Translation and Validation of the Caffeine Expectancy Questionnaire in Brazil (CaffEQ-BR)

 , ,
, ,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
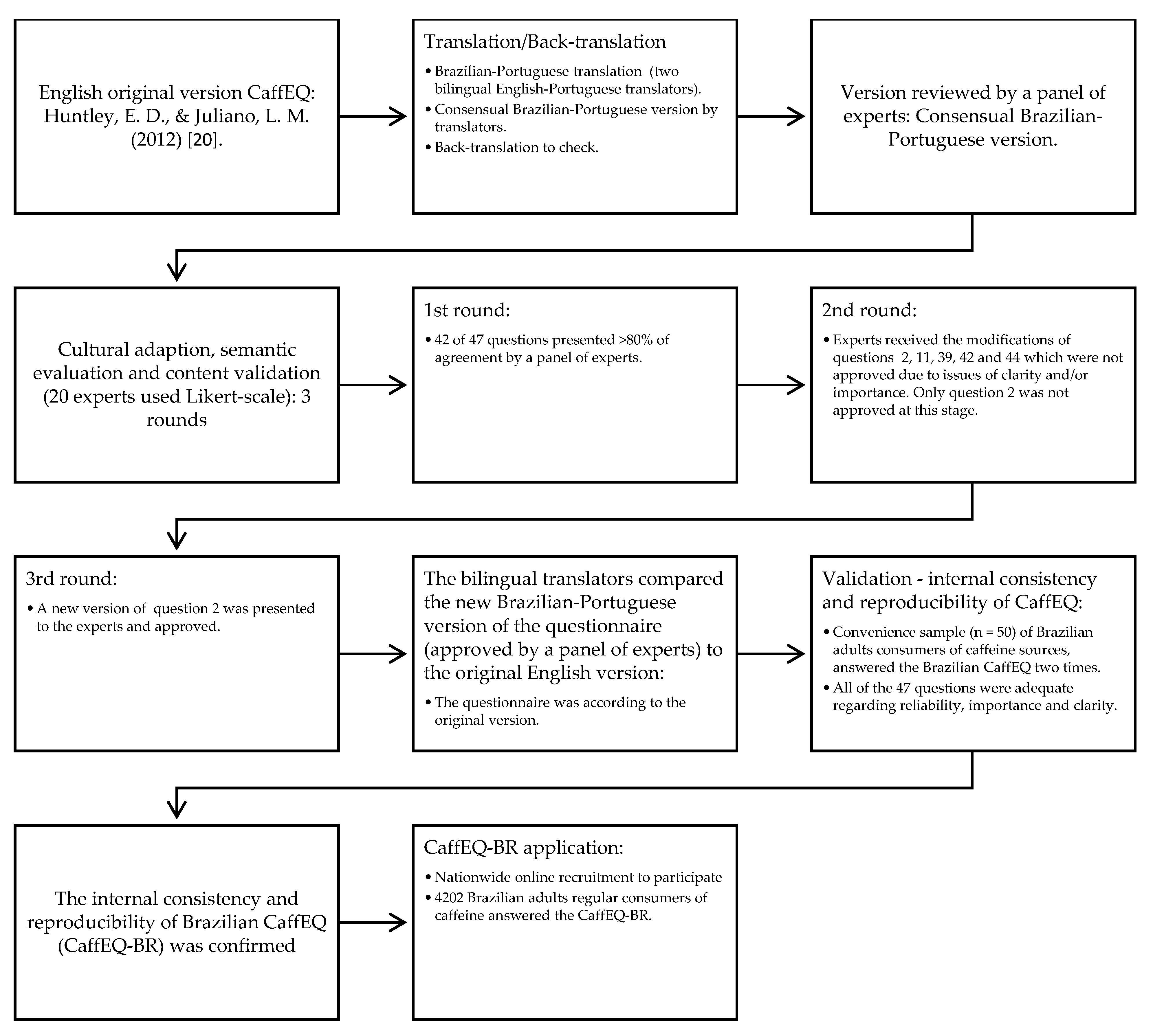
2.1. Translation, Cultural Adaptation, and Semantic Assessment
2.2. Internal Consistency and Reproducibility of CaffEQ-BR
2.3. Brazilian Nationwide Application of CaffEQ-BR
2.3.1. Sociodemographic and Health Data
2.3.2. Caffeine Consumption
2.4. Statistical Analysis
3. Results
3.1. Translation, Cultural Adaptation, Semantic Evaluation, and Content Validation
3.2. Reproducibility and Internal Consistency of the CaffEQ-BR
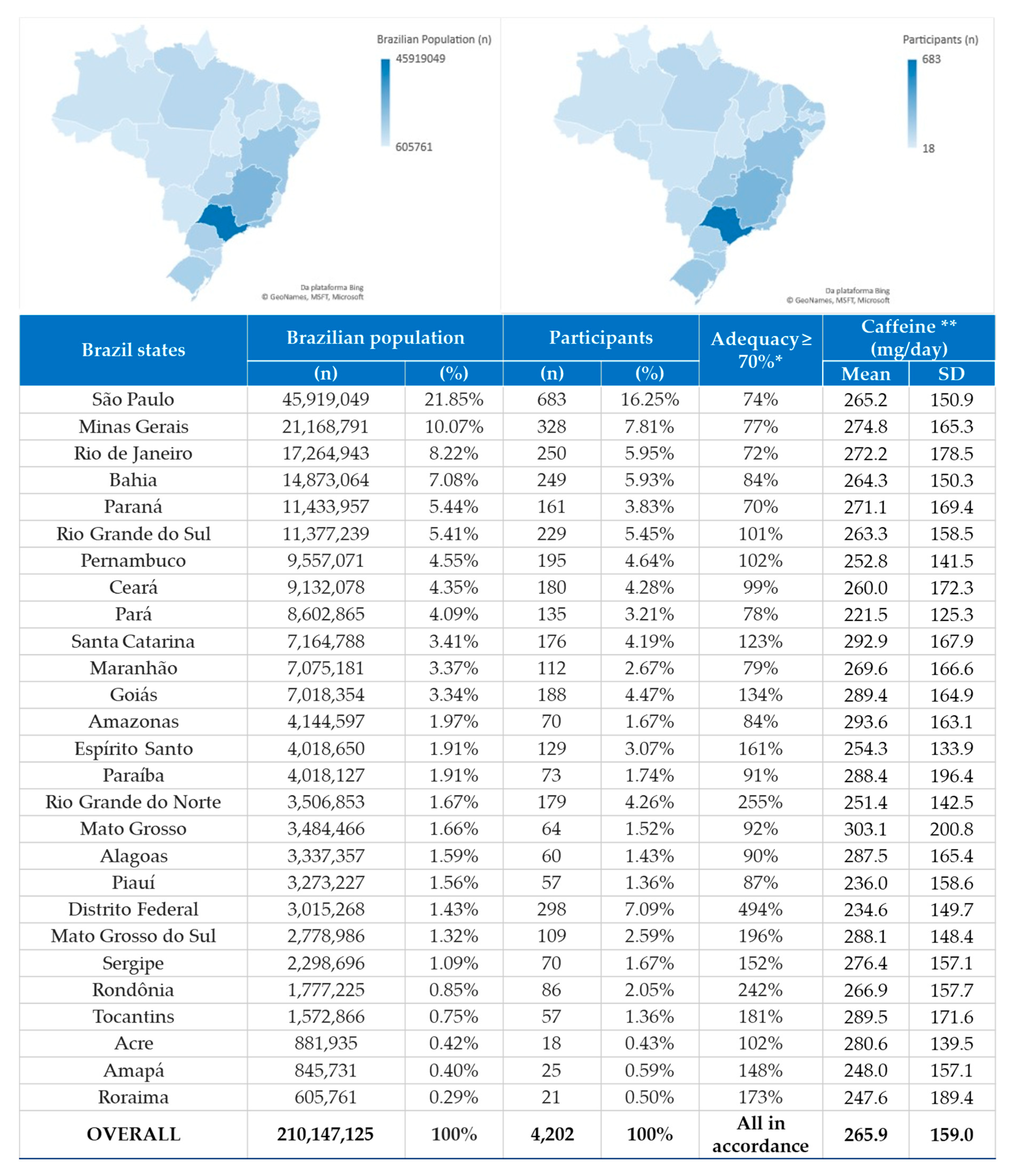
3.3. Brazilian Nationwide Application of the CaffEQ-BR
3.3.1. Participants
3.3.2. Caffeine Consumption
3.3.3. Confirmatory Factor Analysis and Associations of the CaffEQ-BR
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
| Itens | Muito Improvável | Improvável | Um Pouco Improvável | Um Pouco Provável | Provável | Muito Provável |
| 1. Cafeína/café me dá ânimo quando estou cansado | □ | □ | □ | □ | □ | □ |
| 2. Eu fico extrovertido quando tomo cafeína/café | □ | □ | □ | □ | □ | □ |
| 3. Cafeína/café me ajuda a não comer mais do que deveria | □ | □ | □ | □ | □ | □ |
| 4. Fico facilmente estressado depois de tomar cafeína/café | □ | □ | □ | □ | □ | □ |
| 5. Cafeína/café melhora meu desempenho físico | □ | □ | □ | □ | □ | □ |
| 6. Fico menos cansado depois de tomar cafeína | □ | □ | □ | □ | □ | □ |
| 7. A cafeína/café tira minha fome | □ | □ | □ | □ | □ | □ |
| 8. Fico triste quando não tomo cafeína/café | □ | □ | □ | □ | □ | □ |
| 9. Cafeína/café melhora meu humor | □ | □ | □ | □ | □ | □ |
| 10. Eu fico ansioso quando não tomo cafeína/café | □ | □ | □ | □ | □ | □ |
| 11. Eu me sinto angustiado quando tomo cafeína/café | □ | □ | □ | □ | □ | □ |
| 12. Eu me exercito melhor depois de tomar cafeína/café | □ | □ | □ | □ | □ | □ |
| 13. Eu sinto muita falta de cafeína/café quando não tomo | □ | □ | □ | □ | □ | □ |
| 14. Eu não gosto do jeito que eu me sinto após tomar cafeína/café | □ | □ | □ | □ | □ | □ |
| 15. Eu me sinto mal se ficar sem cafeína/café | □ | □ | □ | □ | □ | □ |
| 16. Cafeína/café aumenta minha motivação para trabalhar | □ | □ | □ | □ | □ | □ |
| 17. Eu me sinto mais confiante depois de tomar cafeína/café | □ | □ | □ | □ | □ | □ |
| 18. Tomar cafeína/café a qualquer hora do dia atrapalha o meu sono | □ | □ | □ | □ | □ | □ |
| 19. Quando tomo cafeína/café fico nervoso(a) | □ | □ | □ | □ | □ | □ |
