


Preliminary Comparison of Fractional Absorption of Zinc Sulphate, Zinc Gluconate, and Zinc Aspartate after Oral Supple-Mentation in Healthy Human Volunteers



Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
- −
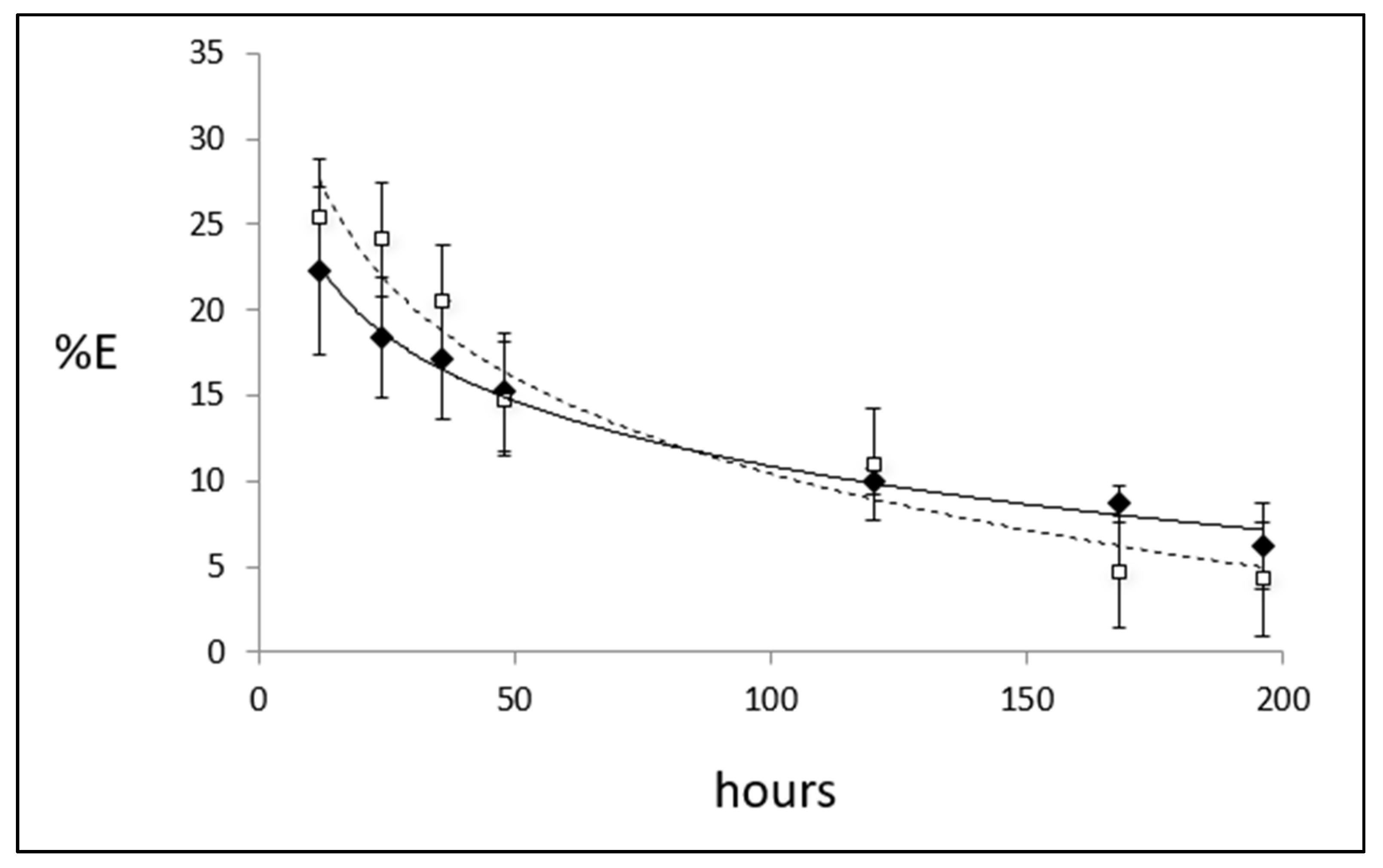
- The first phase aimed at evaluating the precision and accuracy of various isotopic ratios (66Zn/70Zn, 64Zn/70Zn and 68Zn/70Zn) in baseline urine samples, as well as comparing the kinetic dynamics of 70Zn isotopic enrichment (%E) in plasma and urine after oral administration of 2 mg 70ZnSO4. The results obtained in this phase were used to establish the best isotopic ratio used in the second phase.
