
Uncovering the Relationship between Selenium Status, Age, Health, and Dietary Habits: Insights from a Large Population Study including Nonagenarian Offspring from the MARK-AGE Project
 , ,
, ,  , ,
, ,  ,
,  , , , , , and
, , , , , and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population, Recruitment, Data and Blood Collection
2.2. Determination of Se in Plasma and Fractionation Analysis
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Levels of Plasma Se Concentrations According to Age and Demographics
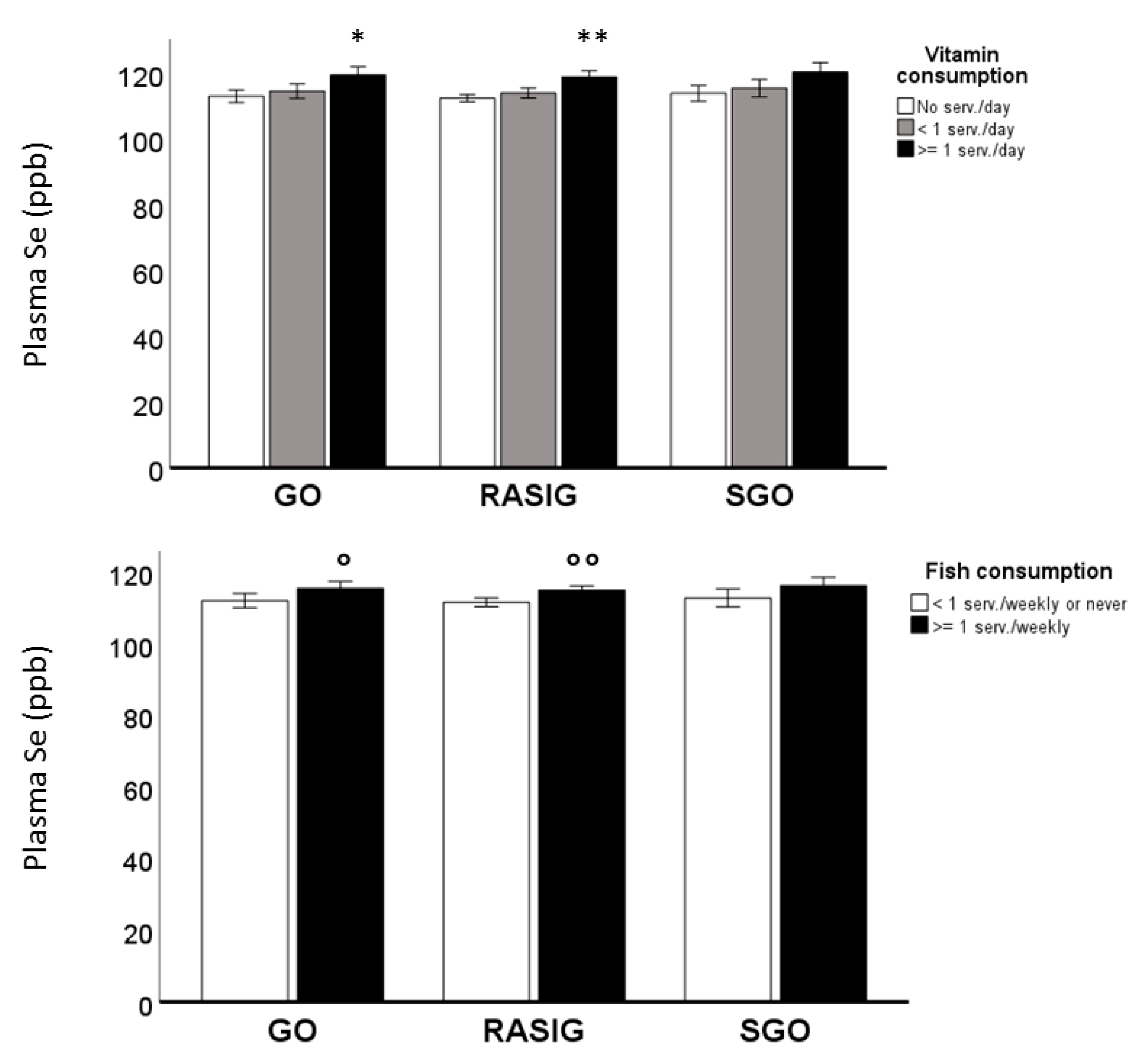
3.3. Influence of Dietary and Inherited Factors on Plasma Se Levels
3.4. Selenium Fractions in MARK-AGE Population
3.5. Association of Glucometabolic, Inflammatory, and Anti-Inflammatory Factors with Plasma Se Levels and Se2 Fraction
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roman, M.; Jitaru, P.; Barbante, C. Selenium biochemistry and its role for human health. Metallomics 2014, 6, 25–54. [Google Scholar] [CrossRef] [PubMed]
- Papp, L.V.; Lu, J.; Holmgren, A.; Khanna, K.K. From Selenium to Selenoproteins: Synthesis, Identity, and Their Role in Human Health. Antioxid. Redox Signal 2007, 9, 75–806. [Google Scholar] [CrossRef]
- Rayman, M.P. The importance of selenium to human health. Lancet 2000, 356, 33–241. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Giacconi, R.; Chiodi, L.; Boccoli, G.; Costarelli, L.; Piacenza, F.; Provinciali, M.; Malavolta, M. Reduced levels of plasma selenium are associated with increased inflammation and cardiovascular disease in an Italian elderly population. Exp. Gerontol. 2021, 145, 111219. [Google Scholar] [CrossRef]
- Food and Nutrition Board. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000. [Google Scholar] [CrossRef]
- Akbaraly, N.T.; Arnaud, J.; Hininger-Favier, I.; Gourlet, V.; Roussel, A.-M.; Berr, C. Selenium and mortality in the elderly: Results from the EVA study. Clin. Chem. 2005, 51, 2117–2123. [Google Scholar] [CrossRef]
- Alis, R.; Santos-Lozano, A.; Sanchis-Gomar, F.; Pareja-Galeano, H.; Fiuza-Luces, C.; Garatachea, N.; Lucia, A.; Emanuele, E. Trace elements levels in centenarian ‘dodgers’. J. Trace Elem. Med. Biol. 2016, 35, 103–106. [Google Scholar] [CrossRef]
- Mocchegiani, E.; Malavolta, M. Role of Zinc and Selenium in Oxidative Stress and Immunosenescence: Implications for Healthy Aging and Longevity. In Handbook of Immunosenescence; Springer International Publishing: Cham, Switzerland, 2018; pp. 1–35. [Google Scholar] [CrossRef]
- Robberecht, H.; De Bruyne, T.; Davioud-Charvet, E.; Mackrill, J.; Hermans, N. Selenium Status in Elderly People: Longevity and Age-Related Diseases. Curr. Pharm Des. 2019, 25, 1694–1706. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.D. Assessment of requirements for selenium and adequacy of selenium status: A review. Eur. J. Clin. Nutr. 2004, 58, 91–402. [Google Scholar] [CrossRef]
