
Effectiveness of Dietary Interventions to Treat Iron-Deficiency Anemia in Women: A Systematic Review of Randomized Controlled Trials





Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Inclusion and Exclusion Criteria
- (1)
- Research study;
- (2)
- Randomized controlled trial;
- (3)
- Study carried out in a group of female menstruating subjects;
- (4)
- Study carried out in a group of subjects with diagnosed anemia or low iron stores;
- (5)
- Dietary intervention applied within the study, while using either regular food products, or fortified food products;
- (6)
- The effectiveness of dietary intervention assessed within the study, while using any biochemical measure of anemia/iron stores;
- (7)
- The effectiveness of dietary intervention, assessed within the study, compared with the effectiveness of supplementation, placebo, control, or another dietary approach;
- (8)
- Full text of the study published in a peer-reviewed journal;
- (9)
- Full text of the study published in English.
- (1)
- Study carried out in animal model;
- (2)
- Study carried out in a mixed population (e.g., female and male, menstruating and not menstruating), if not presenting results separately for sub-groups;
- (3)
- Study carried out in a group of pregnant women;
- (4)
- Study carried out in a group of subjects with any condition which may influence iron status (e.g., celiac disease, bariatric surgery);
- (5)
- Study carried out in a group of subjects with any eating disorder which may influence the reliability of results;
- (6)
- Study carried out in a group of subjects with any intellectual disability which may influence the reliability of results;
- (7)
- Applied dietary intervention not described within the study;
- (8)
- The effectiveness of dietary intervention influenced by interfering variables applied within the study (e.g., pharmacological intervention, physical activity intervention).
2.3. Searching Strategy
2.4. Data Extraction Procedure
- (1)
- General characteristics of the study, including: authors and year of the study, studied intervention, studied group, country/location, studied period;
- (2)
- Study participants, including: number of participants, age, inclusion criteria, exclusion criteria;
- (3)
- Applied dietary intervention, including: studied treatment/treatments, iron intake in groups, vitamin C intake in groups, intervention duration, biochemical measures;
- (4)
- Findings of the study, including: observations described by authors of the study; conclusions formulated by the authors of the study.
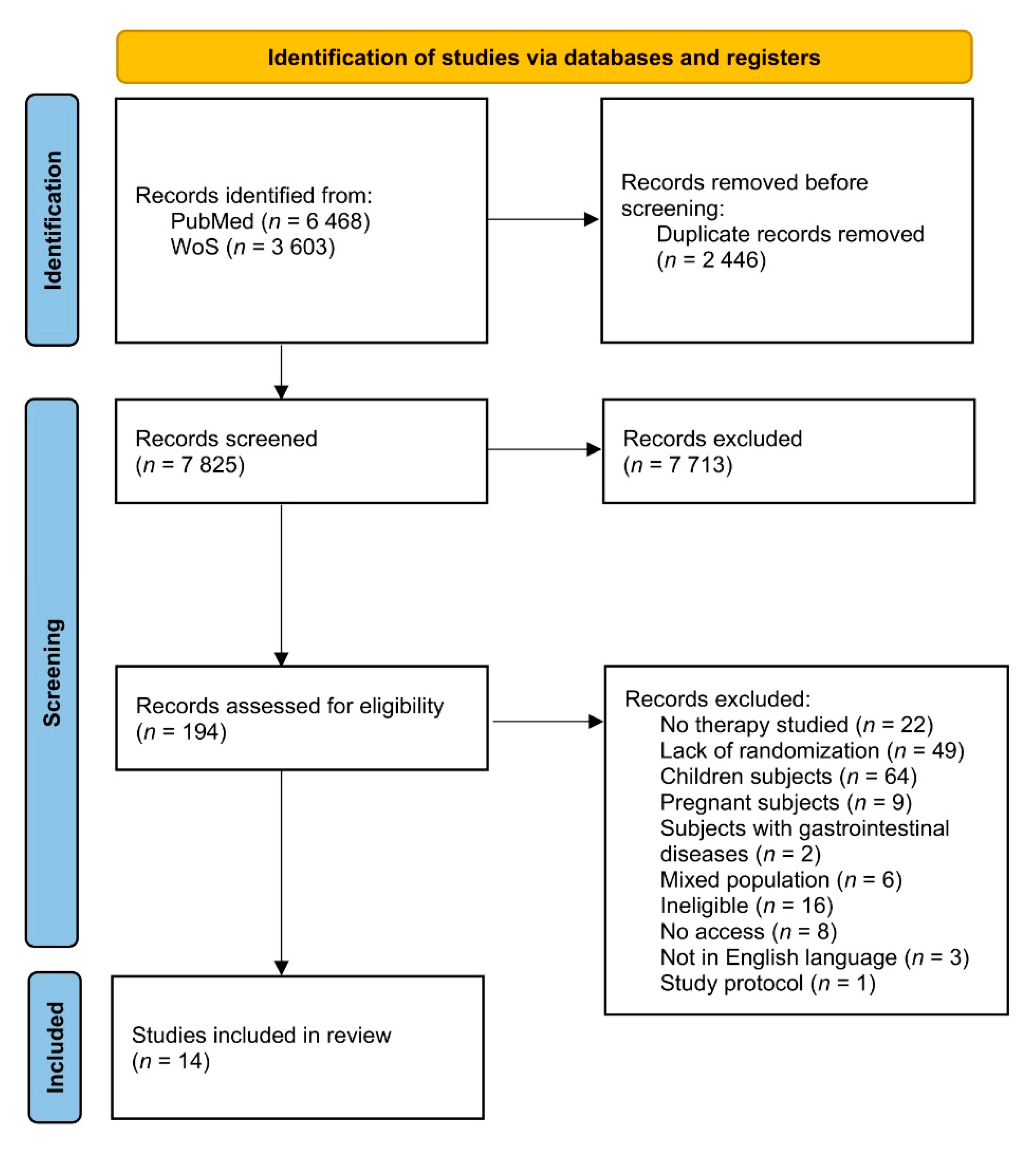
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Badireddy, M.; Baradhi, K.M. Chronic Anemia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK534803/ (accessed on 21 April 2022).
