Pan-European Study on the Prevalence of the Feline Leukaemia Virus Infection – Reported by the European Advisory Board on Cat Diseases (ABCD Europe)


 , ,
, ,  ,
,  , ,
, , 
 , , ,
, , , 
 add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Design of the Prevalence Study
2.2. Sample Collection for the Prevalence Study
2.3. Data Collection for the Prevalence Study
2.4. Sample Preparation and Molecular Analysis
2.5. Pre-Experiment
2.6. Statistical Analysis
2.6.1. Descriptive Analysis
2.6.2. Regression Analysis
2.6.3. Classification Tree Analysis
3. Results
3.1. Pre-Experiment
3.2. Pan-European Prevalence Study
3.2.1. Sample Size and Return Rate
3.2.2. Sample Characteristics
3.2.3. Prevalence of FeLV Viraemia
3.2.4. FeLV Vaccination Status
3.2.5. Regression Analysis
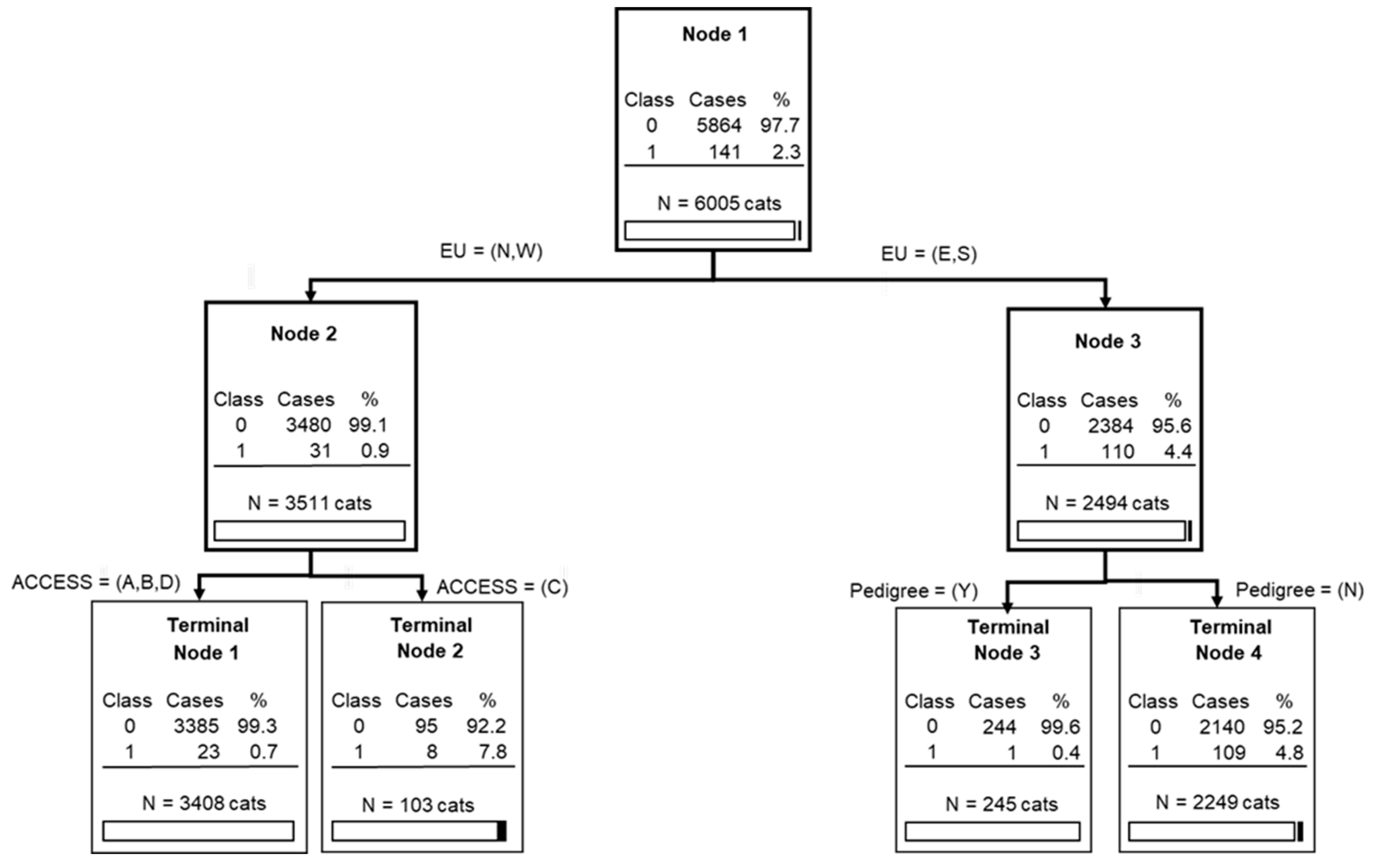
3.2.6. Classification Tree Analysis
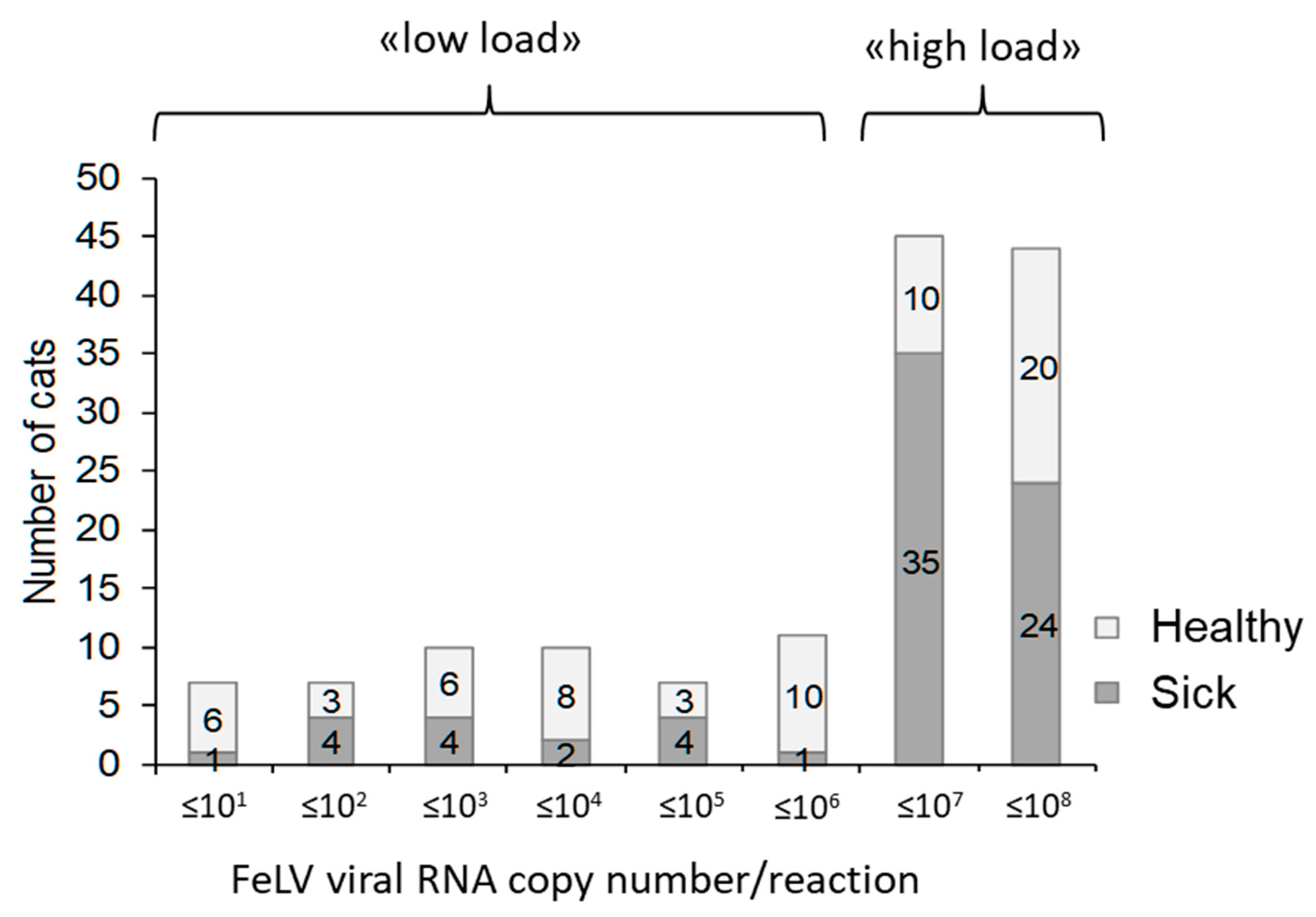
3.2.7. FeLV Viral RNA Loads in Saliva
3.2.8. Clinical Signs Associated with FeLV Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Type | Value Range | Value Required |
|---|---|---|---|
| Country identification | select | list of countries | yes |
| Veterinary practice | text | yes | |
| Six-digit swab number | text | according to tube label | yes |
| Date of collection | date | yes | |
| Cat name | text | yes | |
| Owner name | text | yes | |
| Postal code of cat owner | text | yes | |
| Type of husbandry | select | private/breeder/shelter/rescue cat/other | yes |
| Multicat environment | select | yes/no/not sure | yes |
| If yes: how many cats in the group | select | 2/3/4/≥5 | optional |
| Sex of cat | select | male/female/not sure | yes |
| Reproductive status of cat | select | intact/neutered/not sure | yes |
| Age of cat | select | 0–8 weeks/9–12 weeks/13–52 weeks/1–2 years/2–3 years/…/19–20 years/≥20 years | yes |
| Pedigree cat | select | yes/no/not sure | yes |
| If yes: which breed | text | optional | |
| Indoor and outdoor access | select | Indoor and outdoor/indoor only/outdoor only/not sure | yes |
| Last vaccination against FeLV | select | <1 year/1–3 years/>3 years/never/not sure | yes |
| Health status | select | healthy/sick | yes |
| If sick: major clinical problem | text | optional | |
| Comments | long text | optional |

References
- Jarrett, W.F.; Crawford, E.M.; Martin, W.B.; Davie, F. A Virus-Like Particle Associated with Leukemia (Lymphosarcoma). Nature 1964, 202, 567–569. [Google Scholar] [CrossRef]
- Willett, B.J.; Hosie, M.J. Feline leukaemia virus: Half a century since its discovery. Vet. J. 2013, 195, 16–23. [Google Scholar] [CrossRef]
- Lutz, H.; Addie, D.; Belak, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Hosie, M.J.; Lloret, A.; et al. Feline leukaemia. ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 565–574. [Google Scholar] [CrossRef]
- Helfer-Hungerbuehler, A.K.; Widmer, S.; Kessler, Y.; Riond, B.; Boretti, F.S.; Grest, P.; Lutz, H.; Hofmann-Lehmann, R. Long-term follow up of feline leukemia virus infection and characterization of viral RNA loads using molecular methods in tissues of cats with different infection outcomes. Virus Res. 2015, 197, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Hofmann-Lehmann, R.; Holznagel, E.; Ossent, P.; Lutz, H. Parameters of disease progression in long-term experimental feline retrovirus (feline immunodeficiency virus and feline leukemia virus) infections: Hematology, clinical chemistry, and lymphocyte subsets. Clin. Diagn. Lab. Immunol. 1997, 4, 33–42. [Google Scholar]
- Hofmann-Lehmann, R.; Cattori, V.; Tandon, R.; Boretti, F.S.; Meli, M.L.; Riond, B.; Pepin, A.C.; Willi, B.; Ossent, P.; Lutz, H. Vaccination against the feline leukaemia virus: Outcome and response categories and long-term follow-up. Vaccine 2007, 25, 5531–5539. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.; Crawford, C.; Hartmann, K.; Hofmann-Lehmann, R.; Little, S.; Sundahl, E.; Thayer, V. 2008 American Association of Feline Practitioners’ feline retrovirus management guidelines. J. Feline Med. Surg. 2008, 10, 300–316. [Google Scholar] [CrossRef] [PubMed]
