2.1. Study Design
This was a double-blind, randomized, feeding-controlled, cross-over clinical trial (Registration number: NCT02197910), carried out in a group of pre-hypertensive adult volunteers (130 mmHg < systolic BP (SBP) ≤139 mmHg and 85 mmHg < diastolic BP (DBP) ≤89 mmHg) at moderately increased estimated cardiovascular risk (ESH charts) [
11], consecutively enrolled in the ambulatory service of cardiovascular disease prevention of the Medical and Surgical Sciences Department, University of Bologna.
Patients with known primitive or white coat hypertension, obesity (body mass index (BMI) >25 kg/m2), diabetes mellitus, personal history of atherosclerosis-related cardiovascular diseases (coronary artery disease, cerebrovascular disease, ultrasound diagnosed carotid atherosclerosis), known active thyroid disorders, renal failure or chronic liver disease and subjects consuming drugs, botanical extracts or other dietary supplements potentially affecting BP were excluded from the study as well as subjects with gastrointestinal disease (e.g., celiac disease) that could cause problems in the absorption of bioactive peptides.
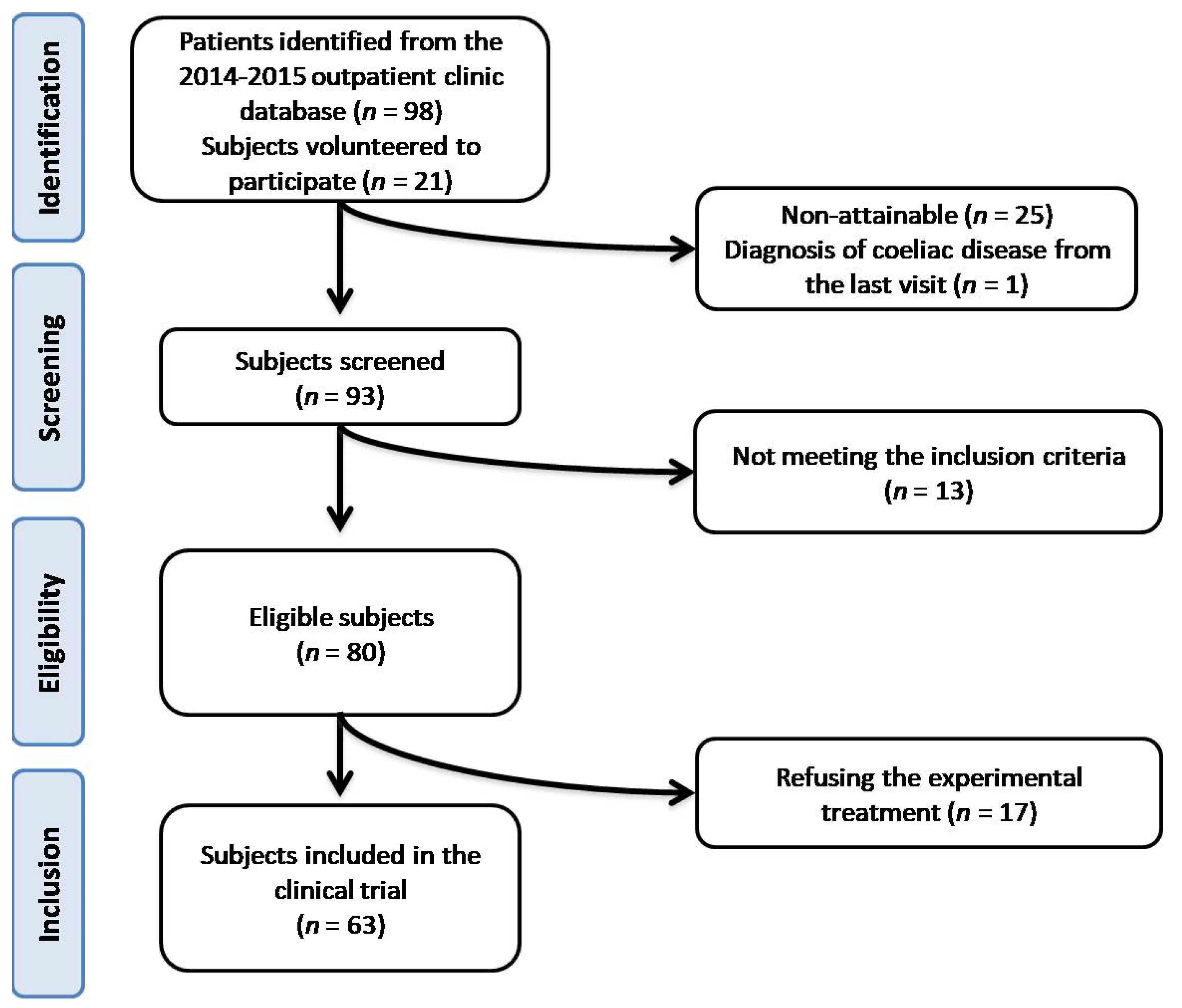
After retrospectively evaluated 3212 patients from the 2014–2015 outpatient clinic database, we indirectly identified 98 potentially recruitable subjects. In addition, 21 subjects from the hospital personnel were offered voluntarily to participate. Firstly, we selected 93 eligible subjects: among them, 13 patients were excluded at the screening visit because the inclusion criteria was not met and 17 subjects refused to give their informed consent to the treatment. At the end, 63 subjects were selected and enrolled (
Figure 1).
