
Ultra-Processed Food Consumption and Risk of Overweight or Obesity in Chinese Adults: Chinese Food Consumption Survey 2017–2020

Abstract
:1. Introduction
2. Materials and Methods
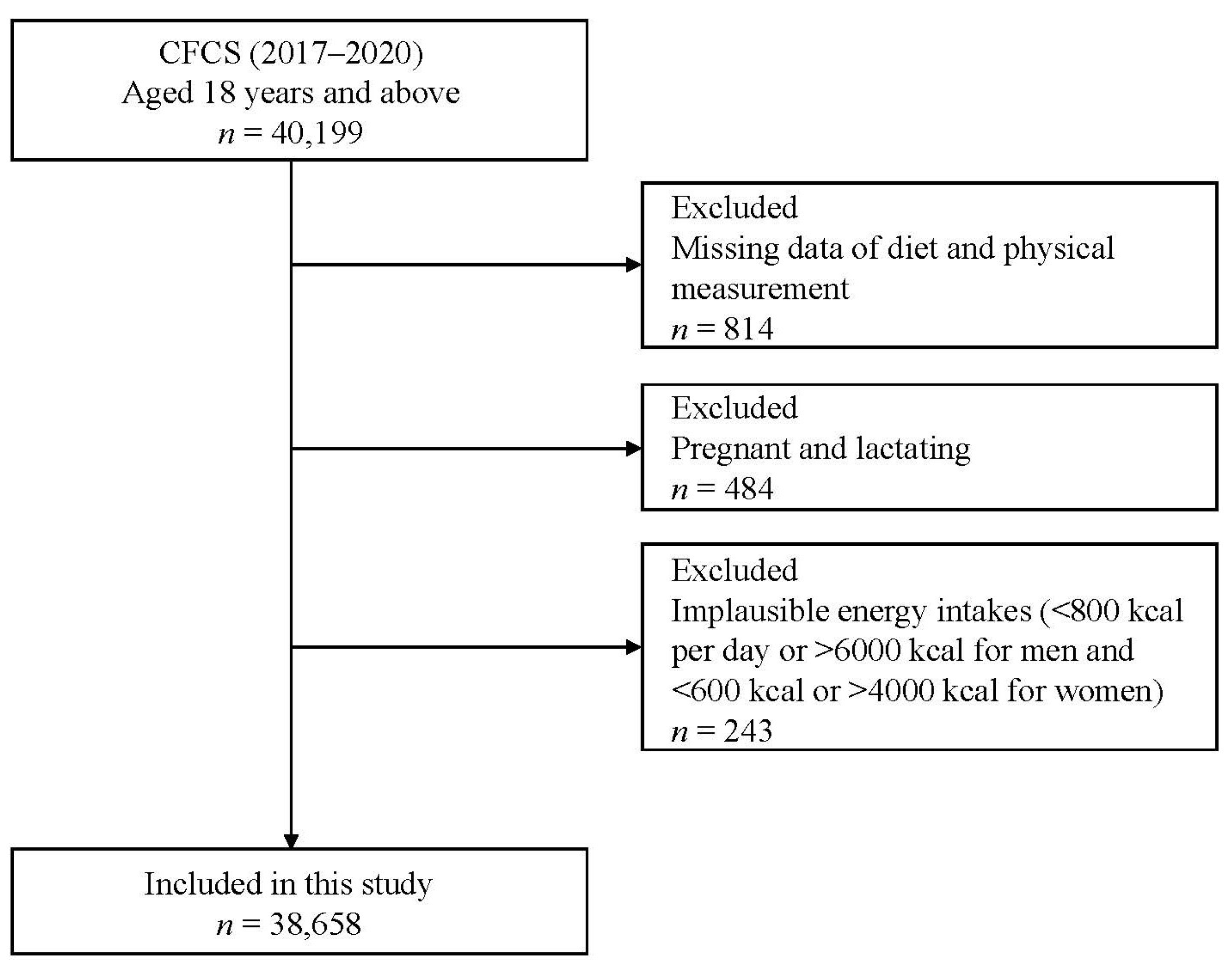
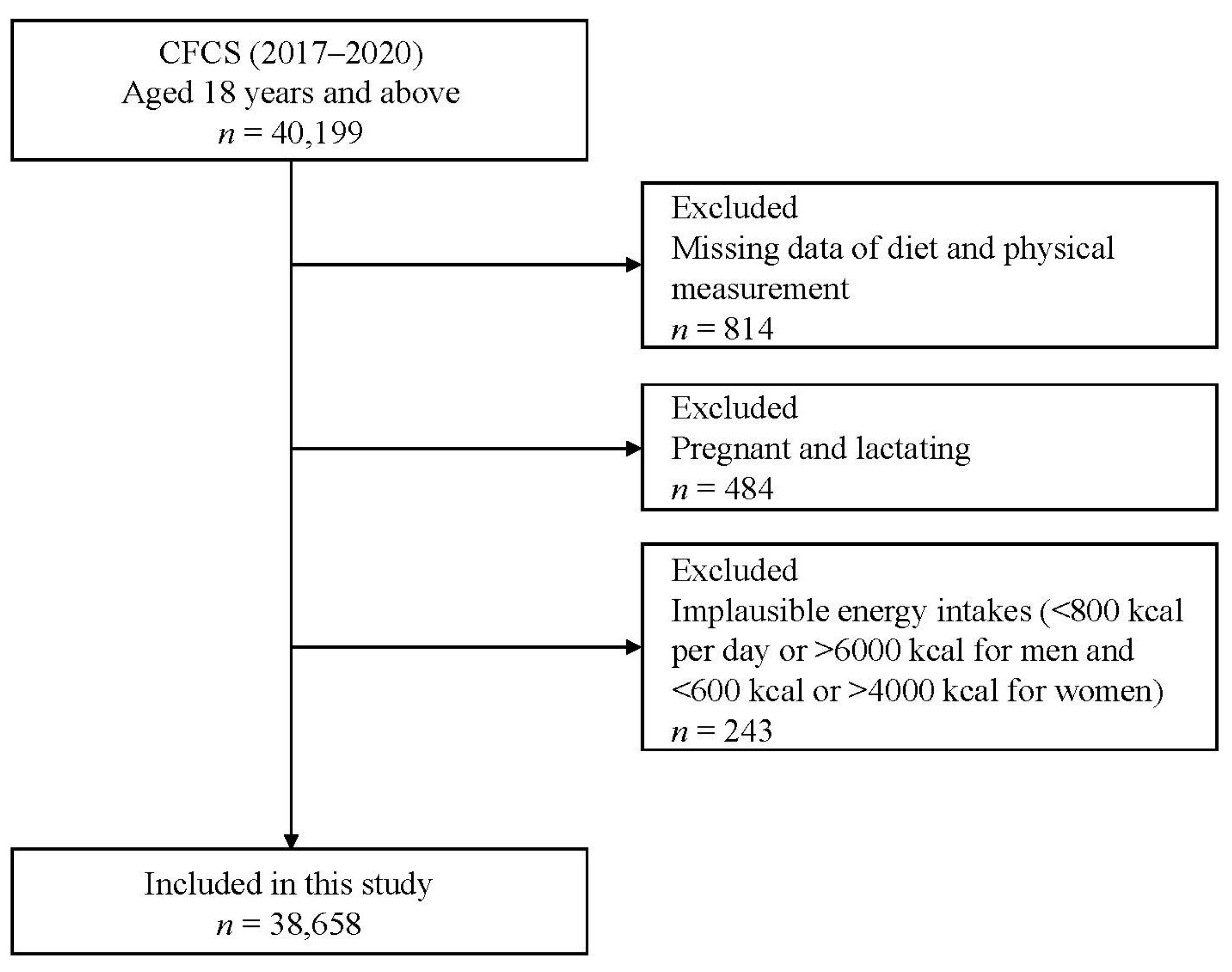
2.1. Study Design and Population
2.2. Definition of UPFs and Dietary Assessment
2.3. Definition of Overweight and Obesity