- McClelland, A.J.; Hardy, W.D.; Zuckerman, E.E. Prognosis of healthy feline leukemia virus infected cats. In Development in Cancer Research; Hardy, W.D., Essex, M., McClelland, A.J., Eds.; Elsevier Scientific Publishing Company: Amsterdam, The Netherlands, 1980; Volume 4, pp. 121–126. [Google Scholar]
- Hartmann, K. Clinical aspects of feline retroviruses: A review. Viruses 2012, 4, 2684–2710. [Google Scholar] [CrossRef]
- Levy, J.K.; Scott, H.M.; Lachtara, J.L.; Crawford, P.C. Seroprevalence of feline leukemia virus and feline immunodeficiency virus infection among cats in North America and risk factors for seropositivity. J. Am. Vet. Med. Assoc. 2006, 228, 371–376. [Google Scholar] [CrossRef]
- Weijer, K.; UijtdeHaag, F.; Osterhaus, A. Control of feline leukaemia virus infection by a removal programme. Vet. Rec. 1986, 119, 555–556. [Google Scholar] [CrossRef]
- Cotter, S.M. Changing epidemiology of FeLV. In Proceedings of the 15th Annual ACVIM Forum, Lake Buena Vista, FL, USA, 22 May 1997; pp. 22–25. [Google Scholar]
- Burling, A.N.; Levy, J.K.; Scott, H.M.; Crandall, M.M.; Tucker, S.J.; Wood, E.G.; Foster, J.D. Seroprevalences of feline leukemia virus and feline immunodeficiency virus infection in cats in the United States and Canada and risk factors for seropositivity. J. Am. Vet. Med. Assoc. 2017, 251, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Gleich, S.E.; Krieger, S.; Hartmann, K. Prevalence of feline immunodeficiency virus and feline leukaemia virus among client-owned cats and risk factors for infection in Germany. J. Feline Med. Surg. 2009, 11, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Hofmann-Lehmann, R.; Gonczi, E.; Riond, B.; Meli, M.; Willi, B.; Howard, J.; Schaarschmidt-Kiener, D.; Regli, W.; Gilli, U.; Boretti, F. [Feline leukemia virus infection: Importance and current situation in Switzerland]. Schweiz Arch. Tierheilkd 2018, 160, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Agger, J.F.; Thomsen, R.L. Risk factors and control of FIV and FeLV infections in Danish cats. In Proceedings of the International Symposia on Veterinary Epidemiology and Economics proceedings—ISVEE13, Belgium, The Netherlands, 20–24 August 2012. [Google Scholar]
- Little, S.; Sears, W.; Lachtara, J.; Bienzle, D. Seroprevalence of feline leukemia virus and feline immunodeficiency virus infection among cats in Canada. Can. Vet. J. 2009, 50, 644–648. [Google Scholar]
- Westman, M.E.; Paul, A.; Malik, R.; McDonagh, P.; Ward, M.P.; Hall, E.; Norris, J.M. Seroprevalence of feline immunodeficiency virus and feline leukaemia virus in Australia: Risk factors for infection and geographical influences (2011–2013). JFMS Open Rep. 2016, 2, 2055116916646388. [Google Scholar] [CrossRef]
- Chhetri, B.K.; Berke, O.; Pearl, D.L.; Bienzle, D. Comparison of the geographical distribution of feline immunodeficiency virus and feline leukemia virus infections in the United States of America (2000–2011). BMC Vet. Res. 2013, 9, 392–398. [Google Scholar] [CrossRef]
- Englert, T.; Lutz, H.; Sauter-Louis, C.; Hartmann, K. Survey of the feline leukemia virus infection status of cats in Southern Germany. J. Feline Med. Surg 2012, 14, 392–398. [Google Scholar] [CrossRef]
- Spada, E.; Perego, R.; Sgamma, E.A.; Proverbio, D. Survival time and effect of selected predictor variables on survival in owned pet cats seropositive for feline immunodeficiency and leukemia virus attending a referral clinic in northern Italy. Prev. Vet. Med. 2018, 150, 38–46. [Google Scholar] [CrossRef]
- Firth, C.L.; Mostl, K. A survey of feline leukaemia virus antigenaemia among cats in eastern Austria: A retrospective analysis of serum samples routinely tested between 1996 and 2011. JFMS Open Rep. 2015, 1, 2055116915598336. [Google Scholar] [CrossRef]
- Ueland, K.; Lutz, H. Prevalence of feline leukemia virus and antibodies to feline immunodeficiency virus in cats in Norway. Zent. Vet. B 1992, 39, 53–58. [Google Scholar] [CrossRef]
