
Body Fat Percentage and Availability of Oral Food Intake: Prognostic Factors and Implications for Nutrition in Amyotrophic Lateral Sclerosis

 , ,
, ,  and
and
Abstract
:1. Introduction
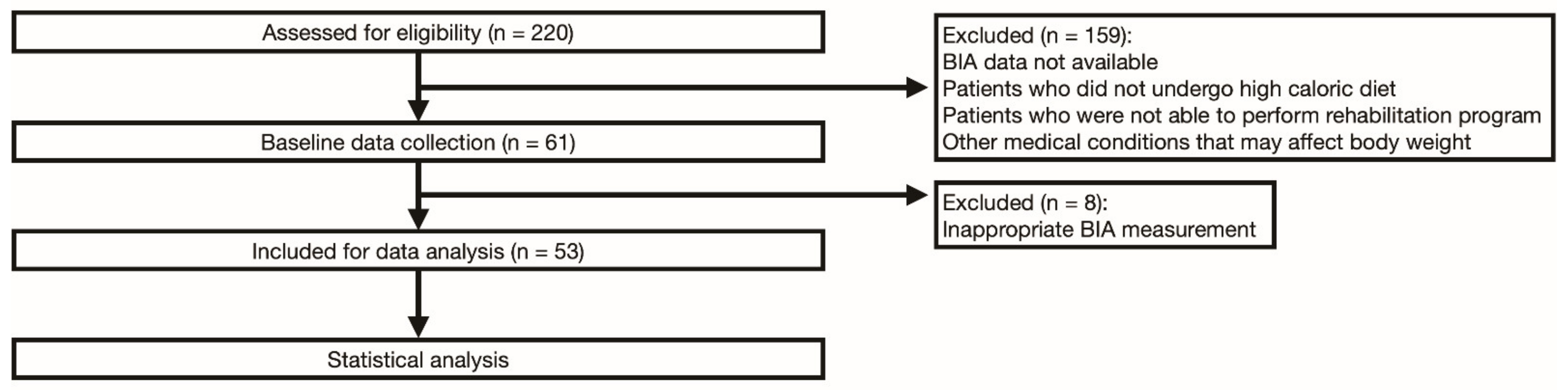
2. Materials and Methods
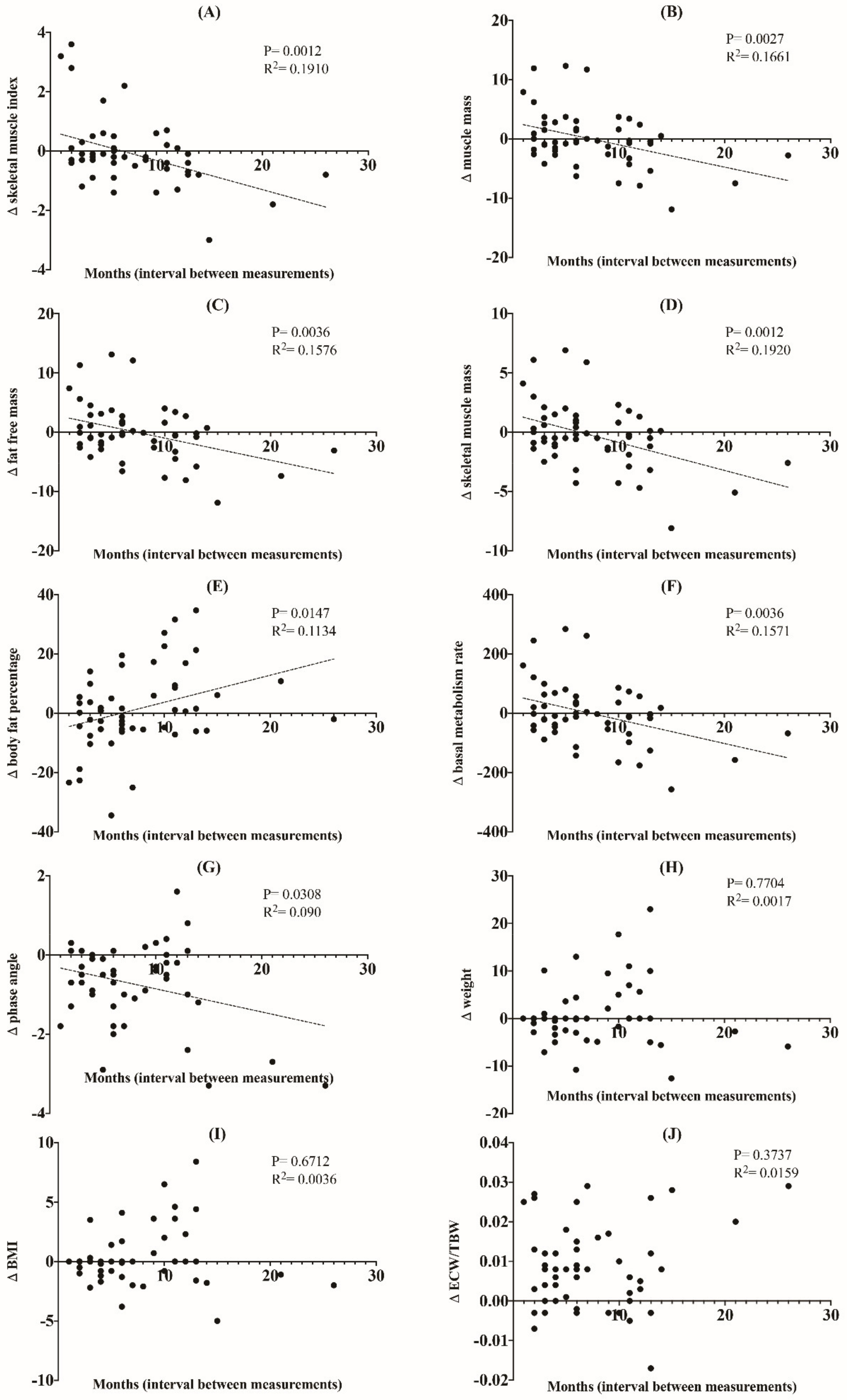
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kiernan, M.C.; Vucic, S.; Cheah, B.C.; Turner, M.R.; Eisen, A.; Hardiman, O.; Burrell, J.R.; Zoing, M.C. Amyotrophic lateral sclerosis. Lancet 2011, 377, 942–955. [Google Scholar] [CrossRef] [Green Version]
- Hardiman, O.; Al-Chalabi, A.; Chio, A.; Corr, E.M.; Logroscino, G.; Robberecht, W.; Shaw, P.J.; Simmons, Z.; van den Berg, L.H. Amyotrophic lateral sclerosis. Nat. Rev. Dis. Primers 2017, 3, 17071. [Google Scholar] [CrossRef]
- Tae, W.S.; Sung, J.H.; Baek, S.H.; Lee, C.N.; Kim, B.J. Shape analysis of the subcortical nuclei in amyotrophic lateral sclerosis without cognitive impairment. J. Clin. Neurol. 2020, 16, 592–598. [Google Scholar] [CrossRef]
- Cozza, F.; Lizio, A.; Greco, L.C.; Bona, S.; Donvito, G.; Carraro, E.; Tavazzi, S.; Ticozzi, N.; Poletti, B.; Sansone, V.A.; et al. Ocular involvement occurs frequently at all stages of amyotrophic lateral sclerosis: Preliminary experience in a large Italian cohort. J. Clin. Neurol. 2021, 17, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Lyon, M.S.; Wosiski-Kuhn, M.; Gillespie, R.; Caress, J.; Milligan, C. Inflammation, immunity, and amyotrophic lateral sclerosis: I. Etiology and pathology. Muscle Nerve 2019, 59, 10–22. [Google Scholar] [CrossRef] [Green Version]
- Ludolph, A.C.; Dorst, J.; Dreyhaupt, J.; Weishaupt, J.H.; Kassubek, J.; Weiland, U.; Meyer, T.; Petri, S.; Hermann, A.; Emmer, A.; et al. Effect of high-caloric nutrition on survival in amyotrophic lateral sclerosis. Ann. Neurol. 2020, 87, 206–216. [Google Scholar] [CrossRef]
- Marin, B.; Desport, J.C.; Kajeu, P.; Jesus, P.; Nicolaud, B.; Nicol, M.; Preux, P.M.; Couratier, P. Alteration of nutritional status at diagnosis is a prognostic factor for survival of amyotrophic lateral sclerosis patients. J. Neurol. Neurosurg. Psychiatry 2011, 82, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Paganoni, S.; Deng, J.; Jaffa, M.; Cudkowicz, M.E.; Wills, A.M. Body mass index, not dyslipidemia, is an independent predictor of survival in amyotrophic lateral sclerosis. Muscle Nerve 2011, 44, 20–24. [Google Scholar] [CrossRef] [Green Version]
