Can Nutritional Intervention for Obesity and Comorbidities Slow Down Age-Related Hearing Impairment?

 , ,
, , 
{kind=link}
Abstract
1. Introduction
2. Search Strategy
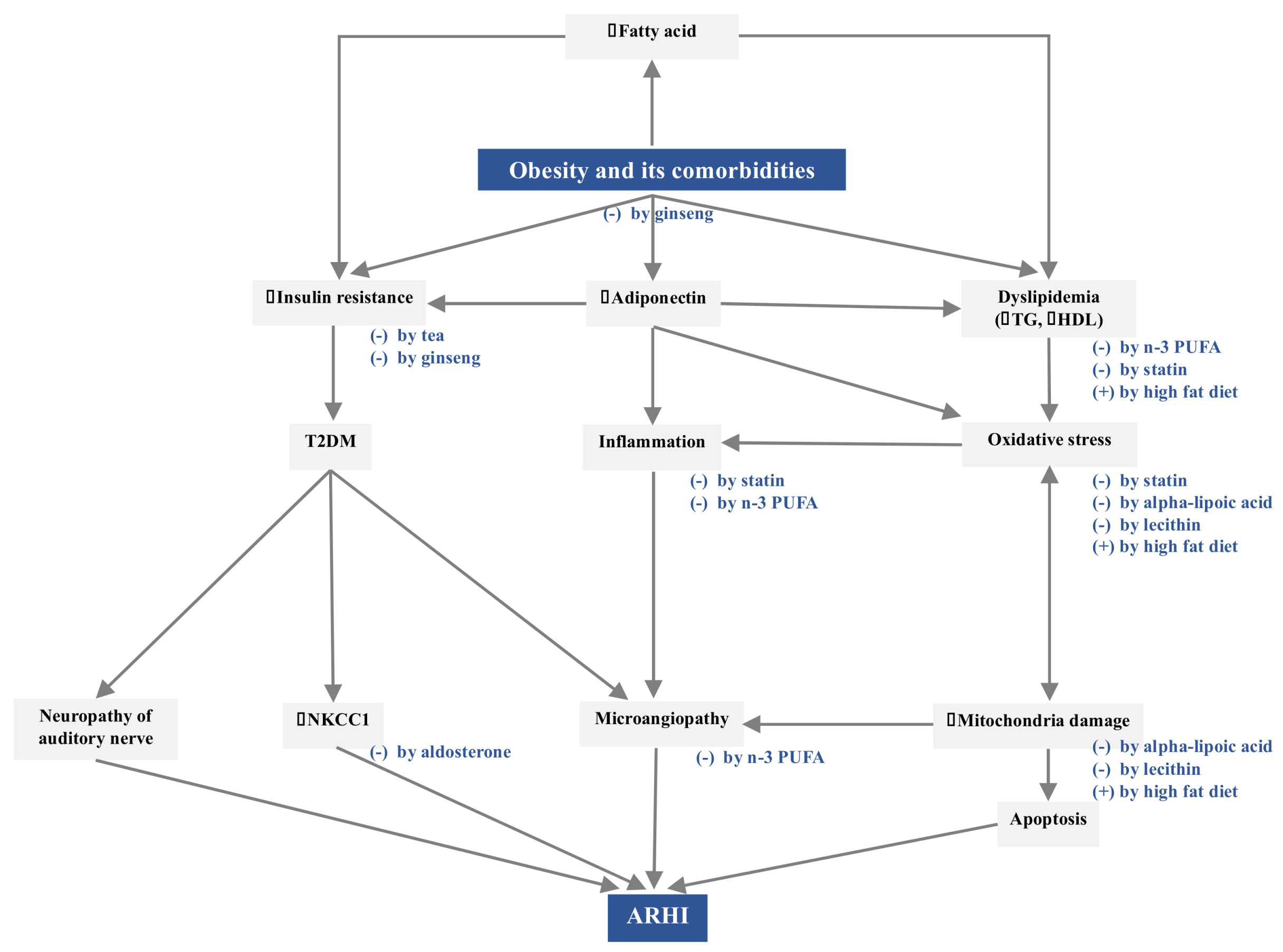
3. Pathogenetic Mechanisms Linking Obesity and Comorbidities to ARHI
3.1. Increased Insulin Resistance
3.2. Decreased Adiponectin Level
3.3. Dyslipidemia
4. Nutritional Interventions for Obesity and Comorbidities against ARHI
4.1. Low-Fat Diet
4.2. Statins
4.3. Aldosterone
4.4. Omega-3 Polyunsaturated Fatty Acids
4.5. Alpha-Lipoic Acid
4.6. Lecithin
4.7. Phytochemicals
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Rosenhall, U. Epidemiology of age related hearing loss. Hear. Balanc. Commun. 2015, 132, 46–50. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Deafness and Hearing Loss; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Lin, F.R.; Niparko, J.K.; Ferrucci, L. Hearing loss prevalence in the united states. Arch. Intern. Med. 2011, 17120, 1851–1853. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Yaffe, K.; Xia, J.; Xue, Q.L.; Harris, T.B.; Purchase-Helzner, E.; Satterfield, S.; Ayonayon, H.N.; Ferrucci, L.; Simonsick, E.M.; et al. Hearing loss and cognitive decline in older adults. JAMA Intern. Med. 2013, 1734, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Metter, E.J.; O’Brien, R.J.; Resnick, S.M.; Zonderman, A.B.; Ferrucci, L. Hearing loss and incident dementia. Arch. Neurol. 2011, 682, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.A.; Victor, C.R.; Vetter, N.J. Hearing difficulty and its psychological implications for the elderly. J. Epidemiol. Community Health 1984, 381, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Pronk, M.; Deeg, D.J.; Smits, C.; van Tilburg, T.G.; Kuik, D.J.; Festen, J.M.; Kramer, S.E. Prospective effects of hearing status on loneliness and depression in older persons: Identification of subgroups. Int. J. Audiol. 2011, 5012, 887–896. [Google Scholar] [CrossRef] [PubMed]
- Genther, D.J.; Frick, K.D.; Chen, D.; Betz, J.; Lin, F.R. Association of hearing loss with hospitalization and burden of disease in older adults. JAMA 2013, 30922, 2322–2324. [Google Scholar] [CrossRef]
- Foley, D.M.; Frick, K.D.; Lin, F.R. Association between hearing loss and healthcare expenditures in older adults. J. Am. Geriatr. Soc. 2014, 626, 1188–1189. [Google Scholar] [CrossRef]
- Nash, S.D.; Cruickshanks, K.J.; Klein, R.; Klein, B.E.; Nieto, F.J.; Huang, G.H.; Pankow, J.S.; Tweed, T.S. The prevalence of hearing impairment and associated risk factors: The beaver dam offspring study. Arch. Otolaryngol. Head Neck Surg. 2011, 1375, 432–439. [Google Scholar] [CrossRef]
- Schuknecht, H.F.; Gacek, M.R. Cochlear pathology in presbycusis. Ann. Otol. Rhinol. Laryngol. 1993, 102, 1–16. [Google Scholar] [CrossRef]