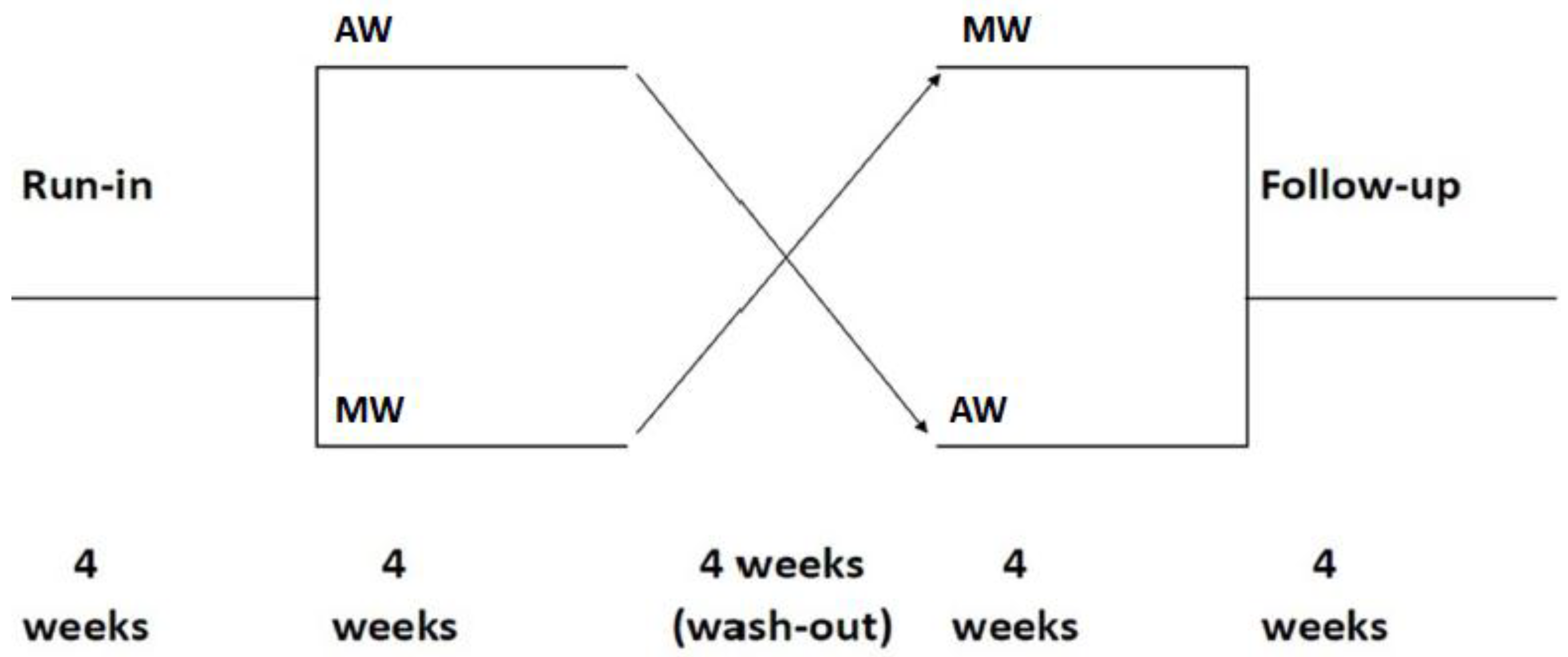
Participants were adhering to a standardized diet for four weeks before being randomly assigned to complete one of two treatment sequences by consuming a prescribed quantity of tested products for a four-week period, followed by a four-week washout before the cross-over to the second treatment. Finally, they were asked to return for a follow-up visit at four weeks, in order to evaluate the reversibility of the eventual bioactive peptide effect after suspension (
Figure 2).
