
Associations between Depression, Nutritional Status and Mediterranean Diet in Dalmatian Kidney Transplant Recipients

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Body Composition and Anthropometric Measurement
2.3. Depression Assessment
2.4. Mediterranean Diet Serving Score
2.5. Medical History and Clinical and Laboratory Parameters
2.6. Statistical Analysis
3. Results
4. Discussion
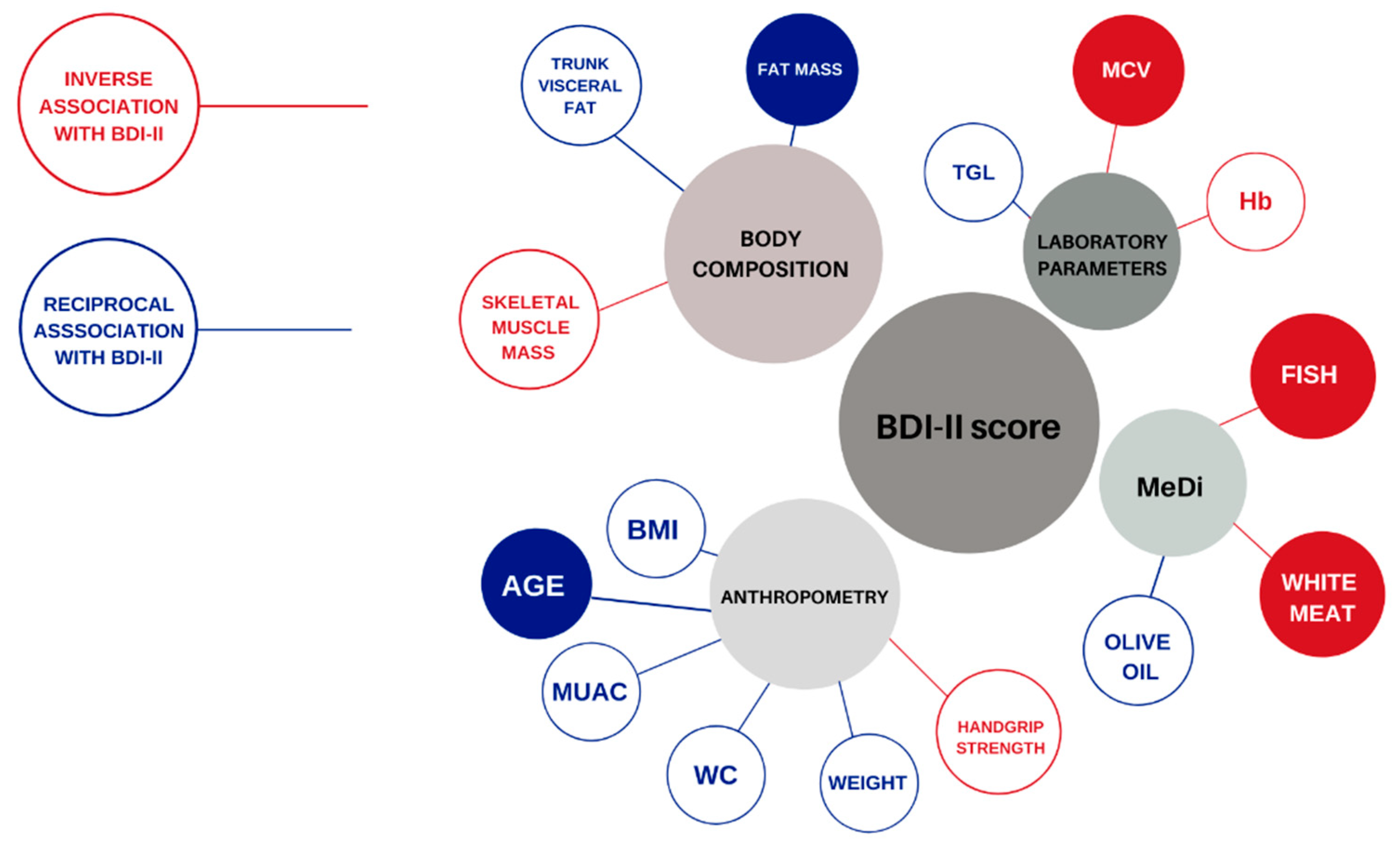
4.1. Body Composition and Depression in Dalmatian KTRs
4.2. Anthropometric Parameters and Depression in Dalmatian KTRs
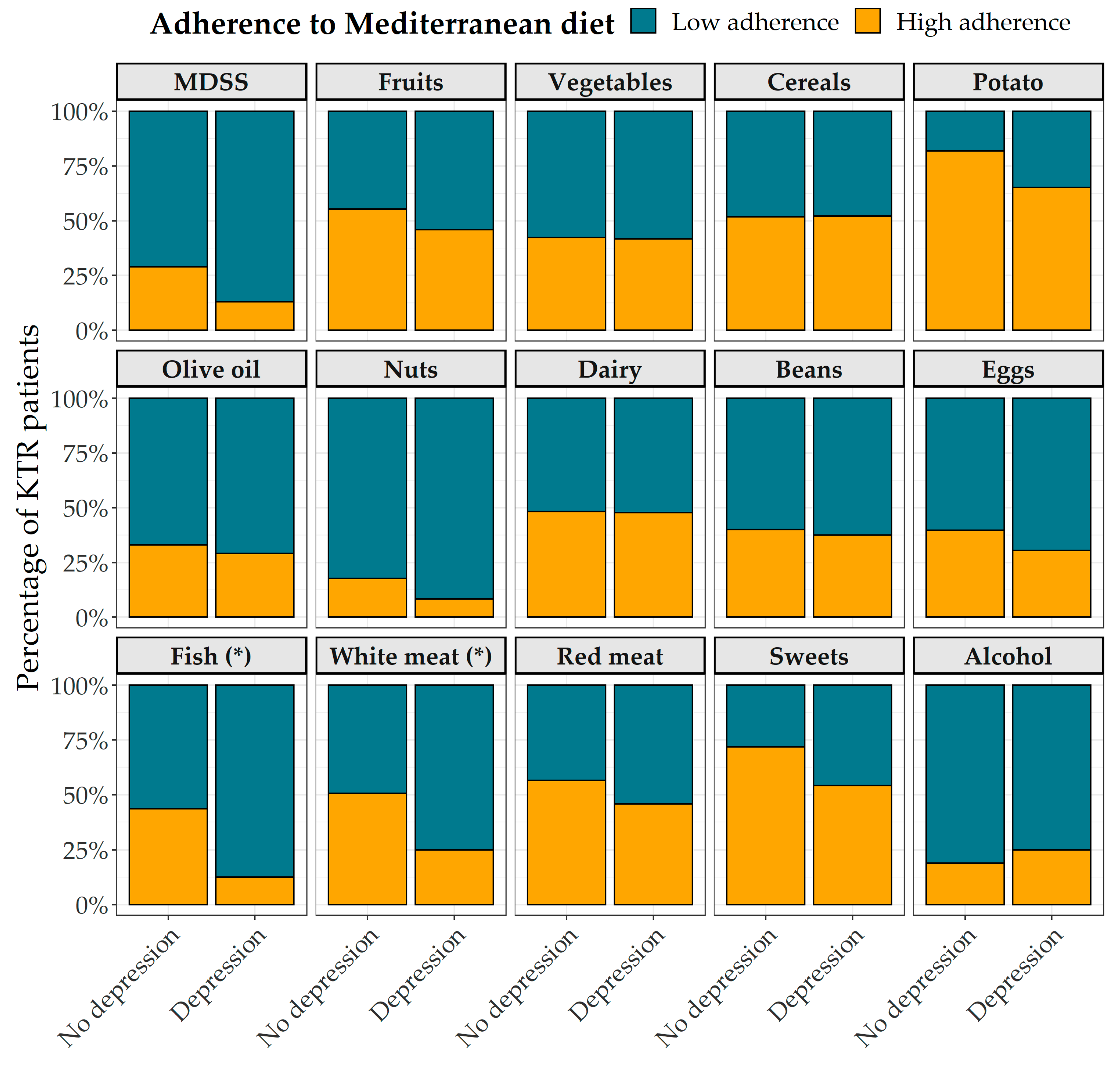
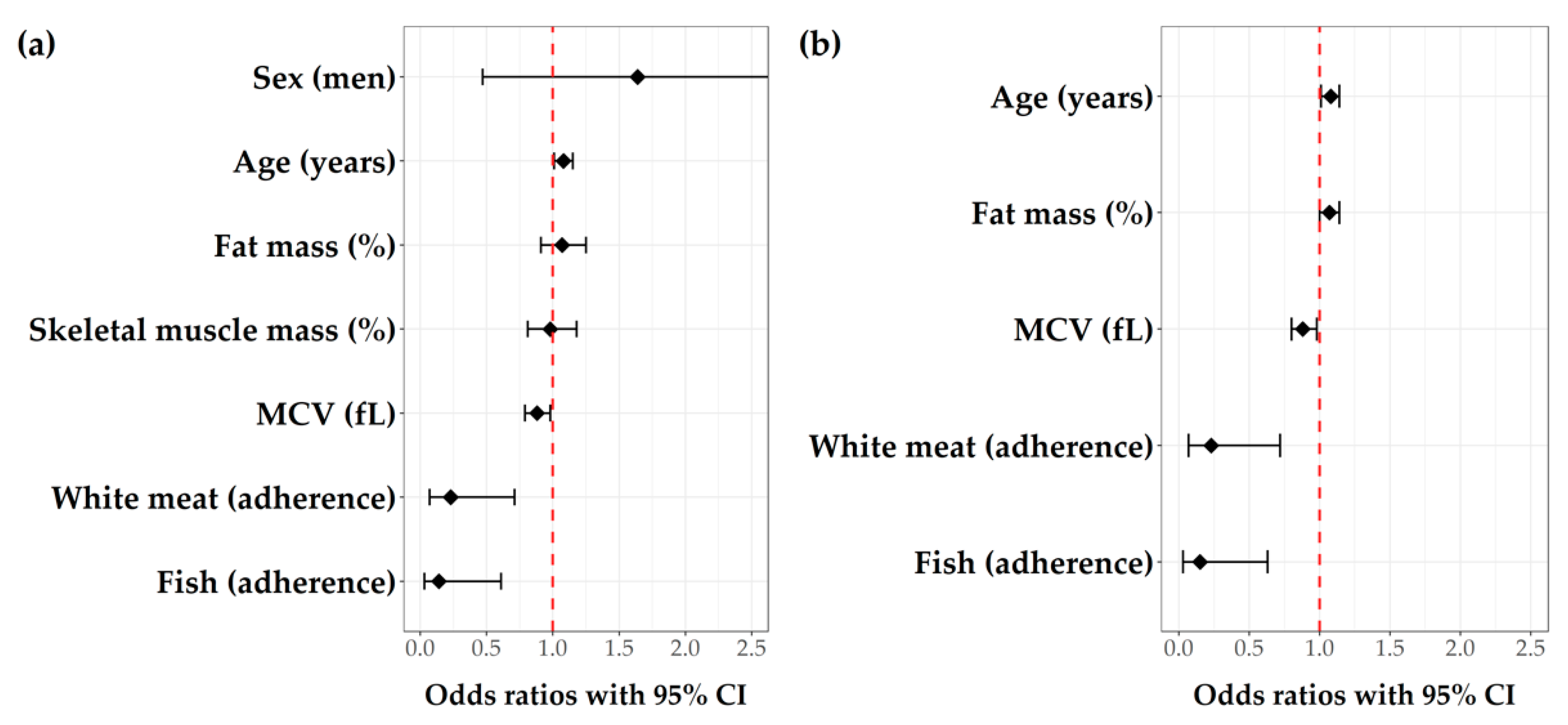
4.3. Mediterranean Diet and Depression in Dalmatian KTRs
4.4. Laboratory Parameters and Depression in Dalmatian KTRs
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tantisattamo, E.; Ho, B.T.; Workeneh, B.T. Editorial: Metabolic Changes After Kidney Transplantation. Front. Med. 2021, 8, 709644. [Google Scholar] [CrossRef] [PubMed]
- de Pasquale, C.; Luisa Pistorio, M.; Veroux, M.; Indelicato, L.; Biffa, G.; Bennardi, N.; Zoncheddu, P.; Martinelli, V.; Giaquinta, A.; Veroux, P. Psychological and Psychopathological Aspects of Kidney Transplantation: A Systematic Review. Front. Psychiatry 2020, 11, 106. [Google Scholar] [CrossRef] [Green Version]
- Palmer, S.; Vecchio, M.; Craig, J.C.; Tonelli, M.; Johnson, D.W.; Nicolucci, A.; Pellegrini, F.; Saglimbene, V.; Logroscino, G.; Fishbane, S.; et al. Prevalence of Depression in Chronic Kidney Disease: Systematic Review and Meta-Analysis of Observational Studies. Kidney Int. 2013, 84, 179–191. [Google Scholar] [CrossRef] [Green Version]
- Chilcot, J.; Spencer, B.W.J.; Maple, H.; Mamode, N. Depression and Kidney Transplantation. Transplantation 2014, 97, 717–721. [Google Scholar] [CrossRef]
- Zelle, D.M.; Dorland, H.F.; Rosmalen, J.G.M.; Corpeleijn, E.; Gans, R.O.B.; Homan van der Heide, J.J.; van Son, W.J.; Navis, G.; Bakker, S.J.L. Impact of Depression on Long-Term Outcome After Renal Transplantation. Transplantation 2012, 94, 1033–1040. [Google Scholar] [CrossRef] [Green Version]
- Novak, M.; Zsolt Molnar, M.; Szeifert, L.; Zsofia Kovacs, A.; Panna Vamos, E.; Zoller, R.; Keszei, A.; Mucsi, I. Depressive Symptoms and Mortality in Patients After Kidney Transplantation: A Prospective Prevalent Cohort Study. Psychosom. Med. 2010, 72, 527–534. [Google Scholar] [CrossRef]