- Roubeau, V.; Blasco, H.; Maillot, F.; Corcia, P.; Praline, J. Nutritional assessment of amyotrophic lateral sclerosis in routine practice: Value of weighing and bioelectrical impedance analysis. Muscle Nerve 2015, 51, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Diverse Populations Collaborative Group. Weight-height relationships and body mass index: Some observations from the Diverse Populations Collaboration. Am. J. Phys. Anthropol. 2005, 128, 220–229. [Google Scholar] [CrossRef]
- Deurenberg-Yap, M.; Schmidt, G.; van Staveren, W.A.; Deurenberg, P. The paradox of low body mass index and high body fat percentage among Chinese, Malays and Indians in Singapore. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1011–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shimizu, T.; Nagaoka, U.; Nakayama, Y.; Kawata, A.; Kugimoto, C.; Kuroiwa, Y.; Kawai, M.; Shimohata, T.; Nishizawa, M.; Mihara, B.; et al. Reduction rate of body mass index predicts prognosis for survival in amyotrophic lateral sclerosis: A multicenter study in Japan. Amyotroph. Lateral Scler. 2012, 13, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Wills, A.M.; Hubbard, J.; Macklin, E.A.; Glass, J.; Tandan, R.; Simpson, E.P.; Brooks, B.; Gelinas, D.; Mitsumoto, H.; Mozaffar, T.; et al. Hypercaloric enteral nutrition in patients with amyotrophic lateral sclerosis: A randomised, double-blind, placebo-controlled phase 2 trial. Lancet 2014, 383, 2065–2072. [Google Scholar] [CrossRef] [Green Version]
- Ludolph, A.; Drory, V.; Hardiman, O.; Nakano, I.; Ravits, J.; Robberecht, W.; Shefner, J. A revision of the El Escorial criteria. Amyotroph. Lateral Scler. Front. Degener. 2015, 16, 291–292. [Google Scholar] [CrossRef]
- Jeon, K.C.; Kim, S.Y.; Jiang, F.L.; Chung, S.; Ambegaonkar, J.P.; Park, J.H.; Kim, Y.J.; Kim, C.H. Prediction equations of the multifrequency standing and supine bioimpedance for appendicular skeletal muscle mass in Korean older people. Int. J. Environ. Res. Public Health 2020, 17, 5847. [Google Scholar] [CrossRef]
- Nishioka, S.; Yamanouchi, A.; Matsushita, T.; Nishioka, E.; Mori, N.; Taguchi, S. Validity of calf circumference for estimating skeletal muscle mass for Asian patients after stroke. Nutrition 2021, 82, 111028. [Google Scholar] [CrossRef]
- Thivel, D.; Verney, J.; Miguet, M.; Masurier, J.; Cardenoux, C.; Lambert, C.; Courteix, D.; Metz, L.; Pereira, B. The accuracy of bioelectrical impedance to track body composition changes depends on the degree of obesity in adolescents with obesity. Nutr. Res. 2018, 54, 60–68. [Google Scholar] [CrossRef]