During the period of diet standardization, patients were given standard behavioral and qualitative dietary suggestion to correct their lifestyle habits. In particular, they were instructed to follow the general indications of a Mediterranean diet (avoiding an excessive intake of dairy and red-meat-derived products), to increase their daily intake of vegetables and not to add salt to fresh and cooked food. They were also recommended to increase their physical activity by walking briskly or cycling 3–5 times per week for at least 20–30 min each time. Thereafter, subjects were asked to maintain constant their habits for the entire duration of the trial, in order to reduce the studied parameters’ variability related to any dietary excesses. In particular, it was asked to the enrolled volunteers to maintain a constant intake of fruits, vegetables, olive oil and wine, in order to reduce the variability in the dietary content of fibers and polyphenols. Nutrient intake was estimated from the 4 days records before the randomization and towards the end of each intervention period. The nutritional evaluation was performed by an expert nutritionist biologist with Software MètaDieta® (Meteda S.r.l., San Benedetto del Tronto, Italy) using Italian Food Composition databases. Compliance with the dietary instructions was further verified by the evaluation of 24 h urinary sodium, as biomarker of salt intake.
Randomization was done by an independent statistician using a specific software. The statistician prepared envelopes containing randomization codes to assign in a progressive way to enroll subjects. All participants, study staffs and data analysis were blinded to the group assignment. A copy of the codes was provided only to the person responsible for performing the statistical analysis.
Throughout the study, we instructed patients to take the first quantity of pasta on the day after they received it in a blinded box. All unused foodstuffs were retrieved for inventory. Product compliance was assessed by counting the number of packaged foodstuffs returned at the time of specified clinic visits. The acceptability of the tested products was assessed by a visual analogue scale.
The present study was fully conducted in accordance with the Declaration of Helsinki, its protocol was approved by the Ethical Committee of the University of Bologna (Code: BACCHUS_Unibo, Bologna, Italy) and a written informed consent was obtained from all patients before they were included in the trial. The trial was registered on
www.clinicaltrial.gov (Code: NCT02197910) as well.
2.2. Wheat Products
The intervention was carried out using wheat products containing different quantities of nsLTP2 (kindly provided by Kamut Enterprises of Europe (KEE), Oudenaarde, Belgium), which appeared and tasted the same. During the treatment periods, volunteers consumed pasta, bread, and crisp toasts naturally containing a low or a high dose of nsLTP2, substituting the amount of usually consumed foodstuff with the ones provided for the study. The experimental ancient wheat utilized in the present study was organic KAMUT® khorasan wheat (Triticum turgidum subsp. turanicum), while a mix of organic modern commercial durum (T. durum) varieties and soft wheat (T. aestivum) were used as nsLTP2 low dose wheat. KAMUT® khorasan (Oudenaarde, Belgium) is characterized by a particularly high content in nsLTP2 compared to the modern wheat.
KAMUT® is a registered trademark of Kamut International, Ltd. and Kamut Enterprises of Europe and guarantees the wheat is pure ancient khorasan wheat and is organically grown and processed.
According to the procedure reported by Bosi et al. (2018), [
10] the nsLTP2 content was quantified by high performance liquid chromatography-ultraviolet (HLPC-UV)/nano-liquid chromatography-nano-electrospray-ionisation quadrupole time-of-flight (ESI-QTOF) mass spectrometry, in both foodstuffs composed by modern wheat and KAMUT
® khorasan wheat. Assuming a mean daily consumption of 100 g of pasta, 100 g of matzo bread and 40 g of crispy, volunteers under modern wheat and KAMUT
® khorasan wheat diet assumed respectively 20.5 and 41.0 mg peptide per day.
The total phenolic compounds contained in the tested products was also estimated based on their content in the flours. Total phenolic compounds were extracted as previously described by Dinelli et al. [
12]. One gram of whole grain flours was extracted with cold 80% ethanol (4 °C) to dissolve the free soluble compounds, followed by acid and alkaline hydrolyses to release the bound forms. The free and bound extracts were pooled together, evaporated to dryness, and reconstituted to a final concentration of 10 mg/mL in pure methanol. The extracts were filtered through a 0.22 mm filter and stored at −20 °C until analysis.
