
Higher Potassium Intake and Lower Sodium Intake May Help in Reducing CVD Risk by Lowering Salt Sensitivity of Blood Pressure in the Han Chinese Population
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Collection
2.2. Assessment of SSBP
2.3. Measurements for Sodium and Potassium Excretion
2.4. Measurements for 10-Year CVD Risk
2.5. Statistic Methods
3. Results
3.1. Study Population and Baseline Characteristics
3.2. Association of SSBP with the 10-Year CVD Risk
3.3. Association of Sodium, Potassium, and Sodium:Potassium Ratio with the 10-Year CVD Risk
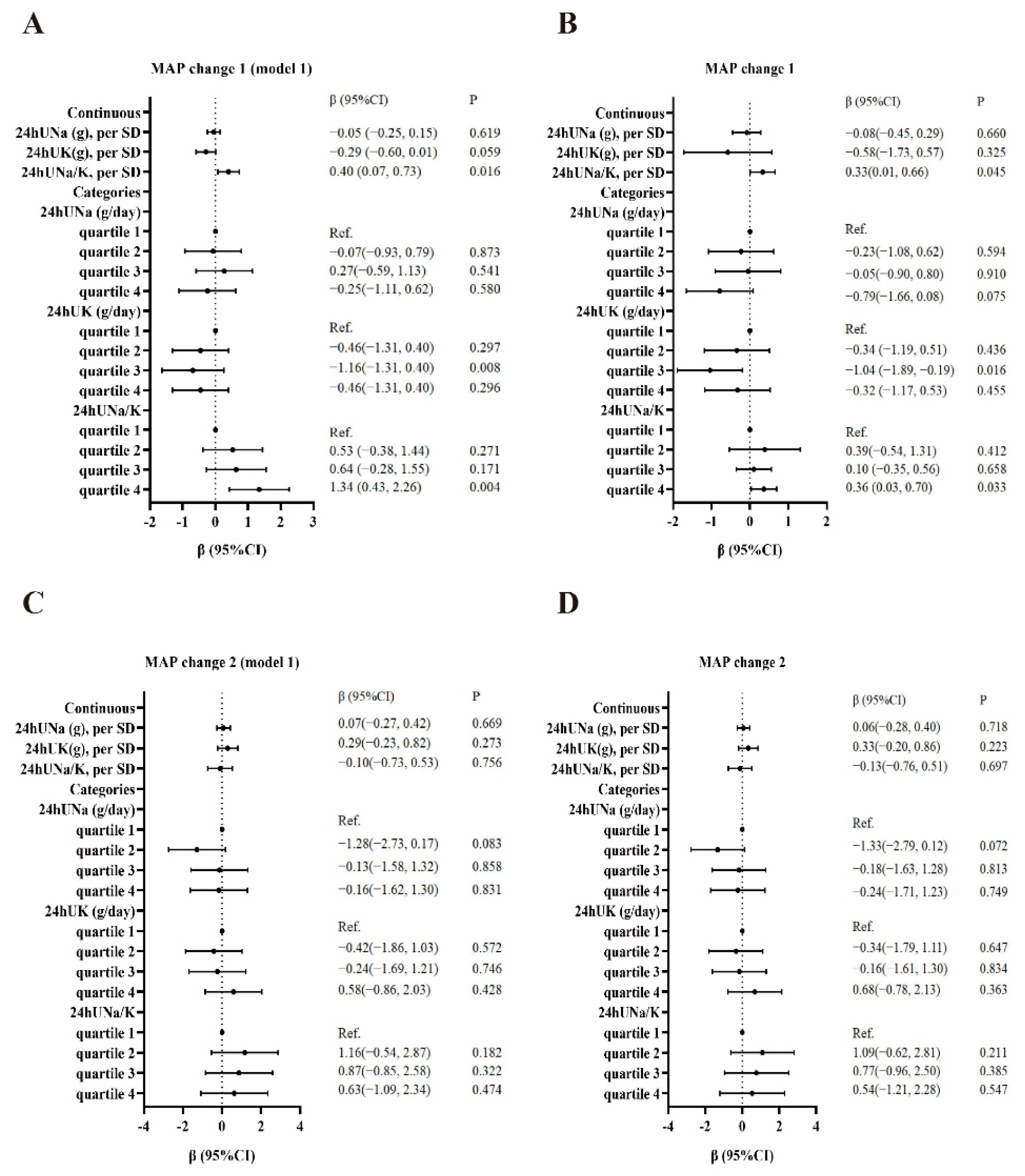
3.4. Association of Sodium, Potassium, and Sodium:Potassium Ratio with the SSBP
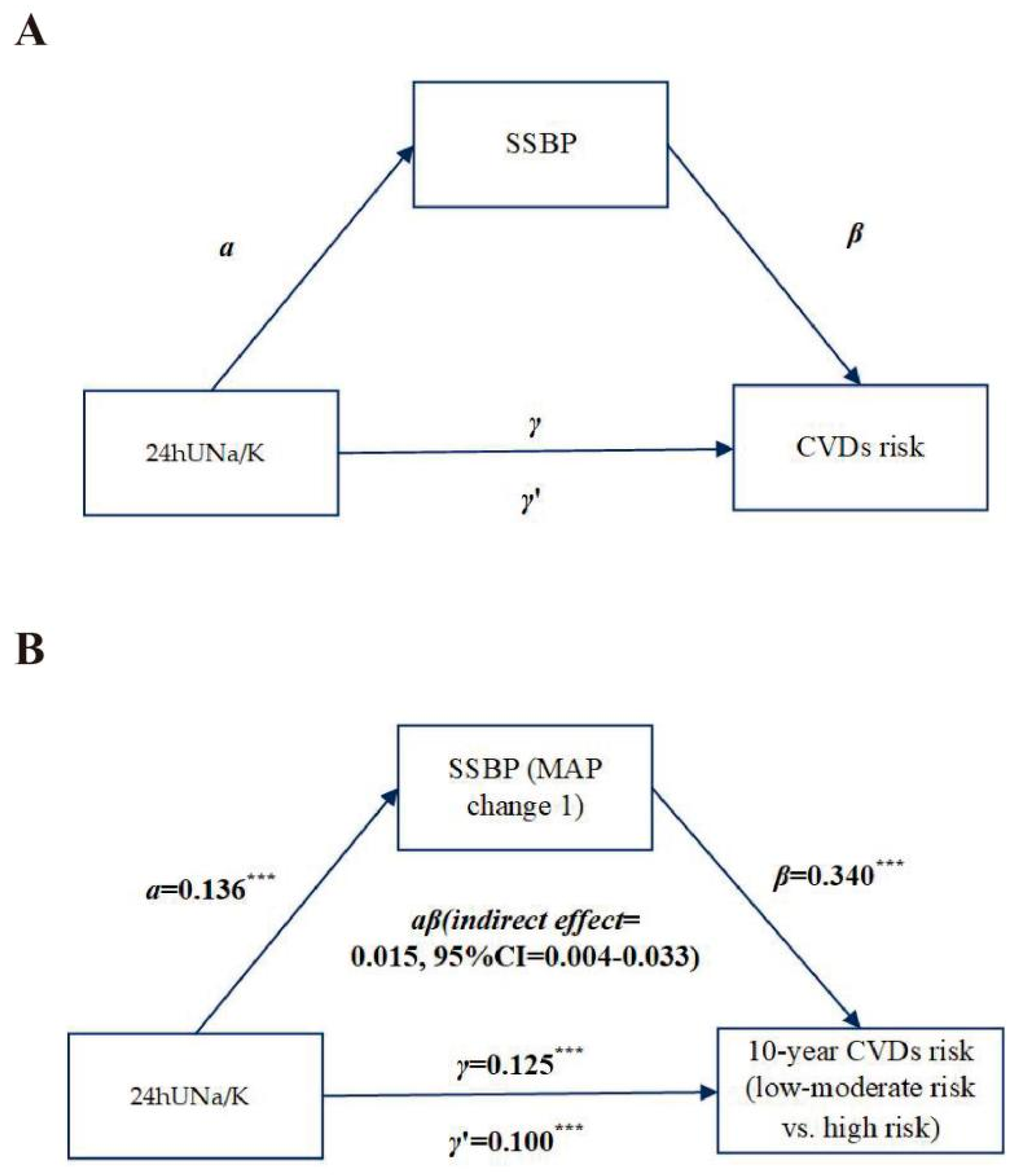
3.5. Mediation Effect of SSBP between Urinary Sodium:Potassium Ratio and the 10-Year CVD Risk
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elijovich, F.; Weinberger, M.H.; Anderson, C.A.; Appel, L.J.; Bursztyn, M.; Cook, N.R.; Dart, R.A.; Newton-Cheh, C.H.; Sacks, F.M.; Laffer, C.L.; et al. Salt Sensitivity of Blood Pressure: A Scientific Statement From the American Heart Association. Hypertension 2016, 68, e7–e46. [Google Scholar] [CrossRef]
- Orlov, S.N.; Mongin, A.A. Salt-sensing mechanisms in blood pressure regulation and hypertension. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H2039–H2053. [Google Scholar] [CrossRef] [PubMed]
- Iso, H. Lifestyle and cardiovascular disease in Japan. J. Atheroscler. Thromb. 2011, 18, 83–88. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Tan, M.; Ma, Y.; MacGregor, G.A. Salt Reduction to Prevent Hypertension and Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 632–647. [Google Scholar] [CrossRef] [PubMed]
- Mente, A.; O’Donnell, M.J.; Rangarajan, S.; McQueen, M.J.; Poirier, P.; Wielgosz, A.; Morrison, H.; Li, W.; Wang, X.; Di, C.; et al. Association of urinary sodium and potassium excretion with blood pressure. N. Engl. J. Med. 2014, 371, 601–611. [Google Scholar] [CrossRef]