- Fujimoto, K.; Inage, K.; Eguchi, Y.; Orita, S.; Suzuki, M.; Kubota, G.; Sainoh, T.; Sato, J.; Shiga, Y.; Abe, K.; et al. Use of bioelectrical impedance analysis for the measurement of appendicular skeletal muscle mass/whole fat mass and its relevance in assessing osteoporosis among patients with low back pain: A comparative analysis using dual x-ray absorptiometry. Asian Spine J. 2018, 12, 839–845. [Google Scholar] [CrossRef] [Green Version]
- Bojmehrani, A.; Bergeron-Duchesne, M.; Bouchard, C.; Simard, S.; Bouchard, P.A.; Vanderschuren, A.; L’Her, E.; Lellouche, F. Comparison of usual and alternative methods to measure height in mechanically ventilated patients: Potential impact on protective ventilation. Respir. Care 2014, 59, 1025–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.; Kazamel, M.; McPherson, T.; McAdam, J.; Bamman, M.; Amara, A.; Smith, D.L., Jr.; King, P.H. Fat mass loss correlates with faster disease progression in amyotrophic lateral sclerosis patients: Exploring the utility of dual-energy x-ray absorptiometry in a prospective study. PLoS ONE 2021, 16, e0251087. [Google Scholar] [CrossRef]
- Nakken, O.; Meyer, H.E.; Stigum, H.; Holmøy, T. High BMI is associated with low ALS risk: A population-based study. Neurology 2019, 93, e424–e432. [Google Scholar] [CrossRef]
- Dardiotis, E.; Siokas, V.; Sokratous, M.; Tsouris, Z.; Aloizou, A.M.; Florou, D.; Dastamani, M.; Mentis, A.A.; Brotis, A.G. Body mass index and survival from amyotrophic lateral sclerosis: A meta-analysis. Neurol. Clin. Pract. 2018, 8, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, Y.; Shimizu, T.; Matsuda, C.; Haraguchi, M.; Hayashi, K.; Bokuda, K.; Nagao, M.; Kawata, A.; Ishikawa-Takata, K.; Isozaki, E. Body weight variation predicts disease progression after invasive ventilation in amyotrophic lateral sclerosis. Sci. Rep. 2019, 9, 12262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ning, P.; Yang, B.; Li, S.; Mu, X.; Shen, Q.; Hu, F.; Tang, Y.; Yang, X.; Xu, Y. Systematic review of the prognostic role of body mass index in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Front. Degener. 2019, 20, 356–367. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Yamashita, T. The effects of leptin on glial cells in neurological diseases. Front. Neurosci. 2019, 13, 828. [Google Scholar] [CrossRef]
- Zhang, W.; Jin, Y.; Wang, D.; Cui, J. Neuroprotective effects of leptin on cerebral ischemia through JAK2/STAT3/PGC-1-mediated mitochondrial function modulation. Brain Res. Bull. 2020, 156, 118–130. [Google Scholar] [CrossRef]
