


Vitamin D Supplementation during Intensive Care Unit Stay Is Associated with Improved Outcomes in Critically Ill Patients with Sepsis: A Cohort Study
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
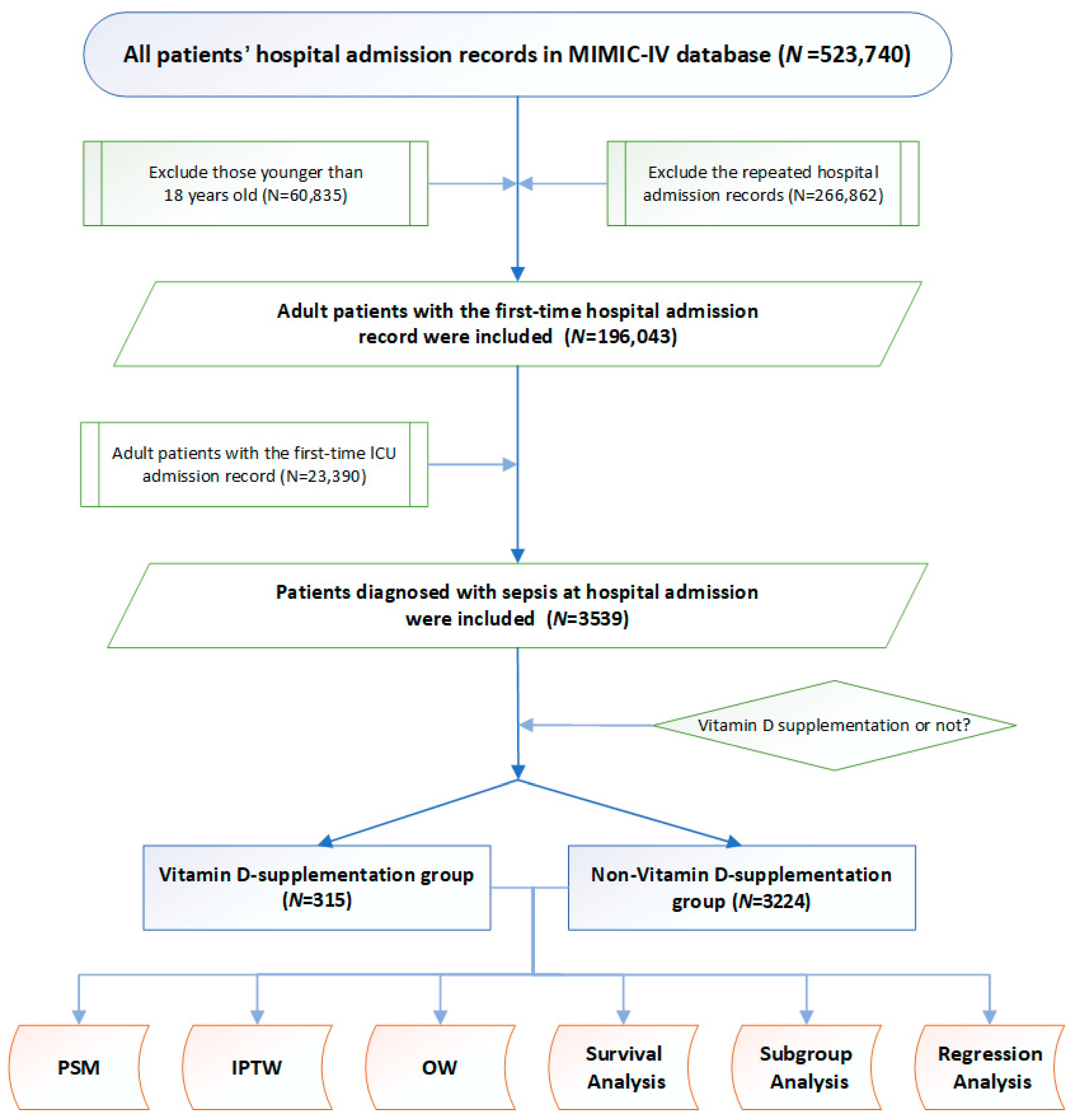
2.2. Study Design and Participants
2.3. Variable Extraction
2.4. Clinical Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Grouping of Study Participants
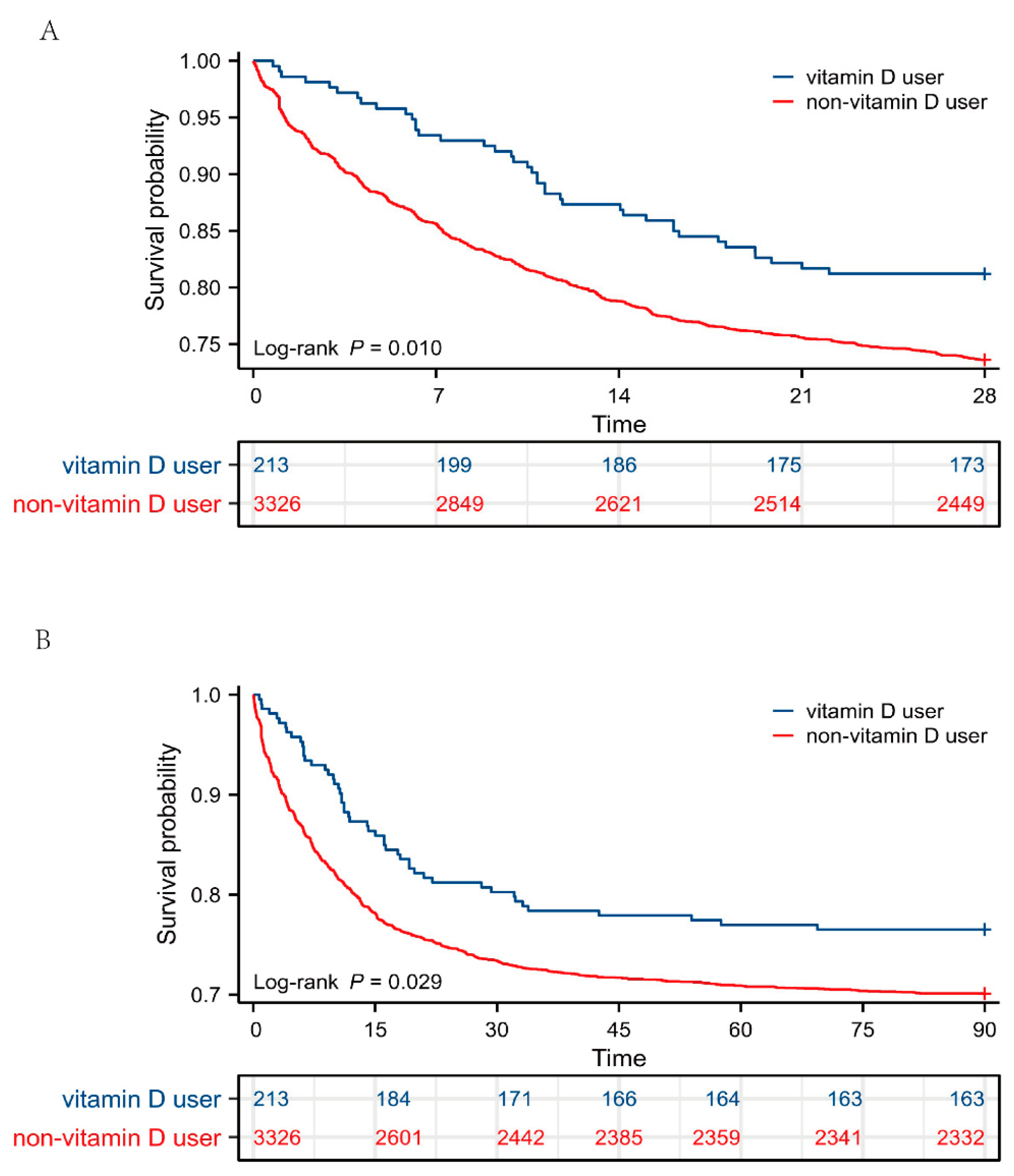
3.2. Unadjusted Clinical Outcomes and Survival Analysis
3.3. Association between Vitamin D Supplementation and Primary Outcomes Based on Multivariate Regression Analysis
3.4. Baseline Characteristics, Clinical Outcomes Post PSM
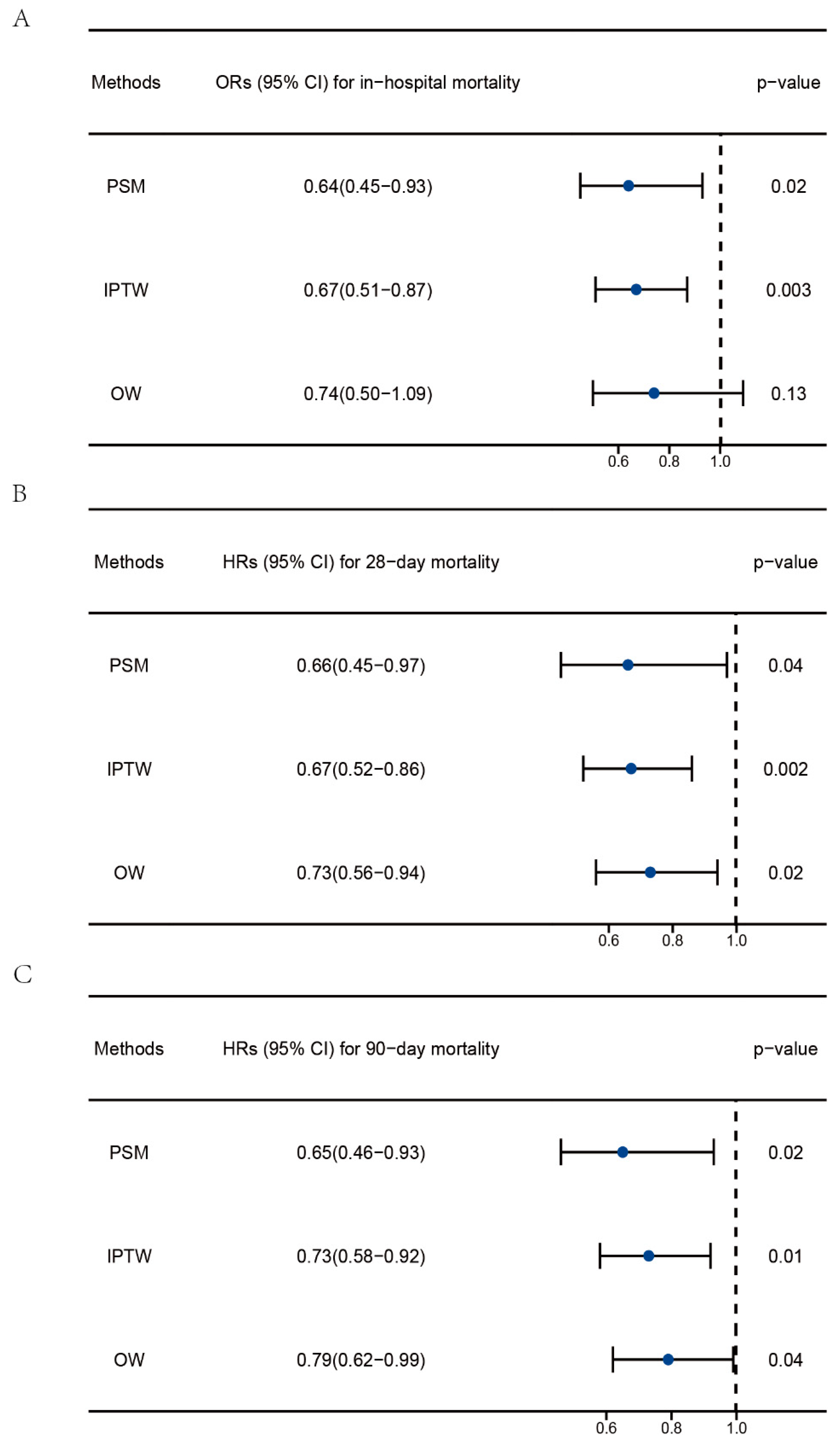
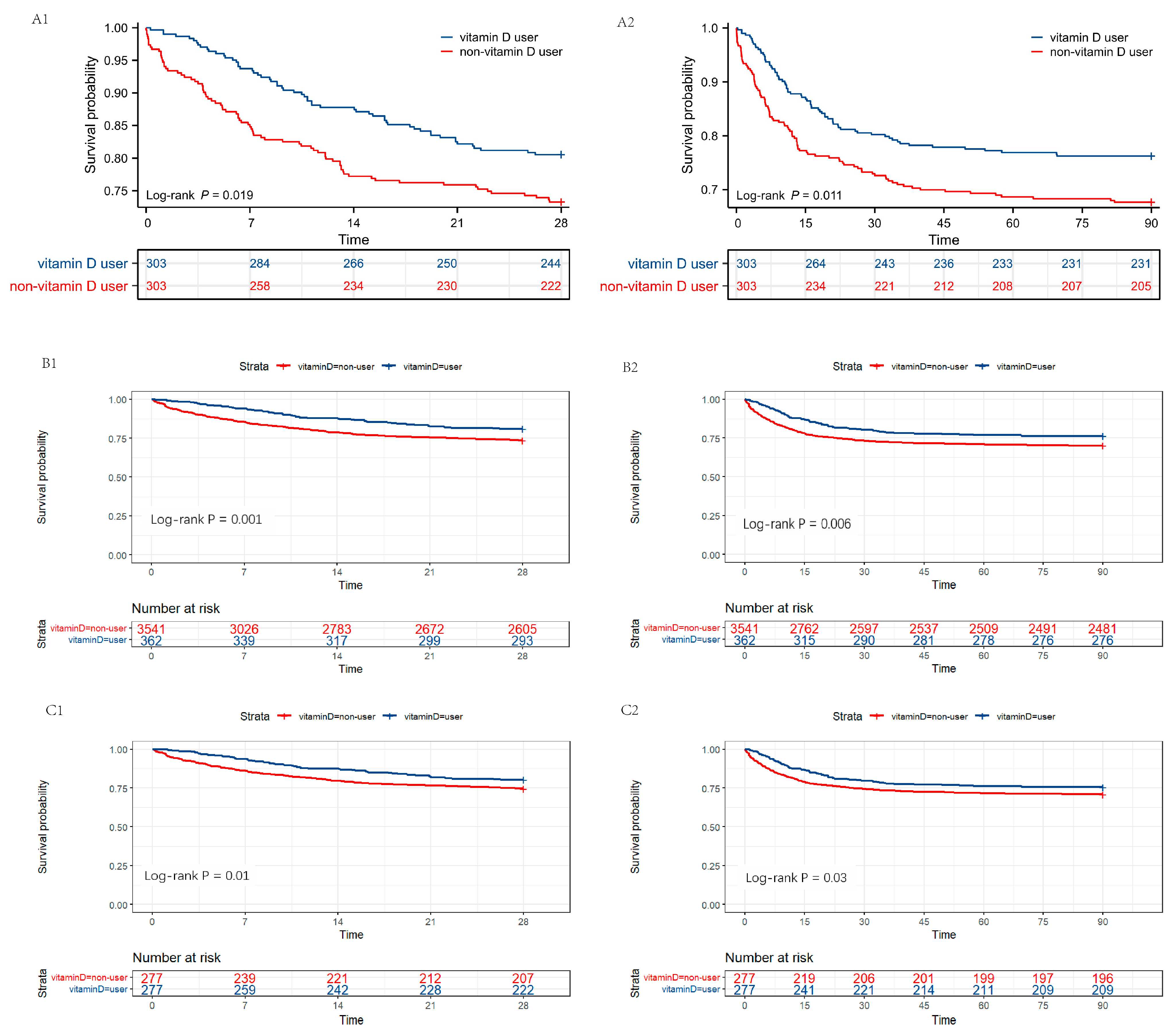
3.5. Regression Analysis and Survival Analysis Post PSM, IPTW, and OW
3.6. Subgroup Analysis
3.7. Post Hoc Analysis to Explore Whether Age and Severity of Sepsis Affect the Protective Effect of Vitamin D Supplementation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vanherwegen, A.-S.; Gysemans, C.; Mathieu, C. Regulation of Immune Function by Vitamin D and Its Use in Diseases of Immunity. Endocrinol. Metab. Clin. N. Am. 2017, 46, 1061–1094. [Google Scholar] [CrossRef]
- Bashar, S.K.; Hossain, M.B.; Ding, E.; Walkey, A.J.; McManus, D.D.; Chon, K.H. Atrial Fibrillation Detection During Sepsis: Study on MIMIC III ICU Data. IEEE J. Biomed. Health Inform. 2020, 24, 3124–3135. [Google Scholar] [CrossRef]
- Baykara, N.; Akalın, H.; Arslantaş, M.K.; Hancı, V.; Çağlayan, Ç.; Kahveci, F.; Demirağ, K.; Baydemir, C.; Ünal, N. Epidemiology of sepsis in intensive care units in Turkey: A multicenter, point-prevalence study. Crit. Care 2018, 22, 93. [Google Scholar] [CrossRef]
- Kempker, J.A.; Han, J.E.; Tangpricha, V.; Ziegler, T.R.; Martin, G.S. Vitamin D and sepsis: An emerging relationship. Dermato-Endocrinology 2012, 4, 101–108. [Google Scholar] [CrossRef]
- Takeuti, F.A.C.; Guimaraes, F.d.S.F.; Guimaraes, P.d.S.F. Applications of vitamin D in sepsis prevention. Discov. Med. 2018, 25, 291–297. [Google Scholar]
- de Haan, K.; Groeneveld, A.B.J.; de Geus, H.R.H.; Egal, M.; Struijs, A. Vitamin D deficiency as a risk factor for infection, sepsis and mortality in the critically ill: Systematic review and meta-analysis. Crit. Care 2014, 18, 660. [Google Scholar] [CrossRef]
- Li, Y.; Ding, S. Serum 25-Hydroxyvitamin D and the risk of mortality in adult patients with Sepsis: A meta-analysis. BMC Infect. Dis. 2020, 20, 189. [Google Scholar] [CrossRef]
- Upala, S.; Sanguankeo, A.; Permpalung, N. Significant association between vitamin D deficiency and sepsis: A systematic review and meta-analysis. BMC Anesth. 2015, 15, 84. [Google Scholar] [CrossRef]
- Han, J.E.; Jones, J.L.; Tangpricha, V.; Brown, M.A.; Brown, L.A.S.; Hao, L.; Hebbar, G.; Lee, M.J.; Liu, S.; Ziegler, T.R.; et al. High Dose Vitamin D Administration in Ventilated Intensive Care Unit Patients: A Pilot Double Blind Randomized Controlled Trial. J. Clin. Transl. Endocrinol. 2016, 4, 59–65. [Google Scholar] [CrossRef]