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.J.; Wang, X.; Liu, L.; Yan, H.; Lee, S.F.; Mony, P.; Devanath, A.; et al. Urinary sodium and potassium excretion, mortality, and cardiovascular events. N. Engl. J. Med. 2014, 371, 612–623. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.; Mente, A.; Rangarajan, S.; McQueen, M.J.; O’Leary, N.; Yin, L.; Liu, X.; Swaminathan, S.; Khatib, R.; Rosengren, A.; et al. Joint association of urinary sodium and potassium excretion with cardiovascular events and mortality: Prospective cohort study. BMJ 2019, 364, l772. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Gao, X.; Zhou, L.; Wu, Y.; Li, Y.; Mai, J.; Nie, Z.; Wu, Y.; Liu, X.; Zhao, L. Urinary sodium excretion and risk of cardiovascular disease in the Chinese population: A prospective study. Hypertens. Res. 2018, 41, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Guo, X.; Lu, Z.; Tang, J.; Li, Y.; Xu, A.; Liu, S. Cardiovascular Diseases Deaths Attributable to High Sodium Intake in Shandong Province, China. J. Am. Heart Assoc. 2019, 8, e010737. [Google Scholar] [CrossRef]
- He, J.; Gu, D.; Chen, J.; Jaquish, C.E.; Rao, D.C.; Hixson, J.E.; Chen, J.C.; Duan, X.; Huang, J.F.; Chen, C.S.; et al. Gender difference in blood pressure responses to dietary sodium intervention in the GenSalt study. J. Hypertens. 2009, 27, 48–54. [Google Scholar] [CrossRef]
- Morimoto, A.; Uzu, T.; Fujii, T.; Nishimura, M.; Kuroda, S.; Nakamura, S.; Inenaga, T.; Kimura, G. Sodium sensitivity and cardiovascular events in patients with essential hypertension. Lancet 1997, 350, 1734–1737. [Google Scholar] [CrossRef]
- Morris, R.C., Jr.; Sebastian, A.; Forman, A.; Tanaka, M.; Schmidlin, O. Normotensive salt sensitivity: Effects of race and dietary potassium. Hypertension 1999, 33, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Ganguli, M.; Tobian, L. Dietary K determines NaCl sensitivity in NaCl-induced rises of blood pressure in spontaneously hypertensive rats. Am. J. Hypertens. 1990, 3, 482–484. [Google Scholar] [CrossRef]
- Dahl, L.K.; Leitl, G.; Heine, M. Influence of dietary potassium and sodium/potassium molar ratios on the development of salt hypertension. J. Exp. Med. 1972, 136, 318–330. [Google Scholar] [CrossRef]
- Yang, X.; Li, J.; Hu, D.; Chen, J.; Li, Y.; Huang, J.; Liu, X.; Liu, F.; Cao, J.; Shen, C.; et al. Predicting the 10-Year Risks of Atherosclerotic Cardiovascular Disease in Chinese Population: The China-PAR Project (Prediction for ASCVD Risk in China). Circulation 2016, 134, 1430–1440. [Google Scholar] [CrossRef]
