
Micronutrient Status in Pregnant Women after Metabolic Bariatric Surgery in the United Arab Emirates: A Prospective Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
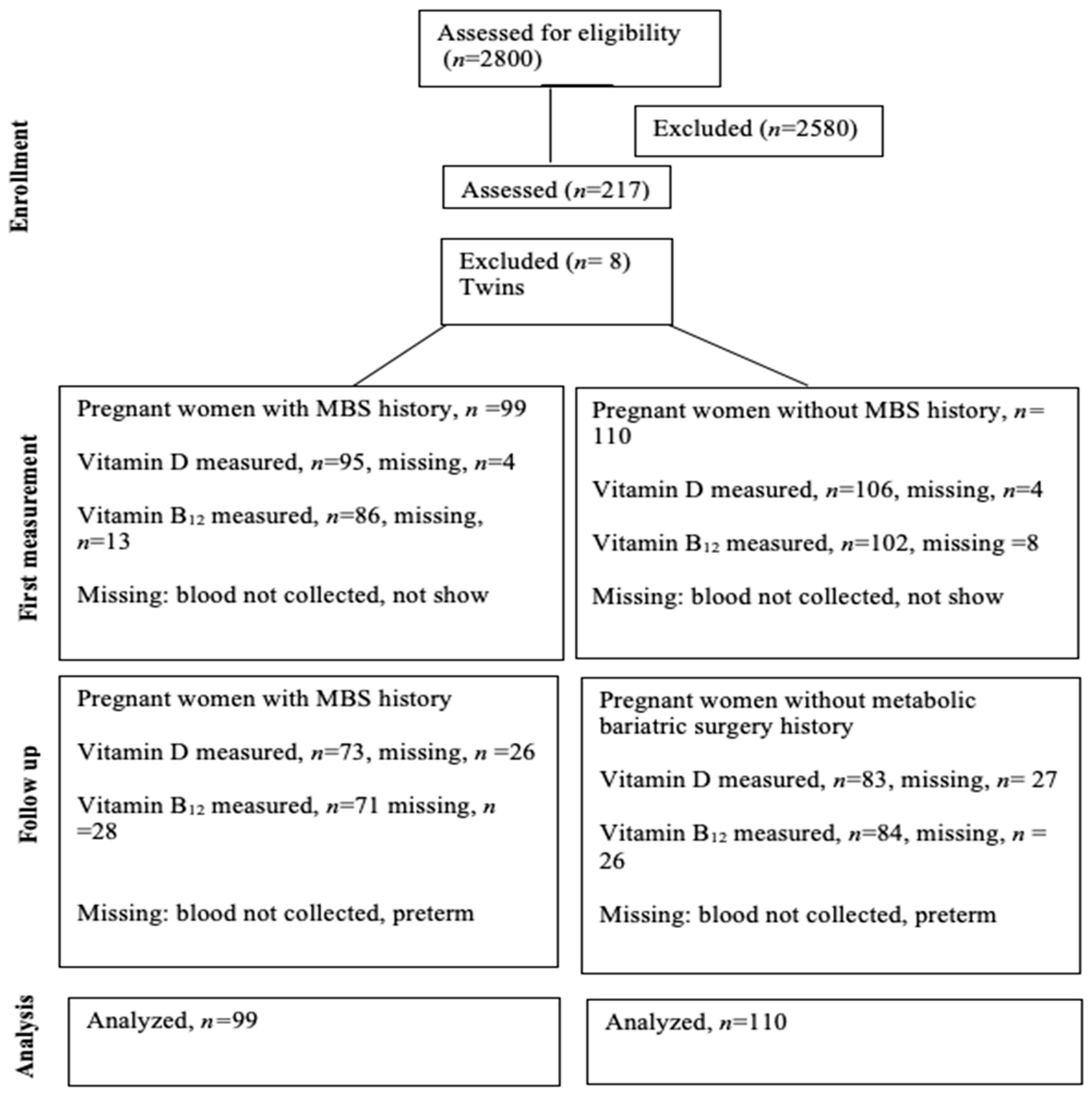
2.2. Setting and Participants
2.3. Data Collection
2.4. Sample Size
2.5. Ethics Approval
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guelinckx, I.; Devlieger, R.; Vansant, G. Reproductive outcome after bariatric surgery: A critical review. Hum. Reprod. Update 2009, 15, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.L.; Mooney, A.; Gonzalvo, J.P. Bariatric Surgery. Adv. Pediatr. 2017, 64, 269–283. [Google Scholar] [CrossRef] [PubMed]
- English, W.J.; DeMaria, E.J.; Brethauer, S.A.; Mattar, S.G.; Rosenthal, R.J.; Morton, J.M. American Society for Metabolic and Bariatric Surgery estimation of metabolic and bariatric procedures performed in the United States in 2016. Surg. Obes. Relat. Dis. 2018, 14, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Cummings, D.E.; Weigle, D.S.; Frayo, R.S.; Breen, P.A.; Ma, M.K.; Dellinger, E.P.; Purnell, J.Q. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N. Engl. J. Med. 2002, 346, 1623–1630. [Google Scholar] [CrossRef] [PubMed]
- Zandi-Nejad, K.; Luyckx, V.A.; Brenner, B.M. Adult hypertension and kidney disease: The role of fetal programming. Hypertension 2006, 47, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Argeri, R.; Thomazini, F.; Lichtenecker, D.C.K.; Thieme, K.; do Carmo Franco, M.; Gomes, G.N. Programmed Adult Kidney Disease: Importance of Fetal Environment. Front. Physiol. 2020, 11, 586290. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Bagby, S.P.; Hanson, M.A. Mechanisms of disease: In utero programming in the pathogenesis of hypertension. Nat. Clin. Pract. Nephrol. 2006, 2, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Nesterenko, T.H.; Aly, H. Fetal and neonatal programming: Evidence and clinical implications. Am. J. Perinatol. 2009, 26, 191–198. [Google Scholar] [CrossRef]
- Tobi, E.W.; Goeman, J.J.; Monajemi, R.; Gu, H.; Putter, H.; Zhang, Y.; Slieker, R.C.; Stok, A.P.; Thijssen, P.E.; Müller, F.; et al. DNA methylation signatures link prenatal famine exposure to growth and metabolism. Nat. Commun. 2014, 5, 5592. [Google Scholar] [CrossRef]
- Fernandez-Twinn, D.S.; Hjort, L.; Novakovic, B.; Ozanne, S.E.; Saffery, R. Intrauterine programming of obesity and type 2 diabetes. Diabetologia 2019, 62, 1789–1801. [Google Scholar] [CrossRef]