- Johnson, C.C.; Fordyce, F.M.; Rayman, M.P. Symposium on ‘Geographical and geological influences on nutrition’: Factors controlling the distribution of selenium in the environment and their impact on health and nutrition. Proc. Nutr. Soc. 2010, 69, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Alarcon, M.; Cabrera-Vique, C. Selenium in food and the human body: A review. Sci. Total Environ. 2008, 400, 115–141. [Google Scholar] [CrossRef]
- Mocchegiani, E.; Costarelli, L.; Giacconi, R.; Malavolta, M.; Basso, A.; Piacenza, F.; Ostan, R.; Cevenini, E.; Gonos, E.S.; Monti, D. Micronutrient-gene interactions related to inflammatory/immune response and antioxidant activity in ageing and inflammation. A systematic review. Mech. Ageing Dev. 2014, 136–137, 29–49. [Google Scholar] [CrossRef] [PubMed]
- Weekley, C.M.; Harris, H.H. Which form is that? The importance of selenium speciation and metabolism in the prevention and treatment of disease. Chem. Soc. Rev. 2013, 42, 870. [Google Scholar] [CrossRef]
- Kryukov, G.V.; Castellano, S.; Novoselov, S.V.; Lobanov, A.V.; Zehtab, O.; Guigó, R.; Gladyshev, V.N. Characterization of mammalian selenoproteomes. Science 2003, 300, 439–1443. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo Busto, M.E.; Oster, C.; Cuello-Nuñez, S.; Deitrich, C.L.; Raab, A.; Konopka, A.; Lehmann, W.D.; Goenaga-Infante, H.; Fisicaro, P. Accurate quantification of selenoproteins in human plasma/serum by isotope dilution ICP-MS: Focus on selenoprotein P. J. Anal. Spectrom. 2016, 31, 1904–1912. [Google Scholar] [CrossRef]
- Alehagen, U.; Opstad, T.B.; Alexander, J.; Larsson, A.; Aaseth, J. Impact of Selenium on Biomarkers and Clinical Aspects Related to Ageing. Rev. Biomol. 2021, 11, 1478. [Google Scholar] [CrossRef]
- Forte, G.; Deiana, M.; Pasella, S.; Baralla, A.; Occhineri, P.; Mura, I.; Madeddu, R.; Muresu, E.; Sotgia, S.; Zinellu, A.; et al. Metals in plasma of nonagenarians and centenarians living in a key area of longevity. Exp. Gerontol. 2014, 60, 197–206. [Google Scholar] [CrossRef]
- de González Vega, R.; Fernández-Sánchez, M.L.; González Iglesias, H.; Coca Prados, M.; Sanz-Medel, A. Quantitative selenium speciation by HPLC-ICP-MS(IDA) and simultaneous activity measurements in human vitreous humor. Anal. Bioanal. Chem. 2015, 407, 2405–2413. [Google Scholar] [CrossRef] [PubMed]
- Michalke, B.; Berthele, A. Contribution to selenium speciation in cerebrospinal fluid samples. J. Anal. At. Spectrom. 2011, 26, 165–170. [Google Scholar] [CrossRef]
- Vinceti, M.; Grill, P.; Malagoli, C.; Filippini, T.; Storani, S.; Malavolti, M.; Michalke, B. Selenium speciation in human serum and its implications for epidemiologic research: A cross-sectional study. J. Trace Elem. Med. Biol. 2015, 31, 1–10. [Google Scholar] [CrossRef]
