
_Rachiotis.png)
Antifungal Agents in the 21st Century: Advances, Challenges, and Future Perspectives

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Mechanisms of Action and Pharmacodynamics
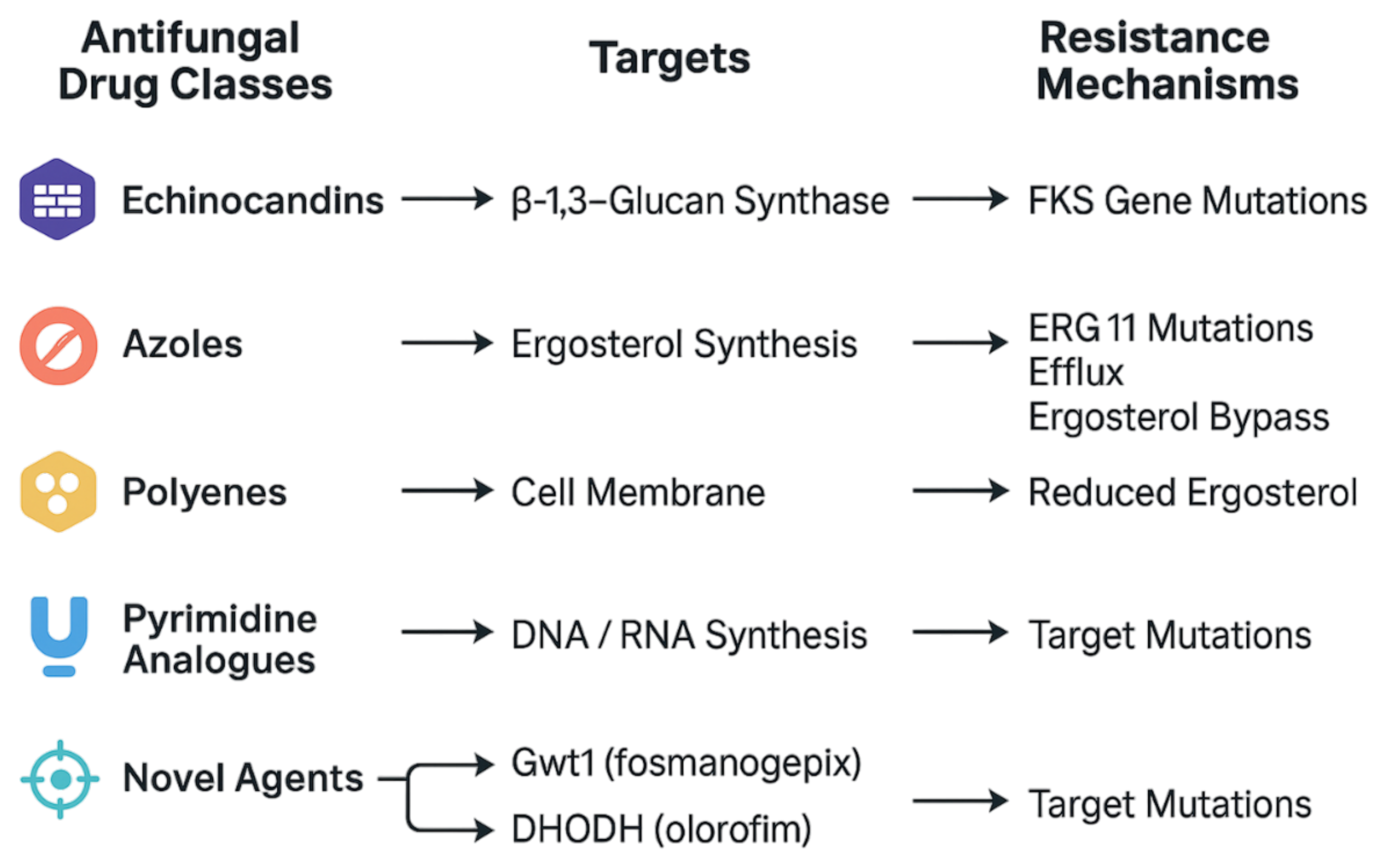
2.1. Main Classes of Antifungals and Their Targets
2.2. Principles of PK/PD Applied to Antifungals
3. Antifungal Resistance
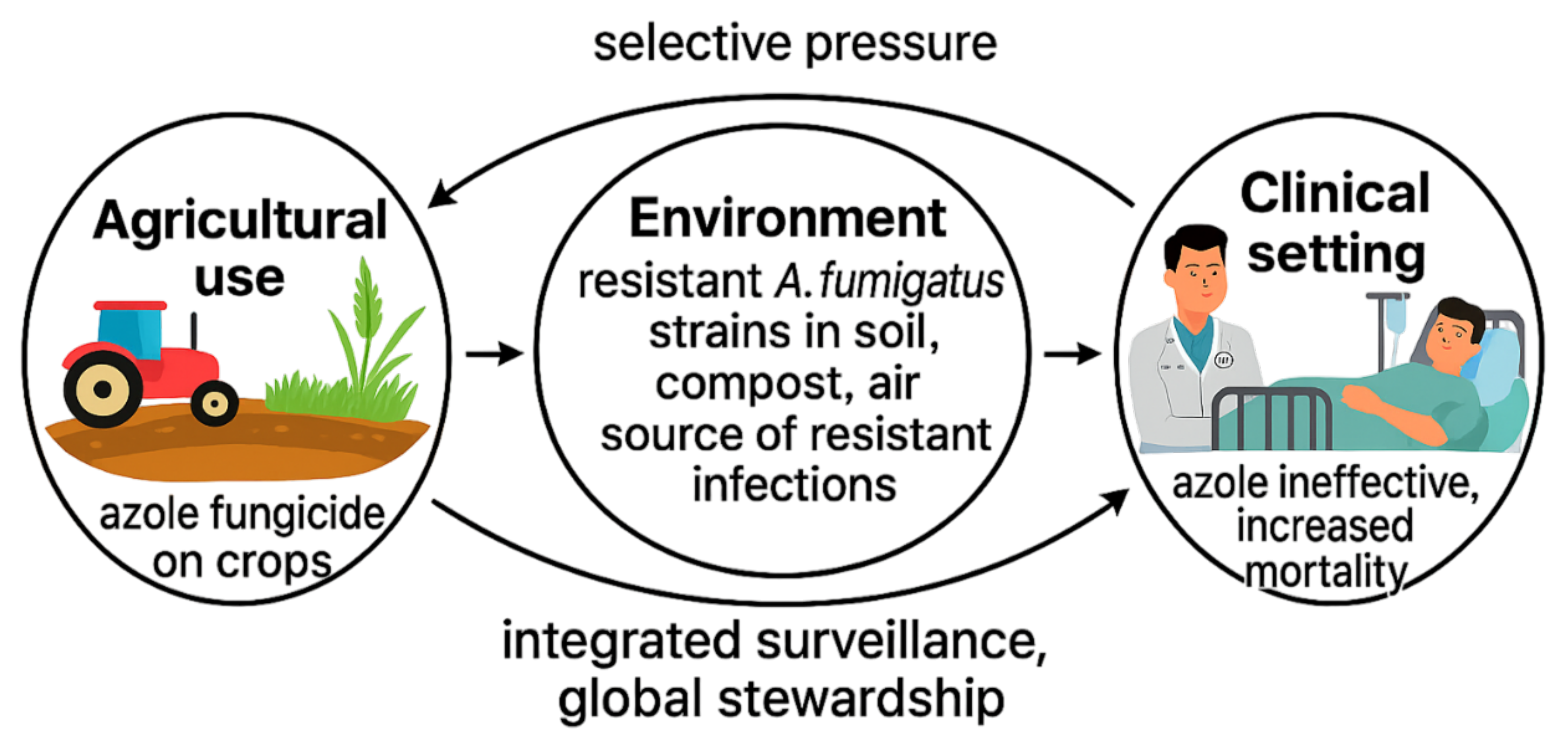
Epidemiology and Global Distribution
4. Clinical Applications
5. Challenges and Future Prospects
5.1. Limitations of Current Antifungal Therapy
5.2. Innovations and Future Directions in Antifungal Therapy
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zhang, Z.; Bills, G.F.; An, Z. Advances in the treatment of invasive fungal disease. PLoS Pathog. 2023, 19, e1011322. [Google Scholar] [CrossRef]
- Ramos, J.T.; Romero, C.A.; Belda, S.; Candel, F.J.; Gallego, B.C.; Fernández-Polo, A.; Antolín, L.F.; Colino, C.G.; Navarro, M.L.; Neth, O.; et al. Clinical practice update of antifungal prophylaxis in immunocompromised children. Rev. Española Quimioter. 2019, 32, 410. [Google Scholar]
- Casalini, G.; Giacomelli, A.; Ridolfo, A.; Gervasoni, C.; Antinori, S. Invasive fungal infections complicating COVID-19: A narrative review. J. Fungi 2021, 7, 921. [Google Scholar] [CrossRef]
- Casalini, G.; Giacomelli, A.; Antinori, S. The WHO fungal priority pathogens list: A crucial reappraisal to review the prioritisation. Lancet Microbe 2024, 5, 717–724. [Google Scholar] [CrossRef]
- Rodrigues, M.L.; Nosanchuk, J.D. Fungal diseases as neglected pathogens: A wake-up call to public health officials. In Advances in Clinical Immunology, Medical Microbiology, COVID-19, and Big Data; Jenny Stanford Publishing: Singapore, 2021; pp. 399–411. [Google Scholar]
- Rayens, E.; Norris, K.A. Prevalence and healthcare burden of fungal infections in the United States, 2018. In Open Forum Infectious Diseases; Oxford University Press US: Cary, NC, USA, 2022; Volume 9, p. ofab593. [Google Scholar]
- Denning, D.W. Global incidence and mortality of severe fungal disease. Lancet Infect. Dis. 2024, 24, e428–e438. [Google Scholar] [CrossRef] [PubMed]
- Benedict, K.; Whitham, H.K.; Jackson, B.R. Economic burden of fungal diseases in the United States. In Open Forum Infectious Diseases; Oxford University Press US: Cary, NC, USA, 2022; Volume 9, p. ofac097. [Google Scholar]
- CDC. Data and Statistics on Fungal Diseases. Available online: https://www.cdc.gov/fungal/data-research/facts-stats/index.html (accessed on 25 April 2025).
- New York Post. Dangerous Fungus Spreading in US Hospitals Has ‘Rapidly Increased’. Available online: https://nypost.com/2025/03/28/health/dangerous-fungus-spreading-in-us-hospitals-has-rapidly-increased/ (accessed on 25 April 2025).
- Time. Deadly Fungal Infections in U.S. Hospitals Are Up 95%. Available online: https://time.com/6264661/fungal-infection-candida-auris-hospitals/ (accessed on 25 April 2025).
- Pallotta, F.; Viale, P.; Barchiesi, F. Candida auris: The new fungal threat. Infez. Med. 2023, 31, 323. [Google Scholar] [PubMed]
- Geremia, N.; Brugnaro, P.; Solinas, M.; Scarparo, C.; Panese, S. Candida auris as an emergent public health problem: A current update on European outbreaks and cases. Healthcare 2023, 11, 425. [Google Scholar] [CrossRef]
- Shelton, J.M.; Rhodes, J.; Uzzell, C.B.; Hemmings, S.; Brackin, A.P.; Sewell, T.R.; Alghamdi, A.; Dyer, P.S.; Fraser, M.; Borman, A.M.; et al. Citizen science reveals landscape-scale exposures to multiazole-resistant Aspergillus fumigatus bioaerosols. Sci. Adv. 2023, 9, eadh8839. [Google Scholar] [CrossRef] [PubMed]
- Seidel, D.; Wurster, S.; Jenks, J.D.; Sati, H.; Gangneux, J.P.; Egger, M.; Alastruey-Izquierdo, A.; Ford, N.P.; Chowdhary, A.; Sprute, R.; et al. Impact of climate change and natural disasters on fungal infections. Lancet Microbe 2024, 5, e594–e605. [Google Scholar] [CrossRef]
