 1.1) |
| Preparing meals at home would NOT improve my health. | 0.3 (−1.2 to 1.7) | −0.01 (−0.9 to 0.9) | −0.3 (−2.0 to 1.5) |
| Cooking meals is a good use of my time b. | −0.5 (−1.5 to 0.4) | 0.3 (−0.6 to 1.2) | 0.9 (−0.4 to 2.1) |
| I enjoy cooking. | 0.3 (−0.4 to 0.9) | −0.002 (−0.8 to 0.8) | −0.2 (−1.3 to 0.8) |
| It is important to know how to prepare food. | 0.2 (−0.5 to 0.9) | −0.1 (−1.0 to 0.9) | −0.3 (−1.5 to 0.9) |
| Cooking is fun. | 0.02 (−0.7 to 0.7) | 0.02 (−0.8 to 0.9) | 0.003 (−1.1 to 1.1) |
| I do NOT like to prepare meals at home because it costs too much money. | 0.4 (−0.7 to 1.4) | −0.7 (−1.4 to 0.04) | −1.0 (−2.3 to 0.2) |
| It is NOT important that I know how to cook. | 0.7 (−0.6 to 2.0) | −0.1 (−0.8 to 0.6) | −0.8 (−2.2 to 0.6) |
| Cooking is interesting. | −0.3 (−1.2 to 0.7) | −0.9 (−1.8 to −0.1) * | −0.7 (−1.9 to 0.6) |
| Meals made at home are affordable. | 0.3 (−0.7 to 1.2) | −0.5 (−1.2 to 0.3) | −0.7 (−1.9 to 0.5) |
| It is important to eat the recommended 3 portions of fruit each day. | −0.1 (−0.7 to 0.5) | −0.1 (−1.2 to 0.9) | −0.03 (−1.2 to 1.2) |
| It is important to eat the recommended 2 portions of vegetables each day. | 0.3 (−0.3 to 1.0) | 0.5 (−0.4 to 1.4) | 0.2 (−0.9 to 1.3) |
| It is easy to prepare meals. | 0.4 (−0.3 to 1.1) | −0.4 (−1.1 to 0.4) | −0.8 (−1.8 to 0.2) |
| Cooking is frustrating. | −0.2 (−1.1 to 0.7) | −0.4 (−1.2 to 0.4) | −0.2 (−1.3 to 1.0) |
| I like trying new recipes. | −0.8 (−1.6 to −0.1) * | −0.3 (−1.0 to 0.5) | 0.6 (−0.5 to 1.6) |
| It is too much work to cook. | 0.2 (−0.8 to 1.2) | −0.1 (−1.2 to 0.9) | −0.3 (−1.7 to 1.1) |
| Making meals at home helps me to eat more healthily. | 0.03 (−0.6 to 0.7) | 0.5 (−0.4 to 1.4) | 0.5 (−0.6 to 1.5) |
| I find cooking tiring. | −0.2 (−1.0 to 0.5) | −0.6 (−1.3 to 0.1) | −0.4 (−1.4 to 0.7) |
| Within-Group Changes (95% CI) | Difference in Changes between Groups (95% CI) | ||
|---|---|---|---|
| NIG (n = 25) | CIG (n = 31) | ||
| Weight (kg) | −0.2 (−0.7 to 0.3) | −1.7 (−2.6 to −0.9) *** | −1.5 (−2.5 to −0.5) ** |
| BMI (kg/m2) | −0.1 (−0.3 to 0.1) | −0.6 (−0.9 to −0.3) *** | −0.5 (−0.8 to −0.2) ** |
| Waist circumference (cm) | −1.0 (−1.8 to −0.3) ** | −2.4 (−3.4 to −1.4) *** | −1.4 (−2.6 to −0.2) * |
| Hip circumference (cm) | −0.6 (−1.2 to 0.1) | −2.0 (−2.8 to −1.2) *** | −1.4 (−2.4 to −0.4) ** |
| Waist/hip ratio | −0.004 (−0.01 to 0.002) | −0.004 (−0.02 to 0.01) | 0.0001 (−0.01 to 0.01) |
| Fat mass (kg) | 1.9 (0.6 to 3.2) ** | 0.2 (−1.2 to 1.6) | −1.7 (−3.6 to 0.3) |
| Fat mass (%) | 2.2 (0.8 to 3.7) ** | 0.5 (−1.0 to 1.9) | −1.7 (−3.8 to 0.3) |