- Seidman, M.D.; Ahmad, N.; Bai, U. Molecular mechanisms of age-related hearing loss. Ageing Res. Rev. 2002, 13, 331–343. [Google Scholar] [CrossRef]
- Puga, A.M.; Pajares, M.A.; Varela-Moreiras, G.; Partearroyo, T. Interplay between nutrition and hearing loss: State of art. Nutrients 2019, 11, 35. [Google Scholar] [CrossRef]
- Van Eyken, E.; Van Camp, G.; Van Laer, L. The complexity of age-related hearing impairment: Contributing environmental and genetic factors. Audiol. Neurotol. 2007, 126, 345–358. [Google Scholar] [CrossRef]
- Hwang, J.H.; Wu, C.C.; Hsu, C.J.; Liu, T.C.; Yang, W.S. Association of central obesity with the severity and audiometric configurations of age-related hearing impairment. Obesity 2009, 17, 1796–1801. [Google Scholar] [CrossRef]
- Croll, P.H.; Voortman, T.; Vernooij, M.W.; Baatenburg de Jong, R.J.; Lin, F.R.; Rivadeneira, F.; Ikram, M.A.; Goedegebure, A. The association between obesity, diet quality and hearing loss in older adults. Aging (Albany NY) 2019, 111, 48–62. [Google Scholar] [CrossRef]
- Frisina, S.T.; Mapes, F.; Kim, S.H.; Frisina, D.R.; Frisina, R.D. Characterization of hearing loss in aged type II diabetics. Hear. Res. 2006, 211, 103–113. [Google Scholar] [CrossRef]
- Meneses-Barriviera, C.L.; Bazoni, J.A.; Doi, M.Y.; De Moraes Marchiori, L.L. Probable association of hearing loss, hypertension and diabetes mellitus in the elderly. Int. Arch. Otorhinolaryngol. 2018, 224, 337–341. [Google Scholar] [CrossRef]
- Duck, S.W.; Prazma, J.; Bennett, P.S.; Pillsbury, H.C. Interaction between hypertension and diabetes mellitus in the pathogenesis of sensorineural hearing loss. Laryngoscope 1997, 10712, 1596–1605. [Google Scholar] [CrossRef]
- Aghazadeh-Attari, J.; Mansorian, B.; Mirza-Aghazadeh-Attari, M.; Ahmadzadeh, J.; Mohebbi, I. Association between metabolic syndrome and sensorineural hearing loss: A cross-sectional study of 11,114 participants. Diabetes Metab. Syndr. Obes. Targets Ther. 2017, 10, 459–465. [Google Scholar] [CrossRef]
- Rosenhall, U.; Sundh, V. Age-related hearing loss and blood pressure. Noise Heal. 2009, 831, 88. [Google Scholar] [CrossRef]
- Dhanda, N.; Taheri, S. A narrative review of obesity and hearing loss. Int. J. Obes. 2017, 417, 1066–1073. [Google Scholar] [CrossRef]
- Khaodhiar, L.; McCowen, K.C.; Blackburn, G.L. Obesity and its comorbid conditions. Clin. Cornerstone 1999, 23, 17–31. [Google Scholar] [CrossRef]
- Boden, G. Obesity and free fatty acids (FFA). Endocrinol. Metab. Clin. N. Am. 2008, 373, 635. [Google Scholar] [CrossRef]
- Friedman, S.A.; Schulman, R.H.; Weiss, S. Hearing and Diabetic Neuropathy. Arch. Intern. Med. 1975, 1354, 573–576. [Google Scholar] [CrossRef]
- Harbawi, A.F.A. The Effect of Diabetes on Hearing Loss. Otol. Neurotol. 2003, 24, 382–386. [Google Scholar]
