
Exclusive Breastfeeding for at Least Four Months Is Associated with a Lower Prevalence of Overweight and Obesity in Mothers and Their Children after 2–5 Years from Delivery


 ,
, 
 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Design
3. Statistical Analysis
4. Results
4.1. Sociodemographic Characteristics and Anthropometric Measures of the Participant Mothers and Their Children
4.2. Exclusive Breastfeeding for at Least 4 Months and Its Association with Sociodemographic Characteristics of the Participant Mothers
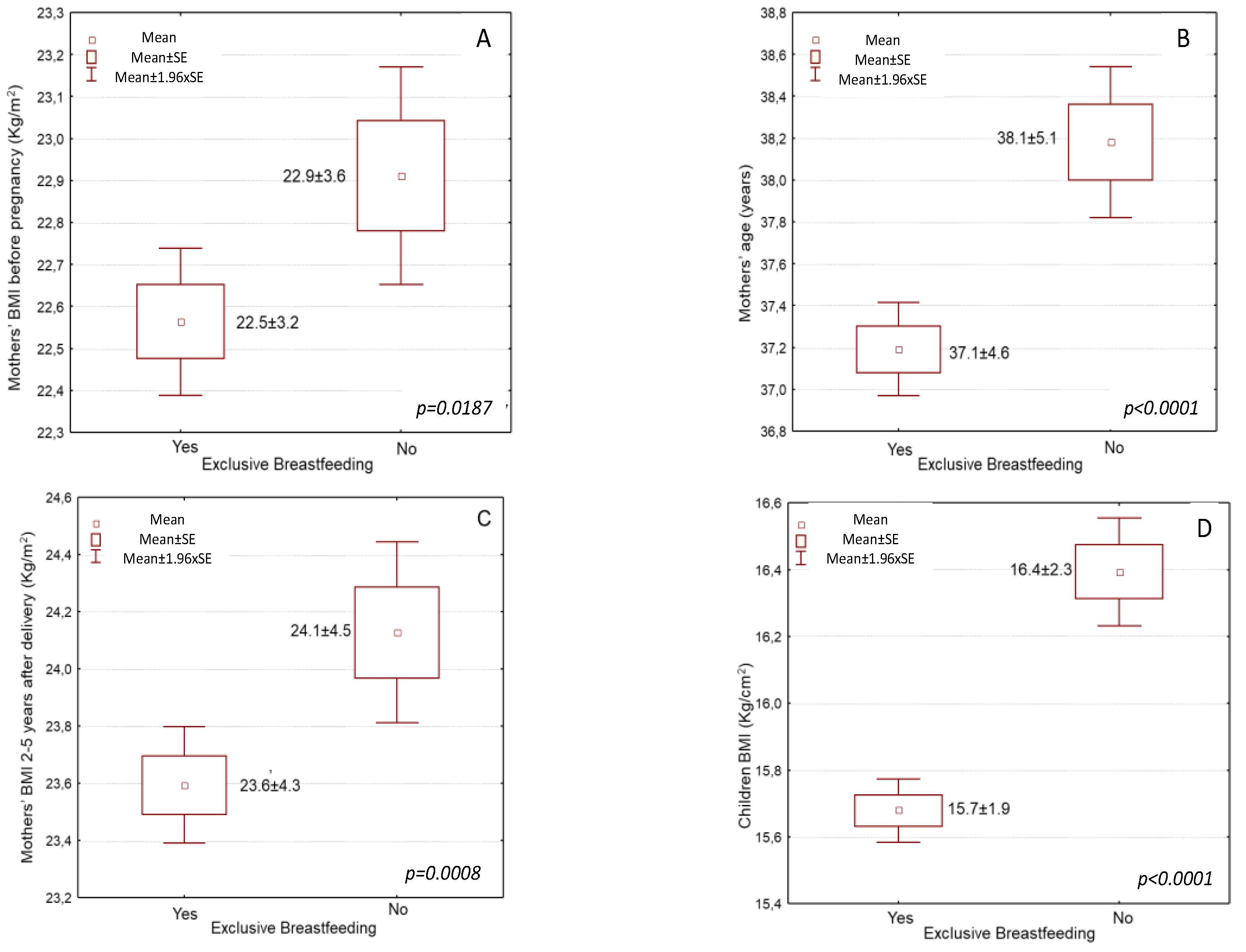
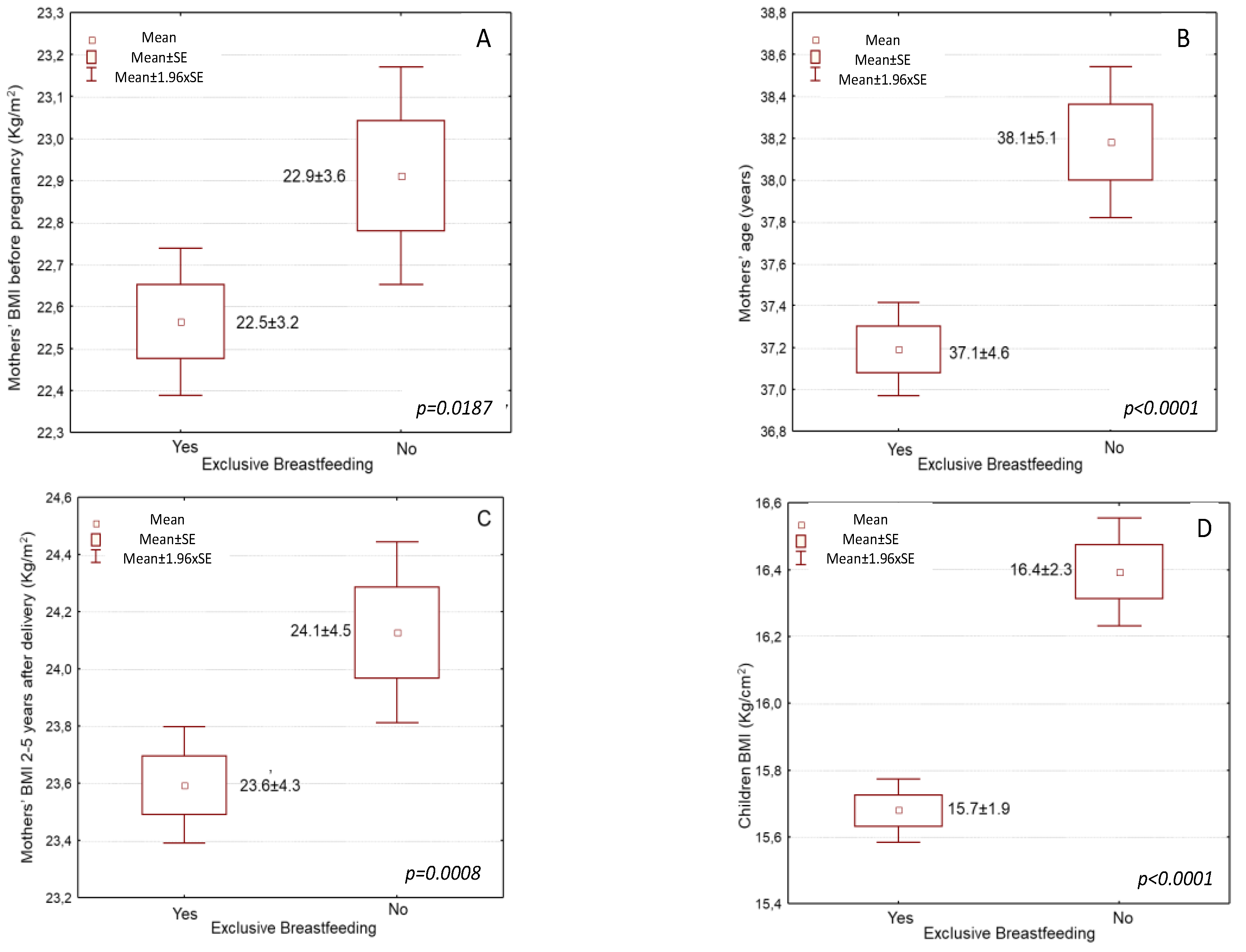
4.3. Exclusive Breastfeeding for at Least 4 Months and Its Association with Maternal and Childhood Anthropometric Measures
4.4. Multivariate Regression Analysis Assessing the Influence of Exclusive Breastfeeding on Maternal and Childhood Overweight and Obesity
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Avila, C.; Holloway, A.C.; Hahn, M.K.; Morrison, K.M.; Restivo, M.; Anglin, R.; Taylor, V.H. An Overview of Links between Obesity and Mental Health. Curr. Obes. Rep. 2015, 4, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Svard, A.; Lahti, J.; Roos, E.; Rahkonen, O.; Lahelma, E.; Lallukka, T.; Manty, M. Obesity, change of body mass index and subsequent physical and mental health functioning: A 12-year follow-up study among ageing employees. BMC Public Health 2017, 17, 744. [Google Scholar] [CrossRef]