- Conroy, R.M.; Pyorala, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetiere, P.; Jousilahti, P.; Keil, U.; et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Qi, H.; Liu, B.; Guo, C.; Liu, Z.; Cao, H.; Liu, K.; Sun, W.; Zhang, L. Effects of environmental and genetic risk factors for salt sensitivity on blood pressure in northern China: The systemic epidemiology of salt sensitivity (EpiSS) cohort study. BMJ Open 2018, 8, e023042. [Google Scholar] [CrossRef]
- Liu, L.-S. 2010 Chinese guidelines for the management of hypertension. Zhonghua Xin Xue Guan Bing Za Zhi 2011, 39, 579–615. [Google Scholar] [PubMed]
- Liu, Z.; Qi, H.; Liu, B.; Liu, K.; Wu, J.; Cao, H.; Zhang, J.; Yan, Y.; He, Y.; Zhang, L. Genetic susceptibility to salt-sensitive hypertension in a Han Chinese population: A validation study of candidate genes. Hypertens. Res. 2017, 40, 876–884. [Google Scholar] [CrossRef]
- Sesso, H.D.; Stampfer, M.J.; Rosner, B.; Hennekens, C.H.; Gaziano, J.M.; Manson, J.E.; Glynn, R.J. Systolic and diastolic blood pressure, pulse pressure, and mean arterial pressure as predictors of cardiovascular disease risk in Men. Hypertension 2000, 36, 801–807. [Google Scholar] [CrossRef]
- Cogswell, M.E.; Wang, C.-Y.; Chen, T.-C.; Pfeiffer, C.M.; Elliott, P.; Gillespie, C.D.; Carriquiry, A.L.; Sempos, C.T.; Liu, K.; Perrine, C.G.; et al. Validity of predictive equations for 24-h urinary sodium excretion in adults aged 18-39 y. Am. J. Clin. Nutr. 2013, 98, 1502–1513. [Google Scholar] [CrossRef]
- Stolarz-Skrzypek, K.; Kuznetsova, T.; Thijs, L.; Tikhonoff, V.; Seidlerova, J.; Richart, T.; Jin, Y.; Olszanecka, A.; Malyutina, S.; Casiglia, E.; et al. Fatal and nonfatal outcomes, incidence of hypertension, and blood pressure changes in relation to urinary sodium excretion. JAMA 2011, 305, 1777–1785. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Liu, F.; Yang, X.; Cao, J.; Chen, S.; Chen, J.; Huang, K.; Shen, C.; Liu, X.; Yu, L.; et al. Validating World Health Organization cardiovascular disease risk charts and optimizing risk assessment in China. Lancet Reg. Health West. Pac. 2021, 8, 100096. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef]