- He, M.; Cao, T.; Wang, J.; Wang, C.; Wang, Z.; Abdelrahim, M.E.A. Vitamin D deficiency relation to sepsis, paediatric risk of mortality III score, need for ventilation support, length of hospital stay, and duration of mechanical ventilation in critically ill children: A meta-analysis. Int. J. Clin. Pract. 2021, 75, e13908. [Google Scholar] [CrossRef]
- Nair, P.; Venkatesh, B.; Center, J.R. Vitamin D deficiency and supplementation in critical illness-the known knowns and known unknowns. Crit. Care 2018, 22, 276. [Google Scholar] [CrossRef] [PubMed]
- Roux, C.; Bischoff-Ferrari, H.A.; Papapoulos, S.E.; de Papp, A.E.; West, J.A.; Bouillon, R. New insights into the role of vitamin D and calcium in osteoporosis management: An expert roundtable discussion. Curr. Med. Res. Opin. 2008, 24, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.M.P.; Eslick, G.D.; Nowson, C.; Smith, C.; Bensoussan, A. Use of calcium or calcium in combination with vitamin D supplementation to prevent fractures and bone loss in people aged 50 years and older: A meta-analysis. Lancet 2007, 370, 657–666. [Google Scholar] [CrossRef]
- Lappe, J.M.; Travers-Gustafson, D.; Davies, K.M.; Recker, R.R.; Heaney, R.P. Vitamin D and calcium supplementation reduces cancer risk: Results of a randomized trial. Am. J. Clin. Nutr. 2007, 85, 1586–1591. [Google Scholar] [CrossRef]
- Bergman, P.; Lindh, A.U.; Björkhem-Bergman, L.; Lindh, J.D. Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2013, 8, e65835. [Google Scholar] [CrossRef]
- Veloudi, P.; Jones, G.; Sharman, J.E. Effectiveness of Vitamin D Supplementation for Cardiovascular Health Outcomes. Pulse 2017, 4, 193–207. [Google Scholar] [CrossRef]
- Triantos, C.; Aggeletopoulou, I.; Mantzaris, G.J.; Mouzaki, A. Molecular basis of vitamin D action in inflammatory bowel disease. Autoimmun. Rev. 2022, 21, 103136. [Google Scholar] [CrossRef]
- Vanichkulbodee, A.; Romposra, M.; Inboriboon, P.C.; Trongtrakul, K. Effects of vitamin D insufficiency on sepsis severity and risk of hospitalisation in emergency department patients: A cross-sectional study. BMJ Open 2023, 13, e064985. [Google Scholar] [CrossRef]
- Ahmad, S.; Zaki, A.; Manda, K.; Mohan, A.; Syed, M.A. Vitamin-D ameliorates sepsis-induced acute lung injury via augmenting miR-149-5p and downregulating ER stress. J. Nutr. Biochem. 2022, 110, 109130. [Google Scholar] [CrossRef]
- Luo, J.; Wang, N.; Hua, L.; Deng, F.; Liu, D.; Zhou, J.; Yuan, Y.; Ouyang, F.; Chen, X.; Long, S.; et al. The Anti-Sepsis Effect of Isocorydine Screened from Guizhou Ethnic Medicine is Closely Related to Upregulation of Vitamin D Receptor Expression and Inhibition of NFκB p65 Translocation into the Nucleus. J. Inflamm. Res. 2022, 15, 5649–5664. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, Z.; Gao, L.; Cao, Z.; Wang, Q. Effects of a single dose of vitamin D in septic children: A randomized, double-blinded, controlled trial. J. Int. Med. Res. 2020, 48, 300060520926890. [Google Scholar] [CrossRef]
- Singh, S.; Sarkar, S.; Gupta, K.; Rout, A. Vitamin D Supplementation in Critically Ill Patients: A Meta-Analysis of Randomized Controlled Trials. Cureus 2022, 14, e24625. [Google Scholar] [CrossRef] [PubMed]