- Trasande, L.; Elbel, B. The economic burden placed on healthcare systems by childhood obesity. Expert Rev. Pharm. Outcomes Res. 2012, 12, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Bomberg, E.; Birch, L.; Endenburg, N.; German, A.J.; Neilson, J.; Seligman, H.; Takashima, G.; Day, M.J. The Financial Costs, Behaviour and Psychology of Obesity: A One Health Analysis. J. Comp. Pathol. 2017, 156, 310–325. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.B.; Smith, M.S. Obesity Statistics. Prim. Care Clin. Off. Pract. 2016, 43, 121–135. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 June 2022).
- World Health Organization. Obesity—Data and Statistics. Available online: http://www.euro.who.int/en/he (accessed on 4 April 2019).
- Choquet, H.; Meyre, D. Molecular basis of obesity: Current status and future prospects. Curr. Genom. 2011, 12, 154–168. [Google Scholar] [CrossRef]
- Lipek, T.; Igel, U.; Gausche, R.; Kiess, W.; Grande, G. Obesogenic environments: Environmental approaches to obesity prevention. J. Pediatric Endocrinol. Metab. JPEM 2015, 28, 485–495. [Google Scholar] [CrossRef]
- Llewellyn, C.; Wardle, J. Behavioral susceptibility to obesity: Gene-environment interplay in the development of weight. Physiol. Behav. 2015, 152, 494–501. [Google Scholar] [CrossRef]
- Albuquerque, D.; Nobrega, C.; Manco, L.; Padez, C. The contribution of genetics and environment to obesity. Br. Med. Bull. 2017, 123, 159–173. [Google Scholar] [CrossRef]
- Bahreynian, M.; Qorbani, M.; Khaniabadi, B.M.; Motlagh, M.E.; Safari, O.; Asayesh, H.; Kelishadi, R. Association between Obesity and Parental Weight Status in Children and Adolescents. J. Clin. Res. Pediatric Endocrinol. 2017, 9, 111–117. [Google Scholar] [CrossRef]