| Fat-free mass (kg) | −1.3 (−3.2 to 0.6) * | −1.8 (−3.5 to −0.2) * | −0.5 (−3.1 to 2.0) |
| Fat-free mass (%) | −2.3 (−3.7 to −0.8) ** | 0.5 (−2.0 to 3.0) | 2.8 (−0.1 to 5.6) |
| SBP (mmHg) a | −1.2 (−6.7 to 4.3) | −7.3 (−12.5 to −2.2) ** | −6.1 (−13.7 to 1.4) |
| DBP (mmHg) a | −1.8 (−4.2 to 0.6) | −3.8 (−6.4 to −1.3) ** | −2.0 (−5.6 to 1.5) |
| Within-Group Changes (95% CI) | Difference in Changes between Groups (95% CI) | ||
|---|---|---|---|
| NIG (n = 23) | CIG (n = 26) | ||
| Glucose (mg/dL) | −0.4 (−3.0 to 2.2) | −4.4 (−7.8 to −1.0) * | −4.0 (−8.3 to 0.3) |
| Insulin (mcU/mL) | 0.3 (−0.6 to 1.2) | −0.4 (−2.0 to 1.2) | −0.7 (−2.5 to 1.1) |
| HOMA-IR | 0.02 (−0.2 to 0.3) | −0.2 (−0.8 to 0.3) | −0.3 (−0.9 to 0.4) |
| Total cholesterol (mg/dL) | 3.7 (−6.3 to 13.6) | 1.7 (−7.2 to 10.5) | −2.0 (−15.3 to 11.3) |
| HDL-c (mg/dL) | −1.1 (−3.3 to 1.1) | −2.1 (−5.0 to 0.8) | −1.0 (−4.7 to 2.6) |
| LDL-c (mg/dL) | 5.4 (−2.2 to 13.0) | 5.0 (−1.9 to 11.8) | −0.4 (−10.6 to 9.8) |
| TG (mg/dL) | −4.8 (−22.8 to 13.2) | −5.1 (−19.4 to 9.2) | −0.3 (−23.3 to 22.7) |
| LDL-c/HDL-c | 0.1 (0.02 to 0.2) * | 0.2 (0.03 to 0.3) * | 0.03 (−0.1 to 0.2) |
| TG/HDL-c | 0.01 (−0.4 to 0.4) | −0.04 (−0.4 to 0.3) | −0.1 (−0.6 to 0.4) |
| CRP (pg/dL) | 0.1 (−0.1 to 0.2) | 0.1 (−0.1 to 0.2) | −0.002 (−0.2 to 0.2) |
| TNF-α (mg/dL) | 6.6 (0.1 to 13.1) * | 7.4 (2.3 to 12.5) ** | 0.8 (−7.5 to 9.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domper, J.; Gayoso, L.; Goni, L.; Perezábad, L.; Razquin, C.; de la O, V.; Etxeberria, U.; Ruiz-Canela, M. An Intensive Culinary Intervention Programme to Promote Healthy Ageing: The SUKALMENA-InAge Feasibility Pilot Study. Nutrients 2024, 16, 1735. https://doi.org/10.3390/nu16111735
Domper J, Gayoso L, Goni L, Perezábad L, Razquin C, de la O V, Etxeberria U, Ruiz-Canela M. An Intensive Culinary Intervention Programme to Promote Healthy Ageing: The SUKALMENA-InAge Feasibility Pilot Study. Nutrients. 2024; 16(11):1735. https://doi.org/10.3390/nu16111735
Chicago/Turabian StyleDomper, Jara, Lucía Gayoso, Leticia Goni, Laura Perezábad, Cristina Razquin, Victor de la O, Usune Etxeberria, and Miguel Ruiz-Canela. 2024. "An Intensive Culinary Intervention Programme to Promote Healthy Ageing: The SUKALMENA-InAge Feasibility Pilot Study" Nutrients 16, no. 11: 1735. https://doi.org/10.3390/nu16111735
APA StyleDomper, J., Gayoso, L., Goni, L., Perezábad, L., Razquin, C., de la O, V., Etxeberria, U., & Ruiz-Canela, M. (2024). An Intensive Culinary Intervention Programme to Promote Healthy Ageing: The SUKALMENA-InAge Feasibility Pilot Study. Nutrients, 16(11), 1735. https://doi.org/10.3390/nu16111735