- Preacher, K.J.; Rucker, D.D.; Hayes, A.F. Addressing Moderated Mediation Hypotheses: Theory, Methods, and Prescriptions. Multivar. Behav. Res. 2007, 42, 185–227. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Gu, D.; Huang, J.; Rao, D.C.; Jaquish, C.E.; Hixson, J.E.; Chen, C.S.; Chen, J.; Lu, F.; Hu, D.; et al. Metabolic syndrome and salt sensitivity of blood pressure in non-diabetic people in China: A dietary intervention study. Lancet 2009, 373, 829–835. [Google Scholar] [CrossRef]
- Weinberger, M.H.; Fineberg, N.S.; Fineberg, S.E.; Weinberger, M. Salt sensitivity, pulse pressure, and death in normal and hypertensive humans. Hypertension 2001, 37, 429–432. [Google Scholar] [CrossRef] [PubMed]
- de Boer, M.P.; Ijzerman, R.G.; de Jongh, R.T.; Eringa, E.C.; Stehouwer, C.D.; Smulders, Y.M.; Serne, E.H. Birth weight relates to salt sensitivity of blood pressure in healthy adults. Hypertension 2008, 51, 928–932. [Google Scholar] [CrossRef] [PubMed]
- Galletti, F.; Strazzullo, P.; Ferrara, I.; Annuzzi, G.; Rivellese, A.A.; Gatto, S.; Mancini, M. NaCl sensitivity of essential hypertensive patients is related to insulin resistance. J. Hypertens. 1997, 15, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Yatabe, M.S.; Yatabe, J.; Yoneda, M.; Watanabe, T.; Otsuki, M.; Felder, R.A.; Jose, P.A.; Sanada, H. Salt sensitivity is associated with insulin resistance, sympathetic overactivity, and decreased suppression of circulating renin activity in lean patients with essential hypertension. Am. J. Clin. Nutr. 2010, 92, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, A.; Weder, A.B. Nocturnal sodium excretion, blood pressure dipping, and sodium sensitivity. Hypertension 2006, 48, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Okayama, A.; Okuda, N.; Miura, K.; Okamura, T.; Hayakawa, T.; Akasaka, H.; Ohnishi, H.; Saitoh, S.; Arai, Y.; Kiyohara, Y.; et al. Dietary sodium-to-potassium ratio as a risk factor for stroke, cardiovascular disease and all-cause mortality in Japan: The NIPPON DATA80 cohort study. BMJ Open 2016, 6, e011632. [Google Scholar] [CrossRef]