| 20. Quando tomo cafeína/café fico mais alerta | □ | □ | □ | □ | □ | □ |
| 21. Mesmo quando tomo uma pequena quantidade de cafeína/café fico ansioso | □ | □ | □ | □ | □ | □ |
| 22. Cafeína/café melhora minha concentração | □ | □ | □ | □ | □ | □ |
| 23. Quando tomo cafeína/café fico mais amigável | □ | □ | □ | □ | □ | □ |
| 24. Eu tenho que tomar cafeína/café todos os dias | □ | □ | □ | □ | □ | □ |
| 25. Cafeína/café me faz suar | □ | □ | □ | □ | □ | □ |
| 26. Cafeína/café me faz pular refeições | □ | □ | □ | □ | □ | □ |
| 27. Tenho muita vontade de tomar cafeína/café se não tiver tomado a quantidade de sempre | □ | □ | □ | □ | □ | □ |
| 28. Tomar cafeína/café na hora de dormir atrapalha meu sono | □ | □ | □ | □ | □ | □ |
| 29. Cafeína/café me deixa irritado | □ | □ | □ | □ | □ | □ |
| 30. Eu desejo cafeína/café o tempo todo | □ | □ | □ | □ | □ | □ |
| 31. Cafeína/café me ajuda a trabalhar por mais tempo | □ | □ | □ | □ | □ | □ |
| 32. Cafeína/café me faz sentir feliz | □ | □ | □ | □ | □ | □ |
| 33. Eu não funciono sem tomar cafeína/café | □ | □ | □ | □ | □ | □ |
| 34. Quando tomo cafeína/café meu coração acelera | □ | □ | □ | □ | □ | □ |
| 35. Eu tenho dificuldade em começar o dia sem tomar cafeína/café | □ | □ | □ | □ | □ | □ |
| 36. Sinto dor de estômago quando tomo cafeína/café | □ | □ | □ | □ | □ | □ |
| 37. Eu não conseguiria parar de tomar cafeína/café | □ | □ | □ | □ | □ | □ |
| 38. Tomar cafeína/café no final da tarde atrapalha o meu sono | □ | □ | □ | □ | □ | □ |
| 39. Cafeína/café me ajuda a regular o peso | □ | □ | □ | □ | □ | □ |
| 40. Quanto não tomo cafeína/café sinto dor de cabeça | □ | □ | □ | □ | □ | □ |
| 41. Cafeína/café melhora minha atenção | □ | □ | □ | □ | □ | □ |
| 42. Eu fico mais extrovertido(a) quando tomo cafeína/café | □ | □ | □ | □ | □ | □ |
| 43. Cafeína/café me ajuda a me exercitar por mais tempo | □ | □ | □ | □ | □ | □ |
| 44. Sinto-me mais disposto quando tomo cafeína/café | □ | □ | □ | □ | □ | □ |
| 45. Cafeína/café me faz sentir com mais energia | □ | □ | □ | □ | □ | □ |
| 46. Cafeína/café diminui o meu apetite | □ | □ | □ | □ | □ | □ |
| 47. Tomar cafeína/café no final do dia não me deixa dormir | □ | □ | □ | □ | □ | □ |
References
- Reyes, C.M.; Cornelis, M.C. Caffeine in the diet: Country-level consumption and guidelines. Nutrients 2018, 10, 1772. [Google Scholar] [CrossRef] [PubMed]
- Boolani, A.; Fuller, D.T.; Mondal, S.; Wilkinson, T.; Darie, C.C.; Gumpricht, E. Caffeine-Containing, Adaptogenic-Rich Drink Modulates the Effects of Caffeine on Mental Performance and Cognitive Parameters: A Double-Blinded, Placebo-Controlled, Randomized Trial. Nutrients 2020, 12, 1922. [Google Scholar] [CrossRef] [PubMed]