- Huvenne, H.; Dubern, B.; Clement, K.; Poitou, C. Rare Genetic Forms of Obesity: Clinical Approach and Current Treatments in 2016. Obes. Facts 2016, 9, 158–173. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, M.O. Genetics of obesity: What genetic association studies have taught us about the biology of obesity and its complications. Lancet. Diabetes Endocrinol. 2018, 6, 223–236. [Google Scholar] [CrossRef]
- Dolton, P.; Xiao, M. The intergenerational transmission of body mass index across countries. Econ. Hum. Biol. 2017, 24, 140–152. [Google Scholar] [CrossRef] [PubMed]
- McAllister, E.J.; Dhurandhar, N.V.; Keith, S.W.; Aronne, L.J.; Barger, J.; Baskin, M.; Benca, R.M.; Biggio, J.; Boggiano, M.M.; Eisenmann, J.C.; et al. Ten putative contributors to the obesity epidemic. Crit. Rev. Food Sci. Nutr. 2009, 49, 868–913. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.L. A Review of the Prevention and Medical Management of Childhood Obesity. Child Adolesc. Psychiatr. Clin. N. Am. 2018, 27, 63–76. [Google Scholar] [CrossRef]
- Gray, L.A.; Hernandez Alava, M.; Kelly, M.P.; Campbell, M.J. Family lifestyle dynamics and childhood obesity: Evidence from the millennium cohort study. BMC Public Health 2018, 18, 500. [Google Scholar] [CrossRef]
- Leonard, S.A.; Rasmussen, K.M.; King, J.C.; Abrams, B. Trajectories of maternal weight from before pregnancy through postpartum and associations with childhood obesity. Am. J. Clin. Nutr. 2017, 106, 1295–1301. [Google Scholar] [CrossRef]
- World Health Organization. Breastfeeding. Available online: https://www.who.int/topics/breastfeeding/en/ (accessed on 10 June 2022).
