
Effects of Caffeine Ingestion on Human Standing Balance: A Systematic Review of Placebo-Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources, Search Strategy and Selection Process
2.3. Study Quality and Risk of Bias Assessment
2.4. Data Collection and Synthesis
3. Results
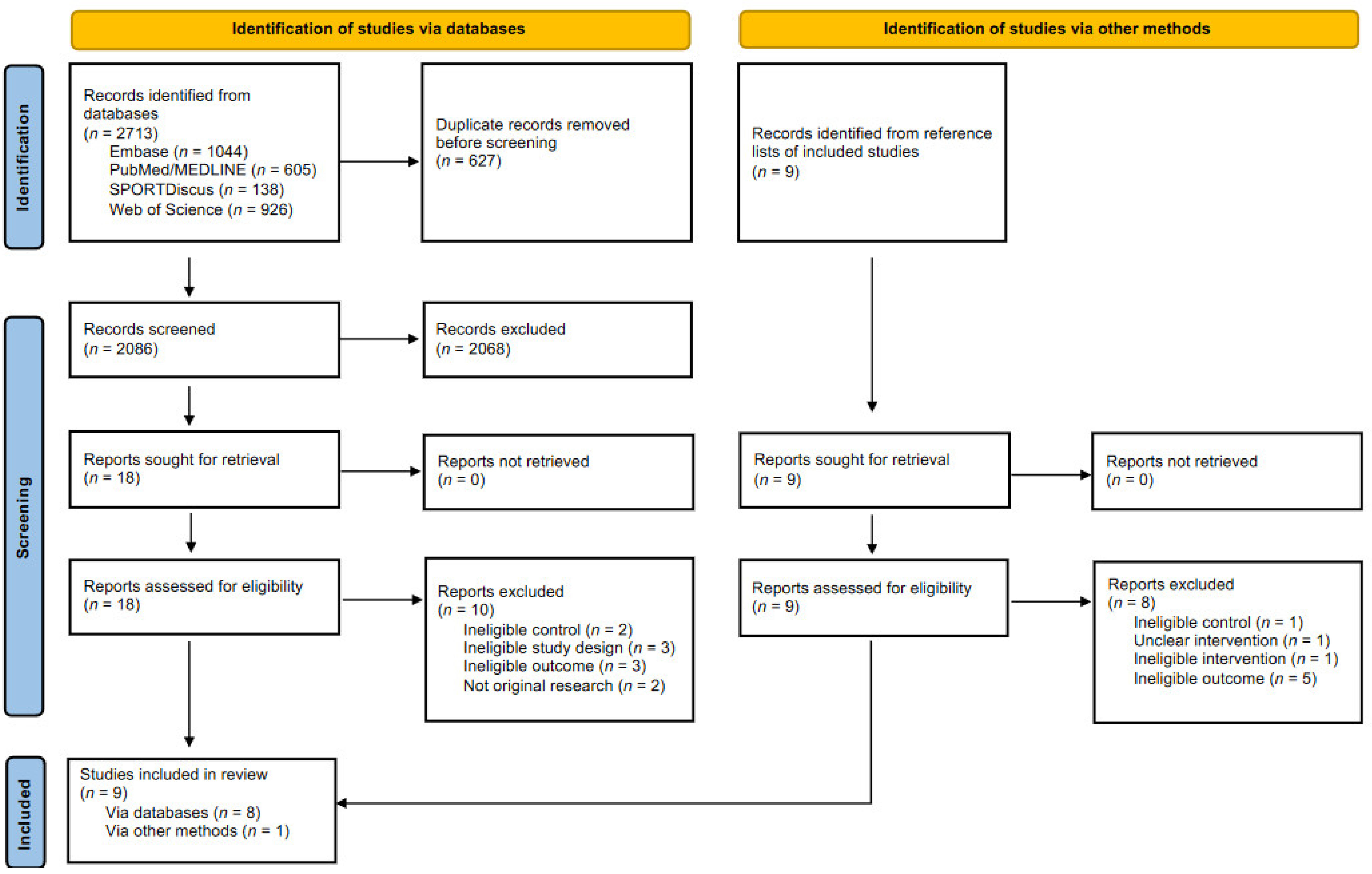
3.1. Study Selection
3.2. Study Quality, Risk of Bias and Characteristics
3.2.1. Younger
3.2.2. Older
3.3. Study Findings
3.3.1. Younger
3.3.2. Older
4. Discussion
4.1. Age-Dependent Effect of Caffeine Ingestion on Human Standing Balance
4.2. Possible Caffeine-Induced Balance Enhancement in Specific Conditions
4.3. Limitations and Future Research
4.4. Implications for Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Registration and Protocol
References
- Fredholm, B.B.; Bättig, K.; Holmén, J.; Nehlig, A.; Zvartau, E.E. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol. Rev. 1999, 51, 83–133. [Google Scholar] [PubMed]
- Abd, E.; Benson, H.A.; Roberts, M.; Grice, J.E. Follicular Penetration of Caffeine from Topically Applied Nanoemulsion Formulations Containing Penetration Enhancers: In vitro Human Skin Studies. Skin Pharmacol. Physiol. 2018, 31, 252–260. [Google Scholar] [CrossRef]
- McCall, A.; Millington, W.; Wurtman, R. Blood-brain barrier transport of caffeine: Dose-related restriction of adenine transport. Life Sci. 1982, 31, 2709–2715. [Google Scholar] [CrossRef]
- Fong, C.W. Permeability of the Blood–Brain Barrier: Molecular Mechanism of Transport of Drugs and Physiologically Important Compounds. J. Membr. Biol. 2015, 248, 651–669. [Google Scholar] [CrossRef]
- Spriet, L.L. Exercise and Sport Performance with Low Doses of Caffeine. Sports Med. 2014, 44, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Nehlig, A.; Daval, J.-L.; DeBry, G. Caffeine and the central nervous system: Mechanisms of action, biochemical, metabolic and psychostimulant effects. Brain Res. Rev. 1992, 17, 139–170. [Google Scholar] [CrossRef]
- Garrett, B.E.; Griffiths, R.R. The Role of Dopamine in the Behavioral Effects of Caffeine in Animals and Humans. Pharmacol. Biochem. Behav. 1997, 57, 533–541. [Google Scholar] [CrossRef]
- Tallis, J.; Duncan, M.J.; James, R.S. What can isolated skeletal muscle experiments tell us about the effects of caffeine on exercise performance? Br. J. Pharmacol. 2015, 172, 3703–3713. [Google Scholar] [CrossRef] [Green Version]
- McLellan, T.M.; Caldwell, J.A.; Lieberman, H.R. A review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci. Biobehav. Rev. 2016, 71, 294–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, J.V.; Horak, F.B. Cortical control of postural responses. J. Neural Transm. 2007, 114, 1339–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maki, B.E.; McIlroy, W.E. Cognitive demands and cortical control of human balance-recovery reactions. J. Neural Transm. 2007, 114, 1279–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warren, G.L.; Park, N.D.; Maresca, R.D.; Mckibans, K.I.; Millard-Stafford, M.L. Effect of Caffeine Ingestion on Muscular Strength and Endurance: A meta-analysis. Med. Sci. Sports Exerc. 2010, 42, 1375–1387. [Google Scholar] [CrossRef]