- Mirmiran, P.; Bahadoran, Z.; Nazeri, P.; Azizi, F. Dietary sodium to potassium ratio and the incidence of hypertension and cardiovascular disease: A population-based longitudinal study. Clin. Exp. Hypertens. 2018, 40, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Okada, E.; Okada, C.; Matsumoto, M.; Fujiwara, A.; Takimoto, H. Dietary sodium:potassium ratio and CVD risk factors among Japanese adults: A retrospective cross-sectional study of pooled data from the National Health and Nutrition Survey, 2003-2017. Br. J. Nutr. 2021, 125, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ (Clin. Res. Ed.) 2013, 346, f1378. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.R. Biomarkers for prediction of cardiovascular events. JAMA 2009, 302, 2089. [Google Scholar] [CrossRef] [PubMed]
- Hunter, R.W.; Dhaun, N.; Bailey, M.A. The impact of excessive salt intake on human health. Nat. Rev. Nephrol. 2022, 18, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R. RAAS inhibition and mortality in hypertension. Glob. Cardiol. Sci. Pract. 2013, 2013, 269–278. [Google Scholar] [CrossRef]
- Wang, Y.-J.; Yeh, T.-L.; Shih, M.-C.; Tu, Y.-K.; Chien, K.-L. Dietary Sodium Intake and Risk of Cardiovascular Disease: A Systematic Review and Dose-Response Meta-Analysis. Nutrients 2020, 12, 2934. [Google Scholar] [CrossRef]
- Staruschenko, A. Beneficial Effects of High Potassium: Contribution of Renal Basolateral K Channels. Hypertension 2018, 71, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.M.; Kwock, C.K.; Park, S.; Eicher-Miller, H.A.; Yang, Y.J. An association of urinary sodium-potassium ratio with insulin resistance among Korean adults. Nutr. Res. Pract. 2018, 12, 443–448. [Google Scholar] [CrossRef]
- Du, S.; Batis, C.; Wang, H.; Zhang, B.; Zhang, J.; Popkin, B.M. Understanding the patterns and trends of sodium intake, potassium intake, and sodium to potassium ratio and their effect on hypertension in China. Am. J. Clin. Nutr. 2014, 99, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Sica, D.A.; Struthers, A.D.; Cushman, W.C.; Wood, M.; Banas, J.S.; Epstein, M. Importance of potassium in cardiovascular disease. J. Clin. Hypertens. (Greenwich) 2002, 4, 198–206. [Google Scholar] [CrossRef]
- Langford, H.G. Sodium-potassium interaction in hypertension and hypertensive cardiovascular disease. Hypertension 1991, 17, I155–I157. [Google Scholar] [CrossRef] [PubMed]
- Adrogue, H.J.; Madias, N.E. Sodium and potassium in the pathogenesis of hypertension: Focus on the brain. Curr. Opin. Nephrol. Hypertens. 2017, 26, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Fujita, T. Mechanism of salt-sensitive hypertension: Focus on adrenal and sympathetic nervous systems. J. Am. Soc. Nephrol. 2014, 25, 1148–1155. [Google Scholar] [CrossRef] [PubMed]