- Robbins, N.; Wright, G.D.; Cowen, L.E. Antifungal drugs: The current armamentarium and development of new agents. Microbiol. Spectr. 2016, 4, 10–1128. [Google Scholar] [CrossRef]
- Steimbach, L.M.; Tonin, F.S.; Virtuoso, S.; Borba, H.H.; Sanches, A.C.; Wiens, A.; Fernandez-Llimós, F.; Pontarolo, R. Efficacy and safety of amphotericin B lipid-based formulations—A systematic review and meta-analysis. Mycoses 2017, 60, 146–154. [Google Scholar] [CrossRef]
- Balcerek, M.I.; Stewart, A.G.; Chapman, P.; Lazarus, S. Reducing the off-target endocrinologic adverse effects of azole antifungals—Can it be done? Int. J. Antimicrob. Agents 2022, 59, 106587. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Vermes, A.; Guchelaar, H.J.; Dankert, J. Flucytosine: A review of its pharmacology, clinical indications, pharmacokinetics, toxicity and drug interactions. J. Antimicrob. Chemother. 2000, 46, 171–179. [Google Scholar] [CrossRef]
- Haghani, I.; Babaie, M.; Hoseinnejad, A.; Rezaei-Matehkolaei, A.; Mofarrah, R.; Yahyazadeh, Z.; Kermani, F.; Javidnia, J.; Shokohi, T.; Azish, M.; et al. High prevalence of Terbinafine Resistance among Trichophyton mentagrophytes/T. Interdigitale Species Complex, a cross-sectional study from 2021 to 2022 in Northern Parts of Iran. Mycopathologia 2024, 189, 52. [Google Scholar] [CrossRef] [PubMed]
- Lepak, A.J.; Andes, D.R. Antifungal pharmacokinetics and pharmacodynamics. Cold Spring Harb. Perspect. Med. 2015, 5, a019653. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.E. Current concepts in antifungal pharmacology. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2011; Volume 86, pp. 805–817. [Google Scholar]
- Bellmann, R.; Smuszkiewicz, P. Pharmacokinetics of antifungal drugs: Practical implications for optimized treatment of patients. Infection 2017, 45, 737–779. [Google Scholar] [CrossRef] [PubMed]
- Theuretzbacher, U. Pharmacokinetics/pharmacodynamics of echinocandins. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 805–812. [Google Scholar] [CrossRef]
- Cowen, L.E.; Sanglard, D.; Howard, S.J.; Rogers, P.D.; Perlin, D.S. Mechanisms of antifungal drug resistance. Cold Spring Harb. Perspect. Med. 2015, 5, a019752. [Google Scholar] [CrossRef]
- Balkis, M.M.; Leidich, S.D.; Mukherjee, P.K.; Ghannoum, M.A. Mechanisms of fungal resistance: An overview. Drugs 2002, 62, 1025–1040. [Google Scholar] [CrossRef]
- De Francesco, M.A. Drug-resistant Aspergillus spp.: A literature review of its resistance mechanisms and its prevalence in Europe. Pathogens 2023, 12, 1305. [Google Scholar] [CrossRef]
- Szymański, M.; Chmielewska, S.; Czyżewska, U.; Malinowska, M.; Tylicki, A. Echinocandins–Structure, mechanism of action and use in antifungal therapy. J. Enzym. Inhib. Med. Chem. 2022, 37, 876–894. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.K.; Wang, T.; Mann, A.; Piguet, V.; Chowdhary, A.; Bakotic, W.L. Mechanisms of resistance against allylamine and azole antifungals in Trichophyton: A renewed call for innovative molecular diagnostics in susceptibility testing. PLoS Pathog. 2025, 21, e1012913. [Google Scholar] [CrossRef] [PubMed]
- Pemán, J.; Cantón, E.; Espinel-Ingroff, A. Antifungal drug resistance mechanisms. Expert Rev. Anti-Infect. Ther. 2009, 7, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Hui, S.T.; Gifford, H.; Rhodes, J. Emerging antifungal resistance in fungal pathogens. Curr. Clin. Microbiol. Rep. 2024, 11, 43–50. [Google Scholar] [CrossRef]
- Casadevall, A. Fungal diseases in the 21st century: The near and far horizons. Pathog. Immun. 2018, 3, 183. [Google Scholar] [CrossRef]
- Osaigbovo, I.I.; Ekeng, B.E.; Davies, A.A.; Ebeigbe, E.; Bongomin, F.; Kanyua, A.; Revathi, G.; Oladele, R.O. Candida auris: A systematic review of a globally emerging fungal pathogen in Africa. In Open Forum Infectious Diseases; Oxford University Press US: Cary, NC, USA, 2024; Volume 11, p. ofad681. [Google Scholar]
