
Incidence, Risk Factors and Prediction of Secondary Hyperparathyroidism in Preterm Neonates under 32 Weeks’ Gestational Age

 ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schulz, E.V.; Wagner, C.L. History, epidemiology and prevalence of neonatal bone mineral metabolic disorders. Semin. Fetal Neonatal Med. 2020, 25, 101069. [Google Scholar] [CrossRef] [PubMed]
- Rustico, S.E.; Calabria, A.C.; Garber, S.J. Metabolic bone disease of prematurity. J. Clin. Transl. Endocrinol. 2014, 1, 85–91. [Google Scholar] [CrossRef][Green Version]
- Montaner Ramón, A. Risk factors of bone mineral metabolic disorders. Semin. Fetal Neonatal Med. 2020, 25, 101068. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.M.; Johnson, K.; McKechnie, E. Osteopenia of prematurity: A national survey and review of practice. Acta Paediatr. Int. J. Paediatr. 2008, 97, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Backström, M.C.; Kouri, T.; Kuusela, A.L.; Sievänen, H.; Koivisto, A.M.; Ikonen, R.S.; Mäki, M. Bone isoenzyme of serum alkaline phosphatase and serum inorganic phosphate in metabolic bone disease of prematurity. Acta Paediatr. Int. J. Paediatr. 2000, 89, 867–873. [Google Scholar] [CrossRef]
- Avila-Alvarez, A.; Urisarri, A.; Fuentes-Carballal, J.; Mandiá, N.; Sucasas-Alonso, A.; Couce, M.L. Metabolic Bone Disease of Prematurity: Risk Factors and Associated Short-Term Outcomes. Nutrients 2020, 12, 3786. [Google Scholar] [CrossRef]
- Chinoy, A.; Mughal, M.Z.; Padidela, R. Metabolic bone disease of prematurity: Causes, recognition, prevention, treatment and long-term consequences. Arch. Dis. Child. Fetal Neonatal Ed. 2019, 104, F560–F566. [Google Scholar] [CrossRef]
- Moreira, A.; Swischuk, L.; Malloy, M.; Mudd, D.; Blanco, C.; Geary, C. Parathyroid hormone as a marker for metabolic bone disease of prematurity. J. Perinatol. 2014, 34, 787–791. [Google Scholar] [CrossRef]