- Nehlig, A. Is Caffeine a Cognitive Enhancer? J. Alzheimer's Dis. 2010, 20, S85–S94. [Google Scholar] [CrossRef] [Green Version]
- Chapman, R.F.; Mickleborough, T.D. The Effects of Caffeine on Ventilation and Pulmonary Function During Exercise: An Often-Overlooked Response. Physician Sportsmed. 2009, 37, 97–103. [Google Scholar] [CrossRef]
- Lord, S.R.; Sherrington, C.; Menz, H.B.; Close, J.C.T. Falls in Older People, 2nd ed.; Cambridge University Press: Cambridge, UK, 2007; ISBN 9780511722233. [Google Scholar]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35, ii7–ii11. [Google Scholar] [CrossRef] [Green Version]
- Ozdemir, R.A.; Contreras-Vidal, J.L.; Paloski, W.H. Cortical control of upright stance in elderly. Mech. Ageing Dev. 2018, 169, 19–31. [Google Scholar] [CrossRef]
- Tallis, J.; James, R.; Cox, V.; Duncan, M. Is the ergogenicity of caffeine affected by increasing age? The direct effect of a physiological concentration of caffeine on the power output of maximally stimulated edl and diaphragm muscle isolated from the mouse. J. Nutr. Health Aging 2017, 21, 440–448. [Google Scholar] [CrossRef]
- Rees, K.; Allen, D.; Lader, M. The influences of age and caffeine on psychomotor and cognitive function. Psychopharmacology 1999, 145, 181–188. [Google Scholar] [CrossRef]
- Polasek, T.M.; Patel, F.; Jensen, B.P.; Sorich, M.J.; Wiese, M.D.; Doogue, M.P. Predicted metabolic drug clearance with increasing adult age. Br. J. Clin. Pharmacol. 2013, 75, 1019–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seashore, R.H.; Ivy, A.C. The effects of analeptic drugs in relieving fatigue. Psychol. Monogr. Gen. Appl. 1953, 67, 1–16. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. HTA Initiative #13 Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research: Edmonton, AB, Canada, 2004. [Google Scholar]
- Franks, H.M.; Hagedorn, H.; Hensley, V.R.; Hensley, W.J.; Starmer, G.A. The effect of caffeine on human performance, alone and in combination with ethanol. Psychopharmacologia 1975, 45, 177–181. [Google Scholar] [CrossRef]
- Nuotto, E.; Mattila, M.J.; Seppälä, T.; Konno, K. Coffee and caffeine and alcohol effects on psychomotor function. Clin. Pharmacol. Ther. 1982, 31, 68–76. [Google Scholar] [CrossRef]
- Swift, C.G.; Tiplady, B. The effects of age on the response to caffeine. Psychopharmacology 1988, 94, 29–31. [Google Scholar] [CrossRef]
- Liguori, A.; Robinson, J.H. Caffeine antagonism of alcohol-induced driving impairment. Drug Alcohol Depend. 2001, 63, 123–129. [Google Scholar] [CrossRef]