- Hosie, M.J.; Robertson, C.; Jarrett, O. Prevalence of feline leukaemia virus and antibodies to feline immunodeficiency virus in cats in the United Kingdom. Vet. Rec. 1989, 125, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Arjona, A.; Escolar, E.; Soto, I.; Barquero, N.; Martin, D.; Gomez-Lucia, E. Seroepidemiological survey of infection by feline leukemia virus and immunodeficiency virus in Madrid and correlation with some clinical aspects. J. Clin. Microbiol. 2000, 38, 3448–3449. [Google Scholar] [PubMed]
- Ludwick, K.; Clymer, J.W. Comparative meta-analysis of feline leukemia virus and feline immunodeficiency virus seroprevalence correlated with GDP per capita around the globe. Res. Vet. Sci. 2019, 125, 89–93. [Google Scholar] [CrossRef] [PubMed]
- StatisticsTimes.com. List of Countries by Projected GDP per capita: International Monetary Fund World Economic Outlook (October—2018). Available online: http://statisticstimes.com/economy/countries-by-projected-gdp-capita.php (accessed on 13 August 2019).
- Gomes-Keller, M.A.; Tandon, R.; Gonczi, E.; Meli, M.L.; Hofmann-Lehmann, R.; Lutz, H. Shedding of feline leukemia virus RNA in saliva is a consistent feature in viraemic cats. Vet. Microbiol. 2006, 112, 11–21. [Google Scholar] [CrossRef]
- United Nations Geoscheme for Europe. Available online: https://unstats.un.org/unsd/methodology/m49/ (accessed on 27 October 2019).
- Matouch, O. The rabies situation in Eastern Europe. Dev. Biol. (Basel) 2008, 131, 27–35. [Google Scholar]
- Cliquet, F.; Picard-Meyer, E.; Robardet, E. Rabies in Europe: What are the risks? Expert Rev. Anti-Infect. Ther. 2014, 12, 905–908. [Google Scholar] [CrossRef]
- Lutz, H.; Lehmann, R.; Winkler, G.; Kottwitz, B.; Dittmer, A.; Wolfensberger, C.; Arnold, P. Feline immunodeficiency virus in Switzerland: Clinical aspects and epidemiology in comparison with feline leukemia virus and coronaviruses. Schweiz Arch. Tierheilkd 1990, 132, 217–225. [Google Scholar]
- Willi, B.; Boretti, F.S.; Baumgartner, C.; Tasker, S.; Wenger, B.; Cattori, V.; Meli, M.L.; Reusch, C.E.; Lutz, H.; Hofmann-Lehmann, R. Prevalence, risk factor analysis, and follow-up of infections caused by three feline hemoplasma species in cats in Switzerland. J. Clin. Microbiol. 2006, 44, 961–969. [Google Scholar] [CrossRef]
- Berger, A.; Willi, B.; Meli, M.L.; Boretti, F.S.; Hartnack, S.; Dreyfus, A.; Lutz, H.; Hofmann-Lehmann, R. Feline calicivirus and other respiratory pathogens in cats with Feline calicivirus-related symptoms and in clinically healthy cats in Switzerland. BMC Vet. Res. 2015, 11, 282. [Google Scholar] [CrossRef]
- Gomes-Keller, M.A.; Gonczi, E.; Tandon, R.; Riondato, F.; Hofmann-Lehmann, R.; Meli, M.L.; Lutz, H. Detection of feline leukemia virus RNA in saliva from naturally infected cats and correlation of PCR results with those of current diagnostic methods. J. Clin. Microbiol. 2006, 44, 916–922. [Google Scholar] [CrossRef]
- Cattori, V.; Tandon, R.; Riond, B.; Pepin, A.C.; Lutz, H.; Hofmann-Lehmann, R. The kinetics of feline leukaemia virus shedding in experimentally infected cats are associated with infection outcome. Vet. Microbiol. 2009, 133, 292–296. [Google Scholar] [CrossRef]
- Tandon, R.; Cattori, V.; Gomes-Keller, M.A.; Meli, M.L.; Golder, M.C.; Lutz, H.; Hofmann-Lehmann, R. Quantitation of feline leukaemia virus viral and proviral loads by TaqMan real-time polymerase chain reaction. J. Virol. Methods 2005, 130, 124–132. [Google Scholar] [CrossRef]
- Major, A.; Cattori, V.; Boenzli, E.; Riond, B.; Ossent, P.; Meli, M.L.; Hofmann-Lehmann, R.; Lutz, H. Exposure of cats to low doses of FeLV: Seroconversion as the sole parameter of infection. Vet. Res. 2010, 41, 17. [Google Scholar] [CrossRef]
- Kahle, D.; Wickham, H. ggmap: Spatial Visualization with ggplot2. R J. 2013, 5, 144–161. [Google Scholar] [CrossRef]
- Giraud, T.; Lambert, N. Cartography: Create and Integrate Maps in your R Workflow. J. Open Source Softw. 2016, 1, 54. [Google Scholar] [CrossRef]
- Evans, J.S.; Ram, K. Package ‘spatialEco’: Spatial Analysis and Modelling Utilities. Available online: https://cran.r-project.org/web/packages/spatialEco/spatialEco.pdf (accessed on 4 April 2018).