- Matejek, T.; Navratilova, M.; Zaloudkova, L.; Malakova, J.; Maly, J.; Skalova, S.; Palicka, V. Parathyroid hormone–reference values and association with other bone metabolism markers in very low birth weight infants–pilot study. J. Matern. Neonatal Med. 2019, 32, 2860–2867. [Google Scholar] [CrossRef]
- Faienza, M.F.; D’Amato, E.; Natale, M.P.; Grano, M.; Chiarito, M.; Brunetti, G.; D’Amato, G. Metabolic bone disease of prematurity: Diagnosis and management. Front. Pediatr. 2019, 7, 143. [Google Scholar] [CrossRef]
- Tong, L.; Gopal-Kothandapani, J.S.; Offiah, A.C. Feasibility of quantitative ultrasonography for the detection of metabolic bone disease in preterm infants—Systematic review. Pediatr. Radiol. 2018, 48, 1537–1549. [Google Scholar] [CrossRef] [PubMed]
- Higgins, R.D.; Jobe, A.H.; Koso-Thomas, M.; Bancalari, E.; Viscardi, R.M.; Hartert, T.V.; Ryan, R.M.; Kallapur, S.G.; Steinhorn, R.H.; Konduri, G.G.; et al. Bronchopulmonary Dysplasia: Executive Summary of a Workshop. J. Pediatr. 2018, 197, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Gregory, K.E.; Deforge, C.E.; Natale, K.M.; Phillips, M.; Van Marter, L.J. Necrotizing enterocolitis in the premature infant: Neonatal nursing assessment, disease pathogenesis, and clinical presentation. Adv. Neonatal Care 2011, 11, 155–164; quiz 165–166. [Google Scholar] [CrossRef]
- Tarby, T.J.; Volpe, J.J. Intraventricular Hemorrhage in the Premature Infant. Pediatr. Clin. N. Am. 1982, 29, 1077–1104. [Google Scholar] [CrossRef]
- International Committee for the Classification of Retinopathy of Prematurity. The International Classification of Retinopathy of Prematurity Revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef]
- Sethi, A.; Priyadarshi, M.; Agarwal, R. Mineral and bone physiology in the foetus, preterm and full-term neonates. Semin. Fetal Neonatal Med. 2020, 25, 101076. [Google Scholar] [CrossRef]
- Kelly, A.; Kovatch, K.J.; Garber, S.J. Metabolic bone disease screening practices among U.S. Neonatologists. Clin. Pediatr. 2014, 53, 1077–1083. [Google Scholar] [CrossRef]
- Moreira, A.; February, M.; Geary, C. Parathyroid hormone levels in neonates with suspected osteopenia. J. Paediatr. Child Health 2013, 49, E12–E16. [Google Scholar] [CrossRef]