- Menger, J.; Lee, Z.-Y.; Notz, Q.; Wallqvist, J.; Hasan, M.S.; Elke, G.; Dworschak, M.; Meybohm, P.; Heyland, D.K.; Stoppe, C. Administration of vitamin D and its metabolites in critically ill adult patients: An updated systematic review with meta-analysis of randomized controlled trials. Crit. Care 2022, 26, 268. [Google Scholar] [CrossRef]
- Ginde, A.A.; Brower, R.G.; Caterino, J.M.; Finck, L.; Banner-Goodspeed, V.M.; Grissom, C.K.; Hayden, D.; Hough, C.L.; Hyzy, R.C.; Khan, A.; et al. Early High-Dose Vitamin D3 for Critically Ill, Vitamin D-Deficient Patients. N. Engl. J. Med. 2019, 381, 2529–2540. [Google Scholar] [CrossRef]
- Bhattacharyya, A.; Subramaniam, R.; Baidya, D.K.; Aggarwal, P.; Wig, N. Effect of Early Administration of Vitamin D on Clinical Outcome in Critically Ill Sepsis Patients: A Randomized Placebo-controlled Trial. Indian J. Crit. Care Med. 2021, 25, 1147–1154. [Google Scholar] [CrossRef]
- Johnson, A.; Bulgarelli, L.; Pollard, T.; Horng, S.; Celi, L.A.; Mark, R. MIMIC-IV (version 1.0). PhysioNet 2021. [Google Scholar]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Nohr, E.A.; Liew, Z. How to investigate and adjust for selection bias in cohort studies. Acta Obstet. Gynecol. Scand. 2018, 97, 407–416. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.J.; Hartog, C.S.; Tsaganos, T.; Schlattmann, P.; Angus, D.C.; Reinhart, K. Assessment of Global Incidence and Mortality of Hospital-treated Sepsis. Current Estimates and Limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef]
- Vincent, J.-L. Current sepsis therapeutics. EBioMedicine 2022, 86, 104318. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Rapidly Increasing Serum 25(OH)D Boosts the Immune System, against Infections-Sepsis and COVID-19. Nutrients 2022, 14, 2997. [Google Scholar] [CrossRef] [PubMed]
- Murdaca, G.; Gangemi, S. Vitamin D in Health and Disease. Biomedicines 2022, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Miao, D.; Goltzman, D. Mechanisms of action of vitamin D in delaying aging and preventing disease by inhibiting oxidative stress. Vitam. Horm. 2023, 121, 293–318. [Google Scholar] [CrossRef]
- Liu, P.T.; Stenger, S.; Li, H.; Wenzel, L.; Tan, B.H.; Krutzik, S.R.; Ochoa, M.T.; Schauber, J.; Wu, K.; Meinken, C.; et al. Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science 2006, 311, 1770–1773. [Google Scholar] [CrossRef]
- Sadeghi, K.; Wessner, B.; Laggner, U.; Ploder, M.; Tamandl, D.; Friedl, J.; Zügel, U.; Steinmeyer, A.; Pollak, A.; Roth, E.; et al. Vitamin D3 down-regulates monocyte TLR expression and triggers hyporesponsiveness to pathogen-associated molecular patterns. Eur. J. Immunol. 2006, 36, 361–370. [Google Scholar] [CrossRef]
- Yeh, C.-L.; Wu, J.-M.; Yang, P.-J.; Lee, P.-C.; Chen, K.-Y.; Yeh, S.-L.; Lin, M.-T. Intravenous calcitriol treatment benefits the homeostasis of CD4+ T cells and attenuates kidney injury in obese mice complicated with polymicrobial sepsis. Nutrition 2022, 103–104, 111741. [Google Scholar] [CrossRef]
- Shiozawa, K.; Shiozawa, S.; Shimizu, S.; Fujita, T. 1 alpha,25-dihydroxyvitamin D3 inhibits pokeweed mitogen-stimulated human B-cell activation: An analysis using serum-free culture conditions. Immunology 1985, 56, 161–167. [Google Scholar]