- Ralph, A.F.; Grenier, C.; Costello, H.M.; Stewart, K.; Ivy, J.R.; Dhaun, N.; Bailey, M.A. Activation of the Sympathetic Nervous System Promotes Blood Pressure Salt-Sensitivity in C57BL6/J Mice. Hypertension 2021, 77, 158–168. [Google Scholar] [CrossRef]
- Liu, K.; Liu, Z.; Qi, H.; Liu, B.; Wu, J.; Liu, Y.; Zhang, J.; Cao, H.; Yan, Y.; He, Y.; et al. Genetic Variation in SLC8A1 Gene Involved in Blood Pressure Responses to Acute Salt Loading. Am. J. Hypertens. 2018, 31, 415–421. [Google Scholar] [CrossRef]
- Cogswell, M.E.; Loria, C.M.; Terry, A.L.; Zhao, L.; Wang, C.-Y.; Chen, T.-C.; Wright, J.D.; Pfeiffer, C.M.; Merritt, R.; Moy, C.S.; et al. Estimated 24-Hour Urinary Sodium and Potassium Excretion in US Adults. JAMA 2018, 319, 1209–1220. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total (n = 2055) | Low-Moderate CVD Risk Group (n = 659) | High CVD Risk Group (n = 1396) | p Value |
|---|---|---|---|---|
| a Sex (male, %) | 555 (27.0) | 126 (19.1) | 429 (30.7) | <0.001 |
| b Age (years) | 59.00 (53.96, 63.29) | 53 (48, 58) | 61 (57, 65) | <0.001 |
| b BMI (kg/m−2) | 25.92 (23.84, 28.15) | 24.64 (22.66, 26.56) | 26.49 (24.59, 28.67) | <0.001 |
| b WHR | 0.89 (0.85, 0.93) | 0.86 (0.82, 0.90) | 0.90 (0.87, 0.94) | <0.001 |
| b FBG (mmol/L) | 5.42 (4.99, 6.18) | 5.18 (4.86, 5.66) | 5.59 (5.06, 6.49) | <0.001 |
| b TG (mmol/L) | 1.63 (1.12, 2.48) | 1.43 (0.99, 2.07) | 1.73 (1.20, 2.64) | <0.001 |
| b TC (mmol/L) | 5.04 (4.35, 5.73) | 5.03 (4.43, 5.69) | 5.05 (4.30, 5.76) | <0.001 |
| b HDL-C (mmol/L) | 1.44 (1.13, 2.40) | 1.63 (1.23, 2.73) | 1.38 (1.09, 2.14) | <0.001 |
| b LDL-C (mmol/L) | 2.14 (1.48, 2.86) | 2.02 (1.47, 2.75) | 2.19 (1.49, 2.93) | <0.001 |
| b 24hUNa (g/day) | 3.15 (2.07, 4.50) | 3.87 (2.46, 5.78) | 4.51 (3.07, 6.36) | <0.001 |
| b 24hUK (g/day) | 1.67 (1.14, 2.28) | 1.56 (1.08, 2.21) | 1.71 (1.18, 2.32) | 0.056 |
| b 24hUNa/K | 3.17 (2.22, 4.26) | 3.08 (2.05, 4.32) | 3.21 (2.31, 4.25) | 0.060 |
| b Response to acute salt loading, mm Hg | ||||
| MAP change 1 | 0.49 (−4.01, 4.99) | −0.01 (−4.92, 4.67) | 1.33 (−2.51, 5.66) | <0.001 |
| b Response to diuresis shrinkage, mm Hg | ||||