- CDC. Increasing Threat of Spread of Antimicrobial-Resistant Fungus in Healthcare Facilities. Available online: https://www.cdc.gov/media/releases/2023/p0320-cauris.html (accessed on 27 April 2025).
- Perlin, D.S.; Rautemaa-Richardson, R.; Alastruey-Izquierdo, A. The global problem of antifungal resistance: Prevalence, mechanisms, and management. Lancet Infect. Dis. 2017, 17, e383–e392. [Google Scholar] [CrossRef]
- Dladla, M.; Gyzenhout, M.; Marias, G.; Ghosh, S. Azole resistance in Aspergillus fumigatus-comprehensive review. Arch. Microbiol. 2024, 206, 305. [Google Scholar] [CrossRef]
- Geremia, N.; Giovagnorio, F.; Colpani, A.; De Vito, A.; Caruana, G.; Meloni, M.C.; Madeddu, G.; Panese, S.; Parisi, S.G. What do We Know about Cryptic Aspergillosis? Microorganisms 2024, 12, 886. [Google Scholar] [CrossRef]
- Barrs, V.R.; Talbot, J.J. Feline aspergillosis. Vet. Clin. Small Anim. Pract. 2014, 44, 51–73. [Google Scholar] [CrossRef]
- Escribano, P.; Rodríguez-Sánchez, B.; Díaz-García, J.; Martín-Gómez, M.T.; Ibáñez-Martínez, E.; Rodríguez-Mayo, M.; Peláez, T.; de la Pedrosa, E.G.G.; Tejero-García, R.; Marimón, J.M.; et al. Azole resistance survey on clinical Aspergillus fumigatus isolates in Spain. Clin. Microbiol. Infect. 2021, 27, 1170.e1–1170.e7. [Google Scholar] [CrossRef]
- Denning, D.W. Antifungal drug resistance: An update. Eur. J. Hosp. Pharm. 2022, 29, 109–112. [Google Scholar] [CrossRef]
- WHO. Global Antimicrobial Resistance and Use Surveillance System (GLASS). Available online: https://www.who.int/initiatives/glass (accessed on 28 April 2025).
- Fisher, M.C.; Alastruey-Izquierdo, A.; Berman, J.; Bicanic, T.; Bignell, E.M.; Bowyer, P.; Bromley, M.; Brüggemann, R.; Garber, G.; Cornely, O.A.; et al. Tackling the emerging threat of antifungal resistance to human health. Nat. Rev. Microbiol. 2022, 20, 557–571. [Google Scholar] [CrossRef]
- Policy Brief AMR Antifungal Resistance V9—Gaffi. Available online: https://gaffi.org/wp-content/uploads/GAFFI-Policy-Brief-AMR-antifungal-resistance.pdf (accessed on 28 April 2025).
- Odoj, K.; Garlasco, J.; Pezzani, M.D.; Magnabosco, C.; Ortiz, D.; Manco, F.; Galia, L.; Foster, S.K.; Arieti, F.; Tacconelli, E. Tracking Candidemia Trends and Antifungal Resistance Patterns across Europe: An In-Depth Analysis of Surveillance Systems and Surveillance Studies. J. Fungi 2024, 10, 685. [Google Scholar] [CrossRef] [PubMed]
- Hope, M.; Kiggundu, R.; Byonanebye, D.M.; Mayito, J.; Tabajjwa, D.; Lwigale, F.; Tumwine, C.; Mwanja, H.; Kambugu, A.; Kakooza, F.; et al. Progress of Implementation of World Health Organization Global Antimicrobial Resistance Surveillance System Recommendations on Priority Pathogen-Antibiotic Sensitivity Testing in Africa: Protocol for a Scoping Review. JMIR Res. Protoc. 2024, 13, e58140. [Google Scholar] [CrossRef] [PubMed]
- Galia, L.; Pezzani, M.D.; Compri, M.; Callegari, A.; Rajendran, N.B.; Carrara, E.; Tacconelli, E.; Network, C.M.E.N. Surveillance of antifungal resistance in candidemia fails to inform antifungal stewardship in European countries. J. Fungi 2022, 8, 249. [Google Scholar] [CrossRef] [PubMed]
- Surveillance—Antimicrobial Resistance (AMR)—The Global Health Network. Available online: https://amr.tghn.org/resources/surveillance (accessed on 28 April 2025).
- Simonsen, G.S. Antimicrobial resistance surveillance in Europe and beyond. Eurosurveillance 2018, 23, 1800560. [Google Scholar] [CrossRef]
- Yamin, D.; Akanmu, M.H.; Al Mutair, A.; Alhumaid, S.; Rabaan, A.A.; Hajissa, K. Global prevalence of antifungal-resistant Candida parapsilosis: A systematic review and meta-analysis. Trop. Med. Infect. Dis. 2022, 7, 188. [Google Scholar] [CrossRef]
- Antimicrobial Resistance in the EU/EEA (EARS-Net)—AER for 2019. Available online: https://www.gov.pl/attachment/67341e01-0120-481e-b250-7d4a5db548b0 (accessed on 28 April 2025).