- Horiuchi, H.; Nagata, I.; Komoriya, K. Protective effect of vitamin D3 analogues on endotoxin shock in mice. Agents Actions 1991, 33, 343–348. [Google Scholar] [CrossRef]
- Zhang, H.; Liu, Y.; Fang, X.; Gu, L.; Luo, C.; Chen, L.; Wang, Q. Vitamin D3 Protects Mice from Diquat-Induced Oxidative Stress through the NF-κB/Nrf2/HO-1 Signaling Pathway. Oxid. Med. Cell. Longev. 2021, 2021, 6776956. [Google Scholar] [CrossRef]
- Sarhan, N.; Abou Warda, A.E.; Sarhan, R.M.; Boshra, M.S.; Mostafa-Hedeab, G.; Alruwaili, B.F.; Ibrahim, H.S.G.; Schaalan, M.F.; Fathy, S. Evidence for the Efficacy of a High Dose of Vitamin D on the Hyperinflammation State in Moderate-to-Severe COVID-19 Patients: A Randomized Clinical Trial. Medicina 2022, 58, 1358. [Google Scholar] [CrossRef]
- Moreno-Torres, V.; Royuela, A.; Múñez, E.; Ortega, A.; Gutierrez, Á.; Mills, P.; Ramos-Martínez, A. Better prognostic ability of NEWS2, SOFA and SAPS-II in septic patients. Med. Clin. 2022, 159, 224–229. [Google Scholar] [CrossRef]
- García-Rodríguez, J.F.; Mariño-Callejo, A. The factors associated with the trend in incidence of Bacteraemia and associated mortality over 30 years. BMC Infect. Dis. 2023, 23, 69. [Google Scholar] [CrossRef]
- Fan, J.; Fu, S.; Chen, X.; Li, Y.; Zhao, Y.; Lv, F.; Yao, Y. Thyroid nodules and its association with vitamin D in centenarians. Exp. Gerontol. 2022, 161, 111730. [Google Scholar] [CrossRef]
- Vandenbroucke, A.; Luyten, F.P.; Flamaing, J.; Gielen, E. Pharmacological treatment of osteoporosis in the oldest old. Clin. Interv. Aging 2017, 12, 1065–1077. [Google Scholar] [CrossRef]
- Marcos-Pérez, D.; Sánchez-Flores, M.; Proietti, S.; Bonassi, S.; Costa, S.; Teixeira, J.P.; Fernández-Tajes, J.; Pásaro, E.; Valdiglesias, V.; Laffon, B. Low Vitamin D Levels and Frailty Status in Older Adults: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2286. [Google Scholar] [CrossRef]
- Chae, B.; Kim, Y.-J.; Kim, S.M.; Hong, S.-I.; Shin, Y.S.; Kim, J.-S.; Ryoo, S.M.; Kim, W.Y. Vitamin D deficiency on admission to the emergency department is a mortality predictor for patients with septic shock treated with early protocol-driven resuscitation bundle therapy. Am. J. Med. Sci. 2022, 365, 361–367. [Google Scholar] [CrossRef]
- Amrein, K.; Litonjua, A.A.; Moromizato, T.; Quraishi, S.A.; Gibbons, F.K.; Pieber, T.R.; Camargo, C.A.; Giovannucci, E.; Christopher, K.B. Increases in pre-hospitalization serum 25(OH)D concentrations are associated with improved 30-day mortality after hospital admission: A cohort study. Clin. Nutr. 2016, 35, 514–521. [Google Scholar] [CrossRef]
- Nair, P.; Venkatesh, B.; Lee, P.; Kerr, S.; Hoechter, D.J.; Dimeski, G.; Grice, J.; Myburgh, J.; Center, J.R. A Randomized Study of a Single Dose of Intramuscular Cholecalciferol in Critically Ill Adults. Crit. Care Med. 2015, 43, 2313–2320. [Google Scholar] [CrossRef]
- Amrein, K.; Sourij, H.; Wagner, G.; Holl, A.; Pieber, T.R.; Smolle, K.H.; Stojakovic, T.; Schnedl, C.; Dobnig, H. Short-term effects of high-dose oral vitamin D3 in critically ill vitamin D deficient patients: A randomized, double-blind, placebo-controlled pilot study. Crit. Care 2011, 15, R104. [Google Scholar] [CrossRef]