- World Health Organization. Focusing on Anaemia: Towards an Integrated Approach for Effective Anaemia Control; World Health Organization: Geneva, Switzerland, 2004.
- Chaparro, C.M.; Suchdev, P.S. Anemia epidemiology, pathophysiology, and etiology in low-and middle-income countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Ansari, T.; Ali, L.; Aziz, T.; Ara, J.; Liaquat, N.; Tahir, H. Nutritional iron deficiency in women of child bearing age—What to do? J. Ayub. Med. Coll. Abbottabad 2009, 21, 17–20. [Google Scholar] [PubMed]
- Benson, C.S.; Shah, A.; Stanworth, S.J.; Frise, C.J.; Spiby, H.; Lax, S.J.; Murray, J.; Klein, A.A. The effect of iron deficiency and anaemia on women’s health. Anaesthesia 2021, 76, 84–95. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Nutrition Targets 2025, Policy Brief Series; WHO/NMH/NHD/14.2; World Health Organization: Geneva, Switzerland, 2014.
- Weinborn, V.; Pizarro, F.; Olivares, M.; Brito, A.; Arredondo, M.; Flores, S.; Valenzuela, C. The effect of plant proteins derived from cereals and legumes on heme iron absorption. Nutrients 2015, 7, 8977–8986. [Google Scholar] [CrossRef]
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on iron and its importance for human health. J. Res. Med. Sci. 2014, 19, 164. [Google Scholar] [PubMed]
- Moustarah, F.; Mohiuddin, S.S. Dietary Iron. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK540969/ (accessed on 21 April 2022).
- Beck, K.L.; Conlon, C.A.; Kruger, R.; Coad, J. Dietary determinants of and possible solutions to iron deficiency for young women living in industrialized countries: A review. Nutrients 2014, 6, 3747–3776. [Google Scholar] [CrossRef]
- Young, I.; Parker, H.M.; Rangan, A.; Prvan, T.; Cook, R.L.; Donges, C.E.; Steinbeck, K.S.; O’Dwyer, N.J.; Cheng, H.L.; Franklin, J.L.; et al. Association between Haem and Non-Haem Iron Intake and Serum Ferritin in Healthy Young Women. Nutrients 2018, 10, 81. [Google Scholar] [CrossRef]
- World Health Organization. Nutritional Anaemias: Tools for Effective Prevention and Control; World Health Organization: Geneva, Switzerland, 2017.
- Nutritional Institutes of Health. Iron. Available online: https://ods.od.nih.gov/factsheets/Iron-HealthProfessional/ (accessed on 7 April 2022).
- Shubham, K.; Anukiruthika, T.; Dutta, S.; Kashyap, A.V.; Moses, J.A.; Anandharamakrishnan, C. Iron deficiency anemia: A comprehensive review on iron absorption, bioavailability and emerging food fortification approaches. Trends Food Sci. Technol. 2020, 99, 58–75. [Google Scholar] [CrossRef]
- Stoltzfus, R.J.; Dreyfuss, M.L.; International Nutritional Anemia Consultative Group (INACG); World Health Organization (WHO); United Nations Childrens Fund (UNICEF). Guidelines for the Use of Iron Supplements to Prevent and Treat Iron Deficiency Anemia; Stoltzfus, R.J., Dreyfuss, M.L., Eds.; ILSI Press: Washington, DC, USA, 1998.
- Tolkien, Z.; Stecher, L.; Mander, A.P.; Pereira, D.I.; Powell, J.J. Ferrous sulfate supplementation causes significant gastrointestinal side-effects in adults: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0117383. [Google Scholar] [CrossRef]
- Bullen, J.; Rogers, H.J.; Spalding, P.B.; Ward, C.G. Iron and infection: The heart of the matter. FEMS Immunol. Med. Microbiol. 2005, 43, 325–330. [Google Scholar] [CrossRef]
- Prentice, A.M.; Mendoza, Y.A.; Pereira, D.; Cerami, C.; Wegmuller, R.; Constable, A.; Spieldenner, J. Dietary strategies for improving iron status: Balancing safety and efficacy. Nutr. Rev. 2017, 75, 49–60. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Micronutrient Deficiencies. Prevention of Micronutrient Deficiencies: Tools for Policymakers and Public Health Workers. In Prevention of Iron Deficiency; Howson, C.P., Kennedy, E.T., Horwitz, A., Eds.; National Academies Press (US): Washington, DC, USA, 1998. Available online: https://www.ncbi.nlm.nih.gov/books/NBK230103/ (accessed on 21 April 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 21, e1000100. [Google Scholar] [CrossRef]
- Assessing Risk of Bias in Non-Randomized Studies. Chapter 13.5.2.3. Available online: http://handbook-5-1.cochrane.org/ (accessed on 16 November 2021).