- Malavolta, M.; Piacenza, F.; Basso, A.; Giacconi, R.; Costarelli, L.; Pierpaoli, S.; Mocchegiani, E. Speciation of trace elements in human serum by micro anion exchange chromatography coupled with inductively coupled plasma mass spectrometry. Anal. Biochem. 2012, 421, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Bürkle, A.; Moreno-Villanueva, M.; Bernhard, J.; Blasco, M.; Zondag, G.; Hoeijmakers, J.H.; Toussaint, O.; Grubeck-Loebenstein, B.; Mocchegiani, E.; Collino, S.; et al. MARK-AGE biomarkers of ageing. Mech. Ageing Dev. 2015, 151, 2–12. [Google Scholar] [CrossRef]
- Capri, M.; Moreno-Villanueva, M.; Cevenini, E.; Pini, E.; Scurti, M.; Borelli, V.; Palmas, M.G.; Zoli, M.; Schön, C.; Siepelmeyer, A.; et al. MARK-AGE population: From the human model to new insights. Mech. Ageing Dev. 2015, 151, 13–17. [Google Scholar] [CrossRef]
- Moreno-Villanueva, M.; Capri, M.; Breusing, N.; Siepelmeyer, A.; Sevini, F.; Ghezzo, A.; de Craen, A.J.M.; Hervonen, A.; Hurme, M.; Schön, C.; et al. MARK-AGE standard operating procedures (SOPs): A successful effort. Mech. Ageing Dev. 2015, 151, 18–25. [Google Scholar] [CrossRef]
- Moreno-Villanueva, M.; Kötter, T.; Sindlinger, T.; Baur, J.; Oehlke, S.; Bürkle, A.; Berthold, M.R. The MARK-AGE phenotypic database: Structure and strategy. Mech. Ageing Dev. 2015, 151, 26–30. [Google Scholar] [CrossRef]
- Franceschi, C.; Bezrukov, V.; Blanché, H.; Bolund, L.; Christensen, K.; de Benedictis, G.; Deiana, L.; Gonos, E.; Hervonen, A.; Yang, H.; et al. Genetics of healthy aging in Europe: The EU-integrated project GEHA (GEnetics of Healthy Aging). Ann. N. Y. Acad. Sci. 2007, 1100, 21–45. [Google Scholar] [CrossRef] [PubMed]
- Ciccarone, F.; Malavolta, M.; Calabrese, R.; Guastafierro, T.; Bacalini, M.G.M.G.; Reale, A.; Franceschi, C.; Capri, M.; Hervonen, A.; Hurme, M.; et al. Age-dependent expression of DNMT1 and DNMT3B in PBMCs from a large European population enrolled in the MARK-AGE study. Aging Cell 2016, 15, 755–765. [Google Scholar] [CrossRef]
- Joy, E.J.M.; Kalimbira, A.A.; Sturgess, J.; Banda, L.; Chiutsi-Phiri, G.; Manase, H.; Gondwe, J.; Ferguson, E.L.; Kalumikiza, Z.; Bailey, E.H.; et al. Biofortified Maize Improves Selenium Status of Women and Children in a Rural Community in Malawi: Results of the Addressing Hidden Hunger with Agronomy Randomized Controlled Trial. Front Nutr. 2022, 8, 788096. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Salisbury, C.; Graham, R.; Lyons, G.; Fenech, M. Increased consumption of wheat biofortified with selenium does not modify biomarkers of cancer risk, oxidative stress, or immune function in healthy Australian males. Env. Mol. Mutagen. 2009, 50, 489–501. [Google Scholar] [CrossRef]