- Shiell, A.W.; Campbell, D.M.; Hall, M.H.; Barker, D.J. Diet in late pregnancy and glucose-insulin metabolism of the offspring 40 years later. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Imhoff-Kunsch, B.; Girard, A.W. Biological mechanisms for nutritional regulation of maternal health and fetal development. Paediatr. Perinat. Epidemiol. 2012, 26 (Suppl. S1), 4–26. [Google Scholar] [CrossRef] [PubMed]
- Georgieff, M.K.; Ramel, S.E.; Cusick, S.E. Nutritional influences on brain development. Acta Paediatr. 2018, 107, 1310–1321. [Google Scholar] [CrossRef] [PubMed]
- Ducarme, G.; Planche, L.; Abet, E.; Desroys du Roure, V.; Ducet-Boiffard, A. A Prospective Study of Association of Micronutrients Deficiencies during Pregnancy and Neonatal Outcome among Women after Bariatric Surgery. J. Clin. Med. 2021, 10, 204. [Google Scholar] [CrossRef] [PubMed]
- Akhter, Z.; Heslehurst, N.; Ceulemans, D.; Rankin, J.; Ackroyd, R.; Devlieger, R. Pregnancy after Bariatric Surgery: A Nested Case-Control Study of Risk Factors for Small for Gestational Age Babies in AURORA. Nutrients 2021, 13, 1699. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.K.; Braun, E.; Semons-Booker, K.; Lak, K.; Cruz, M.; Wlodarczyk, K. Vitamin Deficiency After Bariatric Surgery and Pregnancy Outcomes [39D]. Obstet. Gynecol. 2020, 135, 49S. [Google Scholar] [CrossRef]
- Watanabe, A.; Seki, Y.; Haruta, H.; Kikkawa, E.; Kasama, K. Maternal impacts and perinatal outcomes after three types of bariatric surgery at a single institution. Arch. Gynecol. Obstet. 2019, 300, 145–152. [Google Scholar] [CrossRef]
- Al-Mutawa, A.; Al-Sabah, S.; Anderson, A.K.; Al-Mutawa, M. Evaluation of Nutritional Status Post Laparoscopic Sleeve Gastrectomy—5-Year Outcomes. Obes. Surg. 2018, 28, 1473–1483. [Google Scholar] [CrossRef]
- Coupaye, M.; Legardeur, H.; Sami, O.; Calabrese, D.; Mandelbrot, L.; Ledoux, S. Impact of Roux-en-Y gastric bypass and sleeve gastrectomy on fetal growth and relationship with maternal nutritional status. Surg. Obes. Relat. Dis. 2018, 14, 1488–1494. [Google Scholar] [CrossRef]
- Costa, M.M.; Belo, S.; Souteiro, P.; Neves, J.S.; Magalhães, D.; Silva, R.B.; Oliveira, S.C.; Freitas, P.; Varela, A.; Queirós, J.; et al. Pregnancy after bariatric surgery: Maternal and fetal outcomes of 39 pregnancies and a literature review. J. Obstet. Gynaecol. Res. 2018, 44, 681–690. [Google Scholar] [CrossRef]
- Guthrie, T.M.; Dix, C.F.; Truby, H.; Kumar, S.; de Jersey, S.J. A Systematic Review Investigating Maternal Nutrition During Pregnancy After Bariatric Surgery. Obes. Surg. 2023, 33, 1857–1865. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, K.; Stojanovska, L.; Prakash, M.; Apostolopoulos, V. The effects of vitamin B on the immune/cytokine network and their involvement in depression. Maturitas 2017, 96, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.J.; Perreault, M.; Mottola, M.F.; Atkinson, S.A. Diet in Early Pregnancy: Focus on Folate, Vitamin B12, Vitamin D, and Choline. Can. J. Diet. Pract. Res. 2020, 81, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Sinclair, K.D. One-carbon metabolism and epigenetic regulation of embryo development. Reprod. Fertil. Dev. 2015, 27, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Hildreth, C.J. Maternal Iron Deficiency and the Risk of Schizophrenia in Offspring. JAMA 2008, 300, 2712. [Google Scholar]
- McArdle, H.J.; Gambling, L.; Kennedy, C. Iron deficiency during pregnancy: The consequences for placental function and fetal outcome. Proc. Nutr. Soc. 2014, 73, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Devlieger, R.; Guelinckx, I.; Jans, G.; Voets, W.; Vanholsbeke, C.; Vansant, G.; Laine, K. Micronutrient Levels and Supplement Intake in Pregnancy after Bariatric Surgery: A Prospective Cohort Study. PLoS ONE 2014, 9, e114192. [Google Scholar] [CrossRef] [PubMed]
- Dolin, C.D.; Chervenak, J.; Pivo, S.; Ude Welcome, A.; Kominiarek, M.A. Association between time interval from bariatric surgery to pregnancy and maternal weight outcomes. J. Matern. Fetal. Neonatal. Med. 2021, 34, 3285–3291. [Google Scholar] [CrossRef]
- AlMarri, F.; Al Sabah, S.; Al Haddad, E.; Vaz, J.D. A Call for More Research from the Arabian Gulf. Obes. Surg. 2017, 27, 2034–2043. [Google Scholar] [CrossRef]
- O’Kane, M.; Parretti, H.M.; Pinkney, J.; Welbourn, R.; Hughes, C.A.; Mok, J.; Walker, N.; Thomas, D.; Devin, J.; Coulman, K.D.; et al. British Obesity and Metabolic Surgery Society Guidelines on perioperative and postoperative biochemical monitoring and micronutrient replacement for patients undergoing bariatric surgery—2020 update. Obes. Rev. 2020, 21, e13087. [Google Scholar] [CrossRef]
- Gadgil, M.D.; Chang, H.Y.; Richards, T.M.; Gudzune, K.A.; Huizinga, M.M.; Clark, J.M.; Bennett, W.L. Laboratory testing for and diagnosis of nutritional deficiencies in pregnancy before and after bariatric surgery. J. Womens Health 2014, 23, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Bebber, F.E.; Rizzolli, J.; Casagrande, D.S.; Rodrigues, M.T.; Padoin, A.V.; Mottin, C.C.; Repetto, G. Pregnancy after Bariatric Surgery: 39 Pregnancies Follow-up in a Multidisciplinary Team. Obes. Surg. 2011, 21, 1546–1551. [Google Scholar] [CrossRef] [PubMed]