- Victora, C.G.; Bahl, R.; Barros, A.J.; Franca, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- da Silva Mda, C.; Oliveira Assis, A.M.; Pinheiro, S.M.; de Oliveira, L.P.; da Cruz, T.R. Breastfeeding and maternal weight changes during 24 months post-partum: A cohort study. Matern. Child Nutr. 2015, 11, 780–791. [Google Scholar] [CrossRef]
- Arenz, S.; Ruckerl, R.; Koletzko, B.; von Kries, R. Breast-feeding and childhood obesity--a systematic review. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2004, 28, 1247–1256. [Google Scholar] [CrossRef] [Green Version]
- Yan, J.; Liu, L.; Zhu, Y.; Huang, G.; Wang, P.P. The association between breastfeeding and childhood obesity: A meta-analysis. BMC Public Health 2014, 14, 1267. [Google Scholar] [CrossRef] [PubMed]
- Harder, T.; Bergmann, R.; Kallischnigg, G.; Plagemann, A. Duration of breastfeeding and risk of overweight: A meta-analysis. Am. J. Epidemiol. 2005, 162, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Amir, L.H.; Donath, S. A systematic review of maternal obesity and breastfeeding intention, initiation and duration. BMC Pregnancy Childbirth 2007, 7, 9. [Google Scholar] [CrossRef]
- Ramji, N.; Challa, S.; Murphy, P.A.; Quinlan, J.; Crane, J.M.G. A comparison of breastfeeding rates by obesity class. J. Matern. Fetal Neonatal Med. 2018, 31, 3021–3026. [Google Scholar] [CrossRef] [PubMed]
- Bobrow, K.L.; Quigley, M.A.; Green, J.; Reeves, G.K.; Beral, V. Persistent effects of women’s parity and breastfeeding patterns on their body mass index: Results from the Million Women Study. Int. J. Obes. 2013, 37, 712–717. [Google Scholar] [CrossRef]
- Wiklund, P.; Xu, L.; Lyytikäinen, A.; Saltevo, J.; Wang, Q.; Völgyi, E.; Munukka, E.; Cheng, S.; Alen, M.; Keinänen-Kiukaanniemi, S.; et al. Prolonged breastfeeding protects mothers from later-life obesity and related cardio-metabolic disorders. Public Health Nutr. 2012, 15, 67–74. [Google Scholar] [CrossRef]
- Kirkegaard, H.; Stovring, H.; Rasmussen, K.M.; Abrams, B.; Sørensen, T.I.A.; Nohr, E.A. How do pregnancy-related weight changes and breastfeeding relate to maternal weight and BMI-adjusted waist circumference 7 y after delivery? Results from a path analysis. Am. J. Clin. Nutr. 2014, 99, 312–319. [Google Scholar] [CrossRef]
- Natland, S.T.; Nilsen, T.I.; Midthjell, K.; Andersen, L.F.; Forsmo, S. Lactation and cardiovascular risk factors in mothers in a population-based study: The HUNT-study. Int. Breastfeed. J. 2012, 7, 8. [Google Scholar] [CrossRef]
- Cieśla, E.; Stochmal, E.; Głuszek, S.; Suliga, E. Breastfeeding history and the risk of overweight and obesity in middle-aged women. BMC Womens Health 2021, 21, 196. [Google Scholar]
- Sharma, A.J.; Dee, D.L.; Harden, S.M. Adherence to breast-feeding guidelines and maternal weight 6 years after de-livery. Pediatrics 2014, 134 (Suppl. S1), S42–S49. [Google Scholar] [CrossRef]