- Stoffaneller, R.; Morse, N.L.A. Review of dietary selenium intake and selenium status in Europe and the Middle East. Nutrients 2015, 7, 1494–1537. [Google Scholar] [CrossRef]
- D’Amato, R.; Regni, L.; Falcinelli, B.; Mattioli, S.; Benincasa, P.; Dal Bosco, A.; Pacheco, P.; Proietti, P.; Troni, E.; Santi, C.; et al. Current Knowledge on Selenium Biofortification to Improve the Nutraceutical Profile of Food: A Comprehensive Review. J. Agric. Food Chem. 2020, 68, 4075–4097. [Google Scholar] [CrossRef] [PubMed]
- Baudry, J.; Kopp, J.F.; Boeing, H.; Kipp, A.P.; Schwerdtle, T.; Schulze, M.B. Changes of trace element status during aging: Results of the EPIC-Potsdam cohort study. Eur. J. Nutr. 2020, 59, 3045–3058. [Google Scholar] [CrossRef]
- Lv, Y.; Wei, Y.; Zhou, J.; Xue, K.; Guo, Y.; Liu, Y.; Ju, A.; Wu, B.; Zhao, F.; Chen, C.; et al. Human biomonitoring of toxic and essential metals in younger elderly, octogenarians, nonagenarians and centenarians: Analysis of the Healthy Ageing and Biomarkers Cohort Study (HABCS) in China. Environ. Int. 2021, 156, 106717. [Google Scholar] [CrossRef]
- Zhou, X.; Smith, A.M.; Failla, M.L.; Hill, K.E.; Yu, Z. Estrogen status alters tissue distribution and metabolism of selenium in female rats. J. Nutr. Biochem. 2012, 23, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Berr, C.; Akbaraly, T.; Arnaud, J.; Hininger, I.; Roussel, A.M.; Barberger Gateau, P. Increased selenium intake in elderly high fish consumers may account for health benefits previously ascribed to omega-3 fatty acids. J. Nutr. Health Aging 2009, 3, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Filippini, T.; Michalke, B.; Wise, L.A.; Malagoli, C.; Malavolti, M.; Vescovi, L.; Salvia, C.; Bargellini, A.; Sieri, S.; Krogh, V.; et al. Diet composition and serum levels of selenium species: A cross-sectional study. Food Chem. Toxicol. 2018, 115, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Piacenza, F.; Giacconi, R.; Costarelli, L.; Basso, A.; Bürkle, A.; Moreno-Villanueva, M.; Dollé, M.E.T.; Jansen, E.; Grune, T.; Weber, D.; et al. Age, Sex, and BMI Influence on Copper, Zinc, and Their Major Serum Carrier Proteins in a Large European Population Including Nonagenarian Offspring from MARK-AGE Study. J. Gerontol. Ser. A 2021, 76, 2097–2106. [Google Scholar] [CrossRef]
- Giacconi, R.; D’Aquila, P.; Malavolta, M.; Piacenza, F.; Bürkle, A.; Villanueva, M.M.; Dollé, M.E.T.; Jansen, E.; Grune, T.; Gonos, E.S.; et al. Bacterial DNAemia in Older Participants and Nonagenarian Offspring and Association with Redox Biomarkers: Results from MARK-AGE Study. J. Gerontol. A Biol. Sci. Med. Sci. 2023, 78, 42–50. [Google Scholar] [CrossRef]