- Lagu, T.; Rothberg, M.B.; Shieh, M.-S.; Pekow, P.S.; Steingrub, J.S.; Lindenauer, P.K. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit. Care Med. 2012, 40, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Meyer, N.; Harhay, M.O.; Small, D.S.; Prescott, H.C.; Bowles, K.H.; Gaieski, D.F.; Mikkelsen, M.E. Temporal Trends in Incidence, Sepsis-Related Mortality, and Hospital-Based Acute Care After Sepsis. Crit. Care Med. 2018, 46, 354–360. [Google Scholar] [CrossRef] [PubMed]
- Schleicher, R.L.; Sternberg, M.R.; Lacher, D.A.; Sempos, C.T.; Looker, A.C.; Durazo-Arvizu, R.A.; Yetley, E.A.; Chaudhary-Webb, M.; Maw, K.L.; Pfeiffer, C.M.; et al. The vitamin D status of the US population from 1988 to 2010 using standardized serum concentrations of 25-hydroxyvitamin D shows recent modest increases. Am. J. Clin. Nutr. 2016, 104, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, D.; Lee, H.; Greendale, G.; Cauley, J.; Burnett, S.-A.; Finkelstein, J. Increasing 25-hydroxyvitamin D. levels over time: The Study of Women’s Health Across the Nation (SWAN). J. Bone Miner. Res. 2014, 29, S25. [Google Scholar]
- Lee, S.; Teschemaker, A.R.; Daniel, M.; Maneno, M.K.; Johnson, A.A.; Wutoh, A.K.; Lee, E. Calcium and Vitamin D Use among Older Adults in U.S.: Results from National Survey. J. Nutr. Health Aging 2016, 20, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Gohil, S.K.; Cao, C.; Phelan, M.; Tjoa, T.; Rhee, C.; Platt, R.; Huang, S.S. Impact of Policies on the Rise in Sepsis Incidence, 2000–2010. Clin. Infect. Dis. 2016, 62, 695–703. [Google Scholar] [CrossRef]
- Levy, M.M.; Pronovost, P.J.; Dellinger, R.P.; Townsend, S.; Resar, R.K.; Clemmer, T.P.; Ramsay, G. Sepsis change bundles: Converting guidelines into meaningful change in behavior and clinical outcome. Crit. Care Med. 2004, 32, S595–S597. [Google Scholar] [CrossRef]
- Levy, M.M.; Dellinger, R.P.; Townsend, S.R.; Linde-Zwirble, W.T.; Marshall, J.C.; Bion, J.; Schorr, C.; Artigas, A.; Ramsay, G.; Beale, R.; et al. The Surviving Sepsis Campaign: Results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010, 36, 222–231. [Google Scholar] [CrossRef]
- Fang, X.; Wang, Z.; Yang, J.; Cai, H.; Yao, Z.; Li, K.; Fang, Q. Clinical Evaluation of Sepsis-1 and Sepsis-3 in the ICU. Chest 2018, 153, 1169–1176. [Google Scholar] [CrossRef]
- Vincenzi, B.; Napolitano, A.; Fiocco, M.; Mir, O.; Rutkowski, P.; Blay, J.-Y.; Reichardt, P.; Joensuu, H.; Fumagalli, E.; Gennatas, S.; et al. Adjuvant Imatinib in Patients with GIST Harboring Exon 9 KIT Mutations: Results from a Multi-institutional European Retrospective Study. Clin. Cancer Res. 2022, 28, 1672–1679. [Google Scholar] [CrossRef]
- Minneci, P.C.; Hade, E.M.; Lawrence, A.E.; Sebastião, Y.V.; Saito, J.M.; Mak, G.Z.; Fox, C.; Hirschl, R.B.; Gadepalli, S.; Helmrath, M.A.; et al. Association of Nonoperative Management Using Antibiotic Therapy vs Laparoscopic Appendectomy With Treatment Success and Disability Days in Children With Uncomplicated Appendicitis. JAMA 2020, 324, 581–593. [Google Scholar] [CrossRef] [PubMed]