- Oken, E.; Patel, R.; Guthrie, L.B.; Vilchuck, K.; Bogdanovich, N.; Sergeichick, N.; Palmer, T.M.; Kramer, M.S.; Martin, R.M. Effects of an intervention to promote breastfeeding on maternal adiposity and blood pressure at 11.5 y postpartum: Results from the Promotion of Breastfeeding Intervention Trial, a cluster-randomized controlled trial. Am. J. Clin. Nutr. 2013, 98, 1048–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, E.B.; Ray, R.M.; Stuebe, A.M.; Allison, M.A.; Ness, R.B.; Freiberg, M.S.; Cauley, J.A. Duration of lactation and risk factors for maternal cardiovascular disease. Obstet Gynecol. 2009, 113, 974–982. [Google Scholar] [CrossRef] [PubMed]
- Fallahzadeh, H.; Golestan, M.; Rezvanian, T.; Ghasemian, Z. Breast-feeding history and overweight in 11 to 13-year-old children in Iran. World J. Pediatric 2009, 5, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Oddy, W.H.; Mori, T.A.; Huang, R.C.; Marsh, J.A.; Pennell, C.E.; Chivers, P.T.; Hands, B.P.; Jacoby, P.; Rzehak, P.; Koletzko, B.V.; et al. Early infant feeding and adiposity risk: From infancy to adulthood. Ann. Nutr. Metab. 2014, 64, 262–270. [Google Scholar] [CrossRef]
- Morovic, M.L.; Music Milanovic, S. Breastfeeding Duration as a Predictor of Childhood Lifestyle Habits, Overweight and Obesity in Second- and Third-Grade Schoolchildren in Croatia. Acta Clin. Croat. 2019, 58, 481–490. [Google Scholar]
- Huus, K.; Ludvigsson, J.F.; Enskär, K.; Ludvigsson, J. Exclusive breastfeeding of Swedish children and its possible influence on the development of obesity: A prospective cohort study. BMC Pediatric 2008, 8, 42. [Google Scholar] [CrossRef]
- Durmuş, B.; van Rossem, L.; Duijts, L.; Arends, L.R.; Raat, H.; Moll, H.A.; Hofman, A.; Steegers, E.A.; Jaddoe, V.W. Breast-feeding and growth in children until the age of 3 years: The Generation R Study. Br. J. Nutr. 2011, 105, 1704–1711. [Google Scholar] [CrossRef]
- Vickerstaff, V.; Omar, R.Z.; Ambler, G. Methods to adjust for multiple comparisons in the analysis and sample size calculation of randomised controlled trials with multiple primary outcomes. BMC Med. Res. Methodol. 2019, 19, 129. [Google Scholar]
- World Health Organization. Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ. Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- Food and Drug Administration. National Health and Nutrition Examination Survey (NHANES) Anthropometry Procedures Manual. Food and Drug Administration: Rockville, MD, USA, 2007. [Google Scholar]
- World Health Organization. Country Profiles on Nutrition, Physical Activity and Obesity in the 53 WHO European Region Member States: Methodology and Summary. Available online: http://www.euro.who.int/__data/assets/pdf_f (accessed on 4 April 2019).