- Muñiz, C.S.; Marchante-Gayón, J.M.; García Alonso, J.; Sanz-Medel, A. Speciation of essential elements in human serum using anion exchange chromatography coupled to post-column isotope dilution analysis with double focusing ICP–MS. J. Anal. At. Spectrom. 2001, 16, 587–592. [Google Scholar] [CrossRef]
- Persson-Moschos, M.E.; Stavenow, L.; Akesson, B.; Lindgärde, F. Selenoprotein P in plasma in relation to cancer morbidity in middle-aged Swedish men. Nutr. Cancer 2000, 36, 19–26. [Google Scholar] [CrossRef]
- Jitaru, P.; Goenaga-Infante, H.; Vaslin-Reimann, S.; Fisicaro, P. A systematic approach to the accurate quantification of selenium in serum selenoalbumin by HPLC-ICP-MS. Anal. Chim. Acta. 2010, 657, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, B.R.; Ganio, K.; Roberts, B.R. Expanding beyond ICP-MS to better understand selenium biochemistry. Metallomics 2019, 11, 1974–1983. [Google Scholar] [CrossRef] [PubMed]
- Krassas, G.E.; Pontikides, N.; Tziomalos, K.; Tzotzas, T.; Zosin, I.; Vlad, M.; Luger, A.; Gessl, A.; Marculescu, R.; Toscano, V.; et al. Selenium status in patients with autoimmune and non-autoimmune thyroid diseases from four European countries. Expert Rev. Endocrinol. Metab. 2014, 9, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, S.E.; Guo, H.; Fedarko, N.; DeZern, A.; Fried, L.P.; Xue, Q.L.; Leng, S.; Beamer, B.; Walston, J.D. Glutathione peroxidase enzyme activity in aging. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 505–509. [Google Scholar] [CrossRef]
- Błażewicz, A.; Klatka, M.; Astel, A.; Korona-Glowniak, I.; Dolliver, W.; Szwerc, W.; Kocjan, R. Serum and urinary selenium levels in obese children: A cross-sectional study. J. Trace Elem. Med. Biol. 2015, 29, 116–122. [Google Scholar] [CrossRef]
- Chen, L.; Fan, Z.; Sun, X.; Qiu, W.; Mu, W.; Chai, K.; Cao, Y.; Wang, G.; Lv, G. Diet-derived antioxidants and nonalcoholic fatty liver disease: A Mendelian randomization study. Hepatol. Int. 2022. [Google Scholar] [CrossRef]
- Huang, Y.Q.; Shen, G.; Lo, K.; Huang, J.Y.; Liu, L.; Chen, C.L.; Yu, Y.L.; Sun, S.; Zhang, B.; Feng, Y.Q. Association of circulating selenium concentration with dyslipidemia: Results from the NHANES. J. Trace Elem. Med. Biol. 2020, 58, 126438. [Google Scholar] [CrossRef]
- Wang, T.; Su, L.; Chen, X.; Wang, S.; Han, X.; Cheng, Y.; Lin, S.; Ding, L.; Liu, J.; Chen, C.; et al. Higher blood selenium level is associated with lower risk of hyperhomocysteinemia in the elderly. J. Trace Elem. Med. Biol. 2023, 75, 127078. [Google Scholar] [CrossRef]
- Wang, X.L.; Yang, T.B.; Wei, J.; Lei, G.H.; Zeng, C. Association between serum selenium level and type 2 diabetes mellitus: A non-linear dose-response meta-analysis of observational studies. Nutr. J. 2016, 15, 48. [Google Scholar] [CrossRef]