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Associations of UPF Consumption with Overweight or Obesity
3.3. Stratified Analyses of Overweight or Obesity and UPFs Consumption
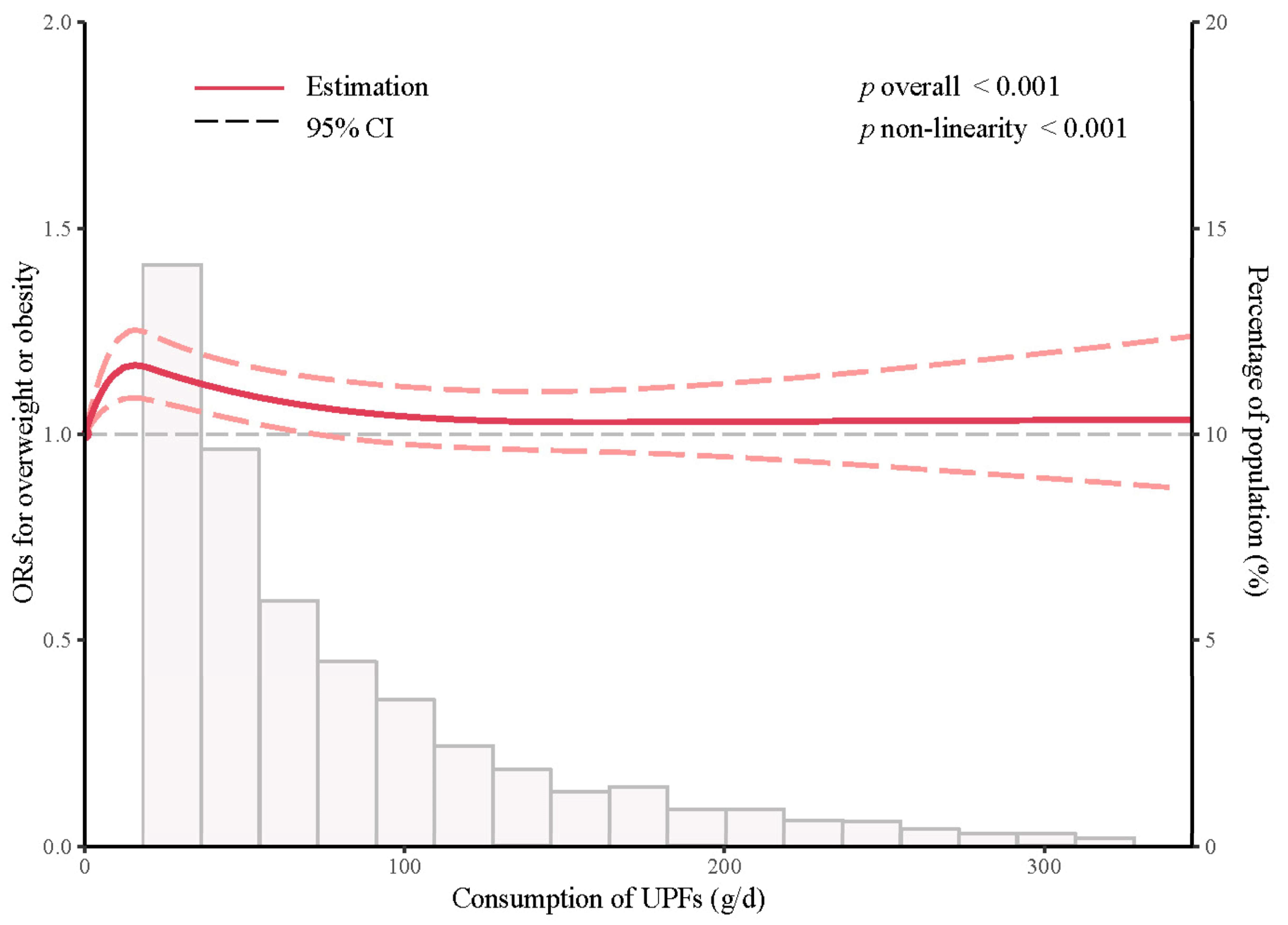
3.4. Nonlinear Relationship between UPF Consumption and ORs of Overweight or Obesity
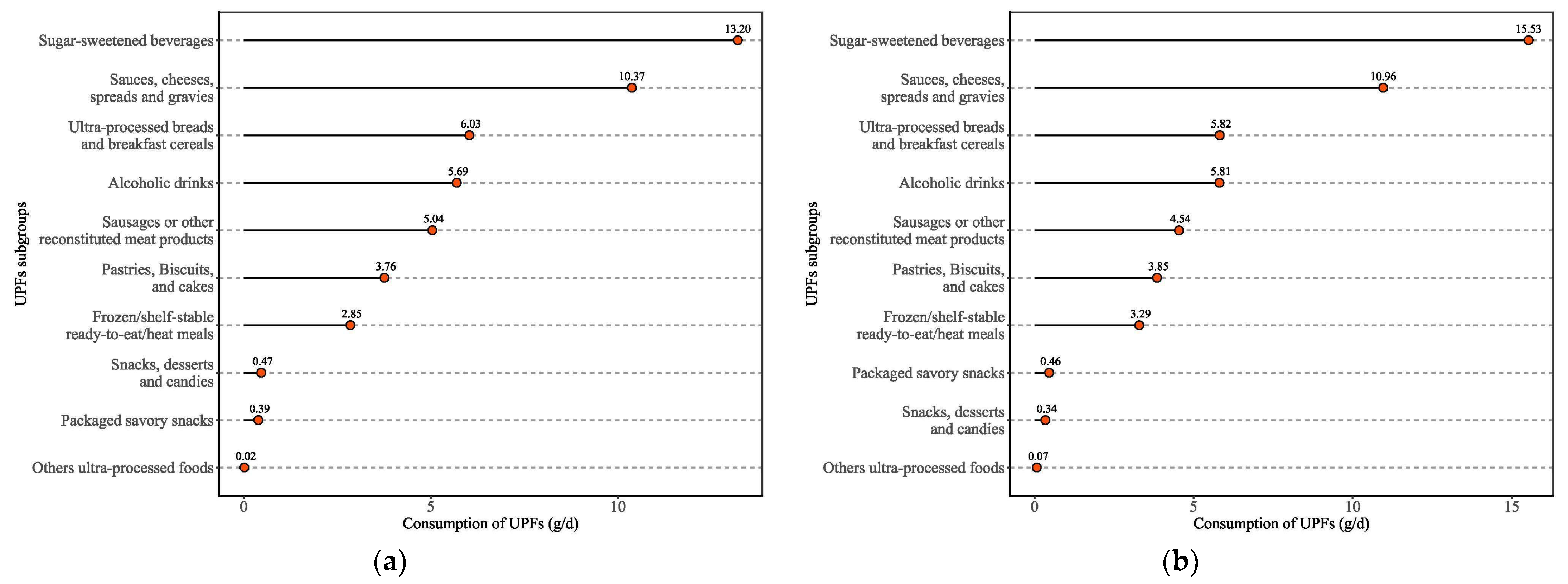
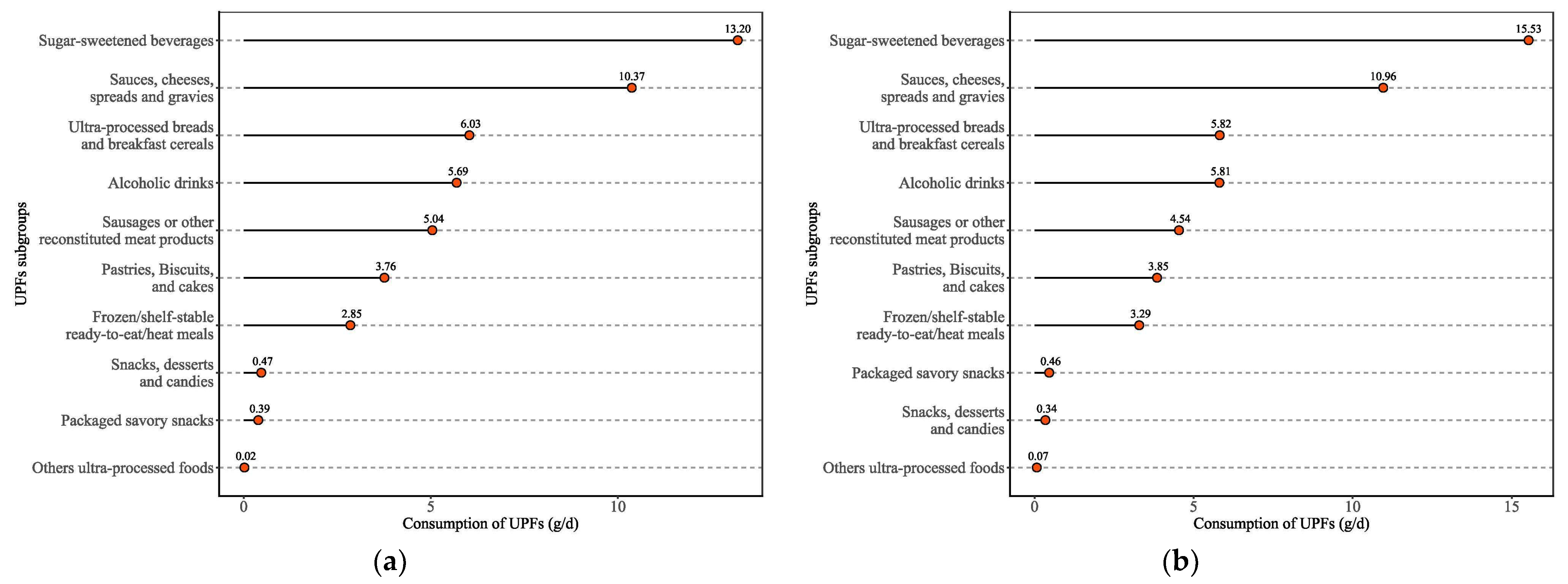
3.5. Subgroups Consumption of UPFs among Overweight or Obesity Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, Regional, and National Prevalence of Overweight and Obesity in Children and Adults During 1980–2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration. Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128.9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [PubMed]
- World Health Organization. Fact Sheets on Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 January 2021).