- González, I.; Rubio, M.A.; Cordido, F.; Bretón, I.; Morales, M.a.J.; Vilarrasa, N.; Monereo, S.; Lecube, A.; Caixàs, A.; Vinagre, I.; et al. Maternal and Perinatal Outcomes After Bariatric Surgery: A Spanish Multicenter Study. Obes. Surg. 2015, 25, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Rottenstreich, A.; Elazary, R.; Goldenshluger, A.; Pikarsky, A.J.; Elchalal, U.; Ben-Porat, T. Maternal nutritional status and related pregnancy outcomes following bariatric surgery: A systematic review. Surg. Obes. Relat. Dis. 2019, 15, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Ladipo, O.A. Nutrition in pregnancy: Mineral and vitamin supplements. Am. J. Clin. Nutr. 2000, 72, 280S–290S. [Google Scholar] [CrossRef] [PubMed]
- Wadhwani, N.S.; Pisal, H.R.; Mehendale, S.S.; Joshi, S.R. A prospective study of maternal fatty acids, micronutrients and homocysteine and their association with birth outcome. Matern. Child Nutr. 2015, 11, 559–573. [Google Scholar] [CrossRef] [PubMed]
- Aasheim, E.T.; Björkman, S.; Søvik, T.T.; Engström, M.; Hanvold, S.E.; Mala, T.; Olbers, T.; Bøhmer, T. Vitamin status after bariatric surgery: A randomized study of gastric bypass and duodenal switch. Am. J. Clin. Nutr. 2009, 90, 15–22. [Google Scholar] [CrossRef]
- Xanthakos, S.A. Nutritional deficiencies in obesity and after bariatric surgery. Pediatr. Clin. N. Am. 2009, 56, 1105–1121. [Google Scholar] [CrossRef]
- Lupoli, R.; Lembo, E.; Saldalamacchia, G.; Avola, C.K.; Angrisani, L.; Capaldo, B. Bariatric surgery and long-term nutritional issues. World J. Diabetes 2017, 8, 464–474. [Google Scholar] [CrossRef]
- Pereira-Santos, M.; Costa, P.R.; Assis, A.M.; Santos, C.A.; Santos, D.B. Obesity and vitamin D deficiency: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 341–349. [Google Scholar] [CrossRef]
- Vargas-Ruiz, A.G.; Hernández-Rivera, G.; Herrera, M.F. Prevalence of Iron, Folate, and Vitamin B12 Deficiency Anemia After Laparoscopic Roux-en-Y Gastric Bypass. Obes. Surg. 2008, 18, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Mead, N.C.; Sakkatos, P.; Sakellaropoulos, G.C.; Adonakis, G.L.; Alexandrides, T.K.; Kalfarentzos, F. Pregnancy outcomes and nutritional indices after 3 types of bariatric surgery performed at a single institution. Surg. Obes. Relat. Dis. 2014, 10, 1166–1173. [Google Scholar] [CrossRef] [PubMed]
- Ciangura, C.c.; Group, B.-M.; Coupaye, M.; Deruelle, P.; Gascoin, G.r.; Calabrese, D.; Cosson, E.; Ducarme, G.; Gaborit, B.; Lelièvre, B.; et al. Clinical Practice Guidelines for Childbearing Female Candidates for Bariatric Surgery, Pregnancy, and Post-partum Management After Bariatric Surgery. Obes. Surg. 2019, 29, 3722–3734. [Google Scholar] [CrossRef] [PubMed]
- Weng, T.C.; Chang, C.H.; Dong, Y.H.; Chang, Y.C.; Chuang, L.M. Anaemia and related nutrient deficiencies after Roux-en-Y gastric bypass surgery: A systematic review and meta-analysis. BMJ Open 2015, 5, e006964. [Google Scholar] [CrossRef] [PubMed]