- CDC. Antimicrobial-Resistant Fungal Diseases. Available online: https://www.cdc.gov/fungal/antimicrobial-resistant-fungi/index.html (accessed on 28 April 2025).
- CDC. Tracking C. auris|Candida auris (C. auris). Available online: https://www.cdc.gov/candida-auris/tracking-c-auris/index.html (accessed on 28 April 2025).
- Beer, K.D. Multidrug-resistant Aspergillus fumigatus carrying mutations linked to environmental fungicide exposure—Three states, 2010–2017. MMWR. Morb. Mortal. Wkly. Rep. 2018, 67, 1064–1067. [Google Scholar] [CrossRef]
- Burks, C.; Darby, A.; Gómez Londoño, L.; Momany, M.; Brewer, M.T. Azole-resistant Aspergillus fumigatus in the environment: Identifying key reservoirs and hotspots of antifungal resistance. PLoS Pathog. 2021, 17, e1009711. [Google Scholar] [CrossRef]
- Won, E.J.; Choi, M.J.; Jeong, S.H.; Kim, D.; Shin, K.S.; Shin, J.H.; Kim, Y.R.; Kim, H.S.; Kim, Y.A.; Uh, Y.; et al. Nationwide surveillance of antifungal resistance of Candida bloodstream isolates in South Korean hospitals: Two year report from Kor-GLASS. J. Fungi 2022, 8, 996. [Google Scholar] [CrossRef]
- Romanescu, M.; Oprean, C.; Lombrea, A.; Badescu, B.; Teodor, A.; Constantin, G.D.; Andor, M.; Folescu, R.; Muntean, D.; Danciu, C.; et al. Current state of knowledge regarding who high priority pathogens—Resistance mechanisms and proposed solutions through candidates such as essential oils: A systematic review. Int. J. Mol. Sci. 2023, 24, 9727. [Google Scholar] [CrossRef]
- Monpierre, L.; Desbois-Nogard, N.; Valsecchi, I.; Bajal, M.; Angebault, C.; Miossec, C.; Botterel, F.; Dannaoui, É. Azole Resistance in Clinical and Environmental Aspergillu s Isolates from the French West Indies (Martinique). J. Fungi 2021, 7, 355. [Google Scholar] [CrossRef]
- Tashiro, M.; Nakano, Y.; Shirahige, T.; Kakiuchi, S.; Fujita, A.; Tanaka, T.; Takazono, T.; Izumikawa, K. Comprehensive Review of Environmental Surveillance for Azole-Resistant Aspergillus fumigatus: A Practical Roadmap for Hospital Clinicians and Infection Control Teams. J. Fungi 2025, 11, 96. [Google Scholar] [CrossRef] [PubMed]
- Mudenda, S. Global Burden of fungal infections and antifungal resistance from 1961 to 2024: Findings and future implications. Pharmacol. Pharm. 2024, 15, 81–112. [Google Scholar] [CrossRef]
- Arastehfar, A.; Gabaldón, T.; Garcia-Rubio, R.; Jenks, J.D.; Hoenigl, M.; Salzer, H.J.; Ilkit, M.; Lass-Flörl, C.; Perlin, D.S. Drug-resistant fungi: An emerging challenge threatening our limited antifungal armamentarium. Antibiotics 2020, 9, 877. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.R.; Neill, C.; Borman, A.M.; Budd, E.L.; Cummins, M.; Fry, C.; Guy, R.L.; Jeffery, K.; Johnson, E.M.; Manuel, R.; et al. The laboratory investigation, management, and infection prevention and control of Candida auris: A narrative review to inform the 2024 national guidance update in England. J. Med. Microbiol. 2024, 73, 001820. [Google Scholar] [CrossRef]
- Czajka, K.M.; Venkataraman, K.; Brabant-Kirwan, D.; Santi, S.A.; Verschoor, C.; Appanna, V.D.; Singh, R.; Saunders, D.P.; Tharmalingam, S. Molecular mechanisms associated with antifungal resistance in pathogenic Candida species. Cells 2023, 12, 2655. [Google Scholar] [CrossRef]
- Fang, W.; Wu, J.; Cheng, M.; Zhu, X.; Du, M.; Chen, C.; Liao, W.; Zhi, K.; Pan, W. Diagnosis of invasive fungal infections: Challenges and recent developments. J. Biomed. Sci. 2023, 30, 42. [Google Scholar] [CrossRef]
- Fung, S.; Shirley, M. Rezafungin: A Review in Invasive Candidiasis. Drugs 2025, 85, 415–423. [Google Scholar] [CrossRef]
- Ghannoum, M.; Arendrup, M.C.; Chaturvedi, V.P.; Lockhart, S.R.; McCormick, T.S.; Chaturvedi, S.; Berkow, E.L.; Juneja, D.; Tarai, B.; Azie, N.; et al. Ibrexafungerp: A novel oral triterpenoid antifungal in development for the treatment of Candida auris infections. Antibiotics 2020, 9, 539. [Google Scholar] [CrossRef]
- Vazquez, J.A.; Pappas, P.G.; Boffard, K.; Paruk, F.; Bien, P.A.; Tawadrous, M.; Ople, E.; Wedel, P.; Oborska, I.; Hodges, M.R. Clinical efficacy and safety of a novel antifungal, fosmanogepix, in patients with candidemia caused by Candida auris: Results from a phase 2 trial. Antimicrob. Agents Chemother. 2023, 67, e01419-22. [Google Scholar] [CrossRef]
- Karthaus, M. Guideline based treatment of invasive aspergillosis. Mycoses 2010, 53, 36–43. [Google Scholar] [CrossRef]
- Douglas, A.P.; Smibert, O.C.; Bajel, A.; Halliday, C.L.; Lavee, O.; McMullan, B.; Yong, M.K.; van Hal, S.J.; Chen, S.C.A.; Committee, A.A.G.S.; et al. Consensus guidelines for the diagnosis and management of invasive aspergillosis, 2021. Intern. Med. J. 2021, 51, 143–176. [Google Scholar] [CrossRef]
- Brunet, K.; Rammaert, B. Mucormycosis treatment: Recommendations, latest advances, and perspectives. J. Mycol. Medicale 2020, 30, 101007. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Mendoza, M.I.; Pérez-Arques, C.; Parker, J.; Xu, Z.; Kelly, S.; Heitman, J. Alternative ergosterol biosynthetic pathways confer antifungal drug resistance in the human pathogens within the Mucor species complex. Mbio 2024, 15, e01661-24. [Google Scholar] [CrossRef] [PubMed]
- Meena, D.S.; Kumar, D.; Bohra, G.K. Combination therapy in Mucormycosis: Current evidence from the world literature, a mini review. J. Med. Mycol. 2023, 33, 101332. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, J.N.; Lawrence, D.S.; Meya, D.B.; Kagimu, E.; Kasibante, J.; Mpoza, E.; Rutakingirwa, M.K.; Ssebambulidde, K.; Tugume, L.; Rhein, J.; et al. Single-dose liposomal amphotericin B treatment for cryptococcal meningitis. N. Engl. J. Med. 2022, 386, 1109–1120. [Google Scholar] [CrossRef]
- Nagai, T.; Matsui, H.; Fujioka, H.; Homma, Y.; Otsuki, A.; Ito, H.; Ohmura, S.; Miyamoto, T.; Shichi, D.; Tomohisa, W.; et al. Low-dose vs conventional-dose trimethoprim-sulfamethoxazole treatment for pneumocystis pneumonia in patients not infected with HIV: A multicenter, retrospective observational cohort study. Chest 2024, 165, 58–67. [Google Scholar] [CrossRef]