The 2,2-diphenyl-1-picrylhydrazyl (DPPH) assay was carried out according to the procedure described by Floegel et al. [
13]. Briefly, a solution of 1 mM DPPH in 80%
v/
v methanol was prepared. Absorbance of the solution was adjusted to 0.65 ± 0.02 arbitrary units (AU) at 517 nm using fresh 80%
v/
v methanol. Subsequently, 50 mL of free and bound extract were mixed with 2.95 mL of DPPH solution and incubated for 30 min in the dark at room temperature. The absorbance at 517 nm was monitored for each sample, along with control against a blank of pure methanol. A calibration curve of Trolox (0–500 mg/L) was performed as a function of the percentage of DPPH radical scavenging activity and the final results expressed as micromoles of Trolox equivalents (TE) per gram of whole wheat flour (mmol TE/g). The Fluorescence Recovery After Photobleaching (FRAP) test was carried out according to Benzie and Strain [
14] with some modifications. The FRAP working solution (WS) was prepared freshly as a mixture of 300 mM acetate buffer pH 3.6 (containing 3.1 g of sodium acetate trihydrate and 16 mL glacial acetic acid), 10 mM TPTZ (in 40 mmol/L HCl), and 20 mM ferric chloride (10:1:1,
v:
v:
v). Eighty microliters of diluted (1:1,
v/
v) free and bound phenolic extracts were mixed with 2.4 mL of WS and the absorbance was measured at 593 nm after 1 h in darkness. Absorbance values were compared with those of ferrous sulphate (FeSO
4·7H
2O) (0–1000 mmol/L) and results expressed as mmol Fe
2+ per 100 g of flour. Each measurement was performed in triplicate.
All transformation preparation procedures were identical for both ancient and modern wheat products. Other cereals were excluded from the diet and replaced by either the ancient or modern wheat products during the intervention phases. The food products were packaged with no labels attached to the packages.
2.3. Assessments
2.3.1. Clinical Data and Anthropometric Measurements
Patients were evaluated by the execution of blood and vascular tests at enrolment and at each control. Each visit included standardized questionnaires updating of personal anamnesis (with specific attention to dietary habit assessment, smoking status, and pharmacological treatments) and a physical examination with anthropometric data collection (height, weight, waist, and hip circumference). Height and body weight were measured by standard procedures to the nearest 0.1 cm and 0.1 kg, respectively, with subjects standing erect with eyes directed straight ahead, wearing light clothes, and with bare feet. Waist circumference (WC) was measured at the end of a normal expiration, in a horizontal plane at the midpoint between the inferior margin of the last rib and the superior iliac crest. Instrumental variables investigated were BP, 24 h ambulatory blood pressure monitoring (ABPM), endothelial function, arterial stiffness, and related parameters.
2.3.2. Blood Pressure Measurement
BP was measured from the right upper arm, in the sitting position and after a 10-min rest in a quiet room. Measurements (obtained early in the morning) were performed using a standard mercury sphygmomanometer (Erkameter 3000, ERKA, Bad Tolz, Germany; Korotkoff I and V) and cuffs of appropriate size and snug fit. To implement detection’s accuracy, the average between three successive BP readings (each one obtained at a 1 min interval) was considered as study-variable. Mean pulse pressure (PP) was calculated as the difference between systolic (SBP) and diastolic blood pressure (DBP) (PP = SBP − DBP). Mean arterial pressure (MAP) was obtained by adding one-third of PP to DBP (MAP = ⅓PP + DBP) [
11].
2.3.3. 24 h Ambulatory Blood Pressure Monitoring (ABPM)
ABPM was performed for 24 h, using a noninvasive automatic monitor (model 90207; Space Labs, Redmond, WA, USA). For ABPM, patients were given instruction about how to normally act and work between 06:00 and 22:00 and rest or sleep between 22:00 and 06:00, without taking any drug or xanthine rich beverages (coffee, tea, and energy drinks), which could potentially affect their BP level.
Readings were automatically obtained at 15 min intervals throughout a 24 h study period. Separate averages were taken into consideration for 24 h daytime (06:00–22:00) and nighttime (22:00–06:00) values. The accuracy of the automatic BP readings were checked twice for each ABPM and compared to the manual readings, which were taken using a standard mercury sphygmomanometer. BP was measured by the same operator, from the right upper arm, with the patient in a sitting position, and after a 5-min rest period before the beginning of the ABPM. Three readings were obtained and averaged. The accuracy test was repeated after the end of each 24 h ABPM. Patients with more than 5 mmHg difference in SBP between the manual and automatic readings were excluded from further analysis. All sampled records were blindly decoded by a trained physician [
11].