- Wikoff, D.; Welsh, B.T.; Henderson, R.; Brorby, G.P.; Britt, J.; Myers, E.; Goldberger, J.; Lieberman, H.R.; O’Brien, C.; Peck, J.; et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem. Toxicol. 2017, 109, 585–648. [Google Scholar] [CrossRef] [PubMed]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017. [Google Scholar] [CrossRef]
- Maughan, R.J.; Burke, L.M.; Dvorak, J.; Larson-Meyer, D.E.; Peeling, P.; Phillips, S.M.; Rawson, E.S.; Walsh, N.P.; Garthe, I.; Geyer, H.; et al. IOC consensus statement: Dietary supplements and the high-performance athlete. Br. J. Sports Med. 2018, 28, 104–105. [Google Scholar]
- Sousa, A.G.; Da Costa, T.H.M. Usual coffee intake in Brazil: Results from the National Dietary Survey 2008-9. Br. J. Nutr. 2015, 113, 1615–1620. [Google Scholar] [CrossRef]
- Pereira, R.A.; Souza, A.M.; Duffey, K.J.; Sichieri, R.; Popkin, B.M. Beverage consumption in Brazil: Results from the first National Dietary Survey. Public Health Nutr. 2015, 18, 1164–1172. [Google Scholar] [CrossRef]
- Souza, A.D.M.; Pereira, R.A.; Yokoo, E.M.; Levy, R.B.; Sichieri, R. Most consumed foods in Brazil: National dietary survey 2008–2009. Rev. Saude Publica 2014, 18, 1164–1172. [Google Scholar] [CrossRef]
- Heckman, M.A.; Weil, J.; de Mejia, E.G. Caffeine (1, 3, 7-trimethylxanthine) in foods: A comprehensive review on consumption, functionality, safety, and regulatory matters. J. Food Sci. 2010, 75, R77–R87. [Google Scholar] [CrossRef]
- Mahoney, C.R.; Giles, G.E.; Marriott, B.P.; Judelson, D.A.; Glickman, E.L.; Geiselman, P.J.; Lieberman, H.R. Intake of caffeine from all sources and reasons for use by college students. Clin. Nutr. 2019, 38, 668–675. [Google Scholar] [CrossRef]
- Fulton, J.L.; Dinas, P.C.; Carrillo, A.E.; Edsall, J.R.; Ryan, E.J.; Ryan, E.J. Impact of genetic variability on physiological responses to caffeine in humans: A systematic review. Nutrients 2018, 10, 1373. [Google Scholar] [CrossRef] [PubMed]
- Ágoston, C.; Urbán, R.; Király, O.; Griffiths, M.D.; Rogers, P.J.; Demetrovics, Z. Why Do You Drink Caffeine? The Development of the Motives for Caffeine Consumption Questionnaire (MCCQ) and Its Relationship with Gender, Age and the Types of Caffeinated Beverages. Int. J. Ment. Health Addict. 2017, 16, 981–999. [Google Scholar] [CrossRef] [PubMed]