- Feng, E.; Jiang, L. Peptidomic analysis of hippocampal tissue for explore leptin neuroprotective effect on the preterm ischemia-hypoxia brain damage model rats. Neuropharmacology 2020, 162, 107803. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.J.; Li, G.M.; Nie, B.M.; Lu, Y.; Yin, M. Neuroprotective effect of the stearic acid against oxidative stress via phosphatidylinositol 3-kinase pathway. Chem. Biol. Interact. 2006, 160, 80–87. [Google Scholar] [CrossRef]
- Fressinaud, C.; Vallat, J.M.; Rigaud, M.; Leboutet, M.J. Analysis of unsaturated fatty acids of endoneurium and perineurium from normal and degenerating rat sciatic nerve. Morphological correlations. J. Neurol. Sci. 1987, 81, 85–92. [Google Scholar] [CrossRef]
- Bourre, J.M.; Dumont, O.; Piciotti, M.; Pascal, G.; Durand, G. Control of brain fatty acids. Upsala J. Med. Sci. Suppl. 1990, 48, 109–131. [Google Scholar]
- Beeharry, N.; Lowe, J.E.; Hernandez, A.R.; Chambers, J.A.; Fucassi, F.; Cragg, P.J.; Green, M.H.; Green, I.C. Linoleic acid and antioxidants protect against DNA damage and apoptosis induced by palmitic acid. Mutat. Res. 2003, 530, 27–33. [Google Scholar] [CrossRef]
- Yang, J.W.; Kim, S.M.; Kim, H.J.; Kim, J.E.; Park, K.S.; Kim, S.H.; Lee, K.W.; Sung, J.J. Hypolipidemia in patients with amyotrophic lateral sclerosis: A possible gender difference? J. Clin. Neurol. 2013, 9, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Pape, J.A.; Grose, J.H. The effects of diet and sex in amyotrophic lateral sclerosis. Rev. Neurol. 2020, 176, 301–315. [Google Scholar] [CrossRef]
- Baek, S.H.; Kim, J.S.; Jang, M.J.; Kim, Y.H.; Kwon, O.; Oh, J.H.; Kang, S.Y.; Kang, J.H.; Park, K.H.; Park, Y.S.; et al. Low body mass index can be associated with the risk and poor outcomes of neuromyelitis optica with aquaporin-4 immunoglobulin G in women. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1228–1230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, R.; Yoo, D.; Jung, Y.J.; Han, K.; Lee, J.Y. Smoking cessation, weight change, and risk of Parkinson’s disease: Analysis of national cohort data. J. Clin. Neurol. 2020, 16, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Kasarskis, E.J.; Berryman, S.; Vanderleest, J.G.; Schneider, A.R.; McClain, C.J. Nutritional status of patients with amyotrophic lateral sclerosis: Relation to the proximity of death. Am. J. Clin. Nutr. 1996, 63, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.; Park, J.; Kim, Y.; Baek, H.; Kim, S.H. Association between nutritional status and disease severity using the amyotrophic lateral sclerosis (ALS) functional rating scale in ALS patients. Nutrition 2015, 31, 1362–1367. [Google Scholar] [CrossRef]