- Szeifert, L.; Molnar, M.Z.; Ambrus, C.; Koczy, A.B.; Kovacs, A.Z.; Vamos, E.P.; Keszei, A.; Mucsi, I.; Novak, M. Symptoms of Depression in Kidney Transplant Recipients: A Cross-Sectional Study. Am. J. Kidney Dis. 2010, 55, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Czira, M.E.; Lindner, A.V.; Szeifert, L.; Molnar, M.Z.; Fornadi, K.; Kelemen, A.; Laszlo, G.; Mucsi, I.; Keszei, A.P.; Kennedy, S.H.; et al. Association between the Malnutrition–Inflammation Score and Depressive Symptoms in Kidney Transplanted Patients. Gen. Hosp. Psychiatry 2011, 33, 157–165. [Google Scholar] [CrossRef]
- Cukor, D.; Rosenthal, D.S.; Jindal, R.M.; Brown, C.D.; Kimmel, P.L. Depression Is an Important Contributor to Low Medication Adherence in Hemodialyzed Patients and Transplant Recipients. Kidney Int. 2009, 75, 1223–1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabbatini, M.; Ferreri, L.; Pisani, A.; Capuano, I.; Morgillo, M.; Memoli, A.; Riccio, E.; Guida, B. Nutritional Management in Renal Transplant Recipients: A Transplant Team Opportunity to Improve Graft Survival. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Hori, S.; Ichikawa, K.; Morizawa, Y.; Gotoh, D.; Itami, Y.; Nakai, Y.; Miyake, M.; Yoneda, T.; Tanaka, N.; Yoshida, K.; et al. Clinical Significance of Postoperative Nutritional Status as a Prognostic Factor in Kidney Transplant Recipients. Transplant. Proc. 2019, 51, 1763–1772. [Google Scholar] [CrossRef]
- Piotti, G.; Gandolfini, I.; Palmisano, A.; Maggiore, U. Metabolic Risk Profile in Kidney Transplant Candidates and Recipients. Nephrol. Dial. Transplant. 2019, 34, 388–400. [Google Scholar] [CrossRef]
- Stanfill, A.; Bloodworth, R.; Cashion, A. Lessons Learned: Experiences of Gaining Weight by Kidney Transplant Recipients. Prog. Transplant. 2012, 22, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Rocca-Rey, L.A.; Bacchi, G.; Wasi, N.; Schmitz, L.; Salvalaggio, P.R.; Abbott, K.C.; Schnitzler, M.A.; Neri, L.; Brennan, D.C. Obesity and Cardiac Risk after Kidney Transplantation: Experience at One Center and Comprehensive Literature Review. Transplantation 2008, 86, 303–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wissing, K.M.; Pipeleers, L. Obesity, Metabolic Syndrome and Diabetes Mellitus after Renal Transplantation: Prevention and Treatment. Transplant. Rev. 2014, 28, 37–46. [Google Scholar] [CrossRef]