- Saunders, B.; de Oliveira, L.F.; da Silva, R.P.; de Salles Painelli, V.; Gonçalves, L.S.; Yamaguchi, G.; Mutti, T.; Maciel, E.; Roschel, H.; Artioli, G.G.; et al. Placebo in sports nutrition: A proof-of-principle study involving caffeine supplementation. Scand. J. Med. Sci. Sport. 2016, 27, 1240–1247. [Google Scholar] [CrossRef] [PubMed]
- Beedie, C.J.; Stuart, E.M.; Coleman, D.A.; Foad, A.J. Placebo effects of caffeine on cycling performance. Med. Sci. Sports Exerc. 2006, 38, 2159–2164. [Google Scholar] [CrossRef]
- Saunders, B.; Saito, T.; Klosterhoff, R.; de Oliveira, L.F.; Barreto, G.; Perim, P.; Pinto, A.J.; Lima, F.; de Sá Pinto, A.L.; Gualano, B. “I put it in my head that the supplement would help me”: Open-placebo improves exercise performance in female cyclists. PLoS ONE 2019, 14, e0222982. [Google Scholar] [CrossRef]
- Dömötör, Z.; Szemerszky, R.; Köteles, F. Subjective and objective effects of coffee consumption—Caffeine or expectations? Acta Physiol. Hung. 2015, 102, 77–85. [Google Scholar] [CrossRef]
- Shabir, A.; Hooton, A.; Tallis, J.; Higgins, M.F. The influence of caffeine expectancies on sport, exercise, and cognitive performance. Nutrients 2018, 10, 1528. [Google Scholar] [CrossRef]
- Heinz, A.J.; Kassel, J.D.; Smith, E.V. Caffeine Expectancy: Instrument Development in the Rasch Measurement Framework. Psychol. Addict. Behav. 2009, 23, 500–511. [Google Scholar] [CrossRef]
- Kearns, N.T.; Blumenthal, H.; Natesan, P.; Zamboanga, B.L.; Ham, L.S.; Cloutier, R.M. Development and initial psychometric validation of the brief-caffeine expectancy questionnaire (B-CaffEQ). Psychol. Assess. 2018, 30, 1597–1611. [Google Scholar] [CrossRef]
- Huntley, E.D.; Juliano, L.M. Caffeine Expectancy Questionnaire (CaffEQ): Construction, psychometric properties, and associations with caffeine use, caffeine dependence, and other related variables. Psychol. Assess. 2012, 24, 592–607. [Google Scholar] [CrossRef]
- Schott, M.; Beiglböck, W.; Neuendorff, R. Translation and Validation of the Caffeine Expectancy Questionnaire (CaffEQ). Int. J. Ment. Health Addict. 2016, 14, 514–525. [Google Scholar] [CrossRef]
- Pasquali, L. Psicometria. Rev. Esc. Enferm. USP 2009, 43, 992–999. [Google Scholar] [CrossRef]
- Knapp, H.; Kirk, S.A. Using pencil and paper, Internet and touch-tone phones for self-administered surveys: Does methodology matter? Comput. Human Behav. 2003, 19, 117–134. [Google Scholar] [CrossRef]
- World Health Organization. Process of Translation and Adaptation of Instruments. Available online: https://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 26 May 2020).