- Aminian, A.; Al-Kurd, A.; Wilson, R.; Bena, J.; Fayazzadeh, H.; Singh, T.; Albaugh, V.L.; Shariff, F.U.; Rodriguez, N.A.; Jin, J.; et al. Association of Bariatric Surgery With Major Adverse Liver and Cardiovascular Outcomes in Patients With Biopsy-Proven Nonalcoholic Steatohepatitis. JAMA 2021, 326, 2031–2042. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Septic Patients (n = 3539) | Non-Vitamin D Supplementation Group (n = 3224) | Vitamin D Supplementation Group (n = 315) | p-Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age (years) | 68 (56–80) | 68 (56–80) | 73 (60–84) | <0.001 |
| Male (n (%)) | 1573 (44.4) | 1463 (44.0) | 110 (51.6) | 0.01 |
| Weight (kg) | 78 (65–95) | 79 (66–95) | 73 (62–91) | 0.03 |
| Vital signs | ||||
| RR (/min) | 21 (18–24) | 21 (18–24) | 21 (18–24) | 0.06 |
| SBP (mmHg) | 113 (98–130) | 113 (98–130) | 111 (97–130) | 0.08 |
| DBP (mmHg) | 57 (49–67) | 57 (49–67) | 59 (49–69) | 0.59 |
| Temperature (°C) | 36.9 (36.6–37.3) | 36.9 (36.6–37.3) | 36.8 (36.6–37.2) | 0.35 |
| Comorbidities | ||||
| Cerebral diseases (n (%)) | 399 (11.3) | 356 (11.0) | 43 (13.7) | 0.16 |
| MI (n (%)) | 303 (8.6) | 279 (8.7) | 24 (7.6) | 0.60 |
| AF (n (%)) | 192 (5.4) | 175 (5.3) | 17 (8.0) | 0.049 |
| CHF (n (%)) | 749 (21.2) | 697 (21.0) | 52 (24.4) | 0.001 |
| CKD (n (%)) | 858 (24.2) | 804 (24.2) | 54 (25.4) | 0.30 |
| AKI (n (%)) | 2257 (63.8) | 2132 (64.1) | 125 (58.7) | 0.36 |
| Diabetes (n (%)) | 1171 (33.1) | 1054 (32.7) | 117 (37.1) | 0.12 |
| Osteoporosis (n (%)) | 208 (5.9) | 157 (4.9) | 51 (16.2) | <0.001 |
| Septic shock (n (%)) | 2043 (57.7) | 1930 (58.0) | 113 (53.1) | 0.17 |
| Clinical indices | ||||
| RBC (m/μL) | 3.3 (2.9–3.8) | 3.3 (2.9–3.8) | 3.3 (2.9–3.8) | 0.61 |
| WBC (K/μL) | 10.3 (6.9–15.5) | 10.4 (7.0–15.5) | 9.2 (6.0–14.7) | 0.75 |
| Platelet (K/μL) | 191 (123–282) | 190 (123–282) | 203 (127–284) | 0.30 |
| Hemoglobin (g/dL) | 9.9 (8.7–11.2) | 9.9 (8.7–11.3) | 9.8 (8.5–11.2) | 0.21 |
| Creatinine (mg/dL) | 1.1 (0.7–2.0) | 1.1 (0.7–2.0) | 1.1 (0.7–1.9) | 0.21 |
| Glucose (mmol/L) | 118 (96–154) | 119 (97–155) | 111 (88–136) | 0.002 |
| Lactate (mg/dL) | 1.7 (1.2–2.8) | 1.7 (1.2–2.8) | 1.7 (1.2–2.9) | 0.30 |
| Potassium (mmol/L) | 4.0 (3.7–4.4) | 4.0 (3.7–4.4) | 4.0 (3.7–4.4) | >0.90 |
| Chloride (mmol/L) | 104 (100–108) | 104 (100–108) | 103 (100–108) | 0.03 |
| Treatment measures | ||||
| Vasopressin (n (%)) | 837 (23.7) | 784 (23.6) | 53 (24.9) | 0.63 |
| Antibiotic (n (%)) | 3468 (98.0) | 3262 (81.1) | 206 (96.7) | 0.29 |
| MV (n (%)) | 2991 (84.5) | 2816 (84.7) | 175 (82.2) | 0.33 |
| Clinical Outcomes | All Septic Patients (n = 3539) | Non-Vitamin D Supplementation Group (n = 3224) | Vitamin D Supplementation Group (n = 315) | p-Value |
|---|---|---|---|---|
| Primary outcomes | ||||
| In-hospital mortality (n (%)) | 987 (27.9) | 944 (28.4) | 43 (20.2) | 0.01 * |
| 28-mortality (n (%)) | 917 (25.9) | 877 (26.4) | 40 (18.8) | 0.01 * |
| 90-mortality (n (%)) | 1044 (29.5) | 994 (29.9) | 50 (23.5) | 0.03 * |
| Secondary outcomes | ||||
| Mean SAPS II | 44 (35–52) | 44 (35–52) | 42 (33–49) | 0.04 * |
| Mean APS III | 62 (46–82) | 62 (47–83) | 55 (43–73) | <0.001 * |
| Mean SOFA | 7 (4–10) | 7 (5–10) | 6 (4–8) | <0.001 * |