- Milano, W.; Ambrosio, P.; Carizzone, F.; de Biasio, V.; di Munzio, W.; Foia, M.G.; Capasso, A. Depression and Obesity: Analysis of Common Biomarkers. Diseases 2020, 8, 23. [Google Scholar] [CrossRef] [PubMed]
- Stanfill, A.; Hathaway, D.; Bloodworth, R.; Cashion, A. A Prospective Study of Depression and Weight Change After Kidney Transplant. Prog. Transplant. 2016, 26, 70–74. [Google Scholar] [CrossRef]
- Wang, H.; Liu, F.; Ma, H.; Yin, H.; Wang, P.; Bai, B.; Guo, L.; Geng, Q. Associations between Depression, Nutrition, and Outcomes among Individuals with Coronary Artery Disease. Nutrition 2021, 86, 111157. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Ruíz-Canela, M.; Gea, A.; Lahortiga, F.; Martínez-González, M.A. The Association Between the Mediterranean Lifestyle and Depression. Clin. Psychol. Sci. 2016, 4, 1085–1093. [Google Scholar] [CrossRef]
- Parletta, N.; Zarnowiecki, D.; Cho, J.; Wilson, A.; Bogomolova, S.; Villani, A.; Itsiopoulos, C.; Niyonsenga, T.; Blunden, S.; Meyer, B.; et al. A Mediterranean-Style Dietary Intervention Supplemented with Fish Oil Improves Diet Quality and Mental Health in People with Depression: A Randomized Controlled Trial (HELFIMED). Nutr. Neurosci. 2019, 22, 474–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliván-Blázquez, B.; Aguilar-Latorre, A.; Motrico, E.; Gómez-Gómez, I.; Zabaleta-del-Olmo, E.; Couso-Viana, S.; Clavería, A.; Maderuelo-Fernandez, J.A.; Recio-Rodríguez, J.I.; Moreno-Peral, P.; et al. The Relationship between Adherence to the Mediterranean Diet, Intake of Specific Foods and Depression in an Adult Population (45–75 Years) in Primary Health Care. A Cross-Sectional Descriptive Study. Nutrients 2021, 13, 2724. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Neto, A.W.; Osté, M.C.J.; Sotomayor, C.G.; van den Berg, E.; Geleijnse, J.M.; Berger, S.P.; Gans, R.O.B.; Bakker, S.J.L.; Navis, G.J. Mediterranean Style Diet and Kidney Function Loss in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2020, 15, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Osté, M.C.J.; Corpeleijn, E.; Navis, G.J.; Keyzer, C.A.; Soedamah-Muthu, S.S.; van den Berg, E.; Postmus, D.; de Borst, M.H.; Kromhout, D.; Bakker, S.J.L. Mediterranean Style Diet Is Associated with Low Risk of New-Onset Diabetes after Renal Transplantation. BMJ Open Diabetes Res. Care 2017, 5, e000283. [Google Scholar] [CrossRef] [Green Version]