- −
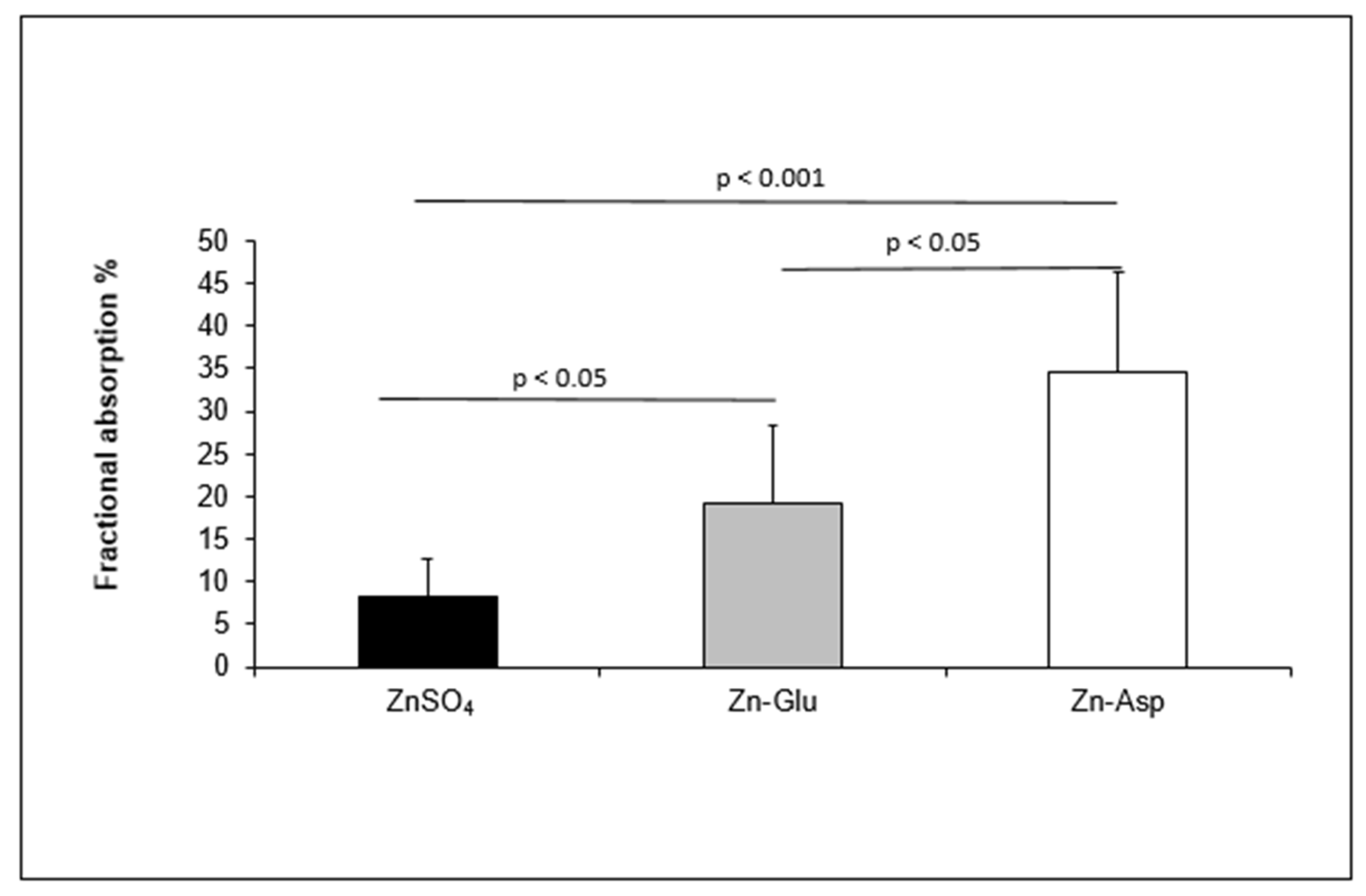
- The second phase aimed at measuring the FZA 48 h after the oral ingestion of 2 mg of 70Zn given in the form of three different complexes: 70Zn-Aspartate (Zn-Asp), 70Zn-Sulfate hydrate (70ZnSO4), and 70Zn-Gluconate (Zn-Glu). This phase was carried out 6 months after the first phase to evaluate any seasonal differences that could affect the %E of 70ZnSO4.