- Meijering, J.V.; Kampen, J.K.; Tobi, H. Quantifying the development of agreement among experts in Delphi studies. Technol. Forecast. Soc. Chang. 2013, 80, 1607–1614. [Google Scholar] [CrossRef]
- Watson, P.F.; Petrie, A. Method agreement analysis: A review of correct methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef]
- Bartlett, J.W.; Chris, F. Reliability, repeatability and reproducibility: Analysis of measurement errors in continuous variables. Ultrasound Obstet. Gynecol. 2008, 31, 466–475. [Google Scholar] [CrossRef]
- Streiner, D.L.; Norman, G.R. Health Measurement Scales: A Practical Guide to Their Development and Use; Oxford University Press: Oxford, UK, 2008; ISBN 9780191724015. [Google Scholar]
- Streiner, D.L.; Streiner, D.L. Starting at the Beginning: An Introduction to Coefficient Alpha and Internal Consistency. J. Pers. Assess. 2003, 80, 99–103. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis; Pearson new international edition; Essex, Pearson Education Limited: London, UK, 2014. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guideline: Sugars Intake for Adults and Children; WHO: Geneva, Switzerland, 2015; ISBN 9789241549028. [Google Scholar]
- Institute of Medicine (IOM). DRI Dietary Reference Intakes: Applications in Dietary Assessment; National Academies Press: Washington, DC, USA, 2000; ISBN 9780309502543. [Google Scholar]
- Shohet, K.L.; Landrum, R.E. Caffeine consumption questionnaire: A standardized measure for caffeine consumption in undergraduate students. Psychol. Rep. 2001, 89, 521–526. [Google Scholar] [CrossRef]
- Irons, J.G.; Bassett, D.T.; Prendergast, C.O.; Landrum, R.E.; Heinz, A.J. Development and Initial Validation of the Caffeine Consumption Questionnaire-Revised. J. Caffeine Res. 2016, 6, 20–25. [Google Scholar] [CrossRef]
- IBGE—Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares: 2008–2009. Antropometria e Estado Nutricional de Crianças, Adolescentes e Adultos no Brasil. ISBN 978-85-240-4131-0. Available online: https://biblioteca.ibge.gov.br/visualizacao/livros/liv50000.pdf (accessed on 7 July 2020).
- Dharmasena, S.; Capps, O.; Clauson, A. Ascertaining the Impact of the 2000 USDA Dietary Guidelines for Americans on the Intake of Calories, Caffeine, Calcium, and Vitamin C from At-Home Consumption of Nonalcoholic Beverages. J. Agric. Appl. Econ. 2011, 43, 13–27. [Google Scholar] [CrossRef][Green Version]
- Vogelzang, J.L. Health Measurement Scales: A Practical Guide to Their Development and Use. J. Nutr. Educ. Behav. 2015, 47, 484.e1. [Google Scholar] [CrossRef]
- IBGE—Instituto Brasileiro de Geografia e Estatística. IBGE Divulga As Estimativas da População dos Municípios para 2019. Estatísticas Sociais 2019. Available online: https://agenciadenoticias.ibge.gov.br/media/com_mediaibge/arquivos/7d410669a4ae85faf4e8c3a0a0c649c7.pdf (accessed on 26 May 2020).
- World Health Organization (WHO). Mean Body Mass Index (BMI). WHO 2017. Available online: https://www.who.int/gho/ncd/risk_factors/bmi_text/en/ (accessed on 26 May 2020).
- Baeza, F.L.C.; Caldieraro, M.A.K.; Pinheiro, D.O.; Fleck, M.P. Translation and cross-cultural adaptation into Brazilian Portuguese of the Measure of Parental Style (MOPS)—A self-reported scale—According to the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) recommendations. Rev. Bras. Psiquiatr. 2010, 32, 159–163. [Google Scholar] [CrossRef]
- Santo, R.M.; Ribeiro-Ferreira, F.; Alves, M.R.; Epstein, J.; Novaes, P. Enhancing the cross-cultural adaptation and validation process: Linguistic and psychometric testing of the Brazilian-Portuguese version of a self-report measure for dry eye. J. Clin. Epidemiol. 2015, 68, 370–378. [Google Scholar] [CrossRef]
- IBGE—Instituto Brasileiro de Geografia e Estatística. Censo Demográfico 2010. Características da População e dos Domicílios. 2010. Available online: https://biblioteca.ibge.gov.br/visualizacao/periodicos/93/cd_2010_caracteristicas_populacao_domicilios.pdf (accessed on 26 May 2020).