- Nafar, M.; Noori, N.; Jalali-Farahani, S.; Hosseinpanah, F.; Poorrezagholi, F.; Ahmadpoor, P.; Samadian, F.; Firouzan, A.; Einollahi, B. Mediterranean Diets Are Associated with a Lower Incidence of Metabolic Syndrome One Year Following Renal Transplantation. Kidney Int. 2009, 76, 1199–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vučković, M.; Radić, J.; Gelemanović, A.; Raos, H.; Bučan Nenadić, D.; Kolak, E.; Radić, M. Mediterranean Diet Adherence and Nutritional Status in Dalmatian Kidney Transplant Recipients—Are They Related? Nutrients 2021, 13, 3246. [Google Scholar] [CrossRef]
- Monteagudo, C.; Mariscal-Arcas, M.; Rivas, A.; Lorenzo-Tovar, M.L.; Tur, J.A.; Olea-Serrano, F. Proposal of a Mediterranean Diet Serving Score. PLoS ONE 2015, 10, e0128594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kursa, M.B.; Rudnicki, W.R. Feature Selection with the Boruta Package. J. Stat. Softw. 2010, 36, 1–13. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://Www.R-Project.Org/ (accessed on 24 April 2020).
- Ronai, K.Z.; Szentkiralyi, A.; Lazar, A.S.; Ujszaszi, A.; Turanyi, C.; Gombos, F.; Mucsi, I.; Bodizs, R.; Molnar, M.Z.; Novak, M. Depressive Symptoms Are Associated With Objectively Measured Sleep Parameters in Kidney Transplant Recipients. J. Clin. Sleep Med. 2017, 13, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Marques, A.; Gomez-Baya, D.; Peralta, M.; Frasquilho, D.; Santos, T.; Martins, J.; Ferrari, G.; Gaspar de Matos, M. The Effect of Muscular Strength on Depression Symptoms in Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5674. [Google Scholar] [CrossRef]
- Kurita, N.; Wakita, T.; Fujimoto, S.; Yanagi, M.; Koitabashi, K.; Suzuki, T.; Yazawa, M.; Kawarazaki, H.; Shibagaki, Y.; Ishibashi, Y. Hopelessness and Depression Predict Sarcopenia in Advanced CKD and Dialysis: A Multicenter Cohort Study. J. Nutr. Health Aging 2021, 25, 593–599. [Google Scholar] [CrossRef]
- Shelton, R.C.; Miller, A.H. Eating Ourselves to Death (and Despair): The Contribution of Adiposity and Inflammation to Depression. Prog. Neurobiol. 2010, 91, 275–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelton, R.C.; Miller, A.H. Inflammation in Depression: Is Adiposity a Cause? Dialogues Clin. Neurosci. 2011, 13, 41–53. [Google Scholar] [CrossRef]