- Pupillo, E.; Bianchi, E.; Chiò, A.; Casale, F.; Zecca, C.; Tortelli, R.; Beghi, E. Amyotrophic lateral sclerosis and food intake. Amyotroph. Lateral. Scler. Front. Degener. 2018, 19, 267–274. [Google Scholar] [CrossRef]
- Okamoto, K.; Kihira, T.; Kondo, T.; Kobashi, G.; Washio, M.; Sasaki, S.; Yokoyama, T.; Miyake, Y.; Sakamoto, N.; Inaba, Y.; et al. Nutritional status and risk of amyotrophic lateral sclerosis in Japan. Amyotroph. Lateral. Scler. 2007, 8, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Marra, M.; Sammarco, R.; De Lorenzo, A.; Iellamo, F.; Siervo, M.; Pietrobelli, A.; Donini, L.M.; Santarpia, L.; Cataldi, M.; Pasanisi, F.; et al. Assessment of body composition in health and disease using bioelectrical impedance analysis (BIA) and dual energy x-ray absorptiometry (DXA): A critical overview. Contrast Media Mol. Imaging 2019, 2019, 3548284. [Google Scholar] [CrossRef]
- Buckinx, F.; Reginster, J.Y.; Dardenne, N.; Croisiser, J.L.; Kaux, J.F.; Beaudart, C.; Slomian, J.; Bruyère, O. Concordance between muscle mass assessed by bioelectrical impedance analysis and by dual energy X-ray absorptiometry: A cross-sectional study. BMC Musculoskelet. Disord. 2015, 16, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fang, W.H.; Yang, J.R.; Lin, C.Y.; Hsiao, P.J.; Tu, M.Y.; Chen, C.F.; Tsai, D.J.; Su, W.; Huang, G.S.; Chang, H.; et al. Accuracy augmentation of body composition measurement by bioelectrical impedance analyzer in elderly population. Medicine 2020, 99, e19103. [Google Scholar] [CrossRef]
- Desport, J.C.; Preux, P.M.; Bouteloup-Demange, C.; Clavelou, P.; Beaufrère, B.; Bonnet, C.; Couratier, P.P. Validation of bioelectrical impedance analysis in patients with amyotrophic lateral sclerosis. Am. J. Clin. Nutr. 2003, 77, 1179–1185. [Google Scholar] [CrossRef] [Green Version]
- Desport, J.C.; Marin, B.; Funalot, B.; Preux, P.M.; Couratier, P. Phase angle is a prognostic factor for survival in amyotrophic lateral sclerosis. Amyotroph. Lateral. Scler. 2008, 9, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S.; Ando, K.; Kobayashi, K.; Nakashima, H.; Seki, T.; Ishizuka, S.; Machino, M.; Morozumi, M.; Kanbara, S.; Ito, S.; et al. Higher extracellular water-to-total body water ratio more strongly reflects the locomotive syndrome risk and frailty than sarcopenia. Arch. Gerontol. Geriatr. 2020, 88, 104042. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variables | HR | 95% CI | p-Value |