- IBGE—Instituto Brasileiro de Geografia e Estatística. Características Gerais dos Domicílios e dos Moradores: 2018. Available online: https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=2101654 (accessed on 26 May 2020).
- Gori-Maia, A. Relative Income, Inequality and Subjective Wellbeing: Evidence for Brazil. Soc. Indic. Res. 2013, 113, 1193–1204. [Google Scholar] [CrossRef]
- Pratesi, C.P.; Häuser, W.; Uenishi, R.H.; Selleski, N.; Nakano, E.Y.; Gandolfi, L.; Pratesi, R.; Zandonadi, R.P. Quality of life of celiac patients in Brazil: Questionnaire translation, cultural adaptation and validation. Nutrients 2018, 10, 1167. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, S.M.; Araújo, W.M.C.; Nakano, E.Y.; Zandonadi, R.P. Brazilian vegetarians diet quality markers and comparison with the general population: A nationwide cross-sectional study. PLoS ONE 2020, 15, e0232954. [Google Scholar] [CrossRef]
- Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise em Saúde e Vigilância de Doenças Não Transmissíveis. Vigitel Brasil 2019: Surveillance of Risk and Protective Factors for Chronic Diseases by Telephone Survey: Estimates of Frequency and Sociodemographic Distribution of Risk and Protective Factors for Chronic Diseases in the Capitals of the 26 Brasilian States. Available online: http://www.crn1.org.br/wp-content/uploads/2020/04/vigitel-brasil-2019-vigilancia-fatores-risco.pdf?x53725 (accessed on 26 May 2020).
- Sommer, I.; Griebler, U.; Mahlknecht, P.; Thaler, K.; Bouskill, K.; Gartlehner, G.; Mendis, S. Socioeconomic inequalities in non-communicable diseases and their risk factors: An overview of systematic reviews. BMC Public Health 2015, 15, 914. [Google Scholar] [CrossRef] [PubMed]
- Giovanini de Oliveira Sartori, A.; Vieira da Silva, M. Caffeine in Brazil: Intake, socioeconomic and demographic determinants, and major dietary sources. Nutrire 2016, 41, 147. [Google Scholar] [CrossRef]
- Dourado, P.; Porto, M.; Dal Pizzol, T.; Ramos, L.; Serrate, S.; Luiza, V.; Leão, N.; Rocha, M.; Oliveira, M.; Dâmaso, A.; et al. Prevalência da automedicação no Brasil e fatores associados. Rev. Saúde Pública 2016, 50. [Google Scholar] [CrossRef]
- dePaula, J.; Farah, A. Caffeine Consumption through Coffee: Content in the Beverage, Metabolism, Health Benefits and Risks. Beverages 2019, 5, 37. [Google Scholar] [CrossRef]
- Choi, J. Motivations Influencing Caffeine Consumption Behaviors among College Students in Korea: Associations with Sleep Quality. Nutrients 2020, 14, 953. [Google Scholar] [CrossRef] [PubMed]
- Temple, J.L.; Ziegler, A.M. Gender Differences in Subjective and Physiological Responses to Caffeine and the Role of Steroid Hormones. J. Caffeine Res. 2011, 1, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Temple, J.L.; Bulkley, A.M.; Briatico, L.; Dewey, A.M. Sex differences in reinforcing value of caffeinated beverages in adolescents. Behav. Pharmacol. 2009, 20, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Temple, J.L.; Dewey, A.M.; Briatico, L.N. Effects of Acute Caffeine Administration on Adolescents. Exp. Clin. Psychopharmacol. 2010, 18, 510–520. [Google Scholar] [CrossRef]
- Dillon, P.; Kelpin, S.; Kendler, K.; Thacker, L.; Dick, D.; Svikis, D. Gender Differences in Any-Source Caffeine and Energy Drink Use and Associated Adverse Health Behaviors. J. Caffeine Adenosine Res. 2019, 9, 12–19. [Google Scholar] [CrossRef]
- Kolb, H.; Kempf, K.; Martin, S. Health Effects of Coffee: Mechanism Unraveled? Nutrients 2020, 12, 1842. [Google Scholar] [CrossRef]
- International Coffee Organization. Trade Statistics; International Coffee Organization (ICO), 2019; Available online: http://www.ico.org/trade_statistics.asp (accessed on 26 May 2020).
- Toledo, R.A. O ciclo do café e o processo de urbanização do Estado de São Paulo. Historien 2012, 6, 76–89. [Google Scholar] [CrossRef]
- Associação Brasileira de Industria do Café—ABIC. Consórcio Pesquisa Café Brasil. Available online: http://www.consorciopesquisacafe.com.br/index.php/publicacoes/637 (accessed on 26 May 2020).