- Nöhre, M.; Schieffer, E.; Hanke, A.; Pape, L.; Schiffer, L.; Schiffer, M.; de Zwaan, M. Obesity After Kidney Transplantation—Results of a KTx360° Substudy. Front. Psychiatry 2020, 11, 399. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Micek, A.; Marventano, S.; Castellano, S.; Mistretta, A.; Pajak, A.; Galvano, F. Dietary N-3 PUFA, Fish Consumption and Depression: A Systematic Review and Meta-Analysis of Observational Studies. J. Affect. Disord. 2016, 205, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Álvarez-Pérez, J.; Toledo, E.; Salas-Salvadó, J.; Ortega-Azorín, C.; Zomeño, M.; Vioque, J.; Martínez, J.; Romaguera, D.; Pérez-López, J.; et al. Seafood Consumption, Omega-3 Fatty Acids Intake, and Life-Time Prevalence of Depression in the PREDIMED-Plus Trial. Nutrients 2018, 10, 2000. [Google Scholar] [CrossRef] [Green Version]
- Yun, H.; Kim, D.-W.; Lee, E.-J.; Jung, J.; Yoo, S. Analysis of the Effects of Nutrient Intake and Dietary Habits on Depression in Korean Adults. Nutrients 2021, 13, 1360. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, S.; Keshteli, A.H.; Saneei, P.; Afshar, H.; Esmaillzadeh, A.; Adibi, P. Red and White Meat Intake in Relation to Mental Disorders in Iranian Adults. Front. Nutr. 2021, 8, 710555. [Google Scholar] [CrossRef]
- Dobersek, U.; Wy, G.; Adkins, J.; Altmeyer, S.; Krout, K.; Lavie, C.J.; Archer, E. Meat and Mental Health: A Systematic Review of Meat Abstention and Depression, Anxiety, and Related Phenomena. Crit. Rev. Food Sci. Nutr. 2021, 61, 622–635. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.-S.; Chao, H.-H.; Huang, W.-T.; Chen, S.C.-C.; Yang, H.-Y. Psychiatric Disorders Risk in Patients with Iron Deficiency Anemia and Association with Iron Supplementation Medications: A Nationwide Database Analysis. BMC Psychiatry 2020, 20, 216. [Google Scholar] [CrossRef]
- Jia, Q.; Yang, H.; Zhuang, N.; Yin, X.; Zhu, Z.; Yuan, Y.; Yin, X.; Wang, Y.; Cheung, E.F.C.; Chan, R.C.K.; et al. The Role of Lipoprotein Profile in Depression and Cognitive Performance: A Network Analysis. Sci. Rep. 2020, 10, 20704. [Google Scholar] [CrossRef]
- Fardeazar, F.E.; Solhi, M.; Soola, A.H.; Amani, F. Depressive Symptoms and Associated Factors among Kidney Transplant Recipients. Electron. J. Gen. Med. 2018, 15. [Google Scholar] [CrossRef]