- Kheniser, K.G.; Kashyap, S.R.; Schauer, P.R.; Lam, E.T.C.; Kullman, E.S. Prevalence of Anemia in Subjects Randomized into Roux-en-Y Gastric Bypass or Sleeve Gastrectomy. Obes. Surg. 2017, 27, 1381–1386. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.D.; Hammoud, A.O.; Davidson, L.E.; Laferrère, B.; Fraser, A.; Stanford, J.B.; Hashibe, M.; Greenwood, J.L.; Kim, J.; Taylor, D.; et al. Maternal and neonatal outcomes for pregnancies before and after gastric bypass surgery. Int. J. Obes. 2015, 39, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical practice guidelines for the perioperative nutrition, metabolic, and nonsurgical support of patients undergoing bariatric procedures—2019 update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Surg. Obes. Relat. Dis. 2020, 16, 175–247. [Google Scholar] [CrossRef] [PubMed]
- ACOG practice bulletin, no. 105: Bariatric surgery and pregnancy. Obs. Gynecol 2009, 113, 1405–1413. [Google Scholar] [CrossRef]
- Heber, D.; Greenway, F.L.; Kaplan, L.M.; Livingston, E.; Salvador, J.; Still, C. Endocrine and nutritional management of the post-bariatric surgery patient: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2010, 95, 4823–4843. [Google Scholar] [CrossRef]
- Yau, P.O.M.D.; Parikh, M.M.D.; Saunders, J.K.M.D.; Chui, P.M.D.; Zablocki, T.N.P.; Welcome, A.U.M.D. Pregnancy after bariatric surgery: The effect of time-to-conception on pregnancy outcomes. Surg. Obes. Relat. Dis. 2017, 13, 1899–1905. [Google Scholar] [CrossRef]
- Crusell, M.; Nilas, L.; Svare, J.; Lauenborg, J. A Time Interval of More Than 18 Months Between a Pregnancy and a Roux-en-Y Gastric Bypass Increases the Risk of Iron Deficiency and Anaemia in Pregnancy. Obes. Surg. 2016, 26, 2457–2462. [Google Scholar] [CrossRef] [PubMed]
- Malakauskienė, L.; Nadišauskienė, R.J.; Ramašauskaitė, D.; Bartusevičienė, E.; Ramonienė, G.; Maleckienė, L. Is it necessary to postpone pregnancy after bariatric surgery: A national cohort study. J. Obstet. Gynaecol. 2020, 40, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Bloomberg, R.D.; Fleishman, A.; Nalle, J.E.; Herron, D.M.; Kini, S. Nutritional deficiencies following bariatric surgery: What have we learned? Obes. Surg. 2005, 15, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Blume, C.A.; Boni, C.C.; Casagrande, D.S.; Rizzolli, J.; Padoin, A.V.; Mottin, C.C. Nutritional profile of patients before and after Roux-en-Y gastric bypass: 3-year follow-up. Obes. Surg. 2012, 22, 1676–1685. [Google Scholar] [CrossRef]
- Nomura, R.M.; Dias, M.C.; Igai, A.M.; Paiva, L.V.; Zugaib, M. Anemia during pregnancy after silastic ring Roux-en-Y gastric bypass: Influence of time to conception. Obes. Surg. 2011, 21, 479–484. [Google Scholar] [CrossRef]