- Ding, B.; Frisina, R.D.; Zhu, X.; Sakai, Y.; Sokolowski, B.; Walton, J.P. Direct control of Na + -K + -2Cl − -cotransport protein (NKCC1) expression with aldosterone. Am. J. Physiol. Physiol. 2013, 3061, C66–C75. [Google Scholar] [CrossRef]
- Wangemann, P. K+ cycling and the endocochlear potential. Hear. Res. 2002, 165, 1–9. [Google Scholar] [CrossRef]
- Sargeant, R.J.; Liu, Z.; Klip, A. Action of insulin on Na+-K+-ATPase and the Na+-K+-2Cl− cotransporter in 3T3–L1 adipocytes. Am. J. Physiol. 1995, 269, C217–C225. [Google Scholar] [CrossRef]
- Gates, G.A.; Cobb, J.L.; D’Agostino, R.B.; Wolf, P.A. The relation of hearing in the elderly to the presence of cardiovascular disease and cardiovascular risk factors. Arch. Otolaryngol. Head Neck Surg. 1993, 119, 156–161. [Google Scholar] [CrossRef]
- Seidman, M.D.; Quirk, W.S.; Shirwany, N.A. Mechanisms of alterations in the microcirculation of the cochlea. Ann. N. Y. Acad. Sci. 1999, 884, 226–232. [Google Scholar] [CrossRef]
- Tan, T.Y.; Rahmat, O.; Prepageran, N.; Fauzi, A.; Noran, N.H.; Raman, R. Hypertensive retinopathy and sensorineural hearing loss. Indian J. Otolaryngol. Head Neck Surg. 2010, 614, 275–279. [Google Scholar] [CrossRef]
- Turer, A.T.; Scherer, P.E. Adiponectin: Mechanistic insights and clinical implications. Diabetologia 2012, 559, 2319–2326. [Google Scholar] [CrossRef]
- Arita, Y.; Kihara, S.; Ouchi, N.; Takahashi, M.; Maeda, K.; Miyagawa, J.I.; Hotta, K.; Shimomura, I.; Nakamura, T.; Miyaoka, K.; et al. Paradoxical decrease of an adipose-specific protein, adiponectin, in obesity. Biochem. Biophys. Res. Commun. 1999, 257, 79–83. [Google Scholar] [CrossRef]
- Yokota, T.; Oritani, K.; Takahashi, I.; Ishikawa, J.; Matsuyama, A.; Ouchi, N.; Kihara, S.; Funahashi, T.; Tenner, A.J.; Tomiyama, Y.; et al. Adiponectin, a new member of the family of soluble defense collagens, negatively regulates the growth of myelomonocytic progenitors and the functions of macrophages. Blood 2000, 965, 1723–1732. [Google Scholar]
- Berg, A.H.; Combs, T.P.; Scherer, P.E. ACRP30/adiponectin: An adipokine regulating glucose and lipid metabolism. Trends Endocrinol. Metab. 2002, 132, 84–89. [Google Scholar] [CrossRef]
- Yamauchi, T.; Kamon, J.; Waki, H.; Terauchi, Y.; Kubota, N.; Hara, K.; Mori, Y.; Ide, T.; Murakami, K.; Tsuboyama-Kasaoka, N.; et al. The fat-derived hormone adiponectin reverses insulin resistance associated with both lipoatrophy and obesity. Nat. Med. 2001, 78, 941–946. [Google Scholar] [CrossRef]
- Shibata, R.; Sato, K.; Pimentel, D.R.; Takemura, Y.; Kihara, S.; Ohashi, K.; Funahashi, T.; Ouchi, N.; Walsh, K. Adiponectin protects against myocardial ischemia-reperfusion injury through AMPK- and COX-2-dependent mechanisms. Nat. Med. 2005, 1110, 1096–1103. [Google Scholar] [CrossRef]