- National Health Commission of the People’s Republic of China. Report on Chinese Residents’ Chronic Diseases and Nutrition 2020; People’s Medical Publishing House: Beijing, China, 2021. [Google Scholar]
- Wang, Y.; Zhao, L.; Gao, L.; Pan, A.; Xue, H. Health Policy and Public Health Implications of Obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 446–461. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, B.; Zhao, Z.; Yang, L.; Zhang, M.; Jiang, Y.; Li, Y.; Zhou, M.; Wang, L.; Huang, Z.; et al. Body-Mass Index and Obesity in Urban and Rural China: Findings from Consecutive Nationally Representative Surveys During 2004–2018. Lancet 2021, 398, 53–63. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Dos-Santos-Silva, I.; Leon, D.A.; Douglas, I.J.; Smeeth, L. Association of BMI with Overall and Cause-Specific Mortality: A Population-Based Cohort Study of 3·6 Million Adults in the UK. Lancet Diabetes Endocrinol. 2018, 6, 944–953. [Google Scholar] [CrossRef]
- Li, Y.; Teng, D.; Shi, X.; Teng, X.; Teng, W.; Shan, Z.; Lai, Y. Diabetes China National, Group Metabolic Disorders Study, Iodine Status the Thyroid Disorders, and Group Diabetes Epidemiological Survey. Changes in the Prevalence of Obesity and Hypertension and Demographic Risk Factor Profiles in China over 10 Years: Two National Cross-Sectional Surveys. Lancet Reg. Health West Pac. 2021, 15, 100227. [Google Scholar] [PubMed]
- Zhai, F.Y.; Du, S.F.; Wang, Z.H.; Zhang, J.G.; Du, W.W.; Popkin, B.M. Dynamics of the Chinese Diet and the Role of Urbanicity, 1991–2011. Obes. Rev. 2014, 15 (Suppl. S1), 16–26. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Z.; Du, W.; Huang, F.; Jiang, H.; Bai, J.; Zhang, X.; Zhang, B.; Wang, H. Twenty-Five-Year Trends in Dietary Patterns among Chinese Adults from 1991 to 2015. Nutrients 2021, 13, 1327. [Google Scholar] [CrossRef]
- Pan, X.F.; Wang, L.; Pan, A. Epidemiology and Determinants of Obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-Processed Foods: What They Are and How to Identify Them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The Un Decade of Nutrition, the Nova Food Classification and the Trouble with Ultra-Processing. Public Health Nutr. 2018, 21, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Steele, E.M.; Du, M.; Pomeranz, J.L.; O’Connor, L.E.; Herrick, K.A.; Luo, H.; Zhang, X.; Mozaffarian, D.; Zhang, F.F. Trends in Consumption of Ultraprocessed Foods among Us Youths Aged 2–19 Years, 1999–2018. JAMA 2021, 326, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Moubarac, J.C.; Batal, M.; Martins, A.P.; Claro, R.; Levy, R.B.; Cannon, G.; Monteiro, C. Processed and Ultra-Processed Food Products: Consumption Trends in Canada from 1938 to 2011. Can. J. Diet. Pract. Res. 2014, 75, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Baker, P.; Friel, S. Food Systems Transformations, Ultra-Processed Food Markets and the Nutrition Transition in Asia. Glob. Health 2016, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Elizabeth, L.; Machado, P.; Zinocker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of Ultra-Processed Foods and Health Status: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, Z.; Yang, H.; Qiu, P.; Wang, H.; Wang, F.; Zhao, Q.; Fang, J.; Nie, J. Consumption of Ultra-Processed Foods and Health Outcomes: A Systematic Review of Epidemiological Studies. Nutr. J. 2020, 19, 86. [Google Scholar] [CrossRef]
- Srour, B.; Kordahi, M.C.; Bonazzi, E.; Deschasaux-Tanguy, M.; Touvier, M.; Chassaing, B. Ultra-Processed Foods and Human Health: From Epidemiological Evidence to Mechanistic Insights. Lancet Gastroenterol. Hepatol. 2022, 7, 1128–1140. [Google Scholar]
- Juul, F.; Martinez-Steele, E.; Parekh, N.; Monteiro, C.A.; Chang, V.W. Ultra-Processed Food Consumption and Excess Weight among Us Adults. Br. J. Nutr. 2018, 120, 90–100. [Google Scholar] [CrossRef]
- Canhada, S.L.; Luft, V.C.; Giatti, L.; Duncan, B.B.; Chor, D.; Fonseca, M.; Matos, S.M.A.; Molina, M.; Barreto, S.M.; Levy, R.B.; et al. Ultra-Processed Foods, Incident Overweight and Obesity, and Longitudinal Changes in Weight and Waist Circumference: The Brazilian Longitudinal Study of Adult Health (Elsa-Brasil). Public Health Nutr. 2020, 23, 1076–1086. [Google Scholar] [CrossRef]
- Li, M.; Shi, Z. Ultra-Processed Food Consumption Associated with Overweight/Obesity among Chinese Adults-Results from China Health and Nutrition Survey 1997–2011. Nutrients 2021, 13, 2796. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y. China Food Composition 2004; Peking University Medical Press: Beijing, China, 2005. [Google Scholar]
- Yang, Y.; Wang, Y.; Pan, X. China Food Composition 2009; Peking University Medical Press: Beijing, China, 2010. [Google Scholar]
- National Health and Family Planning Commission of People’s Republic of China. WS/T 428-2013 Criteria of Weight for Adults. Available online: https://www.chinanutri.cn/fgbz/fgbzhybz/201501/P020170721497677913633.pdf (accessed on 16 January 2015).