- Norager, C.B.; Jensen, M.B.; Madsen, M.R.; Laurberg, S. Caffeine improves endurance in 75-yr-old citizens: A randomized, double-blind, placebo-controlled, crossover study. J. Appl. Physiol. 2005, 99, 2302–2306. [Google Scholar] [CrossRef] [PubMed]
- Momsen, A.H.; Jensen, M.B.; Norager, C.B.; Madsen, M.R.; Vestersgaard-Andersen, T.; Lindholt, J. Randomized double-blind placebo-controlled crossover study of caffeine in patients with intermittent claudication. BJS 2010, 97, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.B.; Norager, C.B.; Fenger-Grøn, M.; Weimann, A.; Moller, N.; Madsen, M.R.; Laurberg, S. Caffeine Supplementation Had No Effect on Endurance Capacity in Elderly Subjects Who Had Abstained from Caffeine-Containing Nutrition for 8 Hours. J. Caffeine Res. 2011, 1, 109–116. [Google Scholar] [CrossRef]
- Ben Waer, F.; Laatar, R.; Srihi, S.; Jouira, G.; Rebai, H.; Sahli, S. Acute effects of low versus high caffeine dose consumption on postural balance in middle-aged women. J. Women Aging 2020, 1–15. [Google Scholar] [CrossRef]
- Tallis, J.; Bradford, C.; Duncan, M.; Leddington-Wright, S.; Higgins, M.; Hill, M. The Effect of Acute Caffeine Ingestion on Cognitive Dual Task Performance during Assessment of Static and Dynamic Balance in Older Adults. Nutrients 2020, 12, 3653. [Google Scholar] [CrossRef]
- McNerney, K.M.; Coad, M.L.; Burkard, R.F. The Influence of Caffeine on the Sensory Organization Test. J. Am. Acad. Audiol. 2014, 25, 521–528. [Google Scholar] [CrossRef]
- Marczinski, C.A.; Fillmore, M.T.; Stamates, A.L.; Maloney, S.F. Alcohol-Induced Impairment of Balance is Antagonized by Energy Drinks. Alcohol. Clin. Exp. Res. 2018, 42, 144–152. [Google Scholar] [CrossRef] [Green Version]
- Kara, M.; Patlar, S.; Stoffregen, T.A.; Erkmen, N. Effect of caffeine on standing balance during perceptual-cognitive tasks. MoHE 2018, 7, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Zhou, B.; Lovegren, M. Effect of Oolong Tea on Balance Performance in Naive Tea Users—A Pilot Study. J. Exerc. Physiol. Online 2007, 10, 43–50. [Google Scholar]
- Enriquez, A.; Sklaar, J.; Viirre, E.; Chase, B. Effects of caffeine on postural stability. Int. Tinnitus J. 2009, 15, 161–163. [Google Scholar] [PubMed]
- Kim, W.S.; Choi, C.K.; Yoon, S.H.; Kwon, J.Y. Usual Dose of Caffeine Has a Positive Effect on Somatosensory Related Postural Stability in Hemiparetic Stroke Patients. Ann. Rehabilitation Med. 2014, 38, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Newman, H.W.; Newman, E.J. Failure of Dexedrine and Caffeine as Practical Antagonists of the Depressant Effect of Ethyl Alcohol in Man. Q. J. Stud. Alcohol 1956, 17, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Epapegaaij, S.; Etaube, W.; Ebaudry, S.; Eotten, E.; Ehortobágyi, T. Aging causes a reorganization of cortical and spinal control of posture. Front. Aging Neurosci. 2014, 6, 28. [Google Scholar] [CrossRef]