- Koukoulis, G.N.; Sakka, C.; Katsaros, F.; Goutou, M.; Tsirona, S.; Tsiapali, E.; Piterou, A.; Stefanidis, I.; Stathakis, N. High rates of obesity prevalence in adults living in central Greece: Data from the ARGOS study. Hormones 2010, 9, 253–262. [Google Scholar] [CrossRef]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Current data in Greek children indicate decreasing trends of obesity in the transition from childhood to adolescence; results from the National Action for Children’s Health (EYZHN) program. J. Prev. Med. Hyg. 2018, 59, E36–E47. [Google Scholar] [CrossRef]
- Theurich, M.A.; Davanzo, R.; Busck-Rasmussen, M.; Diaz-Gomez, N.M.; Brennan, C.; Kylberg, E.; Baerug, A.; McHugh, L.; Weikert, C.; Abraham, K.; et al. Breastfeeding Rates and Programs in Europe: A Survey of 11 National Breastfeeding Committees and Representatives. J. Pediatric Gastroenterol. Nutr. 2019, 68, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Olmedo, N.; Hernandez-Cordero, S.; Neufeld, L.M.; Garcia-Guerra, A.; Mejia-Rodriguez, F.; Mendez Gomez-Humaran, I. The Associations of Maternal Weight Change with Breastfeeding, Diet and Physical Activity During the Postpartum Period. Matern. Child Health J. 2016, 20, 270–280. [Google Scholar] [CrossRef]
- Schalla, S.C.; Witcomb, G.L.; Haycraft, E. Body Shape and Weight Loss as Motivators for Breastfeeding Initiation and Continuation. Int. J. Environ. Res. Public Health 2017, 14, 754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojcicki, J.M. Maternal prepregnancy body mass index and initiation and duration of breastfeeding: A review of the literature. J. Womens Health 2011, 20, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Zielinska, M.A.; Hamulka, J. Reasons for non-exclusive breast-feeding in the first 6 months. Pediatrics Int. Off. J. Jpn. Pediatric Soc. 2018, 60, 276–281. [Google Scholar] [CrossRef]
- Ardid, C.; Usta, O.; Omar, E.; Yildiz, C.; Memis, E. Effects of infant feeding practices and maternal characteristics on early childhood obesity. Arch. Argent. De Pediatric. 2019, 117, 26–33. [Google Scholar] [CrossRef]
- Rito, A.I.; Buoncristiano, M.; Spinelli, A.; Salanave, B.; Kunesova, M.; Hejgaard, T.; Garcia Solano, M.; Fijalkowska, A.; Sturua, L.; Hyska, J.; et al. Association between Characteristics at Birth, Breastfeeding and Obesity in 22 Countries: The WHO European Childhood Obesity Surveillance Initiative—COSI 2015/2017. Obes. Facts 2019, 12, 226–243. [Google Scholar] [CrossRef]
- Wang, L.; Collins, C.; Ratliff, M.; Xie, B.; Wang, Y. Breastfeeding Reduces Childhood Obesity Risks. Child. Obes. 2017, 13, 197–204. [Google Scholar] [CrossRef]
- Lee, J.W.; Lee, M.; Lee, J.; Kim, Y.J.; Ha, E.; Kim, H.S. The Protective Effect of Exclusive Breastfeeding on Overweight/Obesity in Children with High Birth Weight. J. Korean Med. Sci. 2019, 34, e85. [Google Scholar] [CrossRef]
- Yeung, H.; Leff, M.; Rhee, K.E. Effect of Exclusive Breastfeeding among Overweight and Obese Mothers on Infant Weight-for-Length Percentile at 1 Year. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2017, 12, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Tambalis, K.D.; Mourtakos, S.; Panagiotakos, D.B.; Sidossis, L.S. Association of Exclusive Breastfeeding with Risk of Obesity in Childhood and Early Adulthood. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2018, 13, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Qiao, J.; Dai, L.J.; Zhang, Q.; Ouyang, Y.Q. A Meta-Analysis of the Association between Breastfeeding and Early Childhood Obesity. J. Pediatric Nurs. 2020, 53, 57–66. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Sociodemographic and Anthropometric Characteristics | Exclusive Breastfeeding | ||