- Heinze, G.; Schemper, M. A solution to the problem of separation in logistic regression. Stat. Med. 2002, 21, 2409–2419. [Google Scholar] [CrossRef]
- Petrie, A.; Watson, P. Additional techniques. In Statistics for Veterinary and Animal Science, 2nd ed.; Petrie, A., Watson, P., Eds.; Science B. Blackwell Science: Edinburgh, UK, 2006; pp. 191–211. [Google Scholar]
- Breiman, L.; Friedman, J.H.; Olshen, R.A.; Stone, C.H. Classification and Regression Trees; Wadsworth: Pacific Grove, CA, USA, 1984. [Google Scholar]
- Clark, L.A.; Pregibon, D.A. Tress-based models. In Statistical Models; Chambers, J., Hastie, T., Eds.; Wadsworth: Pacific Grove, CA, USA, 1992; pp. 377–419. [Google Scholar]
- Crichton, N.J.; Hinde, J.P.; Marchini, J. Models for diagnosing chest pain: Is CART helpful? Stat. Med. 1997, 16, 717–727. [Google Scholar] [CrossRef]
- Thwaites, G.E.; Chau, T.T.H.; Stepniewska, K.; Phu, N.H.; Chuong, L.V.; Sinh, D.X.; White, N.J.; Parry, C.M.; Farrar, J.J. Diagnosis of adult tuberculous meningitis by use of clinical and laboratory features. Lancet 2002, 360, 1287–1292. [Google Scholar] [CrossRef]
- Saegerman, C.; Speybroeck, N.; Roels, S.; Vanopdenbosch, E.; Thiry, E.; Berkvens, D. Decision support tools for clinical diagnosis of disease in cows with suspected bovine spongiform encephalopathy. J. Clin. Microbiol. 2004, 42, 172–178. [Google Scholar] [CrossRef]
- Speybroeck, N.; Berkvens, D.; Mfoukou-Ntsakala, A.; Aerts, M.; Hens, N.; Van Huylenbroeck, G.; Thys, E. Classification trees versus multinomial models in the analysis of urban farming systems in Central Africa. Agric. Syst. 2004, 80, 133–149. [Google Scholar] [CrossRef]
- Porter, R.S.; Leblond, A.; Lecollinet, S.; Tritz, P.; Cantile, C.; Kutasi, O.; Zientara, S.; Pradier, S.; van Galen, G.; Speybroek, N.; et al. Clinical diagnosis of West Nile fever in equids by classification and regression tree (CART) analysis and comparative study of clinical appearance in three European countries. Transbound. Emerg. Dis. 2011, 58, 197–205. [Google Scholar] [CrossRef]
- Saegerman, C.; Alba-Casals, A.; Garcia-Bocanegra, I.; Dal Pozzo, F.; van Galen, G. Clinical sentinel surveillance of equine West Nile fever, Spain. Transbound. Emerg. Dis. 2016, 63, 184–193. [Google Scholar] [CrossRef]
- Garigliany, M.; Jolly, S.; Dive, M.; Bayrou, C.; Berthemin, S.; Robin, P.; Godenir, R.; Petry, J.; Dahout, S.; Cassart, D.; et al. Risk factors and effect of selective removal on retroviral infections prevalence in Belgian stray cats. Vet. Rec. 2016, 178, 45. [Google Scholar] [CrossRef]
- Saegerman, C.; Porter, S.R.; Humblet, M.F. The use of modelling to evaluate and adapt strategies for animal disease control. Rev. Sci. Tech. OIE 2011, 30, 555–569. [Google Scholar] [CrossRef]
- Jarrett, O.; Golder, M.C.; Stewart, M.F. Detection of transient and persistent feline leukaemia virus infections. Vet. Rec 1982, 110, 225–228. [Google Scholar] [CrossRef]
- Jarrett, O.; Pacitti, A.M.; Hosie, M.J.; Reid, G. Comparison of diagnostic methods for feline leukemia virus and feline immunodeficiency virus. J. Am. Vet. Med. Assoc. 1991, 199, 1362–1364. [Google Scholar]
- Miyazawa, T.; Jarrett, O. Feline leukaemia virus proviral DNA detected by polymerase chain reaction in antigenaemic but non-viraemic (‘discordant’) cats. Arch. Virol. 1997, 142, 323–332. [Google Scholar] [CrossRef]
- Hayes, K.A.; Rojko, J.L.; Mathes, L.E. Incidence of localized feline leukemia virus infection in cats. Am. J. Vet. Res. 1992, 53, 604–607. [Google Scholar]
- Belák, S. (Swedish University of Agricultural Sciences (SLU), Department of Biomedical Sciences and Veterinary Public Health (BVF), 750 07 Uppsala, Sweden; e-mail dated, 2019) relating to an information given by Dr. Lotta Gunnarsson (Swedish National Veterinary Institute SVA, SE-751 89 Uppsala, Sweden; e-mail dated May 20, 2019). 27 May.
- Sukura, A.; Salminen, T.; Lindberg, L.A. A survey of FIV antibodies and FeLV antigens in free-roaming cats in the capital area of Finland. Acta Vet. Scand. 1992, 33, 9–14. [Google Scholar]
- Brutus, K. Prevalence of Feline Immunodeficiency Virus and Feline Leukemia Virus Infection in Shelter Cats in Tartu: Association with Age, Gender, Rhinitis and Serum Haptoglobin Concentration. Ph.D. Thseis, Estonian University of Life Sciences, Tartu, Estonia, 2017. [Google Scholar]
- Stavisky, J.; Dean, R.S.; Molloy, M.H. Prevalence of and risk factors for FIV and FeLV infection in two shelters in the United Kingdom (2011–2012). Vet. Rec. 2017, 181, 451. [Google Scholar] [CrossRef]
- Muirden, A. Prevalence of feline leukaemia virus and antibodies to feline immunodeficiency virus and feline coronavirus in stray cats sent to an RSPCA hospital. Vet. Rec. 2002, 150, 621–625. [Google Scholar] [CrossRef]
- Scherk, M.A.; Ford, R.B.; Gaskell, R.M.; Hartmann, K.; Hurley, K.F.; Lappin, M.R.; Levy, J.K.; Little, S.E.; Nordone, S.K.; Sparkes, A.H. 2013 AAFP Feline Vaccination Advisory Panel Report. J. Feline Med. Surg. 2013, 15, 785–808. [Google Scholar] [CrossRef]