2.3. Materials
2.4. Procedure
2.4.1. Zn Determination in Urine and Plasma Samples
2.4.2. Determination of Zn Isotope Ratios in Urine and Plasma Samples
2.5. Isotopic Zn Absorption
2.6. Sample Size Detectable Difference
2.7. Statistical Analysis
3. Results
3.1. Basal Plasma Zn and Isotope Ratios
3.2. Kinetic of Isotopic Zn Enrichment
3.3. Isotopic Zn Absorption of Different Zn Complexes in Healthy Human Volunteers
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prasad, A.S. Zinc in Human Health: Effect of Zinc on Immune Cells. Mol. Med. 2008, 14, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.H.; Sermersheim, M.; Li, H.; Lee, P.H.U.; Steinberg, S.M.; Ma, J. Zinc in Wound Healing Modulation. Nutrients 2018, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- Rink, L.; Gabriel, P. Zinc and the Immune System. Proc. Nutr. Soc. 2000, 59, 541–552. [Google Scholar] [CrossRef]
- Shrimpton, R.; Gross, R.; Darnton-Hill, I.; Young, M. Zinc Deficiency: What Are the Most Appropriate Interventions? BMJ Br. Med. J. 2005, 330, 347. [Google Scholar] [CrossRef]
- Zinc-Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc-NCBI Bookshelf. Available online: https://www.ncbi.nlm.nih.gov/books/NBK222317/ (accessed on 2 March 2023).
- Fosmire, G.J. Zinc Toxicity. Am. J. Clin. Nutr. 1990, 51, 225–227. [Google Scholar] [CrossRef] [PubMed]
- International Zinc Nutrition Consultative Group (IZiNCG) Technical Document #1. Assessment of the Risk of Zinc Deficiency in Populations and Options for Its Control—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/18046856/ (accessed on 2 March 2023).
- Prasad, A.S. Zinc Is an Antioxidant and Anti-Inflammatory Agent: Its Role in Human Health. Front. Nutr. 2014, 1, 14. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.S.; Beck, F.W.J.; Bao, B.; Fitzgerald, J.T.; Snell, D.C.; Steinberg, J.D.; Cardozo, L.J. Zinc Supplementation Decreases Incidence of Infections in the Elderly: Effect of Zinc on Generation of Cytokines and Oxidative Stress. Am. J. Clin. Nutr. 2007, 85, 837–844. [Google Scholar] [CrossRef]
- Mocchegiani, E.; Romeo, J.; Malavolta, M.; Costarelli, L.; Giacconi, R.; Diaz, L.E.; Marcos, A. Zinc: Dietary Intake and Impact of Supplementation on Immune Function in Elderly. Age 2013, 35, 839–860. [Google Scholar] [CrossRef]
- Udechukwu, M.C.; Collins, S.A.; Udenigwe, C.C. Prospects of Enhancing Dietary Zinc Bioavailability with Food-Derived Zinc-Chelating Peptides. Food Funct. 2016, 7, 4137–4144. [Google Scholar] [CrossRef] [PubMed]
- Wegmüller, R.; Tay, F.; Zeder, C.; Brnić, M.; Hurrell, R.F. Zinc Absorption by Young Adults from Supplemental Zinc Citrate Is Comparable with That from Zinc Gluconate and Higher than from Zinc Oxide. J. Nutr. 2014, 144, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Solomons, N.W.; Romero-Abal, M.E.; Weiss, G.; Michalke, B.; Schümann, K. Bioavailability of Zinc from NutriSet Zinc Tablets Compared with Aqueous Zinc Sulfate. Eur. J. Clin. Nutr. 2011, 65, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.G.; King, J.C. Zinc Fortification: Current Trends and Strategies. Nutrients 2022, 14, 3895. [Google Scholar] [CrossRef]
- Brown, K.H.; De Romaña, D.L.; Arsenault, J.E.; Peerson, J.M.; Penny, M.E. Comparison of the Effects of Zinc Delivered in a Fortified Food or a Liquid Supplement on the Growth, Morbidity, and Plasma Zinc Concentrations of Young Peruvian Children. Am. J. Clin. Nutr. 2007, 85, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Rosado, J.L.; Cassís, L.; Solano, L.; Duarte-Vázquez, M.A. Nutrient Addition to Corn Masa Flour: Effect on Corn Flour Stability, Nutrient Loss, and Acceptability of Fortified Corn Tortillas. Food Nutr. Bull. 2005, 26, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Baqui, A.H.; Zaman, K.; Persson, L.A.; El Arifeen, S.; Yunus, M.; Begum, N.; Black, R.E. Simultaneous Weekly Supplementation of Iron and Zinc Is Associated with Lower Morbidity Due to Diarrhea and Acute Lower Respiratory Infection in Bangladeshi Infants. J. Nutr. 2003, 133, 4150–4157. [Google Scholar] [CrossRef] [PubMed]