- Yang, J.; Chen, E.; Choi, C.; Chan, K.; Yang, Q.; Rana, J.; Yang, B.; Huang, C.; Yang, A.; Lo, K. Cross-Sectional Association of Blood Selenium with Glycemic Biomarkers among U.S. Adults with Normoglycemia in the National Health and Nutrition Examination Survey 2013–2016. Nutrients 2022, 14, 3972. [Google Scholar] [CrossRef]
- Nunes, F.L.D.S.; Lima, S.C.V.C.; Lyra, C.O.; Marchioni, D.M.; Pedrosa, L.F.C.; Barbosa Junior, F.; Sena-Evangelista, K.C.M. The impact of essential and toxic elements on cardiometabolic risk factors in adults and older people. J. Trace Elem. Med. Biol. 2022, 72, 126991. [Google Scholar] [CrossRef]
- Lu, C.W.; Chang, H.H.; Yang, K.C.; Chiang, C.H.; Yao, C.A.; Huang, K.C. Gender Differences with Dose-Response Relationship between Serum Selenium Levels and Metabolic Syndrome-A Case-Control Study. Nutrients 2019, 11, 477. [Google Scholar] [CrossRef] [PubMed]
- Luan, F.; Chen, Y.; Xu, Y.; Jiang, X.; Liu, B.; Wang, Y. Associations between whole blood trace elements concentrations and HbA1c levels in patients with type 2 diabetes. Biometals 2022, 35, 1011–1022. [Google Scholar] [CrossRef]
- Chehaibi, K.; Trabelsi, I.; Mahdouani, K.; Slimane, M.N. Correlation of Oxidative Stress Parameters and Inflammatory Markers in Ischemic Stroke Patients. J. Stroke Cereb. Dis. 2016, 25, 2585–2593. [Google Scholar] [CrossRef]
- Čolak, E.; Ignjatović, S.; Radosavljević, A.; Žorić, L. The association of enzymatic and non-enzymatic antioxidant defense parameters with inflammatory markers in patients with exudative form of age-related macular degeneration. J. Clin. Biochem. Nutr. 2017, 60, 100–107. [Google Scholar] [CrossRef]
- McClung, J.P.; Roneker, C.A.; Mu, W.; Lisk, D.J.; Langlais, P.; Liu, F.; Lei, X.G. Development of insulin resistance and obesity in mice overexpressing cellular glutathione peroxidase. Proc. Natl. Acad. Sci. USA 2004, 101, 8852–8857. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.D.; Vatamaniuk, M.Z.; Wang, S.K.; Roneker, C.A.; Simmons, R.A.; Lei, X.G. Molecular mechanisms for hyperinsulinaemia induced by overproduction of selenium-dependent glutathione peroxidase-1 in mice. Diabetologia 2008, 51, 1515–1524. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Stat | N | Plasma Se (ppb) Mean ± SD or (CI 95%) | p (GLM) | ||
|---|---|---|---|---|---|
| Age group (years) | 35–44 | a | 481 | 112.09 ± 17.59 c | <0.001 |
| 45–54 | b | 552 | 114.71 ± 19.71 | ||
| 55–64 | c | 595 | 115.13 ± 23.49 a,d | ||
| 65–75 | d | 572 | 112.27 ± 20.73 c | ||
| Center | Finland | a | 90 | 133.24 ± 18.55 c,d,e,g,h | <0.001 |
| Italy | b | 383 | 127.57 ± 12.14 c,d,e,g,h | ||
| Austria | c | 380 | 107.11 ± 18.11 a,b,e,g | ||
| Greece | d | 374 | 105.02 ± 14.68 a,b,e,g | ||
| Poland | e | 371 | 95.14 ± 17.26 a,b,c,d,g,h | ||
| The Netherlands | f | - | - | ||
| Belgium | g | 254 | 120.46 ± 25.47 a,b,c,d,g,h | ||