- Teasdale, N.; Bard, C.; LaRue, J.; Fleury, M. On the cognitive penetrability of posture control. Exp. Aging Res. 1993, 19, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.A.B.; Pereira, W.M.; Rossi, L.P.; Kerpers, I.I.; De Paula, A.R.; Oliveira, C. Analysis of electromyographic activity of ankle muscles on stable and unstable surfaces with eyes open and closed. J. Bodyw. Mov. Ther. 2011, 15, 496–501. [Google Scholar] [CrossRef]
- Pasma, J.; Engelhart, D.; Schouten, A.; van der Kooij, H.; Maier, A.; Meskers, C. Impaired standing balance: The clinical need for closing the loop. Neuroscience 2014, 267, 157–165. [Google Scholar] [CrossRef]
- Peterka, R.J. Sensorimotor Integration in Human Postural Control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Day, B.L.; Cole, J. Vestibular-evoked postural responses in the absence of somatosensory information. Brain 2002, 125, 2081–2088. [Google Scholar] [CrossRef]
- Felipe, L.; Simões, L.C.; Gonçalves, D.U.; Mancini, P.C. Evaluation of the caffeine effect in the vestibular test. Braz. J. Otorhinolaryngol. 2005, 71, 758–762. [Google Scholar] [CrossRef] [Green Version]
- McNerney, K.; Coad, M.L.; Burkard, R. The Influence of Caffeine on Calorics and Cervical Vestibular Evoked Myogenic Potentials (cVEMPs). J. Am. Acad. Audiol. 2014, 25, 261–267. [Google Scholar] [CrossRef] [PubMed]
- McNerney, K.M.; Coad, M.L.; Burkard, R. The Influence of Caffeine on Rotary Chair and Oculomotor Testing. J. Am. Acad. Audiol. 2018, 29, 587–595. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, R.C.; Day, B.L. Probing the human vestibular system with galvanic stimulation. J. Appl. Physiol. 2004, 96, 2301–2316. [Google Scholar] [CrossRef]
- Reynolds, R.F.; Osler, C.J. Galvanic Vestibular Stimulation Produces Sensations of Rotation Consistent with Activation of Semicircular Canal Afferents. Front. Neurol. 2012, 3, 104. [Google Scholar] [CrossRef] [Green Version]
- Ramdani, S.; Seigle, B.; Lagarde, J.; Bouchara, F.; Bernard, P.L. On the use of sample entropy to analyze human postural sway data. Med. Eng. Phys. 2009, 31, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, T.; Magnard, J.; Cornu, C. Postural control as a function of time-of-day: Influence of a prior strenuous running exercise or demanding sustained-attention task. J. Neuroeng. Rehabil. 2013, 10, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Higuchi, S.; Motohashi, Y. Changes in postural sway during a period of sustained wakefulness in male adults. Occup. Med. 2001, 51, 490–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorgensen, M.; Rathleff, M.S.; Laessoe, U.; Caserotti, P.; Nielsen, O.; Aagaard, P. Time-of-day influences postural balance in older adults. Gait Posture 2012, 35, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Melzer, I.; Benjuya, N.; Kaplanski, J. Postural stability in the elderly: A comparison between fallers and non-fallers. Age Ageing 2004, 33, 602–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| PICOS Component | Criterion |