- Speed, M.S.; Jefsen, O.H.; Børglum, A.D.; Speed, D.; Østergaard, S.D. Investigating the Association between Body Fat and Depression via Mendelian Randomization. Transl. Psychiatry 2019, 9, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.R.; Jung, S.M.; Bang, H.; Kim, H.S.; Kim, Y.B. The Association between Muscular Strength and Depression in Korean Adults: A Cross-Sectional Analysis of the Sixth Korea National Health and Nutrition Examination Survey (KNHANES VI) 2014 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Public Health 2018, 18, 1123. [Google Scholar] [CrossRef] [Green Version]
- Ponticelli, C.; Favi, E. Physical Inactivity: A Modifiable Risk Factor for Morbidity and Mortality in Kidney Transplantation. J. Pers. Med. 2021, 11, 927. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Total (N = 115) | No Depression (N = 90) | Depression (N = 25) | p * | |
|---|---|---|---|---|
| BDI-II score, median (IQR) | 8 (10) | 6 (7) | 18 (11) | <0.001 |
| Age (years), median (IQR) | 60 (16) | 60 (16) | 67 (12) | 0.011 |
| Sex, N (%) | ||||
| Women | 54 (46.96) | 41 (45.56) | 13 (52) | 0.730 |
| Men | 61 (53.04) | 49 (54.44) | 12 (48) | |
| Time since transplantation (years), median (IQR) | 5 (7) | 5 (6.88) | 7 (8.25) | 0.190 |
| Dialysis duration (years), median (IQR) | 2 (3.5) | 2 (3) | 4 (4) | 0.080 |
| Dialysis type, N (%) | ||||
| PD | 38 (33.63) | 31 (35.23) | 7 (28) | 0.565 |
| HD | 67 (59.29) | 50 (56.82) | 17 (68) | |
| PD + HD | 8 (7.08) | 7 (7.95) | 1 (4) | |
| Smoking status, N (%) | ||||
| Smoker | 52 (50.98) | 40 (51.28) | 12 (50) | 0.874 |
| Former smoker | 26 (25.49) | 19 (24.36) | 7 (29.17) | |
| Non-smoker | 24 (23.53) | 19 (24.36) | 5 (20.83) | |
| COMORBIDITIES | ||||
| Presence of arterial hypertension, N (%) | ||||
| No | 16 (13.91) | 12 (13.33) | 4 (16) | 0.989 |
| Yes | 99 (86.09) | 78 (86.67) | 21 (84) | |
| Presence of diabetes mellitus, N (%) | ||||
| No | 89 (77.39) | 71 (78.89) | 18 (72) | 0.647 |
| Yes | 26 (22.61) | 19 (21.11) | 7 (28) | |
| Presence of chronic kidney disease, N (%) | ||||
| eGFR > 60 mL/min/1.73 m2 | 31 (28.44) | 23 (26.74) | 8 (34.78) | 0.618 |
| eGFR < 60 mL/min/1.73 m2 | 78 (71.56) | 63 (73.26) | 15 (65.22) | |
| ANTHROPOMETRIC PARAMETERS | ||||
| Height (cm), mean (SD) | 172.68 (10.06) | 173.1 (10.27) | 171.2 (9.35) | 0.407 |
| Weight (kg), median (IQR) | 78.51 (14.69) | 79.16 (14.63) | 76.21 (14.94) | 0.378 |
| BMI (kg/m2), mean (SD) | 26.21 (4.1) | 26.26 (4) | 26.06 (4.51) | 0.836 |
| Middle upper arm circumference (cm), median (IQR) | 29 (7) | 28.5 (7) | 30 (7.75) | 0.888 |