| ICU LOS (days) | 3.0 (1.6–7.2) | 3.0 (1.7–7.3) | 2.7 (1.6–5.6) | 0.12 |
| Hospital LOS (days) | 9.9 (5.5–17.9) | 9.9 (5.5–18.0) | 9.7 (5.7–16.2) | 0.11 |
| HRs for 28-Day Mortality | HRs for 90-Day Mortality | ORs for in-Hospital Mortality | |
|---|---|---|---|
| Model 1 | 0.68 (0.52–0.88) | 0.75 (0.59–0.94) | 0.68 (0.51–0.90) |
| Model 2 | 0.63 (0.49–0.82) | 0.70 (0.56–0.89) | 0.64 (0.48–0.85) |
| Model 3 | 0.67 (0.48–0.92) | 0.74 (0.55–0.99) | 0.69 (0.50–0.94) |
| All Septic Patients (n = 606) | Non-Vitamin D Supplementation Group (n = 303) | Vitamin D Supplementation Group (n = 303) | p-Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age (years) | 72 (60–83) | 72 (61–82) | 72 (60–85) | 0.42 |
| Male (n (%)) | 317 (52.3) | 158 (52.1) | 159 (52.5) | >0.90 |
| Weight (kg) | 76 (64–92) | 77 (65–92) | 76 (64–91) | 0.57 |
| Vital signs | ||||
| RR (/min) | 21 (18–24) | 21 (18–24) | 21 (18–23) | 0.33 |
| SBP (mmHg) | 111 (96–129) | 111 (96–127) | 111 (96–130) | 0.74 |
| DBP (mmHg) | 57 (48–67) | 55 (45–66) | 59 (50–69) | 0.08 |
| Temperature (°C) | 36.8 (36.6–37.3) | 36.9 (36.6–37.3) | 36.8 (36.6–37.2) | 0.22 |
| Comorbidities | ||||
| MI (n (%)) | 48 (7.9) | 25 (8.3) | 23 (7.6) | 0.89 |
| AF (n (%)) | 46 (7.6) | 23 (7.6) | 23 (7.6) | >0.90 |
| HF (n (%)) | 164 (27.1) | 78 (25.7) | 86 (28.4) | 0.52 |
| CKD (n (%)) | 171 (28.2) | 92 (30.4) | 79 (26.1) | 0.28 |
| AKI (n (%)) | 379 (62.5) | 195 (64.4) | 184 (60.7) | 0.40 |
| Diabetes (n (%)) | 239 (39.4) | 128 (42.2) | 111 (36.6) | 0.18 |
| Osteoporosis (n (%)) | 106 (17.5) | 56 (18.5) | 50 (16.5) | 0.60 |
| Septic shock (n (%)) | 330 (54.5) | 166 (54.8) | 164 (54.1) | >0.90 |
| Cerebral diseases (n (%)) | 75 (12.4) | 37 (12.2) | 38 (12.5) | >0.90 |
| Clinical indices | ||||
| RBC (m/μL) | 3.3 (2.9–3.8) | 3.3 (2.9–3.9) | 3.3 (2.9–3.7) | 0.44 |
| WBC (K/μL) | 9.7 (6.2–15.3) | 9.6 (6.2–15.3) | 9.7 (6.1–15.2) | 0.60 |
| Platelet (K/μL) | 191 (129–272) | 187 (129–260) | 201 (129–283) | 0.44 |
| Hemoglobin (g/dL) | 9.9 (8.6–11.2) | 9.9 (8.7–11.2) | 9.9 (8.6–11.2) | 0.40 |
| Creatinine (mg/dL) | 1.1 (0.7–1.8) | 1.1 (0.8–1.8) | 1.0 (0.7–1.7) | 0.41 |
| Glucose (mmol/L) | 113 (92–142) | 112 (94–145) | 113 (90–142) | 0.66 |
| Lactate (mg/dL) | 1.7 (1.2–2.8) | 1.7 (1.1–2.9) | 1.7 (1.2–2.8) | 0.83 |
| Potassium (mmol/L) | 4.1 (3.7–4.5) | 4.0 (3.7–4.5) | 4.1 (3.7–4.4) | 0.56 |
| Chloride (mmol/L) | 103 (100–108) | 104 (100–108) | 103 (100–107) | 0.59 |
| Severity-related scores | ||||
| SOFA | 6 (4–9) | 6 (4–9) | 6 (4–9) | >0.90 |
| SAPS II | 42 (35–50) | 42 (36–50) | 41 (34–50) | >0.90 |
| APS III | 61 (47–75) | 61 (49–78) | 61 (46–72) | 0.09 |
| Clinical measures | ||||
| Vasopressin (n (%)) | 167 (27.6) | 88 (29.0) | 79 (26.1) | 0.47 |
| Antibiotic (n (%)) | 588 (97.0) | 294 (97.0) | 294 (97.0) | >0.90 |
| MV (n (%)) | 501 (82.7) | 251 (82.8) | 250 (82.5) | >0.90 |
| Clinical Outcomes | All Septic Patients (n = 606) | Non-Vitamin D Supplementation Group (n = 303) | Vitamin D Supplementation Group (n = 303) | p-Value |
|---|---|---|---|---|
| Primary outcomes | ||||
| In-hospital mortality (n (%)) | 155 (25.6) | 90 (29.7) | 65 (21.5) | 0.03 * |