| MAP change 2 | 0.33 (−3.83, 4.83) | 0.17 (−4.33, 4.83) | 1.00 (−3.17, 4.67) | 0.398 |
| a Hypertension (n, %) | 1060 (51.6) | 132 (20.0) | 928 (66.5) | <0.001 |
| Baseline MAP, mm Hg | 92.17 (83.51, 101.01) | 83.09 (76.12, 90.51) | 95.84 (88.34, 103.84) | <0.001 |
| Antihypertensive medication use (yes) (%) | 829 (40.3) | 107 (16.2) | 722 (51.7) | <0.001 |
| a Diabetes (n, %) | 352 (17.1) | 24 (3.6) | 328 (23.5) | <0.001 |
| a Family history of hypertension | 1144 (57.8) | 350 (53.1) | 794 (62.1) | 0.010 |
| a Family history of coronary heart disease | 532 (25.9) | 179 (27.2) | 353 (25.3) | 0.532 |
| a Family history of stroke | 425 (21.5) | 137 (20.8) | 288 (20.6) | 0.871 |
| a Family history of diabetes | 527 (26.0) | 162 (26.0) | 365 (28.4) | 0.255 |
| Smoking (yes) (%) | 308 (15.2) | 80 (12.1) | 276 (19.8) | <0.001 |
| Drinking (yes) (%) | 962 (47.3) | 342 (51.9) | 620 (44.4) | 0.002 |
| SSBP | Univariate Logistic Regression | * Multivariate Logistic Regression | ||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Continuous | ||||
| MAP change 1, per SD | 1.12 (1.11, 1.13) | <0.001 | 1.03 (1.02, 1.05) | <0.001 |
| MAP change 2, per SD | 1.05 (0.94, 1.18) | 0.395 | 1.00 (0.99, 1.01) | 0.596 |
| Categories | ||||
| MAP change 1, mmHg | ||||
| quartile 1 (≤−4.29) | Reference | Reference | ||
| quartile 2 (−4.30 to 0.49) | 1.09 (0.80, 1.49) | 0.596 | 1.09 (0.79, 1.49) | 0.605 |
| quartile 3 (0.50 to 4.99) | 1.34 (0.97, 1.84) | 0.072 | 1.33 (0.97, 1.83) | 0.077 |
| quartile 4 (≥5.00) | 1.70 (1.23, 2.36) | 0.001 | 1.69 (1.22, 2.33) | 0.002 |
| p for trend | <0.001 | 0.001 | ||
| MAP change 2, mmHg | ||||
| quartile 1 (≤−3.83) | Reference | Reference | ||
| quartile 2 (−3.84 to 0.33) | 0.71 (0.53, 0.96) | 0.025 | 0.72 (0.54, 0.96) | 0.027 |
| quartile 3 (0.33 to 4.83) | 0.94 (0.70, 1.28) | 0.700 | 0.94 (0.70, 1.28) | 0.708 |
| quartile 4 (≥4.84) | 0.90 (0.66, 1.22) | 0.486 | 0.89 (0.66, 1.21) | 0.456 |
| p for trend | 0.915 | 0.908 | ||
| Univariate Logistic Regression | * Multivariate Logistic Regression | |||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Continuous | ||||
| 24hUNa, per SD (g/day) | 1.13 (1.08, 1.19) | <0.001 | 1.07 (1.01, 1.13) | <0.001 |
| 24hUK, per SD (g/day) | 1.10 (1.00, 1.21) | 0.054 | 1.09 (0.99, 1.20) | 0.076 |