|---|---|---|---|
| Univariate Analysis | |||
| Age | 1.047 | 0.997–1.099 | NS |
| Gender | 0.743 | 0.33–1.67 | NS |
| ∆ Body fat percentage/duration (months) | 0.418 | 0.188–0.929 | 0.0323 * |
| Availability of oral food intake | 0.228 | 0.053–0.975 | 0.0461 * |
| ∆ Phase angle/duration (months) | 0.429 | 0.194–0.952 | 0.0374 * |
| ∆ ECW/TBW/duration (months) | 2.871 | 1.261–6.535 | 0.012 * |
| ∆ Skeletal muscle index/duration (months) | 1.31 | 0.601–2.855 | NS |
| ∆ Muscle mass/duration (months) | 1.763 | 0.808–3.846 | NS |
| ∆ Fat-free mass/duration (months) | 1.448 | 0.667–3.146 | NS |
| ∆ Skeletal muscle mass/duration (months) | 2.042 | 0.925–4.509 | NS |
| ∆ Basal metabolism rate/duration (months) | 1.679 | 0.771–3.659 | NS |
| ∆ Weight/duration (months) | 1.635 | 0.686–3.896 | NS |
| ∆ BMI/duration (months) | 1.635 | 0.686–3.896 | NS |
| Presence of tracheostomy | 1.133 | 0.464–2.764 | NS |
| Multivariate Analysis | |||
| ∆ Body fat percentage/duration (months) | 0.374 | 0.158–0.882 | 0.0247 * |
| Availability of oral food intake | 0.167 | 0.037–0.755 | 0.02 * |
| ∆ Phase angle/duration (months) | 1.215 | 0.177–8.344 | NS |
| ∆ ECW/TBW/duration (months) | 3.03 | 0.429–21.384 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-W.; Kim, M.; Baek, S.-H.; Sung, J.H.; Yu, J.-G.; Kim, B.-J. Body Fat Percentage and Availability of Oral Food Intake: Prognostic Factors and Implications for Nutrition in Amyotrophic Lateral Sclerosis. Nutrients 2021, 13, 3704. https://doi.org/10.3390/nu13113704
Park J-W, Kim M, Baek S-H, Sung JH, Yu J-G, Kim B-J. Body Fat Percentage and Availability of Oral Food Intake: Prognostic Factors and Implications for Nutrition in Amyotrophic Lateral Sclerosis. Nutrients. 2021; 13(11):3704. https://doi.org/10.3390/nu13113704
Chicago/Turabian StylePark, Jin-Woo, Minseok Kim, Seol-Hee Baek, Joo Hye Sung, Jae-Guk Yu, and Byung-Jo Kim. 2021. "Body Fat Percentage and Availability of Oral Food Intake: Prognostic Factors and Implications for Nutrition in Amyotrophic Lateral Sclerosis" Nutrients 13, no. 11: 3704. https://doi.org/10.3390/nu13113704
APA StylePark, J.-W., Kim, M., Baek, S.-H., Sung, J. H., Yu, J.-G., & Kim, B.-J. (2021). Body Fat Percentage and Availability of Oral Food Intake: Prognostic Factors and Implications for Nutrition in Amyotrophic Lateral Sclerosis. Nutrients, 13(11), 3704. https://doi.org/10.3390/nu13113704