| Waist circumference (cm), mean (SD) | 99.2 (12.54) | 99.12 (12.51) | 99.5 (12.95) | 0.901 |
| WHtR, mean (SD) | 0.58 (0.07) | 0.57 (0.07) | 0.59 (0.08) | 0.417 |
| Handgrip strength (pounds) | 40 (19) | 42 (16.7) | 34 (19.5) | 0.134 |
| LABORATORY PARAMETERS | ||||
| Alb (g/L), median (IQR) | 42 (4) | 42 (4.5) | 41 (5) | 0.082 |
| Ca (mmol/L), median (IQR) | 2.44 (0.18) | 2.42 (0.2) | 2.47 (0.11) | 0.204 |
| CRP (mg/L), median (IQR) | 2.4 (4.38) | 2.4 (4.3) | 3.3 (4.6) | 0.939 |
| E, median (IQR) | 4.65 (0.68) | 4.61 (0.64) | 4.77 (0.77) | 0.485 |
| GUP (mmol/L), median (IQR) | 5.2 (1.1) | 5.2 (1) | 5.2 (1.2) | 0.632 |
| Hb (g/L), median (IQR) | 134 (18) | 135 (19.5) | 133 (7.5) | 0.537 |
| K (mmol/L), mean (SD) | 4.13 (0.47) | 4.16 (0.47) | 4.01 (0.49) | 0.180 |
| Total cholesterol (mmol/L), mean (SD) | 5.98 (1.31) | 5.97 (1.26) | 6.04 (1.51) | 0.824 |
| Creatinine (mmol/L), median (IQR) | 122 (55) | 121 (54.5) | 128 (57.5) | 0.595 |
| LDL (mmol/L), median (IQR) | 3.62 (1.09) | 3.63 (1.07) | 3.58 (1.19) | 0.866 |
| MCV (fL), mean (SD) | 87.67 (5.5) | 88.29 (5.44) | 85.38 (5.21) | 0.024 |
| Na (mmol/L), median (IQR) | 141 (3) | 141 (2.75) | 141 (2.5) | 0.342 |
| P (mmol/L), median (IQR) | 1.02 (0.23) | 1.02 (0.23) | 1.02 (0.27) | 0.323 |
| Tgl (mmol/L), median (IQR) | 1.85 (1.48) | 1.9 (1.45) | 1.7 (1.4) | 0.685 |
| Uric acid (mmol/L), median (IQR) | 392 (74.25) | 391 (62) | 394 (113) | 0.977 |
| Urea (mmol/L), median (IQR) | 9.5 (4.78) | 9.3 (4.33) | 10.7 (7.67) | 0.469 |
| eGFR (ml/min/1.73 m2), median (IQR) | 46.6 (26.6) | 47.2 (22.85) | 45.9 (33.35) | 0.859 |
| BODY COMPOSITION | ||||
| Fat mass (kg), median (IQR) | 19.15 (10.57) | 19.05 (10.25) | 21.2 (10.1) | 0.230 |
| Fat mass (%), mean (SD) | 23.68 (8.55) | 23.04 (8.36) | 25.94 (9.02) | 0.143 |
| Fat-free mass (kg), median (IQR) | 59.3 (17.48) | 59.45 (17.2) | 54.9 (16.2) | 0.107 |
| Visceral fat, mean (SD) | 9.17 (3.79) | 8.83 (3.85) | 10.43 (3.31) | 0.070 |
| Muscle mass (kg), median (IQR) | 56.3 (17.05) | 56.45 (17.38) | 52.15 (15.48) | 0.113 |
| Skeletal muscle mass (kg), median (IQR) | 31.25 (11.77) | 32.1 (12.07) | 28.25 (9.25) | 0.042 |
| Skeletal muscle mass (%), median (IQR) | 40.9 (7.93) | 42.3 (8.55) | 38.4 (5.73) | 0.012 |
| Body mass (kg), median (IQR) | 3 (0.8) | 3 (0.77) | 2.75 (0.73) | 0.079 |
| Phase angle, median (IQR) | 5.15 (1.17) | 5.2 (1.07) | 4.85 (0.98) | 0.178 |