|---|---|
| Population | Human participants with no exclusions based on age, gender or health status |
| Intervention | Caffeine ingestion in any form |
| Comparison | Placebo control |
| Outcome | Measures of balance control during upright standing |
| Study design | Crossover or parallel, randomised or non-randomised, placebo-controlled trials |
| Search Number | Search Terms | Database | |||
|---|---|---|---|---|---|
| Embase | PubMed/MEDLINE | SPORTDiscus | Web of Science | ||
| (15) | (“Caffeine” OR “Caffeinated” OR “Energy drinks” OR “Energy drink” OR “Coffee”) AND (“Balance” OR “Postural stability” OR “Postural sway” OR “Static balance” OR “Posture” OR “Postural control” OR “Standing” OR “Upright stance”) | 1044 | 605 | 138 | 926 |
| (14) | “Balance” OR “Postural stability” OR “Postural sway” OR “Static balance” OR “Posture” OR “Postural control” OR “Standing” OR “Upright stance” | 389,636 | 409,167 | 60,518 | 732,945 |
| (13) | “Upright stance” | 537 | 540 | 196 | 837 |
| (12) | “Standing” | 91,477 | 79,613 | 14,351 | 157,643 |
| (11) | “Postural control” | 6809 | 6471 | 3042 | 10,433 |
| (10) | “Posture” | 39,863 | 85,822 | 22,218 | 52,414 |
| (9) | “Static balance” | 1176 | 1145 | 705 | 1572 |
| (8) | “Postural sway” | 2485 | 2502 | 990 | 3348 |
| (7) | “Postural stability” | 3640 | 3250 | 1454 | 4986 |
| (6) | “Balance” | 275,715 | 267,320 | 30,810 | 538,394 |
| (5) | “Caffeine” OR “Caffeinated” OR “Energy drinks” OR “Energy drink” OR “Coffee” | 63,704 | 49,123 | 6147 | 72,355 |
| (4) | “Coffee” | 17,314 | 16,606 | 2154 | 36,579 |
| (3) | “Energy drink” OR “Energy drinks” | 1969 | 1619 | 1237 | 2281 |
| (2) | “Caffeinated” | 1439 | 1226 | 292 | 1265 |
| (1) | “Caffeine” | 49,311 | 34,878 | 3461 | 39,350 |
| Study | Question Described | Appropriate Study Design | Appropriate Subject Selection | Characteristics Described | Random Allocation | Researchers Blinded | Subjects Blinded | Outcome Measures Well Defined and Robust to Bias | Sample Size Appropriate | Analytic Methods Well Described | Estimate of Variance Reported | Controlled for Confounding | Results Reported in Detail | Conclusion Supported by Results | Rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Franks et al. (1975) [25] | 1 | 2 | 1 | 2 | 1 | 0 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 2 | Moderate |
| Nuotto et al. (1982) [26] | 1 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | Moderate |
| Swift and Tiplady (1988) [27] | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 0 | 1 | 1 | 1 | 1 | 2 | Moderate |
| Liguori and Robinson (2001) [28] | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | Strong |