- Juvet, F.; Brennan, S.; Mooney, C.T. Assessment of feline blood for transfusion purposes in the Dublin area of Ireland. Vet. Rec. 2011, 168, 352. [Google Scholar] [CrossRef]
- Dorny, P.; Speybroeck, N.; Verstraete, S.; Baeke, M.; De Becker, A.; Berkvens, D.; Vercruysse, J. Serological survey of Toxoplasma gondii, feline immunodeficiency virus and feline leukaemia virus in urban stray cats in Belgium. Vet. Rec. 2002, 151, 626–629. [Google Scholar] [CrossRef]
- Cabral Campello Duarte Turras, M. Estudo da prevalencia de FIV/FeLV numa população de 88 gatos errantes da região metropolitana de Lisboa. Ph.D. Thesis, Faculdade de Medicina Veterinária Lisboa, Lisboa, Portugal, 2014. [Google Scholar]
- Iatta, R.; Furlanello, T.; Colella, V.; Tarallo, V.D.; Latrofa, M.S.; Brianti, E.; Trerotoli, P.; Decaro, N.; Lorusso, E.; Schunack, B.; et al. A nationwide survey of Leishmania infantum infection in cats and associated risk factors in Italy. PLoS Negl. Trop. Dis. 2019, 13, e0007594. [Google Scholar] [CrossRef]
- Spada, E.; Proverbio, D.; della Pepa, A.; Perego, R.; Baggiani, L.; DeGiorgi, G.B.; Domenichini, G.; Ferro, E.; Cremonesi, F. Seroprevalence of feline immunodeficiency virus, feline leukaemia virus and Toxoplasma gondii in stray cat colonies in northern Italy and correlation with clinical and laboratory data. J. Feline Med. Surg. 2012, 14, 369–377. [Google Scholar] [CrossRef]
- Spada, E.; Canzi, I.; Baggiani, L.; Perego, R.; Vitale, F.; Migliazzo, A.; Proverbio, D. Prevalence of Leishmania infantum and co-infections in stray cats in northern Italy. Comp. Immunol. Microb. 2016, 45, 53–58. [Google Scholar] [CrossRef]
- Pennisi, M.G.; Hartmann, K.; Addie, D.D.; Lutz, H.; Gruffydd-Jones, T.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Horzinek, M.C.; Hosie, M.J.; et al. Blood transfusion in cats: ABCD guidelines for minimising risks of infectious iatrogenic complications. J. Feline Med. Surg. 2015, 17, 588–593. [Google Scholar] [CrossRef]
- Persechino, A.; Oliva, G.; Cerundolo, R. Seroepidemiological survey of feline T-lymphotropic lentivurs infeciton in cats of Campania region. Atti. Soc. Ital. Sci. Vet. (SISVet) 1989, 63, 1007–1008. (In Italian) [Google Scholar]
- Persichetti, M.F.; Pennisi, M.G.; Vullo, A.; Masucci, M.; Migliazzo, A.; Solano-Gallego, L. Clinical evaluation of outdoor cats exposed to ectoparasites and associated risk for vector-borne infections in southern Italy. Parasites Vectors 2018, 11, 136. [Google Scholar] [CrossRef]
- Priolo, V.; Martinez-Orellana, P.; Pennisi, M.G.; Masucci, M.; Prandi, D.; Ippolito, D.; Bruno, F.; Castelli, G.; Solano-Gallego, L. Leishmania infantum-specific IFN-gamma production in stimulated blood from cats living in areas where canine leishmaniosis is endemic. Parasites Vector 2019, 12. [Google Scholar] [CrossRef]
- Bechtle, G.; Pennisi, M.G.; Catarsini, O. Studio sieroepidemiologico su FIV, FeLV, FIPV in gatti randagi di una piccola area suburbana. Obiettivi. E Doc. Vet. 1992, 13, 29–32. [Google Scholar]
- Pennisi, M.G.; Borruto, G.; Masucci, M.; Pugliese, A. Pannello sierologico di gatti semiliberi e/o di gattile della Sicilia Orientale. In Proceedings of the VII Congresso Associazione Siciliana Sanità Veterinaria (ASSaV), La Valletta, Malta, 24–25 November 2000; pp. 169–177. (In Italian). [Google Scholar]
- Ippolito, D.; Priolo, V.; Mangano, C.; Persichetti, M.F.; Migliazzo, A.; Purpari, G.; Masucci, M.; Pennisi, M.G. Antibody prevalence of Leishmania infantum in dogs and cats of Messina (Sicily, Italy). In Proceedings of the WorldLeish VI, Toledo, Spain, 16–20 May 2017; p. 1063. [Google Scholar]
- Pennisi, M.G.; Maxia, L.; Vitale, F.; Masucci, M.; Borruto, G.; Caracappa, S. PCR screening for Leishmanial infection of cats from an endemic area (Italian). Atti. Soc. Ital. Sci. Vet. (SISVet) 2000, 56, 215–216. (In Italian) [Google Scholar]
- Pennisi, M.G.; Masucci, M.; Catarsini, O. Presenza di anticorpi anti-Leishmania in gatti FIV+ che vivono in zona endemic. Atti. Soc. Ital. Sci. Vet. (SISVet) 1998, 54, 265–266. (In Italian) [Google Scholar]
- Otranto, D.; Napoli, E.; Latrofa, M.S.; Annoscia, G.; Tarallo, V.D.; Greco, G.; Lorusso, E.; Gulotta, L.; Falsone, L.; Basano, F.S.; et al. Feline and canine leishmaniosis and other vector-borne diseases in the Aeolian Islands: Pathogen and vector circulation in a confined environment. Vet. Parasitol. 2017, 236, 144–151. [Google Scholar] [CrossRef]
- Natoli, E. Spacing Pattern in a Colony of Urban Stray Cats (Felis-Catus L) in the Historic Center of Rome. Appl. Anim. Behav. Sci. 1985, 14, 289–304. [Google Scholar] [CrossRef]
- Natoli, E.; Malandrucco, L.; Minati, L.; Verzichi, S.; Perino, R.; Longo, L.; Pontecorvo, F.; Faini, A. Evaluation of Unowned Domestic Cat Management in the Urban Environment of Rome After 30 Years of Implementation of the No-Kill Policy (National and Regional Laws). Front. Vet. Sci. 2019, 6, 31. [Google Scholar] [CrossRef]
- Voslarova, E.; Passantino, A. Stray dog and cat laws and enforcement in Czech Republic and in Italy. Ann. Ist Super Sanita 2012, 48, 97–104. [Google Scholar] [CrossRef]