- RoB 2: A Revised Cochrane Risk-of-Bias Tool for Randomized Trials. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 10 June 2022).
- Minozzi, S.; Cinquini, M.; Gianola, S.; Gonzalez-Lorenzo, M.; Banzi, R. The revised Cochrane risk of bias tool for randomized trials (RoB 2) showed low interrater reliability and challenges in its application. J. Clin. Epidemiol. 2020, 126, 37–44. [Google Scholar] [CrossRef]
- Heath, A.L.; Skeaff, C.M.; O’Brien, S.M.; Williams, S.M.; Gibson, R.S. Can dietary treatment of non-anemic iron deficiency improve iron status? J. Am. Coll. Nutr. 2001, 20, 477–484. [Google Scholar] [CrossRef]
- Patterson, A.J.; Brown, W.J.; Roberts, D.C.; Seldon, M.R. Dietary treatment of iron deficiency in women of childbearing age. Am. J. Clin. Nutr. 2001, 74, 650–656. [Google Scholar] [CrossRef]
- Garcia, O.P.; Diaz, M.; Rosado, J.L.; Allen, L.H. Ascorbic acid from lime juice does not improve the iron status of iron-deficient women in rural Mexico. Am. J. Clin. Nutr. 2003, 78, 267–273. [Google Scholar] [CrossRef]
- Hansen, M.; Bæch, S.B.; Thomsen, A.D.; Tetens, I.; Sandström, B. Long-term intake of iron fortified wholemeal rye bread appears to benefit iron status of young women. J. Cereal Sci. 2005, 42, 165–171. [Google Scholar] [CrossRef]
- Tetens, I.; Bendtsen, K.M.; Henriksen, M.; Ersbøll, A.K.; Milman, N. The impact of a meat-versus a vegetable-based diet on iron status in women of childbearing age with small iron stores. Eur. J. Nutr. 2007, 46, 439–445. [Google Scholar] [CrossRef]
- Navas-Carretero, S.; Pérez-Granados, A.M.; Schoppen, S.; Sarria, B.; Carbajal, A.; Vaquero, M.P. Iron status biomarkers in iron deficient women consuming oily fish versus red meat diet. J. Physiol. Biochem. 2009, 65, 165–174. [Google Scholar] [CrossRef]
- Beck, K.; Conlon, C.A.; Kruger, R.; Coad, J.; Stonehouse, W. Gold kiwifruit consumed with an iron-fortified breakfast cereal meal improves iron status in women with low iron stores: A 16-week randomised controlled trial. Br. J. Nutr. 2011, 105, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Rojo, R.; Pérez-Granados, A.M.; Toxqui, L.; González-Vizcayno, C.; Delgado, M.A.; Vaquero, M.P. Efficacy of a microencapsulated iron pyrophosphate-fortified fruit juice: A randomised, double-blind, placebo-controlled study in Spanish iron-deficient women. Br. J. Nutr. 2011, 105, 1652–1659. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Rojo, R.; Pérez-Granados, A.M.; Toxqui, L.; Zazo, P.; de la Piedra, C.; Vaquero, M.P. Relationship between vitamin D deficiency, bone remodelling and iron status in iron-deficient young women consuming an iron-fortified food. Eur. J. Nutr. 2013, 52, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Toxqui, L.; Pérez-Granados, A.M.; Blanco-Rojo, R.; Wright, I.; González-Vizcayno, C.; Vaquero, M.P. Effects of an iron or iron and vitamin D-fortified flavored skim milk on iron metabolism: A randomized controlled double-blind trial in iron-deficient women. J. Am. Coll. Nutr. 2013, 32, 312–320. [Google Scholar] [CrossRef]
- Singh, T.S.; Goyal, M.; Sheth, M. Intervention Trials with Pearl Millet Based Iron Rich Ladoo and Iron Folic Acid (IFA) Tablets on Hemoglobin Status of Adolescent Females in Bikaner City. Stud. EthnoMe. 2014, 8, 77–82. [Google Scholar] [CrossRef]
- Armah, S.M.; Boy, E.; Chen, D.; Candal, P.; Reddy, M.B. Regular Consumption of a High-Phytate Diet Reduces the Inhibitory Effect of Phytate on Nonheme-Iron Absorption in Women with Suboptimal Iron Stores. J. Nutr. 2015, 145, 1735–1739. [Google Scholar] [CrossRef]
- Haas, J.D.; Luna, S.V.; Lung’aho, M.G.; Wenger, M.J.; Murray-Kolb, L.E.; Beebe, S.; Gahutu, J.B.; Egli, I.M. Consuming Iron Biofortified Beans Increases Iron Status in Rwandan Women after 128 Days in a Randomized Controlled Feeding Trial. J. Nutr. 2016, 146, 1586–1592. [Google Scholar] [CrossRef]
- Mehta, R.; Platt, A.C.; Sun, X.; Desai, M.; Clements, D.; Turner, E.L. Efficacy of iron-supplement bars to reduce anemia in urban Indian women: A cluster-randomized controlled trial. Am. J. Clin. Nutr. 2017, 105, 746–757. [Google Scholar] [CrossRef][Green Version]
- Aspuru, K.; Villa, C.; Bermejo, F.; Herrero, P.; López, S.G. Optimal management of iron deficiency anemia due to poor dietary intake. Int. J. Gen. Med. 2011, 4, 741. [Google Scholar] [CrossRef]
- Institute for Quality and Efficiency in Health Care. How can I get enough iron? In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2006. Available online: https://www.ncbi.nlm.nih.gov/books/NBK279618/ (accessed on 23 April 2022).