| Germany | h | 345 | 107.15 ± 15.66 a,b,e,g | ||
| Sex | F | a | 1133 | 111.73 ± 20.79 | 0.57 |
| M | b | 1064 | 110.05 ± 20.56 | ||
| BMI classes | <25 | a | 988 | 113.16 ± 20.08 c | <0.001 |
| 25 to <30 | b | 826 | 109.84 ± 21.53 | ||
| ≥30 | c | 378 | 107.41 ± 19.92 a |
| Unstandardized Coefficients | Standardized Coefficients | |||
|---|---|---|---|---|
| Plasma Se Levels | B | Std. Error | Beta | p Value |
| Albumin | 1.301 | 0.144 | 0.197 | p < 0.0001 |
| HDL | 3.917 | 1.243 | 0.083 | 0.002 |
| TC | 1.484 | 0.474 | 0.073 | 0.002 |
| Fibrinogen | 1.048 | 0.320 | 0.071 | 0.001 |
| Homocysteine | −0.200 | 0.078 | −0.056 | 0.010 |
| TG | 1.155 | 0.573 | 0.048 | 0.044 |
| Se2 fraction | B | Std. Error | Beta | p value |
| Fibrinogen | −0.596 | 0.115 | −0.123 | p < 0.0001 |
| Adiponectin | 0.112 | 0.023 | 0.124 | p < 0.0001 |
| HbA1c | 0.854 | 0.251 | 0.077 | 0.001 |
| Ceruloplasmin | 0.064 | 0.023 | 0.068 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giacconi, R.; Piacenza, F.; Aversano, V.; Zampieri, M.; Bürkle, A.; Villanueva, M.M.; Dollé, M.E.T.; Jansen, E.; Grune, T.; Gonos, E.S.; et al. Uncovering the Relationship between Selenium Status, Age, Health, and Dietary Habits: Insights from a Large Population Study including Nonagenarian Offspring from the MARK-AGE Project. Nutrients 2023, 15, 2182. https://doi.org/10.3390/nu15092182
Giacconi R, Piacenza F, Aversano V, Zampieri M, Bürkle A, Villanueva MM, Dollé MET, Jansen E, Grune T, Gonos ES, et al. Uncovering the Relationship between Selenium Status, Age, Health, and Dietary Habits: Insights from a Large Population Study including Nonagenarian Offspring from the MARK-AGE Project. Nutrients. 2023; 15(9):2182. https://doi.org/10.3390/nu15092182
Chicago/Turabian StyleGiacconi, Robertina, Francesco Piacenza, Valentina Aversano, Michele Zampieri, Alexander Bürkle, María Moreno Villanueva, Martijn E. T. Dollé, Eugène Jansen, Tilman Grune, Efstathios S. Gonos, and et al. 2023. "Uncovering the Relationship between Selenium Status, Age, Health, and Dietary Habits: Insights from a Large Population Study including Nonagenarian Offspring from the MARK-AGE Project" Nutrients 15, no. 9: 2182. https://doi.org/10.3390/nu15092182
APA StyleGiacconi, R., Piacenza, F., Aversano, V., Zampieri, M., Bürkle, A., Villanueva, M. M., Dollé, M. E. T., Jansen, E., Grune, T., Gonos, E. S., Franceschi, C., Capri, M., Weinberger, B., Sikora, E., Toussaint, O., Debacq-Chainiaux, F., Stuetz, W., Slagboom, P. E., Bernhardt, J., ... Malavolta, M. (2023). Uncovering the Relationship between Selenium Status, Age, Health, and Dietary Habits: Insights from a Large Population Study including Nonagenarian Offspring from the MARK-AGE Project. Nutrients, 15(9), 2182. https://doi.org/10.3390/nu15092182