- Rauber, F.; Steele, E.M.; Louzada, M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Food Consumption and Indicators of Obesity in the United Kingdom Population (2008–2016). PLoS ONE 2020, 15, e0232676. [Google Scholar] [CrossRef] [PubMed]
- Louzada, M.L.; Baraldi, L.G.; Steele, E.M.; Martins, A.P.; Canella, D.S.; Moubarac, J.C.; Levy, R.B.; Cannon, G.; Afshin, A.; Imamura, F.; et al. Consumption of Ultra-Processed Foods and Obesity in Brazilian Adolescents and Adults. Prev. Med. 2015, 81, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.P.; Steele, E.M.; Levy, R.B.; da Costa Louzada, M.L.; Rangan, A.; Woods, J.; Gill, T.; Scrinis, G.; Monteiro, C.A. Ultra-Processed Food Consumption and Obesity in the Australian Adult Population. Nutr. Diabetes 2020, 10, 39. [Google Scholar] [CrossRef]
- Nardocci, M.; Leclerc, B.S.; Louzada, M.L.; Monteiro, C.A.; Batal, M.; Moubarac, J.C. Consumption of Ultra-Processed Foods and Obesity in Canada. Can. J. Public Health 2019, 110, 4–14. [Google Scholar] [CrossRef]
- Julia, C.; Martinez, L.; Alles, B.; Touvier, M.; Hercberg, S.; Mejean, C.; Kesse-Guyot, E. Contribution of Ultra-Processed Foods in the Diet of Adults from the French Nutrinet-Sante Study. Public Health Nutr. 2018, 21, 27–37. [Google Scholar] [CrossRef]
- Mendonca, R.D.; Pimenta, A.M.; Gea, A.; de la Fuente-Arrillaga, C.; Martinez-Gonzalez, M.A.; Lopes, A.C.; Bes-Rastrollo, M. Ultraprocessed Food Consumption and Risk of Overweight and Obesity: The University of Navarra Follow-up (Sun) Cohort Study. Am. J. Clin. Nutr. 2016, 104, 1433–1440. [Google Scholar] [CrossRef]
- Rauber, F.; Chang, K.; Vamos, E.P.; da Costa Louzada, M.L.; Monteiro, C.A.; Millett, C.; Levy, R.B. Ultra-Processed Food Consumption and Risk of Obesity: A Prospective Cohort Study of UK Biobank. Eur. J. Nutr. 2021, 60, 2169–2180. [Google Scholar] [CrossRef]
- Cordova, R.; Kliemann, N.; Huybrechts, I.; Rauber, F.; Vamos, E.P.; Levy, R.B.; Wagner, K.H.; Viallon, V.; Casagrande, C.; Nicolas, G.; et al. Consumption of Ultra-Processed Foods Associated with Weight Gain and Obesity in Adults: A Multi-National Cohort Study. Clin. Nutr. 2021, 40, 5079–5088. [Google Scholar]
- Gupta, S.; Hawk, T.; Aggarwal, A.; Drewnowski, A. Characterizing Ultra-Processed Foods by Energy Density, Nutrient Density, and Cost. Front. Nutr. 2019, 6, 70. [Google Scholar] [CrossRef] [PubMed]
- Martini, D.; Godos, J.; Bonaccio, M.; Vitaglione, P.; Grosso, G. Ultra-Processed Foods and Nutritional Dietary Profile: A Meta-Analysis of Nationally Representative Samples. Nutrients 2021, 13, 3390. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Ayuketah, A.; Brychta, R.; Cai, H.; Cassimatis, T.; Chen, K.Y.; Chung, S.T.; Costa, E.; Courville, A.; Darcey, V.; et al. Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metab. 2019, 30, 67–77.e3. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Barquera, S.; Corvalan, C.; Hofman, K.J.; Monteiro, C.; Ng, S.W.; Swart, E.C.; Taillie, L.S. Towards Unified and Impactful Policies to Reduce Ultra-Processed Food Consumption and Promote Healthier Eating. Lancet Diabetes Endocrinol. 2021, 9, 462–470. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Lawrence, M.; Costa Louzada, M.D.; Pereira Machado, P. Ultra-Processed Foods, Diet Quality, and Health Using the Nova Classification System; Food and Agriculture Organization of the United Nations: Rome, Italy, 2019. [Google Scholar]
- Harb, A.A.; Shechter, A.; Koch, P.A.; St-Onge, M.P. Ultra-Processed Foods and the Development of Obesity in Adults. Eur. J. Clin. Nutr. 2023, 77, 619–627. [Google Scholar]