- Sjöberg, A.; Hulthén, L. Comparison of food habits, iron intake and iron status in adolescents before and after the withdrawal of the general iron fortification in Sweden. Eur. J. Clin. Nutr. 2015, 69, 494–500. [Google Scholar] [CrossRef]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisie, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Kubberød, E.; Ueland, Ø.; Rødbotten, M.; Westad, F.; Risvik, E. Gender specific preferences and attitudes towards meat. Food Qual. Prefer. 2002, 13, 285–294. [Google Scholar] [CrossRef]
- Masella, R.; Malorni, W. Gender-related differences in dietary habits. Clin. Manag. Issues 2017, 11, 59–62. [Google Scholar] [CrossRef]
- Kalasuramath, S.; Kurpad, A.V.; Thankachan, P. Effect of iron status on iron absorption in different habitual meals in young south Indian women. Indian J. Med. Res. 2013, 137, 324–330. [Google Scholar] [PubMed]
- Fernández-Lázaro, D.; Mielgo-Ayuso, J.; Córdova Martínez, A.; Seco-Calvo, J. Iron and physical activity: Bioavailability enhancers, properties of black pepper (bioperine®) and potential applications. Nutrients 2020, 12, 1886. [Google Scholar] [CrossRef]
- Teucherl, B.; Cori, M.O.H. Enhancers of iron absorption: Ascorbic acid and other organic acids. Int. J. Vitam. Nutr. Res. 2004, 74, 403–419. [Google Scholar] [CrossRef]
- Sabatier, M.; Rytz, A.; Husny, J.; Dubascoux, S.; Nicolas, M.; Dave, A.; Singh, H.; Bodis, M.; Glahn, R.P. Impact of Ascorbic Acid on the In Vitro Iron Bioavailability of a Casein-Based Iron Fortificant. Nutrients 2020, 12, 2776. [Google Scholar] [CrossRef]
- Lynch, S.R.; Cook, J.D. Interaction of vitamin C and iron. Ann. N. Y. Acad. Sci. 1980, 355, 32–44. [Google Scholar] [CrossRef]
- Hurrell, R. How to ensure adequate iron absorption from iron-fortified food. Nutr. Rev. 2002, 60, S7–S15. [Google Scholar] [CrossRef]
- Smith, E.M.; Tangpricha, V. Vitamin D and anemia: Insights into an emerging association. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 432. [Google Scholar] [CrossRef]
- Madar, A.A.; Stene, L.C.; Meyer, H.E.; Brekke, M.; Lagerløv, P.; Knutsen, K.V. Effect of vitamin D 3 supplementation on iron status: A randomized, double-blind, placebo-controlled trial among ethnic minorities living in Norway. Nutr. J. 2015, 15, 74. [Google Scholar] [CrossRef] [PubMed]
- Collings, R.; Harvey, L.J.; Hooper, L.; Hurst, R.; Brown, T.J.; Ansett, J.; King, M.; Fairweather-Tait, S.J. The absorption of iron from whole diets: A systematic review. Am. J. Clin. Nutr. 2013, 98, 65–81. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Jimenez, M.C.; Moreno, G.; Wright, I.; Shih, P.C.; Vaquero, M.P.; Remacha, A.F. Iron deficiency in menstruating adult women: Much more than anemia. Women’s Health Rep. 2020, 1, 26–35. [Google Scholar] [CrossRef]
- Ofojekwu, M.J.N.; Nnanna, O.U.; Okolie, C.E.; Odewumi, L.A.; Isiguzoro, I.O.; Lugos, M.D. Hemoglobin and serum iron concentrations in menstruating nulliparous women in Jos, Nigeria. Lab. Med. 2013, 44, 121–124. [Google Scholar] [CrossRef]
- Napolitano, M.; Dolce, A.; Celenza, G.; Grandone, E.; Perilli, M.G.; Siragusa, S.; Carta, G.; Orecchioni, A.; Mariani, G. Iron-dependent erythropoiesis in women with excessive menstrual blood losses and women with normal menses. Ann. Hematol. 2014, 93, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Harvey, L.J.; Armah, C.N.; Dainty, J.R.; Foxall, R.J.; Lewis, D.J.; Langford, N.J.; Fairweather-Tait, S.J. Impact of menstrual blood loss and diet on iron deficiency among women in the UK. Br. J. Nutr. 2005, 94, 557–564. [Google Scholar] [CrossRef]
- Chalmers, I. The Cochrane Collaboration: Preparing, maintaining, and disseminating systematic reviews of the effects of health care. Ann. N. Y. Acad. Sci 1993, 703, 156–165. [Google Scholar] [CrossRef]


{kind=link}
| PICOS | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Menstruating human subjects with anemia/low iron stores | Patients with any diseases and conditions, which may influence iron status or influence the reliability of results; pregnancy |
| Intervention/exposure | Dietary intervention applied to correct anemia/low iron stores | Dietary intervention not described within the study |
| Comparison | Effectiveness of dietary intervention compared with the effectiveness of supplementation, placebo, control, or the other dietary approach | Effectiveness of dietary intervention influenced by interfering variables applied within the study |