- Ravicini, S.; Pastor, J.; Hawley, J.; Brewer, M.; Castro-Lopez, J.; Beall, M.; Lappin, M.R. Prevalence of selected infectious disease agents in stray cats in Catalonia, Spain. JFMS Open Rep. 2016, 2, 2055116916634109. [Google Scholar] [CrossRef]
- Rypula, K.; Ploneczka-Janeczko, K.; Bierowiec, K.; Kumala, A.; Sapikowski, G. Prevalence of viral infections in cats in southwestern Poland in the years 2006 to 2010. Berl Munch Tierarztl Wochenschr 2014, 127, 163–165. [Google Scholar]
- Kita, P.; Frymus, T. Occurence of feline leukemia virus in Warsaw. Med. Wet. 2003, 217–220. (In Polish) [Google Scholar]
- Ondrejka, R.O.; Slepecká, E.; Ondrejková, A.; Süli, J.; Pošiv&aková, S.; Beníšek, Z.; Prokeš, M.A. Survey of the feline AIDS prevalence in the Slovak Republic. J. Clin. Immunol. Immunopathol. Res. 2009, 2009, 1–6. [Google Scholar]
- Galdo Novo, S.; Bucafusco, D.; Diaz, L.M.; Bratanich, A.C. Viral diagnostic criteria for Feline immunodeficiency virus and Feline leukemia virus infections in domestic cats from Buenos Aires, Argentina. Rev. Argent. Microbiol. 2016, 48, 293–297. [Google Scholar] [CrossRef]
- Chhetri, B.K.; Berke, O.; Pearl, D.L.; Bienzle, D. Comparison of risk factors for seropositivity to feline immunodeficiency virus and feline leukemia virus among cats: A case-case study. BMC Vet. Res. 2015, 11, 30. [Google Scholar] [CrossRef]
- Goldkamp, C.E.; Levy, J.K.; Edinboro, C.H.; Lachtara, J.L. Seroprevalences of feline leukemia virus and feline immunodeficiency virus in cats with abscesses or bite wounds and rate of veterinarian compliance with current guidelines for retrovirus testing. J. Am. Vet. Med. Assoc. 2008, 232, 1152–1158. [Google Scholar] [CrossRef]
- Hosie, M.J.; Addie, D.D.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Horzinek, M.C.; Lloret, A.; Lutz, H.; et al. Matrix vaccination guidelines: 2015 ABCD recommendations for indoor/outdoor cats, rescue shelter cats and breeding catteries. J. Feline Med. Surg. 2015, 17, 583–587. [Google Scholar] [CrossRef]
- Hoover, E.A.; Olsen, R.G.; Hardy, W.D., Jr.; Schaller, J.P.; Mathes, L.E. Feline leukemia virus infection: Age-related variation in response of cats to experimental infection. J. Natl. Cancer Inst. 1976, 57, 365–369. [Google Scholar] [CrossRef]
- Radford, A.D.; Addie, D.; Belak, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Hosie, M.J.; Lloret, A.; et al. Feline calicivirus infection. ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 556–564. [Google Scholar] [CrossRef]
- Addie, D.; Belak, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Hosie, M.J.; Lloret, A.; Lutz, H.; et al. Feline infectious peritonitis. ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 594–604. [Google Scholar] [CrossRef]
- Polak, K.C.; Levy, J.K.; Crawford, P.C.; Leutenegger, C.M.; Moriello, K.A. Infectious diseases in large-scale cat hoarding investigations. Vet. J. 2014, 201, 189–195. [Google Scholar] [CrossRef]
- Nesina, S.; Katrin Helfer-Hungerbuehler, A.; Riond, B.; Boretti, F.S.; Willi, B.; Meli, M.L.; Grest, P.; Hofmann-Lehmann, R. Retroviral DNA--the silent winner: Blood transfusion containing latent feline leukemia provirus causes infection and disease in naive recipient cats. Retrovirology 2015, 12, 105. [Google Scholar] [CrossRef] [PubMed]
- Gleich, S.; Hartmann, K. Hematology and serum biochemistry of feline immunodeficiency virus-infected and feline leukemia virus-infected cats. J. Vet. Intern. Med. 2009, 23, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Cotter, S.M. Anemia associated with feline leukemia virus infection. J. Am. Vet. Med. Assoc. 1979, 175, 1191–1194. [Google Scholar] [PubMed]
- Shelton, G.H.; Linenberger, M.L. Hematologic abnormalities associated with retroviral infections in the cat. Semin. Vet. Med. Surg. (Small Anim) 1995, 10, 220–233. [Google Scholar]
- Abkowitz, J.L.; Holly, R.D.; Grant, C.K. Retrovirus-induced feline pure red cell aplasia. Hematopoietic progenitors are infected with feline leukemia virus and erythroid burst-forming cells are uniquely sensitive to heterologous complement. J. Clin. Investig. 1987, 80, 1056–1063. [Google Scholar] [CrossRef] [PubMed]
- Garden, O.A.; Kidd, L.; Mexas, A.M.; Chang, Y.M.; Jeffery, U.; Blois, S.L.; Fogle, J.E.; MacNeill, A.L.; Lubas, G.; Birkenheuer, A.; et al. ACVIM consensus statement on the diagnosis of immune-mediated haemolytic anaemia in dogs and cats. J. Vet. Intern. Med. 2019, 33, 313–334. [Google Scholar] [CrossRef] [PubMed]
- Francis, D.P.; Essex, M.; Hardy, W.D., Jr. Excretion of feline leukaemia virus by naturally infected pet cats. Nature 1977, 269, 252–254. [Google Scholar] [CrossRef]






| Country or Country Group 1 | Vets Planned | Participating vets | Samples Shipped | Samples and Data Returned | Return Rate % | No of FeLV-pos. 2 | FeLV Prevalence % (95% CI) 3 |
|---|---|---|---|---|---|---|---|
| Northern Europe | |||||||
| Denmark | 40 | 40 | 400 | 277 | 69.3 | 0 | 0.0 (0.0–1.4) |
| Finland | 40 | 40 | 400 | 290 | 72.5 | 0 | 0.0 (0.0–1.3) |
| Ireland | 40 | 39 | 390 | 136 | 34.9 | 7 | 5.1 (2.5–10.2) |