- Tian, Q.; Si, J.; Jiang, F.; Xu, R.; Wei, B.; Huang, B.; Li, Q.; Jiang, Z.; Zhao, T. Caspofungin combined with TMP/SMZ as a first-line therapy for moderate-to-severe PCP in patients with human immunodeficiency virus infection. HIV Med. 2021, 22, 307–313. [Google Scholar] [CrossRef]
- Prosty, C.; Katergi, K.; Sorin, M.; Rjeily, M.B.; Butler-Laporte, G.; McDonald, E.G.; Lee, T.C. Comparative efficacy and safety of Pneumocystis jirovecii pneumonia prophylaxis regimens for people with HIV: A systematic review and network meta-analysis of randomized controlled trials. Clin. Microbiol. Infect. 2024, 30, 866–876. [Google Scholar] [CrossRef]
- Corey, M. Modern antifungal therapy for neutropenic fever. Curr. Infect. Dis. Rep. 2009, 11, 29–34. [Google Scholar] [CrossRef]
- Yoshida, M. Development of a method of measuring β-D-glucan and its use in preemptive therapy for invasive fungal infections. Int. J. Mol. Sci. 2021, 22, 9265. [Google Scholar] [CrossRef]
- Wiederhold, N.P. Antifungal susceptibility testing: A primer for clinicians. In Open Forum Infectious Diseases; Oxford University Press US: Cary, NC, USA, 2021; Volume 8, p. ofab444. [Google Scholar]
- Chakrabarti, A.; Mohamed, N.; Capparella, M.R.; Townsend, A.; Sung, A.H.; Yura, R.; Muñoz, P. The role of diagnostics-driven antifungal stewardship in the management of invasive fungal infections: A systematic literature review. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2022; Volume 9, p. ofac234. [Google Scholar]
- Procacci, C.; Marras, L.; Maurmo, L.; Vivanet, G.; Scalone, L.; Bertolino, G. Antifungal Stewardship in Invasive Fungal Infections, a Systematic Review. In Advances in Experimental Medicine and Biology; Springer: Berlin/Heidelberg, Germany, 2024. [Google Scholar]
- Tverdek, F.P.; Kofteridis, D.; Kontoyiannis, D.P. Antifungal agents and liver toxicity: A complex interaction. Expert Rev. Anti-Infect. Ther. 2016, 14, 765–776. [Google Scholar] [CrossRef]
- Sucher, A.J.; Chahine, E.B.; Balcer, H.E. Echinocandins: The newest class of antifungals. Ann. Pharmacother. 2009, 43, 1647–1657. [Google Scholar] [CrossRef] [PubMed]
- Wong-Beringer, A.; Kriengkauykiat, J. Systemic antifungal therapy: New options, new challenges. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2003, 23, 1441–1462. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Effron, G. Rezafungin—Mechanisms of action, susceptibility and resistance: Similarities and differences with the other echinocandins. J. Fungi 2020, 6, 262. [Google Scholar] [CrossRef] [PubMed]
- Sofjan, A.K.; Mitchell, A.; Shah, D.N.; Nguyen, T.; Sim, M.; Trojcak, A.; Beyda, N.D.; Garey, K.W. Rezafungin (CD101), a next-generation echinocandin: A systematic literature review and assessment of possible place in therapy. J. Glob. Antimicrob. Resist. 2018, 14, 58–64. [Google Scholar] [CrossRef]
- Scorneaux, B.; Angulo, D.; Borroto-Esoda, K.; Ghannoum, M.; Peel, M.; Wring, S. SCY-078 is fungicidal against Candida species in time-kill studies. Antimicrob. Agents Chemother. 2017, 61, 10–1128. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Jørgensen, K.M.; Hare, R.K.; Chowdhary, A. In vitro activity of ibrexafungerp (SCY-078) against Candida auris isolates as determined by EUCAST methodology and comparison with activity against C. albicans and C. glabrata and with the activities of six comparator agents. Antimicrob. Agents Chemother. 2020, 64, 10–1128. [Google Scholar] [CrossRef]
- Nyirjesy, P.; Schwebke, J.R.; Angulo, D.A.; Harriott, I.A.; Azie, N.E.; Sobel, J.D. Phase 2 randomized study of oral ibrexafungerp versus fluconazole in vulvovaginal candidiasis. Clin. Infect. Dis. 2022, 74, 2129–2135. [Google Scholar] [CrossRef]
- Vanbiervliet, Y.; Van Nieuwenhuyse, T.; Aerts, R.; Lagrou, K.; Spriet, I.; Maertens, J. Review of the novel antifungal drug olorofim (F901318). BMC Infect. Dis. 2024, 24, 1256. [Google Scholar] [PubMed]
- Halliday, C.L.; Tay, E.; Green, W.; Law, D.; Lopez, R.; Faris, S.; Meehan, L.; Harvey, E.; Birch, M.; Chen, S.C. In vitro activity of olorofim against 507 filamentous fungi including antifungal drug-resistant strains at a tertiary laboratory in Australia: 2020–2023. J. Antimicrob. Chemother. 2024, 79, 2611–2621. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.J.; Ibrahim, A.S. Fosmanogepix: A review of the first-in-class broad spectrum agent for the treatment of invasive fungal infections. J. Fungi 2020, 6, 239. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, M.; Moloney, M.; Soltow, Q.A.; Pillar, C.M.; Shaw, K.J. Evaluation of resistance development to the Gwt1 inhibitor manogepix (APX001A) in Candida species. Antimicrob. Agents Chemother. 2019, 64, 10–1128. [Google Scholar] [CrossRef]
- Sobel, J.D.; Nyirjesy, P. Oteseconazole: An advance in treatment of recurrent vulvovaginal candidiasis. Future Microbiol. 2021, 16, 1453–1461. [Google Scholar] [CrossRef]
- Hargrove, T.Y.; Friggeri, L.; Wawrzak, Z.; Qi, A.; Hoekstra, W.J.; Schotzinger, R.J.; York, J.D.; Guengerich, F.P.; Lepesheva, G.I. Structural analyses of Candida albicans sterol 14α-demethylase complexed with azole drugs address the molecular basis of azole-mediated inhibition of fungal sterol biosynthesis. J. Biol. Chem. 2017, 292, 6728–6743. [Google Scholar] [CrossRef]
- Murray, A.; Cass, L.; Ito, K.; Pagani, N.; Armstrong-James, D.; Dalal, P.; Reed, A.; Strong, P. PC945, a novel inhaled antifungal agent, for the treatment of respiratory fungal infections. J. Fungi 2020, 6, 373. [Google Scholar] [CrossRef]
- Brown, G.D.; Ballou, E.R.; Bates, S.; Bignell, E.M.; Borman, A.M.; Brand, A.C.; Brown, A.J.; Coelho, C.; Cook, P.C.; Farrer, R.A.; et al. The pathobiology of human fungal infections. Nat. Rev. Microbiol. 2024, 22, 687–704. [Google Scholar] [CrossRef]
- Contagion Live. The 95-95 by 2025 Initiative: Addressing the Global Fungal Infection Crisis. Available online: https://www.contagionlive.com/view/the-95-95-by-2025-initiative-addressing-the-global-fungal-infection-crisis (accessed on 28 April 2025).