- Carwile, J.L.; Michels, K.B. Urinary Bisphenol a and Obesity: Nhanes 2003–2006. Environ. Res. 2011, 111, 825–830. [Google Scholar] [CrossRef]
- Hwang, S.; Lim, J.E.; Choi, Y.; Jee, S.H. Bisphenol a Exposure and Type 2 Diabetes Mellitus Risk: A Meta-Analysis. BMC Endocr. Disord. 2018, 18, 81. [Google Scholar]
- Ranciere, F.; Lyons, J.G.; Loh, V.H.; Botton, J.; Galloway, T.; Wang, T.; Shaw, J.E.; Magliano, D.J. Bisphenol a and the Risk of Cardiometabolic Disorders: A Systematic Review with Meta-Analysis of the Epidemiological Evidence. Environ. Health 2015, 14, 46. [Google Scholar] [CrossRef]
- Forde, C.G.; Mars, M.; de Graaf, K. Ultra-Processing or Oral Processing? A Role for Energy Density and Eating Rate in Moderating Energy Intake from Processed Foods. Curr. Dev. Nutr. 2020, 4, nzaa019. [Google Scholar] [CrossRef]
- Wahlqvist, M.L. Food Structure Is Critical for Optimal Health. Food Funct. 2016, 7, 1245–1250. [Google Scholar]
- Sung, H.; Park, J.M.; Oh, S.U.; Ha, K.; Joung, H. Consumption of Ultra-Processed Foods Increases the Likelihood of Having Obesity in Korean Women. Nutrients 2021, 13, 698. [Google Scholar]
- Fan, J.; Song, Y.; Wang, Y.; Hui, R.; Zhang, W. Dietary Glycemic Index, Glycemic Load, and Risk of Coronary Heart Disease, Stroke, and Stroke Mortality: A Systematic Review with Meta-Analysis. PLoS ONE 2012, 7, e52182. [Google Scholar]
- Mirrahimi, A.; Chiavaroli, L.; Srichaikul, K.; Augustin, L.S.; Sievenpiper, J.L.; Kendall, C.W.; Jenkins, D.J. The Role of Glycemic Index and Glycemic Load in Cardiovascular Disease and Its Risk Factors: A Review of the Recent Literature. Curr. Atheroscler. Rep. 2014, 16, 381. [Google Scholar] [PubMed]
- Gong, P.; Liang, S.; Carlton, E.J.; Jiang, Q.; Wu, J.; Wang, L.; Remais, J.V. Urbanisation and Health in China. Lancet 2012, 379, 843–852. [Google Scholar] [PubMed]
- Popkin, B.M.; Gordon-Larsen, P. The Nutrition Transition: Worldwide Obesity Dynamics and Their Determinants. Int. J. Obes. Relat. Metab. Disord. 2004, 28 (Suppl. S3), S2–S9. [Google Scholar] [CrossRef]
- Su, C.; Song, X.; Hu, H.; Du, W.; Wang, H.; Zhang, B. Longitudinal Association between Urbanicity and Total Dietary Fat Intake in Adults in Urbanizing China from 1991 to 2015: Findings from the Chns. Nutrients 2020, 12, 1597. [Google Scholar]
- Wang, L.; Wang, H.; Zhang, B.; Popkin, B.M.; Du, S. Elevated Fat Intake Increases Body Weight and the Risk of Overweight and Obesity among Chinese Adults: 1991–2015 Trends. Nutrients 2020, 12, 3272. [Google Scholar]
- Huang, K.; Zhao, L.; Guo, Q.; Yu, D.; Yang, Y.; Cao, Q.; Yuan, X.; Ju, L.; Li, S.; Cheng, X.; et al. Comparison of the 24 H Dietary Recall of Two Consecutive Days, Two Non-Consecutive Days, Three Consecutive Days, and Three Non-Consecutive Days for Estimating Dietary Intake of Chinese Adult. Nutrients 2022, 14, 1960. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Quartile of UPFs (g/day) | |||||
|---|---|---|---|---|---|
| Q1 (<4.6) | Q2 (4.6–18.2) | Q3 (18.2–59.1) | Q4 (>59.1) | p-Value | |
| Gender | <0.001 | ||||
| Men | 4149 (42.9) | 4427 (45.8) | 4597 (47.6) | 5394 (55.8) | |
| Women | 5515 (57.1) | 5238 (54.2) | 5066 (52.4) | 4272 (44.2) | |
| Age | <0.001 | ||||
| 18–44 | 3786 (39.2) | 3705 (38.3) | 3891 (40.3) | 4679 (48.4) | |
| 45–59 | 3877 (40.1) | 3837 (39.7) | 3787 (39.2) | 3407 (35.3) | |
| ≥60 | 2001 (20.7) | 2123 (22.0) | 1985 (20.5) | 1580 (16.4) | |
| Education level | <0.001 | ||||
| Primary school or below | 2685 (27.8) | 2200 (22.8) | 1958 (20.3) | 1549 (16.0) | |
| Secondary school | 5319 (55.0) | 5419 (56.1) | 5300 (54.9) | 5080 (52.6) | |
| College or above | 1660 (17.2) | 2046 (21.2) | 2405 (24.9) | 3037 (31.4) | |
| Individual annual income (CNY) | <0.001 | ||||