- Baqui, A.H.; Black, R.E.; El Arifeen, S.; Yunus, M.; Chakraborty, J.; Ahmed, S.; Vaughan, J.P. Effect of Zinc Supplementation Started during Diarrhoea on Morbidity and Mortality in Bangladeshi Children: Community Randomised Trial. BMJ 2002, 325, 1059–1062. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, N.; Mazumder, S.; Taneja, S.; Dube, B.; Agarwal, R.C.; Mahalanabis, D.; Fontaine, O.; Black, R.E.; Bhan, M.K. Effectiveness of Zinc Supplementation plus Oral Rehydration Salts Compared with Oral Rehydration Salts Alone as a Treatment for Acute Diarrhea in a Primary Care Setting: A Cluster Randomized Trial. Pediatrics 2008, 121, e1279–e1285. [Google Scholar] [CrossRef] [PubMed]
- Afkhami-Ardekani, M.; Karimi, M.; Mohammadi, S.M.; Nourani, F. Effect of Sodium Metavanadate Supplementation on Lipid and Glucose Metabolism Biomarkers in Type 2 Diabetic Patients. Malays. J. Nutr. 2008, 14, 113–119. [Google Scholar]
- Siahbazi, S.; Behboudi-Gandevani, S.; Moghaddam-Banaem, L.; Montazeri, A. Effect of Zinc Sulfate Supplementation on Premenstrual Syndrome and Health-Related Quality of Life: Clinical Randomized Controlled Trial. J. Obstet. Gynaecol. Res. 2017, 43, 887–894. [Google Scholar] [CrossRef]
- Fortes, C.; Forastiere, F.; Agabiti, N.; Fano, V.; Pacifici, R.; Virgili, F.; Piras, G.; Guidi, L.; Bartoloni, C.; Tricerri, A.; et al. The Effect of Zinc and Vitamin A Supplementation on Immune Response in an Older Population. J. Am. Geriatr. Soc. 1998, 46, 19–26. [Google Scholar] [CrossRef]
- Nutritional Interactions of Zinc and Calcium—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/13823884/ (accessed on 3 March 2023).
- Blakeborough, P.; Salter, D.N.; Gurr, M.I. Zinc Binding in Cow’s Milk and Human Milk. Biochem. J. 1983, 209, 505. [Google Scholar] [CrossRef] [PubMed]
- Sandström, B.; Cederblad, Å.K.; Lönnerdal, B. Zinc Absorption from Human Milk, Cow’s Milk, and Infant Formulas. Am. J. Dis. Child. 1983, 137, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.S. Discovery of Zinc for Human Health and Biomarkers of Zinc Deficiency. In Molecular, Genetic, and Nutritional Aspects of Major and Trace Minerals; Academic Press: Cambridge, MA, USA, 2017; p. 241. [Google Scholar] [CrossRef]
- Pécoud, A.; Donzel, P.; Schelling, J.L. Effect of Foodstuffs on the Absorption of Zinc Sulfate. Clin. Pharmacol. Ther. 1975, 17, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Jalla, S.; Westcott, J.; Steirn, M.; Miller, L.V.; Bell, M.; Krebs, N.F. Zinc Absorption and Exchangeable Zinc Pool Sizes in Breast-Fed Infants Fed Meat or Cereal as First Complementary Food. J. Pediatr. Gastroenterol. Nutr. 2002, 34, 35–41. [Google Scholar] [CrossRef] [PubMed]
- De Moura, M.S.B.; Soares, N.R.M.; Barros, S.É.d.L.; de Pinho, F.A.; Silva, T.M.C.; Bráz, D.C.; Vieira, E.C.; Lima, M.M.; Parente, J.M.L.; Marreiro, D.d.N.; et al. Zinc Gluconate Supplementation Impacts the Clinical Improvement in Patients with Ulcerative Colitis. BioMetals 2020, 33, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Halim, M.M.; Ghavamzadeh, S.; Makhdoomi, K. Effect of Zinc Supplementation on Insulin Resistance, Lipid Profile, BMI in Type II Diabetic Patients. Indian J. Forensic Med. Toxicol. 2021, 15, 1487–1493. [Google Scholar] [CrossRef]