- Teixeira, A.L.; Diniz, B.S.; Campos, A.C.; Miranda, A.S.; Rocha, N.P.; Talib, L.L.; Gattaz, W.F.; Forlenza, O.V. Decreased levels of circulating adiponectin in mild cognitive impairment and alzheimer’s disease. NeuroMolecular Med. 2013, 151, 115–121. [Google Scholar] [CrossRef]
- Hwang, J.H.; Hsu, C.J.; Liu, T.C.; Yang, W.S. Association of plasma adiponectin levels with hearing thresholds in adults. Clin. Endocrinol. 2011, 755, 614–620. [Google Scholar] [CrossRef]
- Wu, C.C.; Tsai, C.H.; Lu, Y.C.; Lin, H.C.; Hwang, J.H.; Lin, Y.H.; Yang, W.S.; Chen, P.J.; Liao, W.C.; Lee, Y.L.; et al. Contribution of adiponectin and its type 1 receptor to age-related hearing impairment. Neurobiol. Aging 2015, 366, 2085–2093. [Google Scholar] [CrossRef]
- Tanigawa, T.; Shibata, R.; Ouchi, N.; Kondo, K.; Ishii, M.; Katahira, N.; Kambara, T.; Inoue, Y.; Takahashi, R.; Ikeda, N.; et al. Adiponectin deficiency exacerbates age-related hearing impairment. Cell Death Dis. 2014, 5, e1189. [Google Scholar] [CrossRef]
- Ebbert, J.O.; Jensen, M.D. Fat depots, free fatty acids, and dyslipidemia. Nutrients 2013, 52, 495–508. [Google Scholar] [CrossRef]
- Manley, G. Recent advances in the study of age-related hearing loss-A Mini-Review. Gerontology 2013, 712, 233–236. [Google Scholar]
- Martín Villares, C.; San Román Carbajo, J.; Domínguez Calvo, J.; Fernández Pello, M.E.; Pomar Blanco, P.; Tapia Risueño, M. Lipid profile and hearing-loss aged-related. Nutr. Hosp. 2005, 201, 52–57. [Google Scholar]
- Zhao, J.; Zhang, M.; Li, Y.; Zhang, J.; Wang, N.; Yang, X. Association between metabolic syndrome and its components with presbycusis. Wei Sheng Yan Jiu 2015, 444, 538–542. [Google Scholar]
- Guo, Y.; Zhang, C.; Du, X.; Nair, U.; Yoo, T.J. Morphological and functional alterations of the cochlea in apolipoprotein E gene deficient mice. Hear. Res. 2005, 208, 54–67. [Google Scholar] [CrossRef]
- Amiya, E. Interaction of hyperlipidemia and reactive oxygen species: Insights from the lipid-raft platform. World J. Cardiol. 2016, 812, 689. [Google Scholar] [CrossRef]
- Fujimoto, C.; Yamasoba, T. Oxidative stresses and mitochondrial dysfunction in age-related hearing loss. Oxid. Med. Cell Longev. 2014, 2014, 1–6. [Google Scholar] [CrossRef]
- Hwang, J.H.; Chen, J.C.; Hsu, C.J.; Yang, W.S.; Liu, T.C. Plasma reactive oxygen species levels are correlated with severity of age-related hearing impairment in humans. Neurobiol. Aging 2012, 33, 1920–1926. [Google Scholar] [CrossRef]
- Gacek, R.R.; Schuknecht, H.F. Pathology of presbycusis. Int. J. Audiol. 1969, 8, 199–209. [Google Scholar] [CrossRef]
- de Mello, A.H.; Costa, A.B.; Engel, J.D.G.; Rezin, G.T. Mitochondrial dysfunction in obesity. Life Sci. 2018, 192, 26–32. [Google Scholar] [CrossRef]
- Saito, T.; Sato, K.; Saito, H. An experimental study of auditory dysfunction associated with hyperlipoproteinemia. Arch. Otorhinolaryngol. 1986, 243, 242–245. [Google Scholar] [CrossRef]