| 28-day mortality (n (%)) | 140 (23.1) | 81 (26.7) | 59 (19.5) | 0.04 * |
| 90-day mortality (n (%)) | 170 (28.1) | 98 (32.3) | 72 (23.8) | 0.02 * |
| Secondary outcomes | ||||
| Mean SAPS II | 41 (34–50) | 42 (35–51) | 40 (32–49) | 0.12 |
| Mean APS III | 59 (45–78) | 62 (48–82) | 54 (43–73) | 0.001 * |
| Mean SOFA | 6 (4–9) | 7 (4–10) | 6 (4–8) | <0.001 * |
| ICU LOS (days) | 2.8 (1.6–6) | 3 (1.6–6.6) | 2.7 (1.5–5.6) | >0.90 |
| Hospital LOS (days) | 8.9 (5.4–15.7) | 8.3 (5.0–15.0) | 9.7 (5.7–16.4) | 0.21 |
| Number of Patients | OR for in-Hospital Mortality | HR for 28-Day Mortality | HR for 90-Day Mortality | p-Values for Interaction | |
|---|---|---|---|---|---|
| Age | 0.08 | ||||
| >60 | 2421 | 0.57 (0.42–0.79) | 0.62 (0.46–0.82) | 0.67 (0.49–0.93) | |
| <60 | 1118 | 1.01 (0.58–1.76) | 0.85 (0.46–1.57) | 1.10 (0.64–1.88) | |
| Gender | 0.75 | ||||
| Male | 1573 | 0.65 (0.44–0.96) | 0.63 (0.44–0.90) | 0.71 (0.52–0.98) | |
| Female | 1966 | 0.63 (0.42–0.96) | 0.63 (0.43–0.93) | 0.68 (0.48–0.97) | |
| Septic shock | 0.10 | ||||
| Yes | 2043 | 0.60 (0.41–0.86) | 0.62 (0.45–0.86) | 0.67 (0.47–0.86) | |
| No | 1496 | 0.88 (0.56–1.37) | 0.84 (0.53–1.34) | 1.06 (0.70–1.60) | |
| CHF | 0.53 | ||||
| Yes | 749 | 0.56 (0.31–0.99) | 0.56 (0.33–0.95) | 0.60 (0.37–0.98) | |
| No | 2790 | 0.70 (0.50–0.91) | 0.67 (0.50–0.91) | 0.75 (0.58–0.99) | |
| AKI | 0.80 | ||||
| Yes | 2257 | 0.70 (0.50–0.98) | 0.68 (0.50–0.92) | 0.76 (0.58–0.99) | |
| No | 1282 | 0.55 (0.32–0.95) | 0.58 (0.35–0.96) | 0.62 (0.39–0.99) | |
| CKD | 0.53 | ||||
| Yes | 858 | 0.56 (0.32–0.99) | 0.57 (0.34–0.96) | 0.62 (0.38–0.99) | |
| No | 2681 | 0.71 (0.51–0.99) | 0.67 (0.50–0.91) | 0.72 (0.55–0.95) | |
| osteoporosis | 0.75 | ||||
| Yes | 208 | 0.35 (0.15–0.79) | 0.37 (0.17–0.82) | 0.42 (0.21–0.85) | |
| No | 3331 | 0.69 (0.51–0.94) | 0.68 (0.52–0.90) | 0.75 (0.59–0.97) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, B.; Zhu, Y.; Zheng, X.; Li, T.; Niu, K.; Wang, Z.; Lu, X.; Zhang, Y.; Shen, C. Vitamin D Supplementation during Intensive Care Unit Stay Is Associated with Improved Outcomes in Critically Ill Patients with Sepsis: A Cohort Study. Nutrients 2023, 15, 2924. https://doi.org/10.3390/nu15132924
Yang B, Zhu Y, Zheng X, Li T, Niu K, Wang Z, Lu X, Zhang Y, Shen C. Vitamin D Supplementation during Intensive Care Unit Stay Is Associated with Improved Outcomes in Critically Ill Patients with Sepsis: A Cohort Study. Nutrients. 2023; 15(13):2924. https://doi.org/10.3390/nu15132924
Chicago/Turabian StyleYang, Boshen, Yuankang Zhu, Xinjie Zheng, Taixi Li, Kaifan Niu, Zhixiang Wang, Xia Lu, Yan Zhang, and Chengxing Shen. 2023. "Vitamin D Supplementation during Intensive Care Unit Stay Is Associated with Improved Outcomes in Critically Ill Patients with Sepsis: A Cohort Study" Nutrients 15, no. 13: 2924. https://doi.org/10.3390/nu15132924
APA StyleYang, B., Zhu, Y., Zheng, X., Li, T., Niu, K., Wang, Z., Lu, X., Zhang, Y., & Shen, C. (2023). Vitamin D Supplementation during Intensive Care Unit Stay Is Associated with Improved Outcomes in Critically Ill Patients with Sepsis: A Cohort Study. Nutrients, 15(13), 2924. https://doi.org/10.3390/nu15132924