- Stentebjerg, L.L.; Andersen, L.L.T.; Renault, K.; Støving, R.K.; Jensen, D.M. Pregnancy and perinatal outcomes according to surgery to conception interval and gestational weight gain in women with previous gastric bypass. J. Matern.-Fetal Neonatal Med. 2017, 30, 1182–1188. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total Population (n = 217) | Metabolic Bariatric Surgery (n = 105) | Non-Metabolic Bariatric Surgery (n = 112) | p Value |
|---|---|---|---|---|
| Age, years (mean ± SD) | 31.47 ± 5.62 years | 32.69 ± 5.13 years | 30.30 ± 5.84 years | 0.001 b |
| Age group, n (%) | 0.020 a | |||
| ≤35 years | 155 (71.4) | 68 (64.2) | 87 (78.4) | |
| >35 years | 62 (28.6) | 38 (35.8) | 24 (21.6) | |
| Nationality, n (%) | <0.001 a | |||
| Non-Emirati | 45 (20.7) | 9 (8.5) | 36 (32.4) | |
| Emirati | 172 (79.3) | 97 (91.5) | 75 (67.6) | |
| Educational level, n (%) | 0.406 a | |||
| High school | 50 (23) | 27 (25.5) | 23 (20.7) | |
| College | 167 (77) | 79 (74.5) | 88 (79.3) | |
| Working, n (%) | 0.040 a | |||
| No | 152 (70.4 | 67 (63.8) | 85 (76.6) | |
| Yes | 64 (29.6) | 38 (36.2) | 26 (23.4) | |
| Smoking, n (%) | 0.689 a | |||
| No | 212 (97.7) | 104 (98.1) | 108 (97.3) | |
| Yes | 5 (2.3) | 2 (1.9) | 3 (2.7) | |
| Pre-pregnancy BMI median (IQR), kg/m2 | 27.19 (24.22–30.49) kg/m2 | 28.74 (25.53–31.64) kg/m2 | 25.28 (23.71–29.27) kg/m2 | <0.001 c |
| IVF, n (%) | 0.132 a | |||
| No | 209 (96.3) | 100 (95.3) | 109 (98.2) | |
| Yes | 8 (3.7) | 6 (5.7) | 2 (1.8) | |
| Twins, n (%) | 0.017 a | |||
| No | 209 (96.3) | 99 (94.3) | 110 (98.2) | |
| Yes | 8 (3.7) | 6 (5.7) | 2 (1.8) | |
| Hypertension, n (%) | 0.376 a | |||
| No | 211 (97.2) | 102 (96.2) | 109 (98.2) | |
| Yes | 6 (2.8) | 4 (3.8) | 2 (1.8) | |
| Gestational diabetes, n (%) | 0.430 a | |||
| No | 148 (68.2) | 75 (70.8) | 73 (65.8) | |
| Yes | 69 (31.8) | 31 (29.2) | 38 (34.2) | |
| Hypothyroidism n, (%) | 0.088 a | |||
| No | 180 (86.1) | 81 (81.8) | 99 (90) | |
| Yes | 29 (13.9) | 18 (18.2) | 11 (10) |
| Variables | Reference | Metabolic Bariatric Surgery (n = 99) | Non-Metabolic Bariatric Surgery (n = 110) | p Value |
|---|---|---|---|---|
| First vitamin B12 blood level, median (IQR) | 187–883 pg/mL | 236 (186–307) pg/mL | 309 (242–388) pg/mL | < 0.001 c |
| Second vitamin B12 level, median (IQR) | 187–883 pg/mL | 221 (195–269) pg/mL | 254 (204–333) pg/mL | 0.034 c |
| Vitamin B12 deficiency during first blood collection (%) | <187 ng/mL | 24.4 | 3.9 | <0.001 b |
| Vitamin B12 deficiency during second blood collection (%) | <187 ng/mL | 19.2 | 15.5 | 0.453 b |