- Dowa, Y.; Kawai, M.; Kanazawa, H.; Iwanaga, K.; Matsukura, T.; Heike, T. Screening for secondary hyperparathyroidism in preterm infants. Pediatr. Int. 2016, 58, 988–992. [Google Scholar] [CrossRef]
- Villeneuve, A.; Arsenault, V.; Lacroix, J.; Tucci, M. Neonatal red blood cell transfusion. Vox Sang. 2021, 116, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Allali, S.; Brousse, V.; Sacri, A.-S.; Chalumeau, M.; de Montalembert, M. Anemia in children: Prevalence, causes, diagnostic work-up, and long-term consequences. Expert Rev. Hematol. 2017, 10, 1023–1028. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Perinatal Characteristics | |
| ± SD | |
| Gestational age | 29.70 ± 2.07 |
| Maternal age | 33.47 ± 6.33 |
| Maternal BMI | 25.83 ± 6.14 |
| Apgar minute 1 | 6.47 ± 1.75 |
| Apgar minute 5 | 7.89 ± 1.48 |
| Birth weight (g) | 1165.62 ± 259.72 |
| Birth weight (z-score) | −0.49 ± 0.76 |
| No. (%) | |
| Maternal diabetes | 9 (5.9) |
| Maternal smoking | 18 (11.9) |
| Maternal arterial hypertension | 34 (22.1) |
| Multiple gestation | 58 (37.7) |
| IVF | 37 (24) |
| Female | 81 (52.6) |
| Antenatal corticosteroids | 150 (97.4) |
| Chorioamnionitis | 21 (13.6) |
| Caesarean section | 113 (7.4) |
| Small for gestational age | 29 (18.8) |
| Ethnicity = caucasian | 138 (89.6) |
| Neonatal evolution | |
| ± SD | |
| IMV duration (h) | 166.80 ± 219.02 |
| Duration of NIMV (h) | 198.39 ± 191.61 |
| Duration of oxygen therapy (h) | 599.62 ± 655.27 |
| Duration of parenteral nutrition (days) | 12.32 ± 7.42 |
| NICU stay (days) | 24.71 ± 18.24 |
| Weight at discharge (n = 153) | 2349.55 ± 379.77 |
| Weight at discharge z-score (n = 153) | −1.45 ± 1.17 |
| No. (%) | |
| MBD | 22 (14.3) |
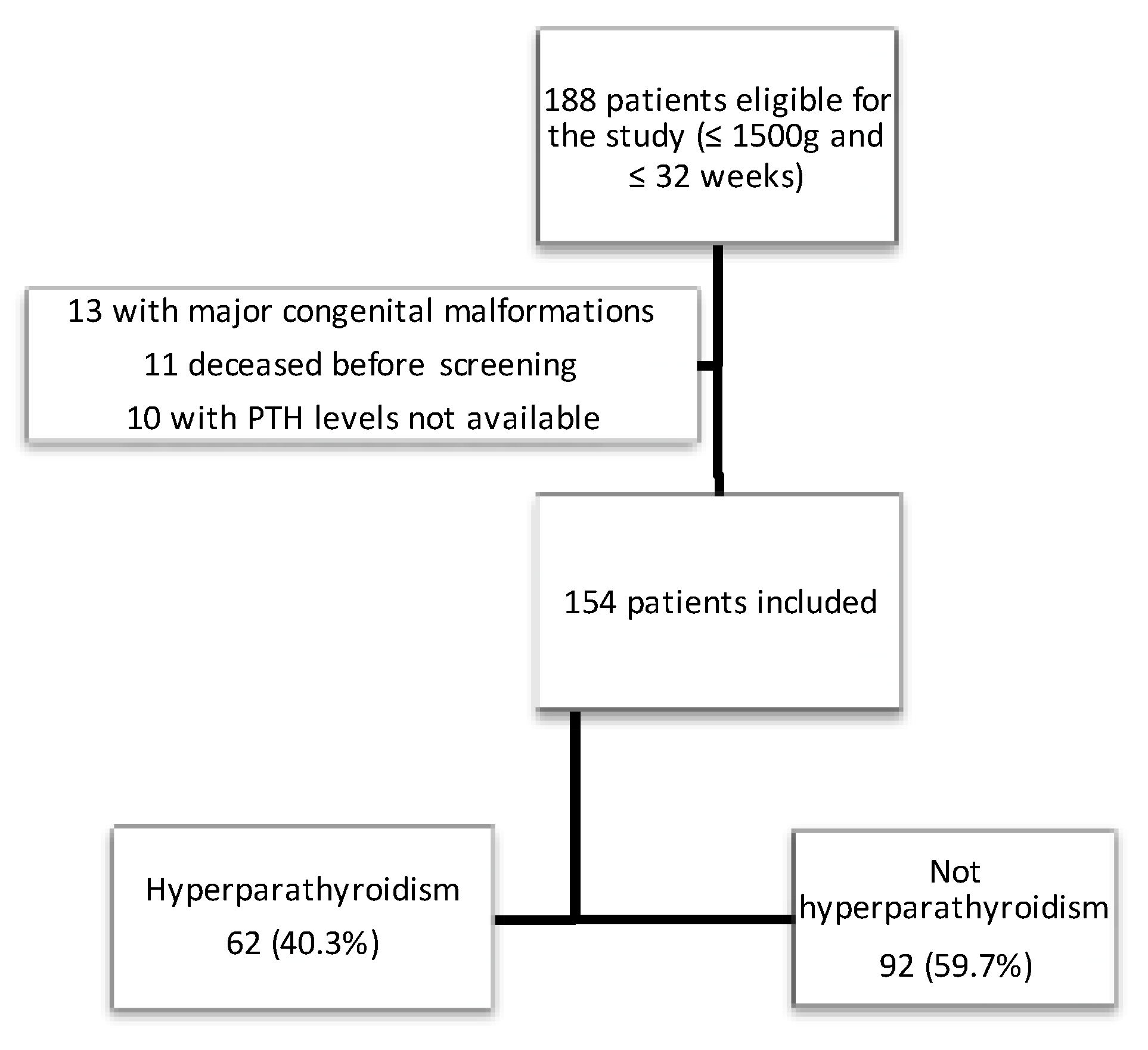
| HPTH | 62 (40.3) |
| Severe hyperparathyroidism | 14 (9.1) |
| Surfactant | 70 (45.5) |
| NIMV during admission | 79 (51.3) |
| IMV during admission | 55 (35.7) |
| Bronchopulmonary dysplasia | 40 (26) |