| Outcome | Biochemical measure of anemia/iron stores | Biochemical measure of anemia/iron stores presented for a mixed population only |
| Study design | Randomized controlled trials | Studies not published in peer-reviewed journals; studies not published in English; retracted articles |
| Database | The Detailed Electronic Searching Strategy |
|---|---|
| PubMed | (“anaemia”[Title/Abstract] OR “anemia”[Title/Abstract] OR “anaemic”[Title/Abstract] OR “anemic”[Title/Abstract] OR “low haemoglobin”[Title/Abstract] OR “iron status”[Title/Abstract]) AND (“iron”[Title/Abstract]) AND (“nutrition”[Title/Abstract] OR “diet”[Title/Abstract] OR “diets”[Title/Abstract] OR “nutritional”[Title/Abstract] OR “dietary”[Title/Abstract]) |
| Web of Science | AB = (anaemia OR anemia OR anaemic OR anemic OR low haemoglobin OR iron status) AND AB = (iron) AND AB = (nutrition OR diet OR diets OR nutritional OR dietary) |
| Ref. | Authors, Year | Studied Intervention | Studied Group | Country/Location | Studied Period |
|---|---|---|---|---|---|
| [25] | Heath et al. 2001 | Diet vs. iron supplement vs. placebo | Young to middle-aged women with mild iron deficiency anemia | New Zealand/Dunedin area | March 1997–September 1998 * |
| [26] | Patterson et al. 2001 | Diet vs. iron supplement vs. control | Iron deficient (in diet and iron supplement group) and iron replete with no history of iron deficiency (in control group) young to middle-aged women | Australia/Newcastle | Not specified |
| [27] | Garcia et al. 2003 | Diet with beverage high in vitamin C vs. diet with placebo beverage | Young to middle-aged iron-deficient women | Mexico/Solís Valley | Not specified |
| [28] | Hansen et al. 2005 | Diet (with bread) vs. diet (with iron-fortified bread) | Young to middle-aged women with low iron stores | Denmark * | Not specified |
| [29] | Tetens et al. 2007 | Meat-based diet vs. vegetable-based diet | Young to middle-aged women with low iron stores | Denmark | Not specified |
| [30] | Navas-Carretero et al. 2009 | Oily fish diet vs. red meat diet | Young women with low iron stores | Not specified | Not specified |
| [31] | Beck et al. 2011 | Diet (with iron-fortified cereals and gold kiwi) vs. diet (with iron-fortified cereals and banana) | Young to middle-aged women with low iron stores | New Zealand/Auckland | Not specified |
| [32] | Blanco-Rojo et al. 2011 | Diet with iron-fortified juice vs. diet with placebo juice | Young women with low iron stores | Spain/Madrid | Not specified |
| [33] | Blanco-Rojo et al. 2013 | Diet with iron-fortified juice vs. diet with placebo juice | Young women with low iron stores | Spain/Madrid | November–March 2009 * |
| [34] | Toxqui et al. 2013 | Diet with iron-fortified flavored milk vs. diet with iron and vitamin D fortified flavored milk | Young women with low iron stores | Spain/Madrid | Not specified |
| [35] | Singh et al. 2014 | Diet vs. supplement vs. control | Anemic adolescent girls | India/Bikaner | Not specified |
| [36] | Armah et al. 2015 | High-phytate diet vs. low-phytate diet | Young women with suboptimal iron stores | United States of America/Iowa state | Spring of 2013 |
| [37] | Haas et al. 2016 | Diet vs. control | Young women with low iron stores | Rwanda/Huye | 7 January–15 May 2013 |
| [38] | Mehta et al. 2017 | Diet with iron-fortified product vs. control | Young anemic women | India/Mumbai and Navi Mumbai | March–August 2014 |
| Ref. | Number of Participants | Age (Mean ± SD/Median/Range) | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|
| [25] | 57 | 25.4–30.8 years, depending on group | Women; 18–40 years; mild iron deficiency anemia (serum ferritin < 20 μg/L and hemoglobin ≥ 120 g/L) | Pregnancy; lactation; irregular menstruation; health problems likely to influence iron status; medication likely to affect iron status; anorexia nervosa or bulimia; veganism; taking iron, vitamin C, or calcium supplements during the study; donating blood |
| [26] | 66 | 18–50 years | Women; ≥18 years; menstruation; hemoglobin ≥ 90 g/L; iron deficiency (serum ferritin < 15 µg/L or serum ferritin 15–20 µg/L with two other hematological parameters indicative of iron deficiency e.g., serum iron < 10 µmol/L, total iron binding capacity > 68 µmol/L, transferrin saturation < 15%), or iron replete group (hemoglobin ≥ 120 g/L and serum ferritin > 20 µg/L) | Major illness; pregnancy; hysterectomy |