- Mocchegiani, E.; Giacconi, R.; Costarelli, L.; Muti, E.; Cipriano, C.; Tesei, S.; Pierpaoli, S.; Giuli, C.; Papa, R.; Marcellini, F.; et al. Zinc Deficiency and IL-6 -174G/C Polymorphism in Old People from Different European Countries: Effect of Zinc Supplementation. ZINCAGE Study. Exp. Gerontol. 2008, 43, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Faber, C.; Gabriel, P.; Ibs, K.H.; Rink, L. Zinc in Pharmacological Doses Suppresses Allogeneic Reaction without Affecting the Antigenic Response. Bone Marrow Transplant. 2004, 33, 1241–1246. [Google Scholar] [CrossRef]
- Sandstead, H.H.; Smith, J.C. Deliberations and Evaluations of Approaches, Endpoints and Paradigms for Determining Zinc Dietary Recommendations. J. Nutr. 1996, 126, 2410S–2418S. [Google Scholar] [CrossRef] [PubMed]
- Sauer, A.K.; Pfaender, S.; Hagmeyer, S.; Tarana, L.; Mattes, A.K.; Briel, F.; Küry, S.; Boeckers, T.M.; Grabrucker, A.M. Characterization of Zinc Amino Acid Complexes for Zinc Delivery in Vitro Using Caco-2 Cells and Enterocytes from HiPSC. Biometals 2017, 30, 643–661. [Google Scholar] [CrossRef] [PubMed]
- Maares, M.; Haase, H. A Guide to Human Zinc Absorption: General Overview and Recent Advances of In Vitro Intestinal Models. Nutrients 2020, 12, 762. [Google Scholar] [CrossRef] [PubMed]
- Hempe, J.M.; Cousins, R.J. Effect of EDTA and Zinc-Methionine Complex on Zinc Absorption by Rat Intestine. J. Nutr. 1989, 119, 1179–1187. [Google Scholar] [CrossRef]
- Wapnir, R.A.; Stiel, L. Zinc Intestinal Absorption in Rats: Specificity of Amino Acids as Ligands. J. Nutr. 1986, 116, 2171–2179. [Google Scholar] [CrossRef] [PubMed]
- Sandstrom, B.; Davidsson, L.; Cederblad, A.; Lonnerdal, B. Oral Iron, Dietary Ligands and Zinc Absorption. J. Nutr. 1985, 115, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Raffaniello, R.D.; Wapnir, R.A. Zinc Uptake by Isolated Rat Enterocytes: Effect of Low Molecular Weight Ligands. Proc. Soc. Exp. Biol. Med. 1989, 192, 219–224. [Google Scholar] [CrossRef]
- Schölmerich, J.; Freudemann, A.; Köttgen, E.; Wietholtz, H.; Steiert, B.; Löhle, E.; Häussinger, D.; Gerok, W. Bioavailability of Zinc from Zinc-Histidine Complexes. I. Comparison with Zinc Sulfate in Healthy Men. Am. J. Clin. Nutr. 1987, 45, 1480–1486. [Google Scholar] [CrossRef]
- Costarelli, L.; Giacconi, R.; Malavolta, M.; Basso, A.; Piacenza, F.; DeMartiis, M.; Giannandrea, E.; Renieri, C.; Busco, F.; Galeazzi, R.; et al. Effects of Zinc-Fortified Drinking Skim Milk (as Functional Food) on Cytokine Release and Thymic Hormone Activity in Very Old Persons: A Pilot Study. Age 2014, 36, 1421–1431. [Google Scholar] [CrossRef] [PubMed]
- Calculation of Zinc Absorption in Humans Using Tracers by Fecal Monitoring and a Compartmental Approach. Available online: https://agris.fao.org/agris-search/search.do?recordID=US9020768 (accessed on 3 March 2023).
- Friel, J.K.; Andrews, W.L.; Simmons, B.S.; Miller, L.V.; Longerich, H.P. Zinc Absorption in Premature Infants: Comparison of Two Isotopic Methods. Am. J. Clin. Nutr. 1996, 63, 342–347. [Google Scholar] [CrossRef]
- Yeung, G.S.; Schauer, C.S.; Zlotkin, S.H. Fractional Zinc Absorption Using a Single Isotope Tracer. Eur. J. Clin. Nutr. 2001, 55, 1098–1103. [Google Scholar] [CrossRef]
- Malavolta, M.; Costarelli, L.; Giacconi, R.; Muti, E.; Bernardini, G.; Tesei, S.; Cipriano, C.; Mocchegiani, E. Single and Three-Color Flow Cytometry Assay for Intracellular Zinc Ion Availability in Human Lymphocytes with Zinpyr-1 and Double Immunofluorescence: Relationship with Metallothioneins. Cytometry A 2006, 69, 1043–1053. [Google Scholar] [CrossRef]
- NDNS: Results from Years 1 to 4 (Combined)—GOV.UK. Available online: https://www.gov.uk/government/statistics/national-diet-and-nutrition-survey-results-from-years-1-to-4-combined-of-the-rolling-programme-for-2008-and-2009-to-2011-and-2012 (accessed on 28 March 2023).