| Lithuania, Latvia, Estonia | 40 | 40 | 400 | 266 | 66.5 | 4 | 1.5 (0.6–3.8) |
| Lithuania | 19 | 19 | 190 | 143 | 75.3 | 4 | |
| Latvia | 12 | 12 | 120 | 68 | 56.7 | 0 | |
| Estonia | 9 | 9 | 90 | 55 | 61.1 | 0 | |
| Norway | 40 | 38 | 380 | 205 | 53.9 | 0 | 0.0 (0.0–1.8) |
| Sweden | 40 | 40 | 400 | 343 | 85.8 | 0 | 0.0 (0.0–1.1) |
| United Kingdom | 40 | 40 | 400 | 136 | 34.0 | 1 | 0.7 (3.8 × 10−4–4.0) |
| England | 32 | 32 | 320 | 119 | 37.1 | 1 | |
| Scotland | 4 | 4 | 40 | 10 | 25.0 | 0 | |
| Northern Ireland | 2 | 2 | 20 | 0 | 0.0 | 0 | |
| Wales | 2 | 2 | 20 | 7 | 35.0 | 0 | |
| Eastern Europe | |||||||
| Bulgaria, Romania | 40 | 24 | 240 | 90 | 37.5 | 0 | 0.0 (0.0–4.1) |
| Bulgaria | 11 | 11 | 110 | 90 | 81.8 | 0 | |
| Romania | 29 | 13 | 130 | 0 | 0 | n.a. | |
| Czech Republic | 40 | 40 | 400 | 361 | 90.3 | 8 | 2.2 (1.1–4.3) |
| Hungary | 40 | 40 | 400 | 219 | 54.8 | 13 | 5.9 (3.5–9.9) |
| Poland | 40 | 40 | 400 | 340 | 85.0 | 17 | 5.0 (3.1–7.9) |
| Slovakia | 40 | 40 | 400 | 255 | 63.8 | 5 | 2.0 (0.8–4.5) |
| Southern Europe | |||||||
| Croatia | 40 | 40 | 400 | 198 | 49.5 | 9 | 4.5 (2.4–8.4) |
| Greece | 40 | 0 | 0 | n.a. | n.a. | n.a. | |
| Portugal | 40 | 40 | 400 | 330 | 82.5 | 29 | 8.8 (6.2–12.3) |
| Spain | 40 | 40 | 400 | 352 | 88.0 | 9 | 2.6 (1.4–4.8) |
| Italy and Malta | 40 | 40 | 400 | 349 | 87.3 | 20 | 5.7 (3.7–8.7) |
| Italy | 39 | 39 | 390 | 340 | 87.2 | 20 | |
| Malta | 1 | 1 | 10 | 9 | 90.0 | 0 | |
| Western Europe | |||||||
| Austria | 40 | 40 | 400 | 309 | 77.3 | 4 | 1.3 (0.5–3.3) |
| Belgium, Luxembourg | 40 | 40 | 400 | 287 | 71.8 | 3 | 1.0 (0.3–3.0) |
| Belgium | 38 | 38 | 380 | 278 | 73.2 | 3 | |
| Luxembourg | 2 | 2 | 20 | 9 | 45.0 | 0 | |
| France | 40 | 40 | 400 | 301 | 75.3 | 3 | 1.0 (0.3–2.9) |
| Germany | 40 | 40 | 400 | 306 | 76.5 | 1 | 0.3 (1.7 × 10−4–1.8) |
| Netherlands | 40 | 40 | 400 | 356 | 89.0 | 0 | 0.0 (0.0–1.0) |
| Switzerland, Liechtenstein | 40 | 40 | 400 | 299 | 74.8 | 8 | 2.7 (1.4–5.2) |
| Switzerland | 39 | 39 | 390 | 290 | 74.4 | 7 | |
| Liechtenstein | 1 | 1 | 10 | 9 | 90.0 | 1 | |
| Total | 920 | 861 | 8610 | 6005 | 69.7 | 141 | 2.3 (2.0–2.8) |
| Variables | Modalities | All Cats (n = 6005) | FeLV-Positive Cats (n = 141) |
|---|---|---|---|
| Health | Healthy | 4060 (67.6 1) | 66 (46.8 2) |
| Sick | 1945 (32.4) | 75 (53.2) | |
| Age | <1 year | 1826 (30.4) | 31 (22.0) |
| 1 to ≤6 years | 2271 (37.8) | 80 (56.7) | |
| >6 years | 1908 (31.8) | 30 (21.3) | |
| Sex | Female intact | 850 (14.2) | 15 (10.6) |
| Female spayed | 1941 (32.3) | 38 (27.0) | |
| Male intact | 914 (15.2) | 37 (26.2) | |
| Male castrated | 2181 (36.3) | 49 (34.8) | |
| Not sure | 119 (2.0) | 2 (1.4) | |
| Pedigree | No | 5156 (85.9) | 139 (98.6) |
| Yes | 792 (13.2) | 2 (1.4) | |
| Not sure | 57 (0.9) | 0 (0.0) | |
| Habitat | Private | 5151 (85.9) | 111 (78.7) |
| Breeder | 177 (2.9) | 0 (0.0) | |
| Shelter | 179 (3.0) | 7 (5.0) | |
| Rescue cat | 446 (7.4) | 21 (14.9) | |
| Other | 52 (0.9) | 2 (1.4) | |
| Multicat environment | Yes | 3373 (56.2) | 85 (60.3) |
| No | 2380 (39.6) | 44 (31.2) | |
| Not sure | 252 (4.2) | 12 (8.5) | |
| Number of cats in group | 1 | 2380 (39.6) | 44 (31.2) |
| 2 | 1670 (27.8) | 32 (22.7) | |
| 3 | 628 (10.5) | 11 (7.8) | |
| 4 | 295 (4.9) | 6 (4.3) | |
| ≥5 | 708 (11.8) | 36 (25.5) | |
| Not sure | 324 (5.4) | 12 (8.5) | |
| Access | Indoor only | 2193 (36.5) | 32 (22.7) |
| Indoor and outdoor | 3245 (54.0) | 83 (58.9) | |
| Outdoor only | 388 (6.5) | 23 (16.3) | |
| FeLV vaccination | Yes | 1462 (24.3) | 14 (9.9) |
| No | 3938 (65.6) | 106 (75.2) | |
| Not sure | 605 (10.1) | 21 (14.9) | |
| Last FeLV vaccination | Never | 3938 (65.6) | 106 (75.2) |
| <1 year | 943 (15.7) | 8 (5.7) | |
| 1 to ≤3 years | 337 (5.6) | 3 (2.1) | |
| >3 years | 182 (3.0) | 3 (2.1) | |
| Not sure | 605 (10.1) | 21 (14.9) |
| Variables | Modalities | FeLV Prevalence | 95% Confidence Interval a | Odds Ratio | 95% Confidence Interval b | p-value |
|---|---|---|---|---|---|---|
| Europe | Eastern | 3.4 | 2.5–4.6 | Reference | - | - |
| Northern | 0.7 | 0.4–1.7 | 0.21 | (0.11–0.40) | <0.001 * | |
| Southern | 5.5 | 4.2–6.9 | 1.64 | (1.11–2.42) | 0.013 * | |
| Western | 1.0 | 0.6–1.6 | 0.29 | (0.17–0.51) | <0.001 * | |
| Pedigree | No | 2.7 | 2.2–3.1 | Reference | - | - |
| Yes | 0.3 | 0.0–1.0 | 0.09 | (0.02–0.37) | 0.001 * | |
| Habitat | Breeder | 0.0 | 0.0–2.1 | Reference | - | - |
| Rescue cat | 4.7 | 2.8–6.8 | 17.94 | (1.08–297.85) | 0.044 * | |
| Private | 2.2 | 1.7–2.5 | 17.57 | (0.82–372.10) | 0.07 | |
| Shelter | 3.9 | 1.5–7.6 | 7.85 | (0.49–126.89) | 0.15 | |
| Other | 3.8 | 5.0–13.2 | 15.43 | (0.87–272.42) | 0.06 | |
| Number of cats in group | 1 | 2.1 | 1.6–2.7 | Reference | - | - |
| 2 | 1.9 | 1.3–2.7 | 0.92 | (0.60–1.43) | 0.72 | |
| 3 | 1.8 | 0.9–3.1 | 0.84 | (0.44–1.62) | 0.61 | |
| 4 | 2.0 | 0.7–4.4 | 0.98 | (0.42–2.30) | 0.97 | |
| ≥5 | 5.1 | 3.6–7.0 | 2.53 | (1.65–3.88) | <0.001 * | |
| Sex | Female intact | 1.8 | 1.0–2.9 | Reference | - | - |
| Female spayed | 2.0 | 1.4–2.7 | 1.11 | (0.61–2.03) | 0.73 | |