| [27] | 36 | 28.2–28.3 years, depending on group | Women; ≥18 years; inhabitants of rural area of Solís Valley; iron deficiency (plasma ferritin < 12 µg/L) | Pregnancy |
| [28] | 43 | 24.1–24.9 years, depending on group | Women; heathy; low iron stores (serum ferritin 11–32 μg/L) | Receiving medical treatment; taking mineral/vitamin supplements within 2 months prior to or during the study; taking any iron supplement 6 months before the study; donating blood during or within 2 months prior to the study; smoking; pregnancy; lactation |
| [29] | 57 | 26 (19–39) years | Women; 19–39 years; premenopausal; low iron stores (serum ferritin ≤ 30 µg/L and hemoglobin ≥ 120 g/L) | Pregnancy; lactation; smoking; performing heavy exercise; donating blood or using any dietary supplements 3 months prior to and during the intervention period |
| [30] | 25 | 18–30 years | Women; 18–30 years; menstruating; non-smoking; low iron stores (ferritin < 30 µg/L) | Hemoglobin < 110 g/L; taking iron supplements or having taken them in the 12 months previous to the study; chronic gastric or iron-metabolism-related disease; being allergic to fish; being vegetarian |
| [31] | 69 | 31–35 years, depending on group | Women; 18–44 years; low iron stores (serum ferritin ≤ 25 µg/L and hemoglobin ≥ 115 g/L) | Pregnancy; lactation; health problems likely to influence iron status; allergy or intolerance to any components of the breakfast meal; donating blood; consuming iron, vitamin C or Ca supplements for the duration of the study; regular consumption of iron supplements within the 3-month period before commencement of the study |
| [32] | 122 | 24.2–24.5 years, depending on group | Women; aged 18–35 years; low iron stores (serum ferritin < 40 µg/L and hemoglobin ≥ 110 g/L) | Amenorrhea; menopause; pregnancy; lactation; smoking; having any known health problems likely to influence iron status; allergy to some of the components of the assay product; being blood donors; regularly consumed iron supplements within the 4 months prior to participating in the intervention |
| [33] | 41 | 25.5 ± 5.9 years | Women; aged 18–35 years; low iron stores (serum ferritin < 40 µg/L and hemoglobin ≥ 110 g/L) | Amenorrhea; menopause; pregnancy; lactation; smoking; having any known health problems likely to influence iron status; allergy to some of the components of the assay product; being blood donors; regularly consumed iron supplements within the 4 months prior to participating in the intervention |
| [34] | 109 | 24.7–24.8 years, depending on group | Women; aged 18–35 years; low iron stores (serum ferritin <30 µg/L and hemoglobin ≥ 110 g/L) | Amenorrhea; menopause; pregnancy; lactation; smoking; having any known health problems likely to influence iron status; allergy to some of the components of the assay product; being blood donors; regularly consumed iron supplements within the 4 months prior to participating in the intervention |
| [35] | 30 | 16–19 years | Female; aged 16–19 years; moderately anemic (hemoglobin 80–109 g/L) | Not specified |
| [36] | 28 | 18–33 years | Women; aged 18–35 years; suboptimal iron stores (serum ferritin ≤ 30 µg/L and hemoglobin ≥ 120 g/L); BMI of 18.5–24.9 kg/m2 | Pregnancy; lactation; smoking; taking any drug that interferes with iron absorption; any gastrointestinal disease/condition that can affect iron absorption |
| [37] | 195 | 22 years | Women; aged 18–27 years; low iron stores (serum ferritin < 20 µg/L and hemoglobin ≥ 90 g/L); students at the University of Rwanda at Huye | Pregnancy; lactation; using iron supplements; any major medical conditions; using medications that could interfere with dietary iron absorption; using psychoactive drugs; BMI < 16 kg/m2 |
| [38] | 179 | 28.6–28.9 years, depending on group | Women; aged 18–35 years; anemia (hemoglobin < 120 g/L) | Pregnancy; nut allergy; taking iron supplements |
| Ref. | Characteristics of Studied Treatment/Treatments | Iron Intake in Groups | Vitamin C Intake in Groups | Intervention Duration | Biochemical Measure |
|---|---|---|---|---|---|
| [25] | (1) Diet: individual dietary advice by a registered dietitian to increase their iron intake and to increase the bioavailability of iron; 250 mL of fruit juice containing 30 mg/dL vitamin C to be consumed with meals (2) Iron supplement: 50 mg of elemental iron (3) Placebo | Diet: 12.4 mg/day; Iron supplement: 11.1 mg/day; Placebo: 11.0 mg/day | Diet: 235 mg/day; Iron supplement: 95.8 mg/day; Placebo: 98.7 mg/day | 16 weeks | Hemoglobin, serum ferritin, serum transferrin receptor |