| <10,000 | 3009 (31.1) | 2343 (24.2) | 2161 (22.4) | 2039 (21.1) | |
| 10,000–39,999 | 5196 (53.8) | 5461 (56.5) | 5284 (54.7) | 5148 (53.3) | |
| 40,000–99,999 | 791 (8.2) | 1133 (11.7) | 1386 (14.3) | 1534 (15.9) | |
| >100,000 | 213 (2.2) | 276 (2.9) | 345 (3.6) | 358 (3.7) | |
| No response | 455 (4.7) | 452 (4.7) | 487 (5.0) | 587 (6.1) | |
| Occupation | <0.001 | ||||
| Student | 123 (1.3) | 110 (1.1) | 126 (1.3) | 244 (2.5) | |
| Retired or unemployed | 3262 (33.8) | 3299 (34.1) | 2999 (31.0) | 2463 (25.5) | |
| Professionals | 1212 (12.5) | 1422 (14.7) | 1649 (17.1) | 1876 (19.4) | |
| Business service | 1436 (14.9) | 1696 (17.6) | 1890 (19.6) | 2115 (21.9) | |
| Manual labor | 2596 (26.9) | 2218 (23.0) | 2132 (22.1) | 2024 (20.9) | |
| Others | 1035 (10.7) | 920 (9.5) | 867 (9.0) | 944 (9.8) | |
| Drinking past month | <0.001 | ||||
| Yes | 2235 (23.1) | 2620 (27.1) | 3069 (31.8) | 3931 (40.7) | |
| No | 7429 (76.9) | 7045 (72.9) | 6594 (68.2) | 5735 (59.3) | |
| Labor intensity | <0.001 | ||||
| Light | 5316 (55.0) | 5747 (59.5) | 5980 (61.9) | 5873 (60.8) | |
| Medium | 3404 (35.2) | 3275 (33.9) | 3041 (31.5) | 3136 (32.4) | |
| Heavy | 944 (9.8) | 643 (6.7) | 642 (6.6) | 657 (6.8) | |
| Place of residence | <0.001 | ||||
| Metropolis | 2335 (24.2) | 3085 (31.9) | 3172 (32.8) | 3504 (36.3) | |
| Small and medium-sized cities | 3069 (31.8) | 3040 (31.5) | 3286 (34.0) | 3083 (31.9) | |
| Rural areas | 4260 (44.1) | 3540 (36.6) | 3205 (33.2) | 3079 (31.9) | |
| Region of residence | <0.001 | ||||
| Eastern regions | 3403 (35.2) | 4958 (51.3) | 4911 (50.8) | 4987 (51.6) | |
| Central regions | 3579 (37.0) | 2466 (25.5) | 2401 (24.9) | 2801 (29.0) | |
| Western regions | 2682 (27.8) | 2241 (23.2) | 2351 (24.3) | 1878 (19.4) | |
| BMI (kg/m2) | 23.4 ± 3.3 | 23.7 ± 3.3 | 23.7 ± 3.4 | 23.6 ± 3.4 | <0.001 |
| Energy (kcal/day) | 1848.2 ± 595.3 | 1807.63 ± 590.4 | 1897.6 ± 579.6 | 2150.0 ± 663.3 | <0.001 |
| Protein (g/day) | 62.1 ± 23.4 | 62.9 ± 23.9 | 66.1 ± 24.0 | 72.8 ± 26.1 | <0.001 |
| Fat (g/day) | 65.4 ± 34.9 | 67.5 ± 35.1 | 74.6 ± 36.4 | 85.1 ± 40.4 | <0.001 |
| Carbohydrate (g/day) | 261.0 ± 106.1 | 244.4 ± 98.7 | 246.2 ± 93.0 | 266.4 ± 98.8 | <0.001 |
| Vitamin A (μgRE) | 377.4 ± 520.5 | 408.1 ± 557.2 | 426.9 ± 536.8 | 432.5 ± 597.7 | <0.001 |
| Vitamin C (mg/day) | 62.6 ± 69.9 | 63.0 ± 74.3 | 65.3 ± 72.3 | 77.9 ± 151.5 | <0.001 |
| Calcium (mg/day) | 321.4 ± 180.2 | 347.4 ± 180.4 | 381.1 ± 202.5 | 427.7 ± 219.4 | <0.001 |
| Sodium (mg/day) | 2943.9 ± 2108.6 | 3510.4 ± 2266.9 | 4057.1 ± 2657.8 | 4315.5 ± 2796.5 | <0.01 |
| Quartile of UPFs (g/day) | |||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | p Trend | |
| Overweight or obesity | |||||
| Median | 3.3 | 10.9 | 23.5 | 60.8 | |
| Model 1 | 1.00 (ref) | 1.16 (1.10, 1.23) *** | 1.14 (1.08, 1.21) *** | 1.08 (1.02, 1.14) * | 0.182 |
| Model 2 | 1.00 (ref) | 1.14 (1.08, 1.21) *** | 1.13 (1.06, 1.20) *** | 1.08 (1.02, 1.14) * | 0.690 |
| Model 3 | 1.00 (ref) | 1.14 (1.07, 1.20) *** | 1.10 (1.04, 1.17) ** | 1.03 (0.97, 1.09) | 0.241 |
| Overweight | |||||
| Median | 3.3 | 11.6 | 26.5 | 67.0 | |
| Model 1 | 1.00 (ref) | 1.18 (1.10, 1.25) *** | 1.13 (1.06, 1.21) *** | 1.08 (1.01, 1.15) * | 0.929 |
| Model 2 | 1.00 (ref) | 1.15 (1.08, 1.22) *** | 1.11 (1.04, 1.19) *** | 1.07 (1.01, 1.15) * | 0.836 |
| Model 3 | 1.00 (ref) | 1.15 (1.08, 1.22) *** | 1.10 (1.03, 1.17) *** | 1.03 (0.97, 1.10) | 0.236 |
| Obesity | |||||
| Median | 3.4 | 11.4 | 25.0 | 63.5 | |
| Model 1 | 1.00 (ref) | 1.11 (1.01, 1.23) * | 1.19 (1.08, 1.32) *** | 1.07 (0.97, 1.19) | 0.739 |
| Model 2 | 1.00 (ref) | 1.10 (1.00, 1.22) | 1.19 (1.08, 1.32) *** | 1.09 (0.98, 1.20) | 0.499 |