- Ortiz, B.; Varela, D.; Fontecha, G.; Torres, K.; Cornely, O.A.; Salmanton-García, J. Strengthening Fungal Infection Diagnosis and Treatment: An In-depth Analysis of Capabilities in Honduras. In Open Forum Infectious Diseases; Oxford University Press US: Cary, NC, USA, 2024; Volume 11, p. ofae578. [Google Scholar]
- Murthy, A.N.; Srinivasan, S.; Patil, V.; Salunke, G.; Dhamne, C.; Roy Moulik, N.; Prasad, M.; C Parambil, B.; Gollamudi, V.R.M.; Chichra, A.; et al. Impact of Invasive Fungal Diseases on Treatment Outcomes in Pediatric Acute Lymphoblastic Leukemia and Lymphoblastic Lymphoma: Insights From a Single-Center Study. Pediatr. Blood Cancer 2025, 72, e31643. [Google Scholar] [CrossRef]
- Kneale, M.; Bartholomew, J.S.; Davies, E.; Denning, D.W. Global access to antifungal therapy and its variable cost. J. Antimicrob. Chemother. 2016, 71, 3599–3606. [Google Scholar] [CrossRef]
- Hassoun, N.; Kassem, I.I.; Hamze, M.; El Tom, J.; Papon, N.; Osman, M. Antifungal Use and Resistance in a Lower–Middle-Income Country: The Case of Lebanon. Antibiotics 2023, 12, 1413. [Google Scholar] [CrossRef]
- WHO. WHO Issues Its First-Ever Reports on Tests and Treatments for Fungal Infections. Available online: https://www.who.int/news/item/01-04-2025-who-issues-its-first-ever-reports-on-tests-and-treatments-for-fungal-infections (accessed on 28 April 2025).
- Wingen-Heimann, S.M.; Cornely, O.A.; Bethe, U.; Seidel, D. Revisiting diagnostics: Early and accurate diagnosis of invasive fungal infections: A health economic view on investing in innovative diagnostics. Clin. Microbiol. Infect. 2025, 31, 1089–1091. [Google Scholar] [CrossRef] [PubMed]
- Kwang, Y.C.; Nguyen, H.T.; Alffenaar, J.W.; Beardsley, J.; Dat, V.Q. Availability and cost of antifungal therapy in Vietnam: A 5-year retrospective study. Med. Mycol. 2025, 63, myaf028. [Google Scholar] [CrossRef] [PubMed]
- AlMaghrabi, R.S.; Al-Musawi, T.; Albaksami, O.; Subhi, A.L.; Fakih, R.E.; Stone, N.R.; AlMaghrabi, R.; Subhi, A.; Elfakih, R.; Stone, N. Challenges in the management of invasive fungal infections in the Middle East: Expert opinion to optimize management using a multidisciplinary approach. Cureus 2023, 15, e44356. [Google Scholar] [CrossRef] [PubMed]
- Gaffi. Improving Outcomes for Patients with Fungal Infections Across the World a Road Map for the Next Decade. Available online: http://gaffi.org/wp-content/uploads/GAFFI_Road_Map_interactive-final0415.pdf (accessed on 28 April 2025).
- DNDi. Ending Cryptococcal Meningitis Deaths by 2030: Strategic Framework. Available online: https://dndi.org/wp-content/uploads/2021/05/EndCryptococcalMeningitisDeaths2030-StrategicFramework-EN-2021.pdf (accessed on 28 April 2025).
- Odabasi, Z.; Mattiuzzi, G.; Estey, E.; Kantarjian, H.; Saeki, F.; Ridge, R.J.; Ketchum, P.A.; Finkelman, M.A.; Rex, J.H.; Ostrosky-Zeichner, L. β-D-glucan as a diagnostic adjunct for invasive fungal infections: Validation, cutoff development, and performance in patients with acute myelogenous leukemia and myelodysplastic syndrome. Clin. Infect. Dis. 2004, 39, 199–205. [Google Scholar] [CrossRef]
- Marty, F.M.; Lowry, C.M.; Lempitski, S.J.; Kubiak, D.W.; Finkelman, M.A.; Baden, L.R. Reactivity of (1→ 3)-β-D-glucan assay with commonly used intravenous antimicrobials. Antimicrob. Agents Chemother. 2006, 50, 3450–3453. [Google Scholar] [CrossRef]
- Sulahian, A.; Touratier, S.; Ribaud, P. False positive test for Aspergillus antigenemia related to concomitant administration of piperacillin and tazobactam. N. Engl. J. Med. 2003, 349, 2366–2367. [Google Scholar] [CrossRef]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and multi-national prevalence of fungal diseases—estimate precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef]
- Schmidt, C.S.; White, C.J.; Ibrahim, A.S.; Filler, S.G.; Fu, Y.; Yeaman, M.R.; Edwards, J.E., Jr.; Hennessey, J.P., Jr. NDV-3, a recombinant alum-adjuvanted vaccine for Candida and Staphylococcus aureus, is safe and immunogenic in healthy adults. Vaccine 2012, 30, 7594–7600. [Google Scholar] [CrossRef]
- Singh, S.; Uppuluri, P.; Mamouei, Z.; Alqarihi, A.; Elhassan, H.; French, S.; Lockhart, S.R.; Chiller, T.; Edwards, J.E., Jr.; Ibrahim, A.S. The NDV-3A vaccine protects mice from multidrug resistant Candida auris infection. PLoS Pathog. 2019, 15, e1007460. [Google Scholar] [CrossRef] [PubMed]
- Devi, S.J. Preclinical efficacy of a glucuronoxylomannan-tetanus toxoid conjugate vaccine of Cryptococcus neoformans in a murine model. Vaccine 1996, 14, 841–844. [Google Scholar] [CrossRef] [PubMed]
- Alapan, D.; Bisweswar, O.; Prasenjit, S.; Prasanjit, D.; Arkapal, B. Recent advances in the clinical development of antifungal vaccines: A narrative review. Front. Trop. Dis. 2024, 5, 1446477. [Google Scholar] [CrossRef]
- Albahar, F.; Alhamad, H.; Abu Assab, M.; Abu-Farha, R.; Alawi, L.; Khaleel, S. The impact of antifungal stewardship on clinical and performance measures: A global systematic review. Trop. Med. Infect. Dis. 2023, 9, 8. [Google Scholar] [CrossRef]
- Ramos, A.; Pérez-Velilla, C.; Asensio, A.; Ruiz-Antorán, B.; Folguera, C.; Cantero, M.; Orden, B.; Muñez, E. Antifungal stewardship in a tertiary hospital. Rev. Iberoam. Micol. 2015, 32, 209–213. [Google Scholar] [CrossRef]
- Sachdev, J.; Gourav, S.; Xess, I.; Soneja, M.; Punjadath, S.; Siddharth, V.; Pandey, M.; Gupta, S.; Manhas, A.; Rana, B.; et al. Impact of an institutional antifungal stewardship program on antifungal usage and outcomes in patients with invasive fungal infections. Med. Mycol. 2025, 63, myaf003. [Google Scholar] [CrossRef]
- Soni, S.; Hettle, D.; Hutchings, S.; Wade, S.; Forrest-Jones, K.; Sequeiros, I.; Borman, A.; Johnson, E.M.; Harding, I. Promoting antifungal stewardship through an antifungal multidisciplinary team in a paediatric and adult tertiary centre in the UK. JAC-Antimicrob. Resist. 2024, 6, dlae119. [Google Scholar] [CrossRef]
- Vitiello, A.; Ferrara, F.; Boccellino, M.; Ponzo, A.; Cimmino, C.; Comberiati, E.; Zovi, A.; Clemente, S.; Sabbatucci, M. Antifungal drug resistance: An emergent health threat. Biomedicines 2023, 11, 1063. [Google Scholar] [CrossRef]
- Exeter Launches Second Round of Global Funding to Tackle Antifungal Drug Resistance—News. Available online: https://news.exeter.ac.uk/faculty-of-health-and-life-sciences/exeter-launches-second-round-of-global-funding-to-tackle-antifungal-drug-resistance/ (accessed on 28 April 2025).