| First vitamin D level (mean ± SD) | 20–50 ng/mL | 22.66 ± 9.86 ng/mL | 27.90 ± 12.79 ng/mL | 0.001 b |
| Second vitamin D level (mean ± SD) | 20–50 ng/mL | 34.62 ± 11.87 ng/mL | 28.10 ± 11.28 ng/mL | <0.001 b |
| Vitamin D deficiency during first blood collection (%) | <20 ng/mL | 62.3 | 37.7 | 0.002 a |
| Vitamin D deficiency during second blood collection (%) | <20 ng/mL | 23.9 | 10.8 | 0.044 b |
| Hemoglobin level at booking (mean ± SD) | 11.6–15 g/dL | 10.96 ± 1.13 g/dL | 10.49 ±1.21 g/dL | 0.004 b |
| Low hemoglobin (%) | <11.6 g/dL | 80.8 | 66.4 | 0.021 a |
| Ferritin level at booking, median (IQR) | 4.63–204 ng/mL | 7.30 (4.93–12.35) | 7.31 (4.87–12.58) | 0.856 c |
| Low ferritin level (%) | <4.63 ng/mL | 57 | 42.3 | 0.838 |
| Serum iron level (mean ± SD) | 20–162 mg/dL | 57.47 ± 37.95 mg/dL | 46.67 ± 26.08 mg/dL | 0.298 b |
| Iron deficiency anemia, n (%) | 131(63.6) | 65 (67) | 66 (60.6) | 0.336 a |
| Iron infusion, n (%) | 103 (49.5) | 66 (67.3) | 37 (33.6) | <0.001 a |
| Vitamin B12 injection, n (%) | 25 (12.1) | 21 (21.6) | 4 (3.6) | <0.001 a |
| Variables | Reference | SG (n = 77) | RYGB (n = 22) | p-Value |
|---|---|---|---|---|
| First vitamin B12 level, median (IQR) | 187–883 pg/mL | 244 (191.5–330) pg/mL | 207 (182–275) pg/mL | 0.155 c |
| Second vitamin B12 level, median (IQR) | 187–883 pg/mL | 221 (198–269) pg/mL | 217 (176–352) pg/mL | 0.843 c |
| First vitamin D level (mean ± SD) | 20–50 ng/mL | 23.21 ± 9.30 ng/mL | 20.61 ± 11.75 ng/mL | 0.297 a |
| Second vitamin D level (mean ± SD) | 20–50 ng/mL | 29.40 ± 10.76 ng/mL | 23.89 ± 12.21 ng/mL | 0.079 a |
| Hemoglobin level (mean ± SD) | 11.6–15 g/dL | 10.57 ± 1.13 g/dL | 10.21 ± 1.48 g/dL | 0.234 a |
| Low hemoglobin, n (%) | <11.6 g/dL | 65 (84.4) | 18 (81.8) | 0.770 a |
| Ferritin level, median (IQR) | 4.63–204 ng/mL | 7.05 (4.73–13) ng/mL | 8.24 (5.29–12.63) ng/mL | 0.549 c |
| Low ferritin, n (%) | <4.63 ng/mL | 14 (26.9) | 3 (18.8) | 0.509 a |
| Serum iron level (mean ± SD) | 20–162 μg/dL | 49.32 ± 27.84 μg/dL | 36.60 ± 16.23 μg/dL | 0.343 a |
| Iron infusion, n (%) | 0.261 a | |||
| Yes | 54 (71.1) | 12 (57.1) | ||
| No | 23 (29.9) | 9 (42.9) | ||
| Viatmin B12 injection, n(%) | 0.149 a | |||
| Yes | 14 (18.4) | 7 (33.3) | ||
| No | 62 (81.6) | 14 (66.7) |
| Variables | Reference | ≤18 Months (n = 49) | >18 Months (n = 50) | p Value |
|---|---|---|---|---|
| First vitamin B12 blood level, median (IQR) | 187–883 pg/mL | 233 (185.75–299) pg/mL | 237 (186–358) pg/mL | 0.966 c |
| Second vitamin B12 level, median (IQR) | 187–883 pg/mL | 232 (198–325) pg/mL | 216 (192–251) pg/mL | 0.125 c |