- Gebara, K.S.; Gasparotto-Junior, A.; Santiago, P.G.; Cardoso, C.A.L.; De Souza, L.M.; Morand, C.; Costa, T.A.; Cardozo-Junior, E.L. Daily Intake of Chlorogenic Acids from Consumption of Maté (Ilex paraguariensis A.St.-Hil.) Traditional Beverages. J. Agric. Food Chem. 2017, 65, 10093–10110. [Google Scholar] [CrossRef] [PubMed]
- Schimpl, F.C.; Da Silva, J.F.; Gonçalves, J.F.D.C.; Mazzafera, P. Guarana: Revisiting a highly caffeinated plant from the Amazon. J. Ethnopharmacol. 2013, 150, 14–31. [Google Scholar] [CrossRef]
- Liang, N.; Kitts, D.D. Role of chlorogenic acids in controlling oxidative and inflammatory stress conditions. Nutrients 2016, 8, 16. [Google Scholar] [CrossRef]
- IBGE—Instituto Brasileiro de Geografia e Estatística. Acesso à Internet e à Televisão e Posse de Telefone Móvel. Available online: https://biblioteca.ibge.gov.br/index.php/biblioteca-catalogo?view=detalhes&id=2101543 (accessed on 26 May 2020).
- Schatzkin, A.; Kipnis, V.; Carroll, R.J.; Midthune, D.; Subar, A.F.; Bingham, S.; Schoeller, D.A.; Troiano, R.P.; Freedman, L.S. A comparison of a food frequency questionnaire with a 24-hour recall for use in an epidemiological cohort study: Results from the biomarker-based Observing Protein and Energy Nutrition (OPEN) study. Int. J. Epidemiol. 2003, 32, 1054–1062. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factors | N. Items | Internal Consistency Cronbach Alpha (95% CI) | Reproducibility Intraclass Correlation Coefficient (95% CI) |
|---|---|---|---|
| Withdrawal/dependence | 12 | 0.948 (0.923–0.968) | 0.983 (0.969–0.991) |
| Energy/work enhancement | 8 | 0.926 (0.888–0.923) | 0.953 (0.912–0.975) |
| Appetite suppression | 5 | 0.872 (0.802–0.923) | 0.951 (0.903–0.974) |
| Social/mood enhancement | 6 | 0.889 (0.829–0.932) | 0.949 (0.900–0.973) |
| Physical performance enhancement | 3 | 0.924 (0.875–0.956) | 0.965 (0.936–0.981) |
| Anxiety/negative physical effects | 9 | 0.872 (0.807–0.921) | 0.953 (0.907–0.976) |
| Sleep disturbance | 4 | 0.941 (0.907–0.965) | 0.970 (0.945–0.983) |
| Overall | 47 | 0.948 (0.923–0.967) | 0.976 (0.935–0.989) |
| Categories | Total (n = 4202) | ||
|---|---|---|---|
| n | % | ||
| Gender | Male | 2063 | 49.1 |
| Female | 2139 | 50.9 | |
| Age | 19–24 | 822 | 19.5 |
| 25–30 | 755 | 18.0 | |
| 31–40 | 1331 | 31.7 | |
| 41–59 | 1294 | 30.8 | |
| Body Mass Index * (kg/m²) | <18.5 | 106 | 2.5 |
| 18.5–24.9 | 1751 | 41.7 | |
| 25–29.9 | 1498 | 35.6 | |
| ≥30 | 847 | 20.2 | |
| Self-Identified ethnicity | Asia descendants | 114 | 2.7 |
| White | 2328 | 55.4 | |
| Indigenous | 41 | 1.0 | |
| Pardo | 1330 | 31.6 | |
| Black | 309 | 7.4 | |
| Without description | 80 | 1.9 | |
| Physical Exercises ≥ 150 min/week | No | 1924 | 45.8 |
| Yes | 2278 | 54.2 | |
| Educational Level | No schooling | 3 | 0.1 |
| Incomplete elementary school | 17 | 0.4 | |
| Completed elementary school | 37 | 0.9 | |
| Incomplete high school | 101 | 2.4 | |
| Completed high school | 596 | 14.2 | |
| Incomplete higher education | 955 | 22.7 | |
| Higher education graduate | 1162 | 27.6 | |
| Postgraduate studies | 1315 | 31.3 | |
| Without description | 16 | 0.4 | |
| Monthly Income (BRL) ** | 1000.00 | 407 | 9.7 |
| 1000.01 to 2000.00 | 769 | 18.3 | |
| 2000.01 to 3000.00 | 669 | 15.9 | |
| 3000.01 to 5000.00 | 865 | 20.6 | |
| 5000.01 to 10,000.00 | 796 | 18.9 | |
| Above 10,000.00 | 575 | 13.7 | |
| Without description | 121 | 2.9 | |
| Self-Reported Chronic Diseases | No | 3397 | 80.8 |
| Yes | 805 | 19.2 | |