| Male intact | 4.0 | 2.9–5.5 | 2.35 | (1.28–4.31) | 0.006 * | |
| Male castrated | 2.2 | 1.7–3.0 | 1.28 | (0.71–2.29) | 0.41 | |
| Not sure | 1.7 | 0.2–5.9 | 0.95 | (0.21–4.21) | 0.95 | |
| Age | < 1 year | 1.7 | 1.2–2.4 | Reference | - | - |
| 1 to ≤6 years | 3.5 | 2.8–4.4 | 2.11 | (1.39–3.22) | <0.001 * | |
| >6 years | 1.6 | 1.1–2.2 | 0.92 | (0.56–1.53) | 0.77 | |
| Access | Indoor only | 1.5 | 1.0–2.1 | Reference | - | - |
| In- and outdoor | 2.6 | 2.0–3.1 | 1.77 | (1.17–2.67) | 0.006 * | |
| Outdoor only | 5.9 | 3.8–8.8 | 4.26 | (2.46–7.35) | 0.001 * | |
| Not sure | 1.7 | 0.3–4.8 | 1.15 | (0.35–3.80) | 0.82 | |
| Last FeLV vaccination | Never | 2.7 | 2.2–3.2 | Reference | - | - |
| <1 year | 0.8 | 0.4–1.7 | 0.31 | (0.15–0.64) | 0.001 * | |
| 1 to ≤3 years | 0.9 | 0.2–2.6 | 0.32 | (0.10–1.03) | 0.056 | |
| >3 years | 1.6 | 0.3–4.7 | 0.61 | (0.19–1.93) | 0.40 | |
| Not sure | 3.5 | 2.2–5.3 | 1.30 | (0.81–2.09) | 0.28 | |
| Health | Healthy | 1.6 | 1.3–2.1 | Reference | - | - |
| Sick | 3.9 | 3.0–4.8 | 2.43 | (1.74–3.39) | <0.001 * |
| Variables | Modalities | FeLV Prevalence | 95% Confidence Interval a | Odds Ratio | 95% Confidence Interval b | p-value |
|---|---|---|---|---|---|---|
| Europe | Eastern | 3.4 | 2.5–4.6 | Reference | - | - |
| Northern | 0.7 | 0.4–1.7 | 0.29 | (0.15–0.56) | <0.001 * | |
| Southern | 5.5 | 4.2–6.9 | 1.81 | (1.20–2.72) | 0.005 * | |
| Western | 1.0 | 0.6–1.6 | 0.42 | (0.23–0.74) | 0.003 * | |
| Pedigree | No | 2.7 | 2.2–3.1 | Reference | - | - |
| Yes | 0.3 | 0.0–1.0 | 0.15 | (0.04–0.60) | 0.008 * | |
| Number of cats in group | 1 | 2.1 | 1.6–2.7 | Reference | - | |
| 2 | 1.9 | 1.3–2.7 | 0.96 | (0.62–1.51) | 0.87 | |
| 3 | 1.8 | 0.9–3.1 | 0.79 | (0.41–1.54) | 0.49 | |
| 4 | 2.0 | 0.7–4.4 | 0.90 | (0.39–2.15) | 0.82 | |
| ≥5 | 5.1 | 3.6–7.0 | 1.63 | (1.03–2.58) | 0.040 * | |
| Sex | Female intact | 1.8 | 1.0–2.9 | Reference | - | - |
| Female spayed | 2.0 | 1.4–2.7 | 1.38 | (0.72–2.64) | 0.33 | |
| Male intact | 4.0 | 2.9–5.5 | 2.24 | (1.20–4.18) | 0.01 * | |
| Male castrated | 2.2 | 1.7–3.0 | 1.48 | (0.79–2.78) | 0.23 | |
| Not sure | 1.7 | 0.2–5.9 | 0.97 | (0.21–4.53) | 0.84 | |
| Age category | < 1 year | 1.7 | 1.2–2.4 | Reference | - | - |
| 1 to ≤6 years | 3.5 | 2.8–4.4 | 2.04 | (1.27–3.28) | 0.003 * | |
| >6 years | 1.6 | 1.1–2.2 | 1.01 | (0.56–1.83) | 0.97 | |
| Access | Indoor only | 1.5 | 1.0–2.1 | Reference | - | - |
| In- and outdoor | 2.6 | 2.0–3.1 | 1.72 | (1.12–2.65) | 0.01 * | |
| Outdoor only | 5.9 | 3.8–8.8 | 1.88 | (1.03–3.44) | 0.04 * | |
| Not sure | 1.7 | 0.3–4.8 | 1.07 | (0.31–3.69) | 0.92 | |
| Last FeLV vaccination | Never | 2.7 | 2.2–3.2 | Reference | - | - |
| <1 year | 0.8 | 0.4–1.7 | 0.49 | (0.23–1.03) | 0.06 | |
| 1 to ≤3 years | 0.9 | 0.2–2.6 | 0.39 | (0.12–1.26) | 0.11 | |
| >3 years | 1.6 | 0.3–4.7 | 0.79 | (0.24–2.62) | 0.70 | |
| Not sure | 3.5 | 2.2–5.3 | 1.40 | (0.85–2.33) | 0.19 | |
| Health | Healthy | 1.6 | 1.3–2.1 | Reference | - | - |
| Sick | 3.9 | 3.0–4.8 | 2.04 | (1.41–2.90) | <0.001 * |
| Clinical Problem | FeLV-Negative Sick Cats (%) | FeLV-Positive Sick Cats (%) | Odds Ratio (95% Confidence Interval) | pF * |
|---|---|---|---|---|
| Anaemia Yes No | 23 (1.2) 1847 (98.8) | 8 (10.7) 67 (89.3) | 9.6 (4.4–21.4) | <0.0001 |
| Anorexia Yes No | 45 (2.4) 1825 (97.6) | 6 (8.0) 69 (92.0) | 3.5 (1.6–8.3) | 0.0122 |
| Gingivitis and/or stomatitis Yes No | 121 (6.5) 1749 (93.5) | 11 (14.7) 64 (85.3) | 2.5 (1.3–4.8) | 0.0152 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Studer, N.; Lutz, H.; Saegerman, C.; Gönczi, E.; Meli, M.L.; Boo, G.; Hartmann, K.; Hosie, M.J.; Moestl, K.; Tasker, S.; et al. Pan-European Study on the Prevalence of the Feline Leukaemia Virus Infection – Reported by the European Advisory Board on Cat Diseases (ABCD Europe). Viruses 2019, 11, 993. https://doi.org/10.3390/v11110993
Studer N, Lutz H, Saegerman C, Gönczi E, Meli ML, Boo G, Hartmann K, Hosie MJ, Moestl K, Tasker S, et al. Pan-European Study on the Prevalence of the Feline Leukaemia Virus Infection – Reported by the European Advisory Board on Cat Diseases (ABCD Europe). Viruses. 2019; 11(11):993. https://doi.org/10.3390/v11110993
Chicago/Turabian StyleStuder, Nadine, Hans Lutz, Claude Saegerman, Enikö Gönczi, Marina L. Meli, Gianluca Boo, Katrin Hartmann, Margaret J. Hosie, Karin Moestl, Séverine Tasker, and et al. 2019. "Pan-European Study on the Prevalence of the Feline Leukaemia Virus Infection – Reported by the European Advisory Board on Cat Diseases (ABCD Europe)" Viruses 11, no. 11: 993. https://doi.org/10.3390/v11110993
APA StyleStuder, N., Lutz, H., Saegerman, C., Gönczi, E., Meli, M. L., Boo, G., Hartmann, K., Hosie, M. J., Moestl, K., Tasker, S., Belák, S., Lloret, A., Boucraut-Baralon, C., Egberink, H. F., Pennisi, M.-G., Truyen, U., Frymus, T., Thiry, E., Marsilio, F., ... Hofmann-Lehmann, R. (2019). Pan-European Study on the Prevalence of the Feline Leukaemia Virus Infection – Reported by the European Advisory Board on Cat Diseases (ABCD Europe). Viruses, 11(11), 993. https://doi.org/10.3390/v11110993