| First vitamin D level (mean ± SD) | 20–50 ng/mL | 22.94 ± 10.01 ng/mL | 22.40 ± 9.80 ng/mL | 0.791 b |
| Second vitamin D level (mean ± SD) | 20–50 ng/mL | 27.70 ± 10.91 ng/mL | 28.50 ± 11.83 ng/mL | 0.771 b |
| Hemoglobin level (mean ± SD) | 11.6–15 g/dL | 10.60 ± 1.22 g/dL | 10.38 ± 1.20 g/dL | 0.364 b |
| Ferritin level, median (IQR) | 4.63–204 ng/mL | 7.15 (4.5–11.66) ng/mL | 7.56 (4.94–15.95) ng/mL | 0.511 c |
| Ferritin deficiency, n (%) | <4.63 ng/mL | 27 (55.1) | 21 (42) | 0.419 a |
| Serum iron level (mean ± SD) | (20–162) µg/dL | 51.38 ± 25.40 µg/dL | 44.31 ± 26.92 µg/dL | 0.544 b |
| Iron deficiency anemia, n (%) | 0.221 a | |||
| Yes | 30 (61.2) | 35 (72.9) | ||
| No | 19 (38.8) | 13 (27.1) | ||
| Iron infusion, n (%) | 0.031 a | |||
| Yes | 28 (57.1) | 38 (77.6) | ||
| No | 21 (42.9) | 11 (22.4) | ||
| Vitamin B12 injection, n (%) | 0.847 a | |||
| Yes | 11 (22.4) | 10 (20.8) | ||
| No | 38 (77.6) | 38 (79.2) |
| Variables | Total Population (n = 209) | Metabolic Bariatric Surgery (n = 99) | Non-Metabolic Bariatric Surgery (n = 110) | p-Value |
|---|---|---|---|---|
| Oral iron, n (%) | ||||
| No | 163 (78) | 84 (84.8) | 79 (71.8) | 0.023 a |
| Yes | 46 (22) | 15 (15.2) | 31 (28.2) | |
| Vitamin D supplement, n (%) | ||||
| No | 137 (65.6) | 61 (61.6) | 76 (69.1) | 0.256 a |
| Yes | 72 (34.4) | 38 (38.4) | 34 (30.9) | |
| Pregnacare supplement, n (%) | ||||
| No | 63 (30.1) | 32 (32.3) | 31 (28.2) | 0.515 a |
| Yes | 146 (69.9) | 67 (67.7) | 79 (71.8) | |
| Folic acid supplement, n (%) | ||||
| No | 163 (78) | 74 (74.7) | 89 (80.9) | 0.283 a |
| Yes | 46 (22) | 25 (25.3) | 21 (19.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Mansoori, A.; Bataineh, M.F.; Al Momani, H.; Ali, H.I. Micronutrient Status in Pregnant Women after Metabolic Bariatric Surgery in the United Arab Emirates: A Prospective Study. Nutrients 2024, 16, 72. https://doi.org/10.3390/nu16010072
Al Mansoori A, Bataineh MF, Al Momani H, Ali HI. Micronutrient Status in Pregnant Women after Metabolic Bariatric Surgery in the United Arab Emirates: A Prospective Study. Nutrients. 2024; 16(1):72. https://doi.org/10.3390/nu16010072
Chicago/Turabian StyleAl Mansoori, Amna, Mo’ath F. Bataineh, Hazem Al Momani, and Habiba I. Ali. 2024. "Micronutrient Status in Pregnant Women after Metabolic Bariatric Surgery in the United Arab Emirates: A Prospective Study" Nutrients 16, no. 1: 72. https://doi.org/10.3390/nu16010072
APA StyleAl Mansoori, A., Bataineh, M. F., Al Momani, H., & Ali, H. I. (2024). Micronutrient Status in Pregnant Women after Metabolic Bariatric Surgery in the United Arab Emirates: A Prospective Study. Nutrients, 16(1), 72. https://doi.org/10.3390/nu16010072