| Caffeine Sources ¹ | Coffee 2 | Tea 3 | Chocolate 4 | Chocolate Beverages 5 | Soft Drinks 6 | Medication 7 | Energy Drinks 8 | Sports Supplements 9 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | N | (%) | ||
| Time of the Day | Early morning (00:00–06:00) | 202 | 4.8% | 79 | 1.9% | 153 | 3.6% | 70 | 1.7% | 149 | 3.5% | 115 | 2.7% | 109 | 2.6% | 19 | 0.5% |
| Morning (06:00–12:00) | 3853 | 91.7% | 503 | 12.0% | 644 | 15.3% | 653 | 15.5% | 362 | 8.6% | 505 | 12.0% | 188 | 4.5% | 333 | 7.9% | |
| Afternoon (12:00–18:00) | 2829 | 67.3% | 686 | 16.3% | 1594 | 37.9% | 523 | 12.4% | 1361 | 32.4% | 396 | 9.4% | 324 | 7.7% | 206 | 4.9% | |
| Evening (18:00–24:00) | 1508 | 35.9% | 878 | 20.9% | 1291 | 30.7% | 563 | 13.4% | 1058 | 25.2% | 699 | 16.6% | 348 | 8.3% | 122 | 2.9% | |
| N° of Servings Per Day | 1 | 971 | 23.1% | 1178 | 28.0% | 1647 | 39.2% | 908 | 21.6% | 985 | 23.4% | 824 | 19.6% | 530 | 12.6% | 463 | 11.0% |
| 2 | 1958 | 46.6% | 322 | 7.7% | 537 | 12.8% | 273 | 6.5% | 543 | 12.9% | 209 | 5.0% | 141 | 3.4% | 78 | 1.9% | |
| 3 | 983 | 23.4% | 92 | 2.2% | 235 | 5.6% | 89 | 2.1% | 209 | 5.0% | 111 | 2.6% | 43 | 1.0% | 19 | 0.5% | |
| 4 | 139 | 3.3% | 12 | 0.3% | 64 | 1.5% | 22 | 0.5% | 58 | 1.4% | 35 | 0.8% | 7 | 0.2% | 1 | 0.0% | |
| Total Recorded | 4051 | 96.4% | 1604 | 38.2% | 2483 | 59.1% | 1292 | 30.7% | 1795 | 42.7% | 1179 | 28.1% | 721 | 17.2% | 561 | 13.4% | |
| Sources | Factors of the CaffEQ-BR * | ||||||
|---|---|---|---|---|---|---|---|
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | |
| Caffeine ** (mg/day) | 0.085 *** | 0.102 *** | 0.081 *** | 0.141 *** | 0.097 *** | 0.095 *** | −0.074 *** |
| Regions ** | Factors of the CaffEQ-BR * Mean (SD) | ||||||
|---|---|---|---|---|---|---|---|
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | |
| North | 3.48 (1.49) | 4.16 (1.37) | 2.21 (1.15) | 3.56 (1.45) | 3.49 (1.55) | 1.78 (0.69) | 2.51 (1.60) |
| Northeast | 3.44 (1.41) | 4.15 (1.31) | 2.24 (1.14) | 3.44 (1.38) | 3.55 (1.53) | 1.81 (0.77) | 2.45 (1.58) |
| Midwest | 3.34 (1.39) | 4.08 (1.32) | 2.13 (1.14) | 3.25 (1.34) | 3.50 (1.53) | 1.85 (0.82) | 2.62 (1.69) |
| Southeast | 3.60 (1.45) | 4.17 (1.33) | 2.26 (1.18) | 3.41 (1.38) | 3.47 (1.49) | 1.75 (0.75) | 2.44 (1.62) |
| South | 3.47 (1.43) | 4.08 (1.30) | 2.36 (1.24) | 3.42 (1.34) | 3.24 (1.48) | 1.74 (0.75) | 2.36 (1.57) |
| Brazil | 3.48 (1.43) | 4.14 (1.32) | 2.24 (1.17) | 3.41 (1.38) | 3.47 (1.51) | 1.78 (0.77) | 2.47 (1.62) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendes, G.F.; Reis, C.E.G.; Nakano, E.Y.; da Costa, T.H.M.; Saunders, B.; Zandonadi, R.P. Translation and Validation of the Caffeine Expectancy Questionnaire in Brazil (CaffEQ-BR). Nutrients 2020, 12, 2248. https://doi.org/10.3390/nu12082248
Mendes GF, Reis CEG, Nakano EY, da Costa THM, Saunders B, Zandonadi RP. Translation and Validation of the Caffeine Expectancy Questionnaire in Brazil (CaffEQ-BR). Nutrients. 2020; 12(8):2248. https://doi.org/10.3390/nu12082248
Chicago/Turabian StyleMendes, Guilherme Falcão, Caio Eduardo Gonçalves Reis, Eduardo Yoshio Nakano, Teresa Helena Macedo da Costa, Bryan Saunders, and Renata Puppin Zandonadi. 2020. "Translation and Validation of the Caffeine Expectancy Questionnaire in Brazil (CaffEQ-BR)" Nutrients 12, no. 8: 2248. https://doi.org/10.3390/nu12082248
APA StyleMendes, G. F., Reis, C. E. G., Nakano, E. Y., da Costa, T. H. M., Saunders, B., & Zandonadi, R. P. (2020). Translation and Validation of the Caffeine Expectancy Questionnaire in Brazil (CaffEQ-BR). Nutrients, 12(8), 2248. https://doi.org/10.3390/nu12082248