| Norager et al. (2005) [29] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | Strong |
| Momsen et al. (2010) [30] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | Strong |
| Jensen et al. (2011) [31] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | Strong |
| Ben Waer et al. (2020) [32] | 2 | 2 | 1 | 2 | 0 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | Strong |
| Tallis et al. (2020) [33] | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 1 | 2 | Strong |
| Authors (Date of Publication) | Country | Participant Characteristics | Study Design | Caffeine Abstinence Protocol | Caffeine Condition(s) | Placebo Condition | Balance Measurement Timing (Post-Ingestion) | Balance Measurement Type | Balance Outcome (i.e., Effect of Caffeine) |
|---|---|---|---|---|---|---|---|---|---|
| Franks et al. (1975) [25] | Australia | 68 healthy participants 31 M, 37 F 20–28 years 1 | Randomised parallel | Caffeinated beverages before arrival (duration not reported) | Sugar-free orange squash 2 followed by 300 mg/70 kg (i.e., 4.3 mg∙kg−1) in de-caffeinated coffee | Sugar-free orange squash 2 followed by decaffeinated coffee alone | 20, 80 and 140 min | Body sway EO, EC | ↑Body sway (EO 20 min, 27% 3) EO 80 and 140 min, ns EC 20, 80 and 140 min, ns |
| Nuotto et al. (1982) [26] | Finland | 10 healthy participants 10 M, 0 F 21.1 ± 1.7 years | Randomised double-blind crossover | Caffeinated beverages for 24 h | Pellegrino beverage 2 followed by 500 mg in decaffeinated coffee (2 x 250 mg doses separated by 45 min) | Pellegrino beverage 2 followed by decaffeinated coffee alone (2 doses separated by 45 min) | 30, 60 and 120 min after first dose | Body sway EO, EC | EO 30, 60 and 120 min, ns EC 30, 60 and 120 min, ns |
| Swift and Tiplady (1988) [27] | UK | 6 healthy participants 2 M, 4 F 18–37 years 1 | Randomised double-blind crossover | Not reported | 200 mg capsule | Matching capsule | 60, 120 and 180 min | AP body sway EO | EO 60, 120 and 180 min, ns |
| Liguori and Robinson (2001) [28] | USA | 15 healthy participants 6 M, 9 F 21–45 years 1 (mean 32 years) | Randomised double-blind crossover | 24 h | (a) 200 mg capsule (b) 400 mg capsule followed by orange juice 2 | Methylcellulose capsule followed by orange juice 2 | 45 min | AP body sway Composite score based on six conditions of the EquiTest | (a) 200 mg caffeine Composite score, ns (b) 400 mg caffeine Composite score, ns |
| Ben Waer et al. (2020) [32] | Tunisia | 25 healthy participants 0 M, 25 F 53 ± 4 years | Double-blind crossover | 12 h | (a) 100 mg capsule (b) 400 mg capsule | Empty capsule | 30 min | COPVelMean COPMLpath COPAPpath EO, EC, EOF, ECF | (a) 100 mg caffeine: ↓COPVelMean, ↓COPMLpath and ↓COPAPpath (ECF all −16% 3) EO, EC and EOF, ns (b) 400 mg caffeine: EO, EC, EOF and ECF, ns |