2.3.4. Pulse Wave Velocity and Related Measures
Arterial stiffness parameters and endothelial function were assessed using the Vicorder
® apparatus (Skidmore Medical Ltd, Bristol, UK), a validated cuff-based device that estimates central BP using a brachial-to-aortic transfer function. Pulse wave velocity (PWV) consists in the measurement of the pulse wave transmission through the arteries and it is considered a reliable and early marker of arterial stiffness as well as a strong predictor of cardiovascular risk [
15]. Theoretical basis of PWV are explained with the Moens–Kortewe equation [
16], while in clinical practice PWV is calculated as the length between two measurement sites divided by the time the pulse wave takes to cover that distance (m/s) [
17]. Augmentation Index (AIx) is obtained through the BP waveform analysis. It represents, as well as PWV, a measure of wave reflection and arterial stiffness and a marker of cardiovascular risk [
18]. It is calculated as the ratio of the pressure increment caused by the reflected wave (augmented pressure) to the pulse pressure [
19]. Pulse Wave Analysis, from which AIx is obtained, is recorded simply with a brachial cuff placed at the right arm of the subjects: the Vicorder
® apparatus registers the radial pressure and with a specific algorithm derives the central BP curve. PWV is calculated with a simultaneous measurement of carotid and femoral BP. A small neck pad containing a photoplethysmographic sensor is placed around the neck and a normal cuff is positioned around the thigh of the patient. The distance between the suprasternal notch and the thigh cuff is measured with a measuring tape. This length represents the distance covered by the pulse wave in its carotid–femoral path and it is used by the Vicorder
® apparatus to establish the PWV value [
20,
21]. The Vicorder
® apparatus guarantees a very good intra- and interoperator reliability [
22].
2.3.5. Endothelial Function
Endothelial function was evaluated though the Endocheck
® (BC Biomedical Laboratories Ltd, Vancouver, BC, Canada), a method embedded within the Vicorder
® device, which is supposed to record brachial pulse volume (PV) waveforms, at baseline and during reactive hyperemia. Reactive hyperemia usually is provoked through PV displacement, obtained by inflating a cuff positioned distally around the forearm. After a 10 min rest, brachial BP is evaluated and PV waveforms are recorded at the baseline for 10 s. Then, the cuff is inflated to 200 mmHg for 5 min and PV waveforms are recorded for 3 min after cuff released. PV displacement is, then, calculated as a percent change in the PV waveform area, comparing waveforms before and during hyperemia through the equation:
where PV
1 represents PV at the baseline and PV
2 represents PV during hyperemia [
23].
2.3.6. Laboratory Data
All measurements were centrally performed in the laboratory of our department. The biochemical analysis were carried out on venous blood and all subjects had fasted for at least 12 h at the time of sampling. Plasma used was obtained by addition of Disodium ethylenediaminetetraacetate dehydrate (Na
2EDTA) (1 mg/mL) and centrifuged at 3000×
g for 15 min at 25 °C. Trained personnel performed laboratory analysis according to standardized methods [
24], immediately after centrifugation, evaluating total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), apolipoprotein B (apoB), apolipoprotein A1 (apoA1), fasting plasma glucose (FPG), creatinine, liver transaminases and creatinine phosphokinase (CPK). At the end of the first visit, participants were given two three-liter plastic bottles and standardized instructions on how to collect urine. They were asked to first empty their bladder, discard the urine and write down the time (start of the collection). The end of the collection was determined by the last urine void in the study center at the second visit or, if not possible, by the time of the last void. Participants were asked whether any collection of urine was lost or forgotten. Then the sodium content was measured with standardized methods.
2.3.7. Statistical Analyses
Sample size was calculated for the primary endpoint of the study (improvement in endothelial reactivity). Considering a Type I error of 0.05 and a power of 0.80 and expecting a minimum pulse volume change improvement of 3.3% with a SD of 5.5%, and considering a drop-out rate of 10%, we calculated to enroll at least 61 patients (to be treated with both tested foodstuffs in the context of a crossover trial). Data were analyzed using intention to treat by means of the Statistical Package for Social Science (SPSS) version 21.0 (IBM Corporation, Armonk, NY, USA) for Windows. Normally distributed baseline characteristics of the population were described by using independent T-test and χ2 test (Fisher corrected for categorical variables). Two-way analysis of variance for crossover design were used in order to assess the treatment effect during the use of low or high nsLPT2. Given their not normal distribution, total polyphenol content and antioxidant activities of the tested ancient and modern wheats were compared using non parametric analysis of variance (Kruskal‒Wallis test) followed by Mann‒Whitney-U. All data were expressed as mean ± standard deviation (SD). To verify the basic assumptions of crossover design, besides the evaluation of period effect, the presence of a carryover effect was excluded. A P-value of 0.05 was considered significant for all tests.

 ,
, 







{kind=link}
{kind=link}