|---|---|---|---|
| No | Yes | p-Value | |
| Mothers’ age (years) | 38.1 ± 5.1 | 37.1 ± 4.6 | p < 0.0001 |
| Mothers’ nationality (% Greek) | 48.7 | 47.1 | p = 0.0001 |
| Mothers’ BMI (kg/m2) | 24.1 ± 4.5 | 23.6 ± 4.3 | p = 0.0008 |
| Mothers’ BMI (% overweight or obese) | 35.2 | 33.1 | p < 0.0001 |
| Mothers’ education (years) | 14.7 ± 2.3 | 15.3 ± 2.1 | p < 0.0001 |
| Mothers’ economic status (scale 0–5) | 3.58 ± 0.9 | 3.64 ± 1.1 | p = 0.0322 |
| Mothers’ smoking habits (% smokers) | 51.30 | 48.70 | p = 0.0195 |
| Children age (years) | 4.07 ± 1.06 | 4.03 ± 1.04 | p = 0.2613 |
| Children gender (%male) | 49.8 | 49.9 | p = 0.5347 |
| Children BMI (kg/m2) | 16.4 ± 2.3 | 15.7 ± 1.9 | p < 0.0001 |
| Children BMI (% overweight or obese) | 30.9 | 27.2 | p < 0.0001 |
| Sociodemographic and Anthropometric Characteristics | Exclusive Breastfeeding | |
|---|---|---|
| HR * (95% CI **) | p-Value | |
| Age (below/over mean value) | 1.52 (0.881–2.319) | p = 0.0023 |
| Nationality (Greek/other nationality) | 0.88 (0.262–1.632) | p = 0.0537 |
| BMI (normal/overweight or obese) | 2.14 (1.871–2.427) | p < 0.0001 |
| Education (below/over mean value) | 1.77 (0.944–2.558) | p = 0.0045 |
| Economic status (below/over mean value) | 1.64 (0.375–2.983) | p = 0.3781 |
| Smoking habits (No/Yes) | 2.87 (1.591–3.294) | p = 0.1941 |
| Sociodemographic and Anthropometric Characteristics | Exclusive Breastfeeding | |
|---|---|---|
| HR * (95% CI **) | p-Value | |
| Mothers’ age (below/over mean value) | 1.61 (0.74–2.419) | p = 0.0082 |
| Children gender (male/female) | 1.08 (0.125–2.376) | p = 0.4891 |
| Mothers’ nationality (Greek/other nationality) | 0.72 (0.102–2.391) | p = 0.1349 |
| Children BMI (normal/overweight or obese) | 2.07 (1.704–2.398) | p < 0.0001 |
| Mothers’ education (below/over mean value) | 1.83 (0.827–2.901) | p = 0.0321 |
| Mothers’ economic status (below/over mean value) | 1.42 (0.176–3.479) | p = 0.6287 |
| Mothers’ smoking habits (No/Yes) | 2.54 (0.876–4.176) | p = 0.5279 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantzorou, M.; Papandreou, D.; Vasios, G.K.; Pavlidou, E.; Antasouras, G.; Psara, E.; Taha, Z.; Poulios, E.; Giaginis, C. Exclusive Breastfeeding for at Least Four Months Is Associated with a Lower Prevalence of Overweight and Obesity in Mothers and Their Children after 2–5 Years from Delivery. Nutrients 2022, 14, 3599. https://doi.org/10.3390/nu14173599
Mantzorou M, Papandreou D, Vasios GK, Pavlidou E, Antasouras G, Psara E, Taha Z, Poulios E, Giaginis C. Exclusive Breastfeeding for at Least Four Months Is Associated with a Lower Prevalence of Overweight and Obesity in Mothers and Their Children after 2–5 Years from Delivery. Nutrients. 2022; 14(17):3599. https://doi.org/10.3390/nu14173599
Chicago/Turabian StyleMantzorou, Maria, Dimitrios Papandreou, Georgios K. Vasios, Eleni Pavlidou, Georgios Antasouras, Evmorfia Psara, Zainab Taha, Efthymios Poulios, and Constantinos Giaginis. 2022. "Exclusive Breastfeeding for at Least Four Months Is Associated with a Lower Prevalence of Overweight and Obesity in Mothers and Their Children after 2–5 Years from Delivery" Nutrients 14, no. 17: 3599. https://doi.org/10.3390/nu14173599
APA StyleMantzorou, M., Papandreou, D., Vasios, G. K., Pavlidou, E., Antasouras, G., Psara, E., Taha, Z., Poulios, E., & Giaginis, C. (2022). Exclusive Breastfeeding for at Least Four Months Is Associated with a Lower Prevalence of Overweight and Obesity in Mothers and Their Children after 2–5 Years from Delivery. Nutrients, 14(17), 3599. https://doi.org/10.3390/nu14173599