- Sikora, M.A.; Morizono, T.; Ward, W.D.; Paparella, M.M.; Leslie, K. Diet-induced hyperlipidemia and auditory dysfunction. Acta Otolaryngol. 1986, 102, 372–381. [Google Scholar] [CrossRef]
- Du, Z.; Yang, Y.; Hu, Y.; Sun, Y.; Zhang, S.; Peng, W.; Zhong, Y.; Huang, X.; Kong, W. A long-term high-fat diet increases oxidative stress, mitochondrial damage and apoptosis in the inner ear of d-galactose-induced aging rats. Hear. Res. 2012, 287, 15–24. [Google Scholar] [CrossRef]
- Vasilyeva, O.N.; Frisina, S.T.; Zhu, X.; Walton, J.P.; Frisina, R.D. Interactions of hearing loss and diabetes mellitus in the middle age CBA/CaJ mouse model of presbycusis. Hear. Res. 2009, 249, 44–53. [Google Scholar] [CrossRef]
- Hwang, J.H.; Hsu, C.J.; Yu, W.H.; Liu, T.C.; Yang, W.S. Diet-induced obesity exacerbates auditory degeneration via hypoxia, inflammation, and apoptosis signaling pathways in CD/1 mice. PLoS ONE 2013, 84, e60730. [Google Scholar] [CrossRef]
- Fujita, T.; Yamashita, D.; Uehara, N.; Inokuchi, G.; Hasegawa, S.; Otsuki, N.; Nibu, K.I. A high-fat diet delays age-related hearing loss progression in C57BL/6J mice. PLoS ONE 2015, 101, e0117547. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; Teber, E.; McMahon, C.M.; Mitchell, P. Dietary intake of cholesterol is positively associated and use of cholesterol-lowering medication is negatively associated with prevalent age-related hearing loss. J. Nutr. 2011, 1417, 1355–1361. [Google Scholar] [CrossRef]
- Bonfim, M.R.; Oliveira, A.S.B.; Amaral, S.L.D.; Monteiro, H.L. Treatment of dyslipidemia with statins and physical exercises: Recent findings of skeletal muscle responses. Arq. Bras. Cardiol. 2015, 104, 324–331. [Google Scholar] [CrossRef]
- Syka, J.; Ouda, L.; Nachtigal, P.; Solichová, D.; Semecký, V. Atorvastatin slows down the deterioration of inner ear function with age in mice. Neurosci. Lett. 2007, 4112, 112–116. [Google Scholar] [CrossRef]
- Choudhury, R.P.; Carrelli, A.L.; Stern, J.D.; Chereshnev, I.; Soccio, R.; Elmalem, V.I.; Fallon, J.T.; Fisher, E.A.; Reis, E.D. Effects of simvastatin on plasma lipoproteins and response to arterial injury in wild-type and apolipoprotein-E-deficient mice. J. Vasc. Res. 2004, 411, 75–83. [Google Scholar] [CrossRef]
- John, S.; Schneider, M.P.; Delles, C.; Jacobi, J.; Schmieder, R.E. Lipid-independent effects of statins on endothelial function and bioavailability of nitric oxide in hypercholesterolemic patients. Am. Heart J. 2005, 1493, 473.e1–473.e10. [Google Scholar] [CrossRef]
- Bełtowski, J. Statins and modulation of oxidative stress. Toxicol. Mech. Methods 2005, 152, 61–92. [Google Scholar] [CrossRef]