| Home oxygen | 7 (4.5) |
| Survival without BPD | 112 (72.7) |
| Caffeine | 148 (96.1) |
| Steroids for BPD | 18 (11.7) |
| Furosemide | 6 (3.9) |
| Breastfeeding | 134 (87) |
| Fortification of breastfeeding | 124 (80.5) |
| Death | 2 (1.3) |
| PDA | 25 (16.2) |
| NEC | 8 (5.2) |
| ROP grade ≥ II | 7 (5) |
| Nosocomial sepsis | 57 (37) |
| IVH grade ≥ II | 6 (3.9) |
| PVL | 5 (3.2) |
| Blood transfusion | 126 (88.1) |
| ± SD | ||
|---|---|---|
| Age at screening (days) | 15.68 ± 2.10 | |
| Serum creatinine (mg/dL) | 0.48 ± 0.20 | |
| Phosphorus in blood (mg/dL) | 6.01 ± 1.18 | |
| Calcium in blood (mg/dL) | 9.78 ± 0.58 | |
| Blood magnesium (mg/dL) (n = 127) | 2.05 ± 0.21 | |
| ALP in blood (IU/L) | 846.15 ± 351.91 | |
| PTH (pg/mL) | 88.29 ± 72.44 | |
| Vitamin D (ng/mL) (n = 141) | 34.60 ± 11.93 | |
| Phosphorus in urine (mg/dL) n = 76 | 11.86 ± 13.39 | |
| Calcium in urine (mg/dL) n = 76 | 7.46 ± 5.91 | |
| Creatinine in urine (mg/dL) n = 77 | 11.50 ± 9.22 | |
| Ca/Cr ratio in urine n = 76 | 0.92 ± 1.50 | |
| P/Cr ratio in urine n = 76 | 1.26 ± 1.54 | |
| P/Ca ratio in urine (mg/mg) n = 75 | 2.46 ± 4.06 | |
| Tubular phosphate reabsorption (%) n = 74 | 90.77 ± 12.22 | |
| OR (95% CI) | OR Adjusted by GA (95%) | |
|---|---|---|
| Perinatal variables | ||
| Maternal body mass index | 1.07 (1.01–1.14) | 1.05 (0.99–1.12) |
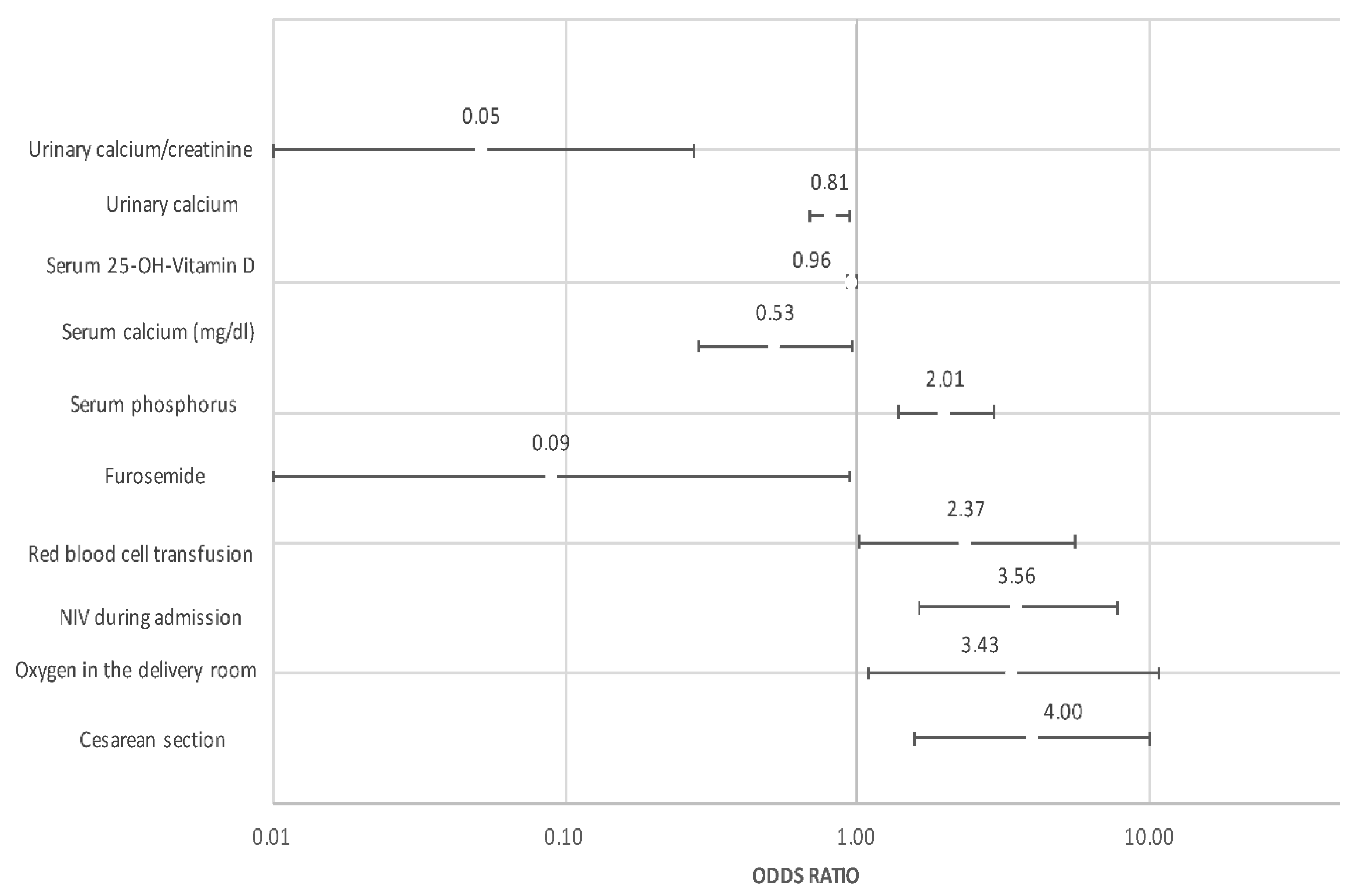
| Cesarean section | 2.24 (1.02–4.91) | 4.00 (1.59–10.06) |
| Oxygen in resuscitation | 4.56 (1.49–13.98) | 3.43 (1.09–10.81) |
| Intubation in resuscitation | 2.94 (1.20–7.24) | 2.18 (0.85–5.59) |
| Neonatal Evolution | ||
| Oxygen | 2.47 (1.13–5.39) | 1.61 (0.69–3.78) |
| NIMV | 3.12 (1.59–6.14) | 2.08 (0.93–4.68) |
| Invasive mechanical ventilation | 4.67 (2.31–9.45) | 3.56 (1.63–7.77) |
| Surfactant | 2.97 (1.52–5.79) | 2.08 (0.99–4.37) |
| Patent ductus arteriosus | 2.62 (1.09–6.29) | 1.45 (0.54–3.92) |
| Necrotizing enterocolitis | 4.82 (0.94–24.72) | 3.29 (0.61–17.76) |
| Anemia requiring transfusion | 3.50 (1.65–7.42) | 2.37 (1.01–5.57) |