| Model 3 | 1.00 (ref) | 1.09 (0.99, 1.21) | 1.15 (1.04, 1.27) ** | 1.02 (0.92, 1.14) | 0.556 |
| Quartile of UPFs (g/day) | |||||
|---|---|---|---|---|---|
| Q1 (<4.6) | Q2 (4.6–18.2) | Q3 (18.2–59.1) | Q4 (>59.1) | p for Interaction | |
| Gender | 0.006 | ||||
| Men | 1.00 (ref) | 1.18 (1.08, 1.29) *** | 1.18 (1.08, 1.29) *** | 1.08 (0.99, 1.17) | |
| Women | 1.00 (ref) | 1.14 (1.05, 1.23) ** | 1.12 (1.03, 1.22) ** | 1.10 (1.01, 1.20) * | |
| Age | 0.392 | ||||
| 18–44 | 1.00 (ref) | 1.08 (0.98, 1.19) | 1.09 (0.99, 1.20) | 1.02 (0.93, 1.13) | |
| 45–59 | 1.00 (ref) | 1.14 (1.04, 1.25) ** | 1.12 (1.02, 1.23) ** | 1.06 (0.96, 1.17) | |
| ≥60 | 1.00 (ref) | 1.22 (1.07, 1.38) ** | 1.16 (1.02, 1.33) ** | 1.08 (0.93, 1.24) | |
| Education level | 0.850 | ||||
| Primary school or below | 1.00 (ref) | 1.18 (1.05, 1.33) ** | 1.14 (1.01, 1.29) * | 1.11 (0.97, 1.27) | |
| Secondary school | 1.00 (ref) | 1.10 (1.02, 1.19) ** | 1.11 (1.02, 1.20) ** | 1.02 (0.94, 1.11) | |
| College or above | 1.00 (ref) | 1.19 (1.03, 1.37) * | 1.16 (1.00, 1.33) * | 1.10 (0.96, 1.26) | |
| Individual annual income (CNY) | |||||
| <10,000 | 1.00 (ref) | 1.22 (1.10, 1.37) *** | 1.15 (1.02, 1.29) * | 1.08 (0.95, 1.22) | 0.363 |
| 10,000–39,999 | 1.00 (ref) | 1.12 (1.03, 1.21) ** | 1.13 (1.04, 1.23) ** | 1.04 (0.96, 1.13) | |
| 40,000–99,999 | 1.00 (ref) | 1.06 (0.88, 1.29) | 1.01 (0.84, 1.22) | 0.93 (0.77, 1.12) | |
| >100,000 | 1.00 (ref) | 1.21 (0.81, 1.79) | 1.06 (0.73, 1.54) | 1.10 (0.74, 1.64) | |
| No response | 1.00 (ref) | 0.87 (0.65, 1.15) | 0.81 (0.61, 1.08) | 0.85 (0.64, 1.12) | |
| Occupation | 0.123 | ||||
| Student | 1.00 (ref) | 1.54 (0.76, 3.12) | 1.60 (0.80, 3.20) | 1.11 (0.58, 2.14) | |
| Retired or unemployed | 1.00 (ref) | 1.18 (1.07, 1.30) *** | 1.19 (1.07, 1.32) *** | 1.07 (0.95, 1.20) | |
| Professionals | 1.00 (ref) | 1.21 (1.03, 1.43) * | 1.06 (0.90, 1.25) | 1.07 (0.91, 1.25) | |
| Business service | 1.00 (ref) | 1.04 (0.90, 1.21) | 1.15 (0.99, 1.34) | 1.09 (0.94, 1.27) | |
| Manual labor | 1.00 (ref) | 1.04 (0.92, 1.17) | 1.01 (0.89, 1.13) | 0.99 (0.87, 1.12) | |
| Others | 1.00 (ref) | 1.25 (1.04, 1.51) * | 1.15 (0.95, 1.40) | 0.96 (0.79, 1.16) | |
| Place of residence | 0.047 | ||||
| Metropolis | 1.00 (ref) | 1.10 (0.98, 1.23) | 1.02 (0.91, 1.15) | 0.94 (0.84, 1.06) | |
| Small and medium-sized cities | 1.00 (ref) | 1.25 (1.12, 1.38) *** | 1.12 (1.01, 1.25) ** | 1.13 (1.01, 1.26) ** | |
| Rural areas | 1.00 (ref) | 1.04 (0.95, 1.14) | 1.13 (1.02, 1.24) ** | 1.01 (0.91, 1.11) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, F.; Zhang, T.; Mao, W.; Zhao, F.; Luan, D.; Li, J. Ultra-Processed Food Consumption and Risk of Overweight or Obesity in Chinese Adults: Chinese Food Consumption Survey 2017–2020. Nutrients 2023, 15, 4005. https://doi.org/10.3390/nu15184005
Pan F, Zhang T, Mao W, Zhao F, Luan D, Li J. Ultra-Processed Food Consumption and Risk of Overweight or Obesity in Chinese Adults: Chinese Food Consumption Survey 2017–2020. Nutrients. 2023; 15(18):4005. https://doi.org/10.3390/nu15184005
Chicago/Turabian StylePan, Feng, Tongwei Zhang, Weifeng Mao, Fanglei Zhao, Dechun Luan, and Jianwen Li. 2023. "Ultra-Processed Food Consumption and Risk of Overweight or Obesity in Chinese Adults: Chinese Food Consumption Survey 2017–2020" Nutrients 15, no. 18: 4005. https://doi.org/10.3390/nu15184005
APA StylePan, F., Zhang, T., Mao, W., Zhao, F., Luan, D., & Li, J. (2023). Ultra-Processed Food Consumption and Risk of Overweight or Obesity in Chinese Adults: Chinese Food Consumption Survey 2017–2020. Nutrients, 15(18), 4005. https://doi.org/10.3390/nu15184005