- NIAID. Apply to Develop Global Infectious Disease Research Training Programs. Available online: https://www.niaid.nih.gov/grants-contracts/global-infectious-disease-research-training-programs (accessed on 28 April 2025).

{kind=link}
{kind=link}
| Antifungal Class | Specific Molecular Target | Main Mechanism of Action | Activity vs. Key Pathogens | Primary PK/ PD Index | Main Known Resistance Mechanisms | Notes |
|---|---|---|---|---|---|---|
| Azoles (Triazoles: Fluconazole, Itraconazole, Voriconazole, Posaconazole, Isavuconazole) | Lanosterol 14-demethylase (Erg11/Cyp51A) | Inhibits ergosterol synthesis, accumulation of toxic methylated sterols | Fungistatic (Candida, Aspergillus, Cryptococcus, dimorphic fungi—variable spectrum) | AUC/MIC [23] | ERG11/cyp51A mutations/ overexpression, efflux pump overexpression (ABC/MFS) [27] | Significant CYP P450 interactions, Hepatotoxicity [23] |
| Polyenes (Amphotericin B) | Membrane ergosterol | Binds ergosterol, pore/channel formation, alters membrane permeability | Fungicidal (Broad spectrum: Candida, Aspergillus, Cryptococcus, Mucorales, dimorphic fungi) | Cmax/MIC [23] | Decreased ergosterol content, membrane alterations (rare); intrinsic resistance (e.g., A. terreus) [28] | Nephrotoxicity, infusion reactions (reduced with lipid formulations) [23] |
| Echinocandins (Caspofungin, Micafungin, Anidulafungin, Rezafungin) | -(1,3)-D-glucan synthase (Fks1/Fks2) | Inhibits -(1,3)-D-glucan synthesis, damages cell wall | Fungicidal (Candida spp.), Fungistatic (Aspergillus spp.) | AUC/MIC, Cmax/MIC [24] | Hotspot mutations in FKS1/FKS2 genes [29] | Well tolerated, low CYP interaction potential, IV only, limited spectrum (inactive vs Cryptococcus, Mucorales) [23] |
| Allylamines (Terbinafine) | Squalene epoxidase (Erg1) | Inhibits ergosterol synthesis, accumulation of toxic squalene | Fungicidal (dermatophytes) | Not well defined for systemic IFI | ERG1/SQLE mutations/ overexpression [30] | Limited systemic use (dermatomycoses), good tolerability [23] |
| Flucytosine (5-FC) | DNA and RNA synthesis | Intracellular conversion to 5-FU, inhibits thymidylate synthase and incorporates into RNA | Fungistatic (Candida spp., Cryptococcus spp.) | T > MIC | Mutations in permeases or metabolic enzymes (cytosine deaminase, UMP pyrophosphorylase) [31] | Almost always used in combination, Myelotoxicity [24] |
| Pathogen-Drug Combination | North America | South America | Europe | Asia | Africa | Middle East | Oceania | Notes/Key Sources |
|---|---|---|---|---|---|---|---|---|
| A. fumigatus—Azoles (Clinical) | <5% | >10% in Brazil | >10–20% (NL, UK, Spain); <10% elsewhere | 10–20% (China, Japan) | No robust data | >15% in Iran | <5% (sparse data) | Linked to environmental TR%; [28,59] |
| A. fumigatus—Azoles (Environmental, TR%) | <5% | 5–15% (patchy) | 10–20% (NL, UK, Spain) | 30–80% (China, Vietnam) | 5–10% (few studies) | >50% (Iran) | 5–10% (limited) | Main markers: TR34/L98H, TR46/Y121F/ T289A [55] |
| C. auris—Fluconazole | >90% | >90% | >90% | >90% | 91% (South Africa) | >90% | >90% | Near-universal resistance [32,34] |
| C. auris—Amphotericin B | 8–15% | 33% (Colombia) | 10–30% (varies by country) | 10–30% (India) | 21% (South Africa) | 10–20% (limited) | 10–20% (limited) | Resistance varies by clade/region [61,62] |
| C. auris—Echinocandins | <5%, but outbreaks reported | <2% | <5%, occasional outbreaks | <5% | 1.7% (South Africa) | <5% | <5% | Generally susceptible; resistance emerging [34,35] |
| C. glabrata—Fluconazole | 15–20% | Insufficient data | 86–100% (Slovenia, Croatia) | Patchy, scarce data | No reliable data | No reliable data | Insufficient data | High resistance in some regions [45,63] |
| C. glabrata—Echinocandins | 10–15% (USA) | Insufficient data | <5% | <5% | No reliable data | No reliable data | No reliable data | Emerging resistance in USA [61] |
| C. parapsilosis—Fluconazole | <10% | 15% (pooled) | 73–81% (Italy, Croatia) | 15% (pooled) | Sparse data | Sparse data | Sparse data | High resistance in selected countries [45,50] |
| Infection/Pathogen | First-Line Therapy | Alternative (Backup) Therapy |
|---|---|---|
| Cryptococcal meningitis (Cryptococcus neoformans) | Amphotericin B (lipid or deoxycholate) + Flucytosine (induction), followed by Fluconazole (maintenance) | Fluconazole monotherapy (if flucytosine unavailable), or Amphotericin B alone |
| Invasive candidiasis (Candida spp.) | Echinocandin (e.g., caspofungin, micafungin) | Fluconazole (in stable patients), Liposomal Amphotericin B (if echinocandins unavailable) |
| Invasive aspergillosis (Aspergillus fumigatus) | Voriconazole or Isavuconazole | Liposomal Amphotericin B; Posaconazole as salvage therapy |
| Mucormycosis (Rhizopus, Mucor) | Liposomal Amphotericin B | Posaconazole or Isavuconazole |
| Pneumocystis jirovecii pneumonia (PJP) | Trimethoprim–sulfamethoxazole (TMP–SMX) | Pentamidine, Atovaquone, or Dapsone + Trimethoprim |
| Disseminated histoplasmosis (Histoplasma capsulatum) | Liposomal Amphotericin B (initial), followed by Itraconazole | Amphotericin B deoxycholate (if lipid formulation unavailable), Fluconazole (less effective) |
| Drug Name | Class/ Mechanism | Primary Target Pathogens | Route(s) | Key Advantage(s) | Limitation(s) | Development Status | Representative Chemical Structure |
|---|---|---|---|---|---|---|---|
| Rezafungin | Echinocandin (Glucan synthase inhibitor) | Candida spp. (incl. C. auris) | IV | Weekly administration (long half-life) | IV-only, spectrum similar to other echinocandins | Approved (Candidemia) | Cyclic lipopeptide with hexapeptide core and lipid side chain |
| Ibrexafungerp | Triterpenoid (Glucan synthase inhibitor—distinct Fks site) | Candida spp. (incl. resistant), Aspergillus spp. | PO | Oral, activity against echinocandin-resistant strains | Inactive against Mucorales/Fusarium | Approved (RVVC) | Semi-synthetic triterpenoid (enfumafungin derivative) with polycyclic core |