| Nosocomial sepsis | 2.54 (1.29–4.98) | 1.91 (0.93–3.90) |
| ROP Grade > 2 | 3.97 (1.31–11.98) | 2.40 (0.71–8.10) |
| Bronchopulmonary dysplasia | 3.00 (1.43–6.31) | 1.66 (0.65–4.29) |
| Home oxygen | 9.75 (1.14–83.12) | 5.84 (0.65–52.13) |
| Breastfeeding Fortification | 0.37 (0.16–0.83) | 0.30 (0.13–0.70) |
| Serum phosphorus (mg/dL) | 1.59 (1.16–2.17) | 2.01 (1.38–2.91) |
| Serum Calcium (mg/dL) | 0.48 (0.26–0.87) | 0.52 (0.28–0.96) |
| Vitamin D (ng/mL) | 0.97 (0.94–1.00) | 0.96 (0.93–0.99) |
| Urine phosphorus (mg/dL) | 1.03 (0.99–1.07) | 1.02 (0.98–1.06) |
| Urine calcium (mg/dL) | 0.87 (0.77–0.98) | 0.81 (0.69–0.94) |
| Calcium/Creatinine Ratio | 0.14 (0.03–0.57) | 0.05 (0.01–0.27) |
| Phosphorus/Calcium Ratio | 1.22 (0.97–1.53) | 1.23 (0.98–1.53) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avila-Alvarez, A.; Perez Tato, H.; Sucasas Alonso, A.; Prado Carro, A.; Fuentes Carballal, J. Incidence, Risk Factors and Prediction of Secondary Hyperparathyroidism in Preterm Neonates under 32 Weeks’ Gestational Age. Nutrients 2022, 14, 3397. https://doi.org/10.3390/nu14163397
Avila-Alvarez A, Perez Tato H, Sucasas Alonso A, Prado Carro A, Fuentes Carballal J. Incidence, Risk Factors and Prediction of Secondary Hyperparathyroidism in Preterm Neonates under 32 Weeks’ Gestational Age. Nutrients. 2022; 14(16):3397. https://doi.org/10.3390/nu14163397
Chicago/Turabian StyleAvila-Alvarez, Alejandro, Helena Perez Tato, Andrea Sucasas Alonso, Ana Prado Carro, and Jesus Fuentes Carballal. 2022. "Incidence, Risk Factors and Prediction of Secondary Hyperparathyroidism in Preterm Neonates under 32 Weeks’ Gestational Age" Nutrients 14, no. 16: 3397. https://doi.org/10.3390/nu14163397
APA StyleAvila-Alvarez, A., Perez Tato, H., Sucasas Alonso, A., Prado Carro, A., & Fuentes Carballal, J. (2022). Incidence, Risk Factors and Prediction of Secondary Hyperparathyroidism in Preterm Neonates under 32 Weeks’ Gestational Age. Nutrients, 14(16), 3397. https://doi.org/10.3390/nu14163397