| [26] | (1) Diet: high iron diet to provide the recommended daily intake of absorbed iron (2.25 mg); iron-absorption enhancers (meat or vitamin C rich products) at each meal; consumption of tea, coffee, and milk discouraged at lunch and dinner and for 1 h afterward; “meat vouchers” to purchase lean beef or lamb (2) Iron supplement: 350 mg ferrous sulphate supplement (equivalent to 105 mg of inorganic iron) (3) Control | Non-heme + heme iron Diet: 10.5 + 1.3 mg/day; Iron supplement: 12.0 + 0.8 mg/day; Control: 9.5 + 1.2 mg/day | Diet: 174.6 mg/day; Iron supplement: 131.2 mg/day; Control: 113.7 mg/day | 12 weeks + 6 months (follow-up) | Hemoglobin, serum ferritin, serum iron, iron binding capacity |
| [27] | (1) Diet with beverage high in vitamin C (500 mL limeade containing 25 mg of ascorbic acid), consumed within 30 min of 2 main daily meals 6 days/week (2) Diet with placebo beverage (lime-flavored, free of ascorbic acid or citric acid), consumed within 30 min of 2 main daily meals 6 days/week | Non-heme + heme iron Diet with beverage high in vitamin C: 11.1 + 0.8 mg/day; Diet with placebo beverage: 11.4 + 1.0 mg/day | Diet with beverage high in vitamin C: 112.9 mg/day; Diet with placebo beverage: 56.0 mg/day | 8 months | Hemoglobin, plasma ferritin, plasma transferrin receptors |
| [28] | (1) Diet with bread: 120–160 g rye bread daily (iron 1.4 mg/100 g bread) (2) Diet with iron-fortified bread: 120–160 g rye bread daily fortified with ferrous fumarate (total iron content 7.5 mg/100 g bread) | Habitual intake Diet with bread: 13.5 mg/day; Diet with iron-fortified bread: 13.9 mg/day | Habitual intake Diet with bread: 127 mg/day; Diet with iron-fortified bread: 114 mg/day | 5 months | Hemoglobin, serum ferritin |
| [29] | (1) Meat-based diet: 150 g meat daily (2) Vegetable-based diet: maximum of 250 g meat and 120 g fish per week | Meat-based diet: 11.0 mg/day; Vegetable-based diet: 12.3 mg/day | Meat-based diet: 80 mg/day; Vegetable-based diet: 150 mg/day | 20 weeks | Hemoglobin, serum ferritin |
| [30] | (1) Oily fish diet: 5 portions of red meat, 1 portion of lean fish, 2 portions of poultry, and 2 eggs per week (2) Red meat diet: 2 portions of salmon, 1 of water-packed tuna, 1 of sardines in olive oil, 1 portion of lean fish, 1 portion of red meat, 2 portions of poultry, and 2 eggs per week Crossover of treatment applied after 8 weeks | Oily fish diet: 11.54 mg/day; Red meat diet: 13.93 mg/day | Oily fish diet: 94.3 mg/day; Red meat diet: 89.2 mg/day | 16 weeks | Hemoglobin, hematocrit, serum ferritin, serum iron, serum transferrin, serum transferrin receptor |
| [31] | (1) Diet with iron-fortified cereals and gold kiwi: breakfast including 64.4 g of iron-fortified cereals with dried apricot pieces (16 mg of iron per serving), 150 mL of low-fat milk, and 171 of gold kiwi (2) Diet with iron-fortified cereals and banana: breakfast including 64.4 g of iron-fortified cereals with dried apricot pieces (16 mg of iron per serving), 150 mL of low-fat milk and 104 g of banana | Meal with gold kiwi: 16.6 mg/day; Meal with banana: 16.4 mg/day | Meal with gold kiwi: 164 mg/day; Meal with banana: 1.4 mg/day | 16 weeks | Hemoglobin, serum ferritin, soluble transferrin receptor |
| [32] | (1) Diet with iron-fortified juice (500 mL, containing 18 mg of iron) (2) Diet with placebo juice (500 mL) | Diet with iron-fortified juice: 30.4 mg/day; Diet with placebo juice: 12.9 mg/day | Diet with iron-fortified juice: 190.2 mg/day; Diet with placebo juice: 199.8 mg/day | 16 weeks | Total erythrocytes, hematocrit, mean corpuscular volume, red blood cell distribution width, hemoglobin, serum iron, serum ferritin, serum transferrin, transferrin saturation, soluble transferrin receptor |
| [33] | (1) Diet with iron-fortified juice (500 mL, containing 18 mg of iron) (2) Diet with placebo juice (500 mL) | Diet with iron-fortified juice: 32.1 mg/day; Diet with placebo juice: 14 mg/day | Diet with iron-fortified juice: 206.2 mg/day; Diet with placebo juice: 200.6 mg/day | 16 weeks | Hemoglobin, serum ferritin, serum transferrin, transferrin saturation |