| Trunk visceral fat (kg), median (IQR) | 10.2 (6.5) | 9.9 (7.28) | 10.6 (5.25) | 0.212 |
| Mediterranean Diet Serving Score (MDSS) | ||||
| Total MDSS points, mean (SD) | 10.45 (4.27) | 10.78 (4.35) | 9.26 (3.84) | 0.131 |
| Adherence to MeDi, N (%) | ||||
| MDSS < 14 points | 79 (74.53) | 59 (71.08) | 20 (86.96) | 0.202 |
| MDSS ≥ 14 points | 27 (25.47) | 24 (28.92) | 3 (13.04) | |
| Parameter | R | p * |
|---|---|---|
| Handgrip strength | −0.285 | 0.005 |
| Skeletal muscle mass (%) | −0.278 | 0.003 |
| MCV (fL) | −0.201 | 0.038 |
| Hb (mmol/L) | −0.196 | 0.041 |
| Olive oil (adherence) | 0.189 | 0.049 |
| Age (years) | 0.210 | 0.024 |
| Fat mass (%) | 0.240 | 0.012 |
| Predictor | OR | 95% CI | p | Nagelkerke R2 |
|---|---|---|---|---|
| Weight (kg) | 1.08 | 1.01–1.16 | 0.033 | 0.16 |
| Waist circumference (cm) | 1.09 | 1.01–1.19 | 0.034 | 0.20 |
| Fat mass (%) | 1.12 | 1.01–1.24 | 0.038 | 0.13 |
| Fat mass (kg) | 1.15 | 1.02–1.30 | 0.022 | 0.18 |
| BMI (kg/m2) | 1.29 | 1.03–1.63 | 0.030 | 0.16 |
| Trunk visceral fat | 1.29 | 1.04–1.60 | 0.019 | 0.19 |
| Middle upper arm circumference (cm) | 1.38 | 1.05–1.80 | 0.019 | 0.26 |
| Tgl (mmol/L) | 5.83 | 1.02–33.48 | 0.048 | 0.32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vučković, M.; Radić, J.; Gelemanović, A.; Bučan Nenadić, D.; Kolak, E.; Radić, M. Associations between Depression, Nutritional Status and Mediterranean Diet in Dalmatian Kidney Transplant Recipients. Nutrients 2021, 13, 4479. https://doi.org/10.3390/nu13124479
Vučković M, Radić J, Gelemanović A, Bučan Nenadić D, Kolak E, Radić M. Associations between Depression, Nutritional Status and Mediterranean Diet in Dalmatian Kidney Transplant Recipients. Nutrients. 2021; 13(12):4479. https://doi.org/10.3390/nu13124479
Chicago/Turabian StyleVučković, Marijana, Josipa Radić, Andrea Gelemanović, Dora Bučan Nenadić, Ela Kolak, and Mislav Radić. 2021. "Associations between Depression, Nutritional Status and Mediterranean Diet in Dalmatian Kidney Transplant Recipients" Nutrients 13, no. 12: 4479. https://doi.org/10.3390/nu13124479
APA StyleVučković, M., Radić, J., Gelemanović, A., Bučan Nenadić, D., Kolak, E., & Radić, M. (2021). Associations between Depression, Nutritional Status and Mediterranean Diet in Dalmatian Kidney Transplant Recipients. Nutrients, 13(12), 4479. https://doi.org/10.3390/nu13124479