- Frisina, R.D.; Ding, B.; Zhu, X.; Walton, J.P. Age-related hearing loss: Prevention of threshold declines, cell loss and apoptosis in spiral ganglion neurons. Aging (Albany NY) 2016, 89, 2081–2099. [Google Scholar] [CrossRef]
- Halonen, J.; Hinton, A.S.; Frisina, R.D.; Ding, B.; Zhu, X.; Walton, J.P. Long-term treatment with aldosterone slows the progression of age-related hearing loss. Hear. Res. 2016, 336, 63–71. [Google Scholar] [CrossRef]
- Tadros, S.F.; Frisina, S.T.; Mapes, F.; Frisina, D.R.; Frisina, R.D. Higher serum aldosterone correlates with lower hearing thresholds: A possible protective hormone against presbycusis. Hear. Res. 2005, 209, 10–18. [Google Scholar] [CrossRef]
- Harris, W.S. Alpha-linolenic acid: A gift from the land? Circulation 2005, 11122, 2872–2874. [Google Scholar] [CrossRef][Green Version]
- Pizzini, A.; Lunger, L.; Demetz, E.; Hilbe, R.; Weiss, G.; Ebenbichler, C.; Tancevski, I. The role of omega-3 fatty acids in reverse cholesterol transport: A review. Nutrients 2017, 9, 1099. [Google Scholar] [CrossRef]
- Liew, G.; Wong, T.Y.; Mitchell, P.; Newall, P.; Smith, W.; Wang, J.J. Retinal microvascular abnormalities and age-related hearing loss: The Blue Mountains hearing study. Ear Hear. 2007, 283, 394–401. [Google Scholar] [CrossRef]
- Shen, J.; Bi, Y.L.; Das, U.N. Potential role of polyunsaturated fatty acids in diabetic retinopathy. Arch. Med. Sci. 2014, 10, 1167–1174. [Google Scholar] [CrossRef]
- Curhan, S.G.; Eavey, R.D.; Wang, M.; Rimm, E.B.; Curhan, G.C. Fish and fatty acid consumption and the risk of hearing loss in women. Am. J. Clin. Nutr. 2014, 100, 1371–1377. [Google Scholar] [CrossRef]
- Martínez-Vega, R.; Partearroyo, T.; Vallecillo, N.; Varela-Moreiras, G.; Pajares, M.A.; Varela-Nieto, I.; Gopinath, J. Long-term omega-3 fatty acid supplementation prevents expression changes in cochlear homocysteine metabolism and ameliorates progressive hearing loss in C57BL/6J mice. Nutr. Biochem. 2015, 2612, 1424–1433. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; Rochtchina, E.; McMahon, C.M.; Mitchell, P. Consumption of omega-3 fatty acids and fish and risk of age-related hearing loss. Am. J. Clin. Nutr. 2010, 922, 416–421. [Google Scholar] [CrossRef]
- Dullemeijer, C.; Verhoef, P.; Brouwer, I.A.; Kok, F.J.; Brummer, R.J.M.; Durga, J. Plasma very long-chain n-3 polyunsaturated fatty acids and age-related hearing loss in older adults. J. Nutr. Heal. Aging 2010, 145, 347–351. [Google Scholar] [CrossRef]
- Seidman, M.D.; Khan, M.; Bai, U.; Shirwany, N.; Quirk, W. Biologic activity of mitochondrial metabolites on aging and age-related hearing loss. Am. J. Otolaryngol. 2005, 212, 161–167. [Google Scholar] [CrossRef]
- Li, X.Z.; Park, B.K.; Hong, B.C.; Ahn, J.S.; Shin, J.S. Effect of soy lecithin on total cholesterol content, fatty acid composition and carcass characteristics in the Longissimus dorsi of Hanwoo steers (Korean native cattle). Anim. Sci. J. 2017, 886, 847–853. [Google Scholar] [CrossRef]