| [34] | (1) Diet with iron-fortified flavored skim milk (500 mL, containing 15 mg of iron) (2) Diet with iron and vitamin D fortified flavored skim milk (500 mL, containing 15 mg of iron and 5 µg of vitamin D) | Diet with iron-fortified flavored milk: 27.5 mg/day; Diet with iron and vitamin D fortified flavored milk: 26.1 mg/day | Not specified | 16 weeks | Total erythrocytes, hemoglobin, hematocrit, red blood cell distribution width, mean corpuscular volume, mean corpuscular hemoglobin, serum iron, serum ferritin, serum transferrin, transferrin saturation, total iron binding capacity, soluble transferrin receptor |
| [35] | (1) Diet: 100 g of pearl-millet-based iron rich product (15 mg non-heme iron), 200 mL of lemon water (2) Supplement: iron (60 mg elemental iron), folic acid (3) Control | Not specified | Not specified | 45 days | Hemoglobin |
| [36] | (1) Diet of high-phytate: high-phytate foods with at least 2 daily meals (whole grain ready-to-eat cereals, whole wheat pasta/spaghetti, tortillas, bagels, bread and dinner rolls, corn tortillas, brown rice, canned black beans, edamame, tofu, nuts, legume products) (2) Diet of low-phytate: low-phytate foods with at least 2 daily meals (foods made from refined wheat and white rice, eggs, and cheese), instructed to avoid high-phytate foods | Diet of high-phytate: 14.1 mg/day; Diet of low-phytate: 14.1 mg/day | Diet of high-phytate: 76 mg/day; Diet of low-phytate: 52 mg/day | 8 weeks | Serum ferritin, serum transferrin receptor, body iron |
| [37] | (1) Diet including Fe-beans for 2 meals per day (175 g of cooked beans per meal) (2) Control diet including regular beans for 2 meals per day (175 g of cooked beans per meal) | Iron from beans Diet including Fe-beans: 14.5 mg/day; Control diet: 8.6 mg/day | For both diets: 158 mg/day * | 128 days | Hemoglobin, serum ferritin, soluble transferrin receptor, body iron |
| [38] | (1) Diet with iron-fortified product: iron-supplement bar (14 mg of iron) (2) Control | Not specified | Not specified | 90 days | Hemoglobin, hematocrit |
| Dietary Approach | Ref. | Conclusion * | |
|---|---|---|---|
| Increasing iron supply | [28] | Supporting | |
| [29] | Supporting | ||
| [30] | Not supporting | ||
| [32] | Supporting | ||
| [33] | Supporting | ||
| [37] | Supporting | ||
| [38] | Supporting | ||
| Increasing iron supply and increasing its absorption by vitamin C supply | [25] | Supporting | |
| [26] | Supporting | ||
| [35] | Supporting | ||
| Increasing iron absorption | Increasing vitamin C supply | [27] | Not supporting |
| [31] | Supporting | ||
| Increasing vitamin D supply | [34] | Supporting | |
| Decreasing phytate supply | [36] | Not supporting | |
| Ref. | D1 | D2 | D3 | D4 | D5 | Overall Bias | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Increasing iron supply | [28] |  |  | | |  |  | | Low risk | |
| [29] | | | | | |  | | Some concerns | ||
| [30] | | | | | | | | High risk | ||
| [32] | | | | | | | ||||
| [33] | | | | | | | ||||
| [37] | | | | | | | ||||
| [38] | | | | | | | ||||
| Increasing iron supply and increasing its absorption by vitamin C supply | [25] | | | | | | | |||
| [26] | | | | | | | ||||
| [35] | | | | | | | ||||
| Increasing iron absorption | Increasing vitamin C supply | [27] | | | | | | | ||
| [31] | | | | | | | ||||
| Increasing vitamin D supply | [34] | | | | | | | |||
| Decreasing phytate supply | [36] | | | | | | | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skolmowska, D.; Głąbska, D.; Kołota, A.; Guzek, D. Effectiveness of Dietary Interventions to Treat Iron-Deficiency Anemia in Women: A Systematic Review of Randomized Controlled Trials. Nutrients 2022, 14, 2724. https://doi.org/10.3390/nu14132724
Skolmowska D, Głąbska D, Kołota A, Guzek D. Effectiveness of Dietary Interventions to Treat Iron-Deficiency Anemia in Women: A Systematic Review of Randomized Controlled Trials. Nutrients. 2022; 14(13):2724. https://doi.org/10.3390/nu14132724
Chicago/Turabian StyleSkolmowska, Dominika, Dominika Głąbska, Aleksandra Kołota, and Dominika Guzek. 2022. "Effectiveness of Dietary Interventions to Treat Iron-Deficiency Anemia in Women: A Systematic Review of Randomized Controlled Trials" Nutrients 14, no. 13: 2724. https://doi.org/10.3390/nu14132724
APA StyleSkolmowska, D., Głąbska, D., Kołota, A., & Guzek, D. (2022). Effectiveness of Dietary Interventions to Treat Iron-Deficiency Anemia in Women: A Systematic Review of Randomized Controlled Trials. Nutrients, 14(13), 2724. https://doi.org/10.3390/nu14132724