| Authors (Date of Publication) | Country | Participant Characteristics | Study Design | Caffeine Abstinence Protocol | Caffeine Condition(s) | Placebo Condition | Balance Measurement Timing (Post-Ingestion) | Balance Measurement Type | Balance outcome (i.e., Effect of Caffeine) |
|---|---|---|---|---|---|---|---|---|---|
| Swift and Tiplady (1988) [27] | UK | 6 healthy participants 3 M, 3 F 65–75 years 1 | Randomised double-blind crossover | Not reported | 200 mg capsule | Matching capsule | 60, 120 and 180 min | AP body sway EO | ↑AP body sway (EO 180 min) EO 60 and 120 min, ns |
| Norager et al. (2005) [29] | Denmark | 30 healthy participants 15 M, 15 F 74.7 ± 5.5 years | Randomised double-blind crossover | 48 h | 6 mg∙kg−1 capsule | Glucose monohydrate capsule | 60 min | COPVelMom EO, EC, EOST | ↑COPVelMom (EO 25%, EC 43%) EOST, ns |
| Momsen et al. (2010) [30] | Denmark | 88 patients with intermittent claudication 50 M, 38 F 67.5 ± 6.9 years | Randomised double-blind crossover | 48 h | 6 mg∙kg−1 capsule | Glucose monohydrate capsule | 75 min | COPVelMom EO, EC | ↑COPVelMom (EO 22%, EC 22%) |
| Jensen et al. (2011) [31] | Denmark | 30 healthy participants 15 M, 15 F 74.1 (70.2–84.9) years 2 | Randomised double-blind crossover | 8 h | 6 mg∙kg−1 capsule | Glucose monohydrate capsule | 60 min | COPVelMom EO, EC, EOST | ↑COPVelMom (EO 19%, EC 42%) EOST, ns |
| Tallis et al. (2020) [33] | UK | 12 healthy participants 4 M, 8 F 72 ± 4 years | Randomised double-blind crossover | 12 h | 3 mg∙kg−1 capsule | Maltodextrin capsule | 45 min | COPVelMean COPPath COPMLmax COPAPmax COPEllipse EO, EC, EOF, ECF, EO3s, EO7s, EOF3s, EOF7s | ↑COPVelMean (EO 21%, EC 25%, EOF 8%, ECF 6%, EO3s 3%, EO7s 8%, EOF3s −6%, EOF7s 9%) ↑COPPath (EO 22%, EC 27%, EOF 8%, ECF 6%, EO3s 2%, EO7s 8%, EOF3s −6%, EOF7s 6%) ↑COPMLmax (EO 89%, EC 114%, EOF 34%, ECF 23%, EO3s 9%, EO7s 93%, EOF3s 6%, EOF7s 2%) COPAPmax, ns COPEllipse, ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briggs, I.; Chidley, J.B.; Chidley, C.; Osler, C.J. Effects of Caffeine Ingestion on Human Standing Balance: A Systematic Review of Placebo-Controlled Trials. Nutrients 2021, 13, 3527. https://doi.org/10.3390/nu13103527
Briggs I, Chidley JB, Chidley C, Osler CJ. Effects of Caffeine Ingestion on Human Standing Balance: A Systematic Review of Placebo-Controlled Trials. Nutrients. 2021; 13(10):3527. https://doi.org/10.3390/nu13103527
Chicago/Turabian StyleBriggs, Isobel, Joel B. Chidley, Corinna Chidley, and Callum J. Osler. 2021. "Effects of Caffeine Ingestion on Human Standing Balance: A Systematic Review of Placebo-Controlled Trials" Nutrients 13, no. 10: 3527. https://doi.org/10.3390/nu13103527
APA StyleBriggs, I., Chidley, J. B., Chidley, C., & Osler, C. J. (2021). Effects of Caffeine Ingestion on Human Standing Balance: A Systematic Review of Placebo-Controlled Trials. Nutrients, 13(10), 3527. https://doi.org/10.3390/nu13103527