- Seidman, M.D.; Khan, M.J.; Tang, W.X.; Quirk, W.S. Influence of lecithin on mitochondrial DNA and age-related hearing loss. Otolaryngol. Head Neck Surg. 2002, 1273, 138–144. [Google Scholar] [CrossRef]
- Castaneda, R.; Natarajan, S.; Jeong, S.Y.; Hong, B.N.; Kang, T.H. Traditional oriental medicine for sensorineural hearing loss: Can ethnopharmacology contribute to potential drug discovery? J. Ethnopharmacol. 2019, 231, 409–428. [Google Scholar] [CrossRef]
- Hwang, J.H.; Chan, Y.C.; Hsu, C.J.; Liu, T.C.; Chen, J.C. Effects of tea drinking on auditory functions in aged subjects. J. Nutr. Health Aging 2012, 163, 252–256. [Google Scholar] [CrossRef]
- Hosoda, K.; Wang, M.F.; Liao, M.L.; Chuang, C.K.; Iha, M.; Clevidence, B.; Yamamoto, S. Antihyperglycemic effect of oolong tea in type 2 diabetes. Diabetes Care 2003, 26, 1714–1718. [Google Scholar] [CrossRef]
- Broadhurst, C.L.; Polansky, M.M.; Anderson, R.A. Insulin-like biological activity of culinary and medicinal plant aqueous extracts in vitro. J. Agric. Food Chem. 2000, 483, 849–852. [Google Scholar] [CrossRef]
- Tian, C.; Kim, Y.J.; Lim, H.J.; Kim, Y.S.; Park, H.Y.; Choung, Y.H. Red ginseng delays age-related hearing and vestibular dysfunction in C57BL/6 mice. Exp. Gerontol. 2014, 57, 224–232. [Google Scholar] [CrossRef]
- Hong, B.N.; Ji, M.G.; Kang, T.H. The efficacy of red ginseng in type 1 and type 2 diabetes in animals. Evid. Based Complement Alternat. Med. 2013, 2013, 593181. [Google Scholar] [CrossRef]
- Zhang, L.; Virgous, C.; Si, H. Ginseng and obesity: Observations and understanding in cultured cells, animals and humans. J. Nutr. Biochem. 2017, 44, 1–10. [Google Scholar] [CrossRef]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, T.-H.; Hwang, J.-H.; Yang, T.-H.; Hsu, C.-J.; Wu, C.-C.; Liu, T.-C. Can Nutritional Intervention for Obesity and Comorbidities Slow Down Age-Related Hearing Impairment? Nutrients 2019, 11, 1668. https://doi.org/10.3390/nu11071668
Tang T-H, Hwang J-H, Yang T-H, Hsu C-J, Wu C-C, Liu T-C. Can Nutritional Intervention for Obesity and Comorbidities Slow Down Age-Related Hearing Impairment? Nutrients. 2019; 11(7):1668. https://doi.org/10.3390/nu11071668
Chicago/Turabian StyleTang, Ting-Hsuan, Juen-Haur Hwang, Ting-Hua Yang, Chuan-Jen Hsu, Chen-Chi Wu, and Tien-Chen Liu. 2019. "Can Nutritional Intervention for Obesity and Comorbidities Slow Down Age-Related Hearing Impairment?" Nutrients 11, no. 7: 1668. https://doi.org/10.3390/nu11071668
APA StyleTang, T.-H., Hwang, J.-H., Yang, T.-H., Hsu, C.-J., Wu, C.-C., & Liu, T.-C. (2019). Can Nutritional Intervention for Obesity and Comorbidities Slow Down Age-Related Hearing Impairment? Nutrients, 11(7), 1668. https://doi.org/10.3390/nu11071668