| 24hUNa/K, per SD | 1.05 (1.01, 1.09) | 0.024 | 1.05 (1.01, 1.09) | 0.025 |
| Categories | ||||
| 24hUNa (g/day) | ||||
| quartile 1 | Reference | Reference | ||
| quartile 2 | 1.57 (1.20, 2.06) | 0.001 | 1.62 (1.25, 2.09) | <0.001 |
| quartile 3 | 1.54 (1.17, 2.03) | 0.002 | 1.67 (1.29, 2.16) | <0.001 |
| quartile 4 | 1.720 (1.29, 2.29) | <0.001 | 1.98 (1.52, 2.58) | <0.001 |
| p for trend | <0.001 | <0.001 | ||
| 24hUK (g/day) | ||||
| quartile 1 | Reference | Reference | ||
| quartile 2 | 1.23 (0.95, 1.59) | 0.115 | 1.20 (0.91, 1.58) | 0.204 |
| quartile 3 | 1.33 (1.02, 1.72) | 0.033 | 1.43 (1.08, 1.89) | 0.014 |
| quartile 4 | 1.44 (1.10, 1.87) | 0.007 | 1.46 (1.10, 1.94) | 0.009 |
| p for trend | 0.006 | 0.004 | ||
| 24hUNa/K | ||||
| quartile 1 | Reference | Reference | ||
| quartile 2 | 1.36 (1.05, 1.75) | 0.021 | 1.45 (1.09, 1.92) | 0.010 |
| quartile 3 | 1.54 (1.18, 2.00) | 0.001 | 1.48 (1.11, 1.96) | 0.007 |
| quartile 4 | 1.49 (1.15, 1.93) | 0.003 | 1.20 (0.91, 1.59) | 0.191 |
| p for trend | 0.002 | 0.194 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, Y.; Qi, H.; Peng, W.; Li, B.; Wen, F.; Zhang, F.; Zhang, L. Higher Potassium Intake and Lower Sodium Intake May Help in Reducing CVD Risk by Lowering Salt Sensitivity of Blood Pressure in the Han Chinese Population. Nutrients 2022, 14, 4436. https://doi.org/10.3390/nu14204436
Xie Y, Qi H, Peng W, Li B, Wen F, Zhang F, Zhang L. Higher Potassium Intake and Lower Sodium Intake May Help in Reducing CVD Risk by Lowering Salt Sensitivity of Blood Pressure in the Han Chinese Population. Nutrients. 2022; 14(20):4436. https://doi.org/10.3390/nu14204436
Chicago/Turabian StyleXie, Yunyi, Han Qi, Wenjuan Peng, Bingxiao Li, Fuyuan Wen, Fengxu Zhang, and Ling Zhang. 2022. "Higher Potassium Intake and Lower Sodium Intake May Help in Reducing CVD Risk by Lowering Salt Sensitivity of Blood Pressure in the Han Chinese Population" Nutrients 14, no. 20: 4436. https://doi.org/10.3390/nu14204436
APA StyleXie, Y., Qi, H., Peng, W., Li, B., Wen, F., Zhang, F., & Zhang, L. (2022). Higher Potassium Intake and Lower Sodium Intake May Help in Reducing CVD Risk by Lowering Salt Sensitivity of Blood Pressure in the Han Chinese Population. Nutrients, 14(20), 4436. https://doi.org/10.3390/nu14204436