| Olorofim | Orotomide (DHODH inhibitor – pyrimidine synthesis) | Molds (e.g., resistant Aspergillus, Lomentospora, Scedosporium) | PO | Novel mechanism, oral, active against difficult molds | Inactive against yeasts/Mucorales, potential CYP450 interactions | Phase 3 | Diarylamide core with substituted pyrimidine ring |
| Fosmanogepix | Gwt1 inhibitor (GPI-anchored protein maturation) | Broad spectrum (Candida, Aspergillus, Cryptococcus, rare molds) | IV, PO | Novel mechanism, broad spectrum, IV/PO options | Inactive against C. krusei | Phase 2/3 planned | Prodrug of manogepix: hydroxypyridazinone core with phosphonooxymethyl group |
| Oteseconazole | Tetrazole (Selective CYP51 inhibitor) | Candida spp. (incl. fluconazole-resistant) | PO | Oral, high CYP51 selectivity (potentially fewer interactions/toxicity) | Potential embryofetal risk, long half-life, only for recurrent VVC | Approved (RVVC, USA) | Tetrazole ring replacing triazole of azoles, with substituted aromatic moieties |
| Opelconazole | Triazole (CYP51 inhibitor) | Aspergillus spp. | Inh. | High lung concentrations, low systemic exposure | Pulmonary-only, likely needs adjunct systemic therapy | Phase 2/3 | Triazole core structure with fluorinated phenyl side chains |
| Invasive Fungal Infection | Estimated Mortality Rate (%) in High-Income Countries (HICs) | Estimated Mortality Rate (%) in LMICs |
|---|---|---|
| Cryptococcal meningitis | 9–15 | 22–96 |
| Invasive aspergillosis | 30–50 | 70–90 (est.) |
| Invasive candidiasis | 20–40 | 40–70 (est.) |
| Pneumocystis jirovecii pneumonia | 10–20 | 30–50 (est.) |
| Antifungal Agent | Availability in HICs | Availability in LMICs |
| Fluconazole | Widely available | Limited |
| Amphotericin B (deoxycholate/lipid) | Widely available | Limited |
| Flucytosine | Available | Rarely available or absent |
| Voriconazole | Available | Limited |
| Echinocandins | Available | Limited |
| Diagnostic Method | Key Advantages | Key Limitations (Including LMIC Contexts) | Current Availability in LMICs |
|---|---|---|---|
| Culture | Standard method for identification; allows antifungal susceptibility testing | Slow (days to weeks); variable sensitivity; may be difficult to distinguish colonization from infection | High |
| Microscopy | Rapid; inexpensive | Requires expertise; variable sensitivity; not always specific | High |
| -D-Glucan Test | Pan-fungal marker; useful for early detection of candidiasis and aspergillosis | Non-specific; false positives (e.g., hemodialysis, IVIG); not useful for Mucorales or Cryptococcus | Low |
| Galactomannan (GM) Test | Useful for early diagnosis of invasive aspergillosis; can be performed on serum or BAL | Specific for Aspergillus; false positives (e.g., antibiotics, foods); not useful for Candida, Cryptococcus, or Mucorales | Low |
| PCR-based Tests | Rapid; high sensitivity and specificity | Requires specialized equipment and expertise; costly; may not distinguish viable organisms from DNA; limited availability in LMICs | Low |
| Antigen Detection | Rapid; may be point-of-care (e.g., CrAg for Cryptococcus) | Variable specificity; limited availability for many pathogens in LMICs | Low |
| Metagenomics | Detects broad range of organisms; may identify rare or mixed infections | Expensive; requires bioinformatics expertise; complex interpretation; extremely limited availability in LMICs | Very Low |
| Lateral Flow Assays (LFA) | Rapid; point-of-care; potentially inexpensive | Variable sensitivity and specificity depending on test; limited availability for many pathogens | Low |
| Action Area | Specific Recommendations | Stakeholders |
|---|---|---|
| Policy and Awareness | Officially recognize IFIs as a global health priority; integrate IFIs into pandemic preparedness plans | WHO, Governments, Regulatory Bodies |
| Research and Development | Increase funding for basic research, development of new antifungals, diagnostics, and vaccines; promote translational and clinical research | Governments, Funding Agencies, Pharmaceutical Industry, Research Institutions |
| Diagnostics | Invest in the development and distribution of rapid, accurate, and affordable diagnostic tests, including POCTs, especially in LMICs; strengthen laboratory capacity in LMICs | WHO, Governments, Funding Agencies, Diagnostic Industry |
| Treatment and Antifungal Stewardship | Ensure access to essential and affordable antifungal drugs in LMICs; implement and strengthen antifungal stewardship programs in clinical and hospital settings; develop treatment guidelines tailored to LMICs | WHO, Governments, Healthcare Providers, Pharmaceutical Industry |
| Capacity Building | Train healthcare workers in LMICs in IFI diagnosis, management, and prevention; develop mycology reference centers and expert networks | WHO, Governments, Academic Institutions, Non-Governmental Organizations |
| Financing | Increase public and philanthropic funding for research, development, and implementation of IFI-related interventions | Governments, Funding Agencies, Philanthropic Foundations |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Branda, F.; Petrosillo, N.; Ceccarelli, G.; Giovanetti, M.; De Vito, A.; Madeddu, G.; Scarpa, F.; Ciccozzi, M. Antifungal Agents in the 21st Century: Advances, Challenges, and Future Perspectives. Infect. Dis. Rep. 2025, 17, 91. https://doi.org/10.3390/idr17040091
Branda F, Petrosillo N, Ceccarelli G, Giovanetti M, De Vito A, Madeddu G, Scarpa F, Ciccozzi M. Antifungal Agents in the 21st Century: Advances, Challenges, and Future Perspectives. Infectious Disease Reports. 2025; 17(4):91. https://doi.org/10.3390/idr17040091
Chicago/Turabian StyleBranda, Francesco, Nicola Petrosillo, Giancarlo Ceccarelli, Marta Giovanetti, Andrea De Vito, Giordano Madeddu, Fabio Scarpa, and Massimo Ciccozzi. 2025. "Antifungal Agents in the 21st Century: Advances, Challenges, and Future Perspectives" Infectious Disease Reports 17, no. 4: 91. https://doi.org/10.3390/idr17040091
APA StyleBranda, F., Petrosillo, N., Ceccarelli, G., Giovanetti, M., De Vito, A., Madeddu, G., Scarpa, F., & Ciccozzi, M. (2025). Antifungal Agents in the 21st Century: Advances, Challenges, and Future Perspectives. Infectious Disease Reports, 17(4), 91. https://doi.org/10.3390/idr17040091