- The Efficiency of Zinc-Aspartate Complex on Zinc Uptake in Plasma and Different Organs in Normal SD Rats -Molecular & Cellular Toxicology. Available online: https://koreascience.kr/article/JAKO200710736967409.j (accessed on 3 March 2023).
- Lönnerdal, B. Dietary Factors Influencing Zinc Absorption. J. Nutr. 2000, 130, 1378S–1383S. [Google Scholar] [CrossRef] [PubMed]
- Spencer, H.; Kramer, L.; Norris, C.; Osis, D. Effect of Calcium and Phosphorus on Zinc Metabolism in Man. Am. J. Clin. Nutr. 1984, 40, 1213–1218. [Google Scholar] [CrossRef]
- Dawson-Hughes, B.; Seligson, F.H.; Hughes, V.A. Effects of Calcium Carbonate and Hydroxyapatite on Zinc and Iron Retention in Postmenopausal Women. Am. J. Clin. Nutr. 1986, 44, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Giacconi, R.; Simm, A.; Santos, A.N.; Costarelli, L.; Malavolta, M.; Mecocci, P.; Piacenza, F.; Basso, A.; Fulop, T.; Rink, L.; et al. Influence of +1245 A/G MT1A Polymorphism on Advanced Glycation End-Products (AGEs) in Elderly: Effect of Zinc Supplementation. Genes Nutr. 2014, 9, 426. [Google Scholar] [CrossRef] [PubMed]
- Rosenkranz, E.; Metz, C.H.D.; Maywald, M.; Hilgers, R.D.; Weßels, I.; Senff, T.; Haase, H.; Jager, M.; Ott, M.; Aspinall, R.; et al. Zinc Supplementation Induces Regulatory T Cells by Inhibition of Sirt-1 Deacetylase in Mixed Lymphocyte Cultures. Mol. Nutr. Food Res. 2016, 60, 661–671. [Google Scholar] [CrossRef]
- Friel, J.K.; Naake, V.L.; Miller, L.V.; Fennessey, P.V.; Hambidge, K.M. The Analysis of Stable Isotopes in Urine to Determine the Fractional Absorption of Zinc. Am. J. Clin. Nutr. 1992, 55, 473–477. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Source | Type III Sum of Squares | F | Sig. * |
|---|---|---|---|
| Zn-Complex a | 2665.88 | 17.33 | <0.001 |
| Zn-Complex × Sex | 365.45 | 2.38 | 0.135 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piacenza, F.; Giacconi, R.; Costarelli, L.; Malavolta, M. Preliminary Comparison of Fractional Absorption of Zinc Sulphate, Zinc Gluconate, and Zinc Aspartate after Oral Supple-Mentation in Healthy Human Volunteers. Nutrients 2023, 15, 1885. https://doi.org/10.3390/nu15081885
Piacenza F, Giacconi R, Costarelli L, Malavolta M. Preliminary Comparison of Fractional Absorption of Zinc Sulphate, Zinc Gluconate, and Zinc Aspartate after Oral Supple-Mentation in Healthy Human Volunteers. Nutrients. 2023; 15(8):1885. https://doi.org/10.3390/nu15081885
Chicago/Turabian StylePiacenza, Francesco, Robertina Giacconi, Laura Costarelli, and Marco Malavolta. 2023. "Preliminary Comparison of Fractional Absorption of Zinc Sulphate, Zinc Gluconate, and Zinc Aspartate after Oral Supple-Mentation in Healthy Human Volunteers" Nutrients 15, no. 8: 1885. https://doi.org/10.3390/nu15081885
APA StylePiacenza, F., Giacconi, R., Costarelli, L., & Malavolta, M. (2023). Preliminary Comparison of Fractional Absorption of Zinc Sulphate, Zinc Gluconate, and Zinc Aspartate after Oral Supple-Mentation in Healthy Human Volunteers. Nutrients, 15(8), 1885. https://doi.org/10.3390/nu15081885