Histological and Nanomechanical Properties of a New Nanometric Hydroxiapatite Implant Surface. An In Vivo Study in Diabetic Rats


 , and
, and 
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Induction of Diabetes Mellitus
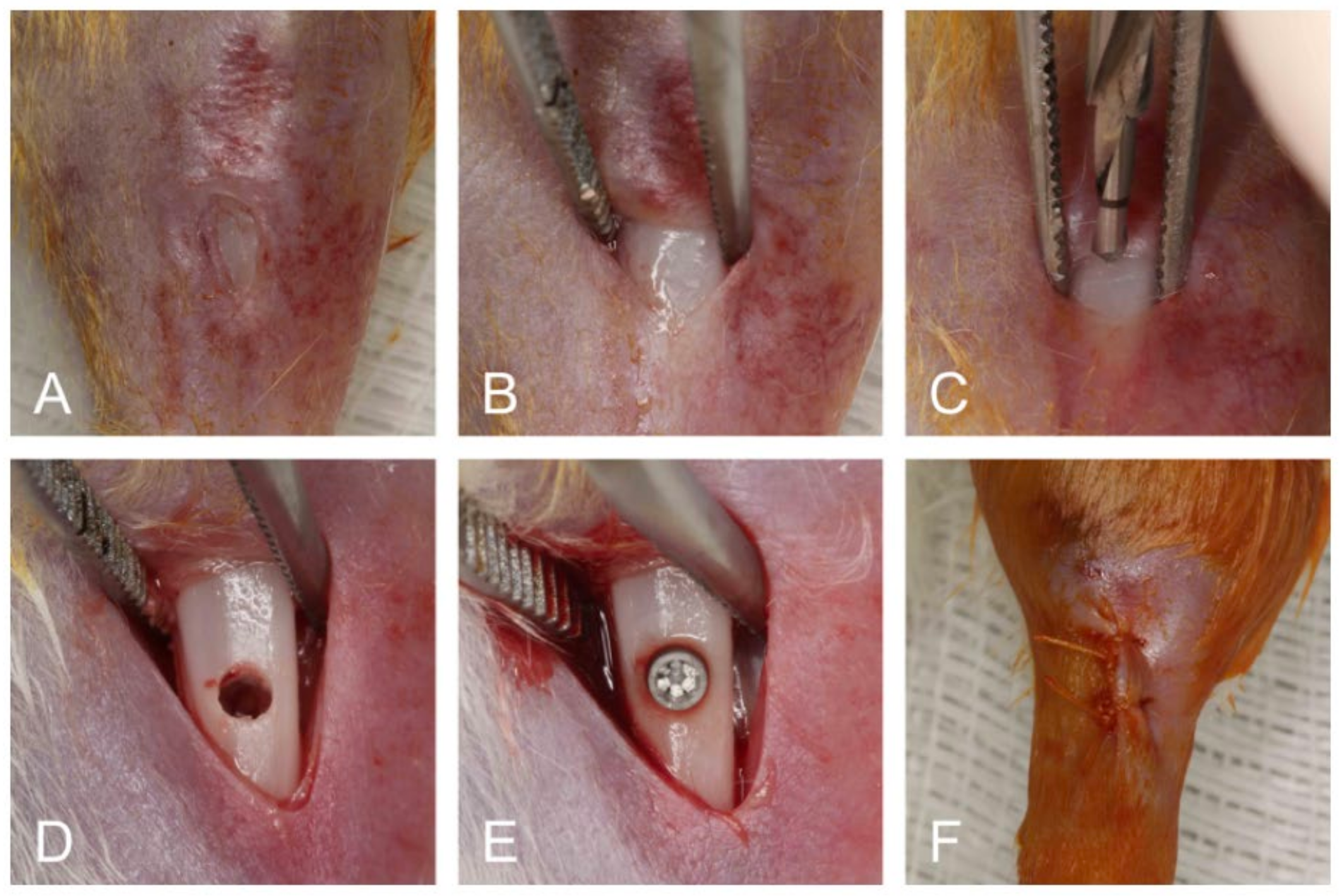
2.3. Surgical Procedures
2.4. Experimental Groups
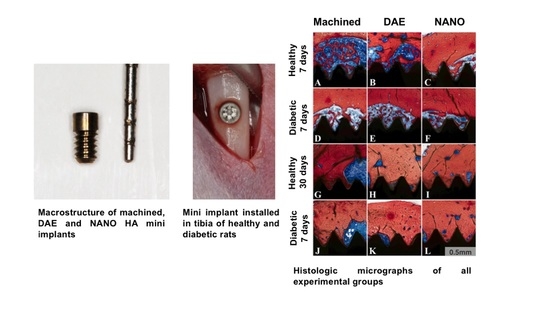
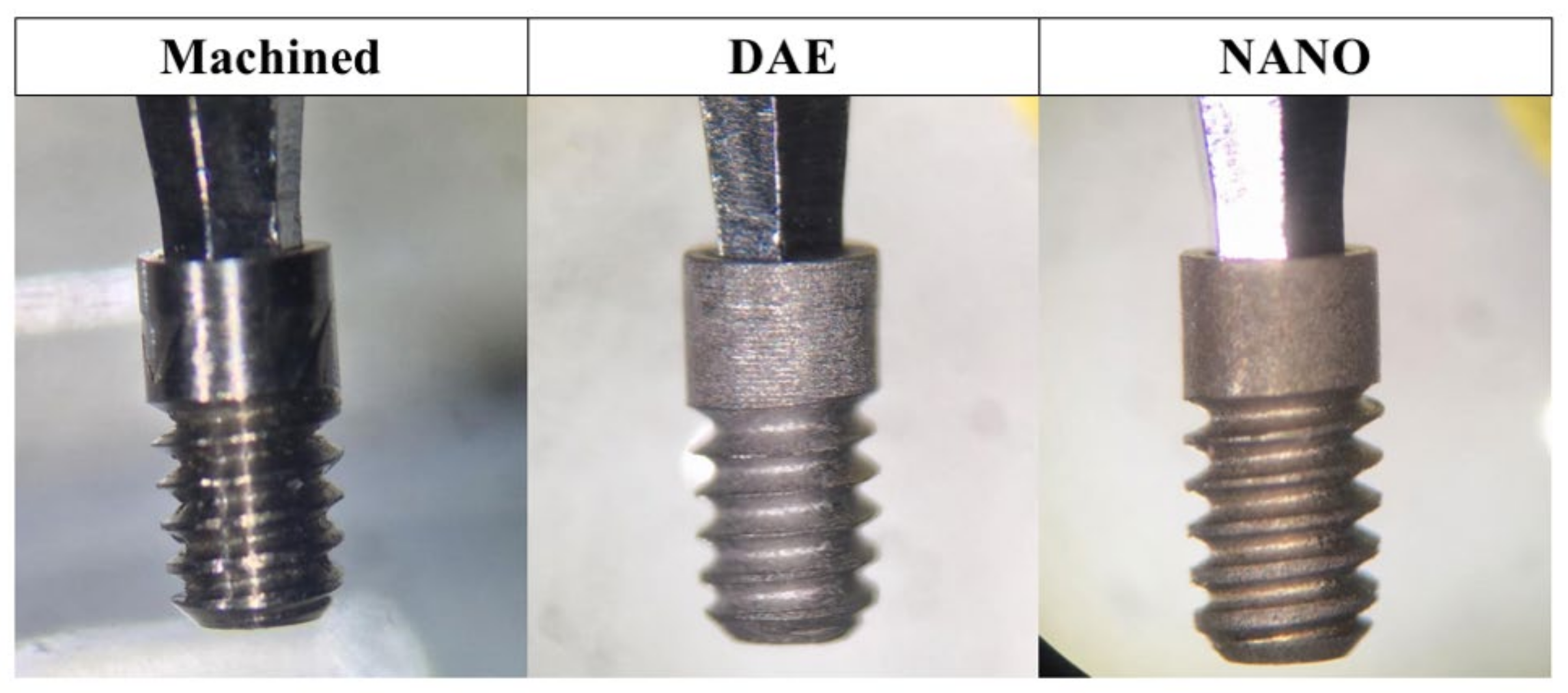
2.5. Implant Design
2.5.1. Machined Surface
2.5.2. DAE Surface
2.5.3. NANO Surface
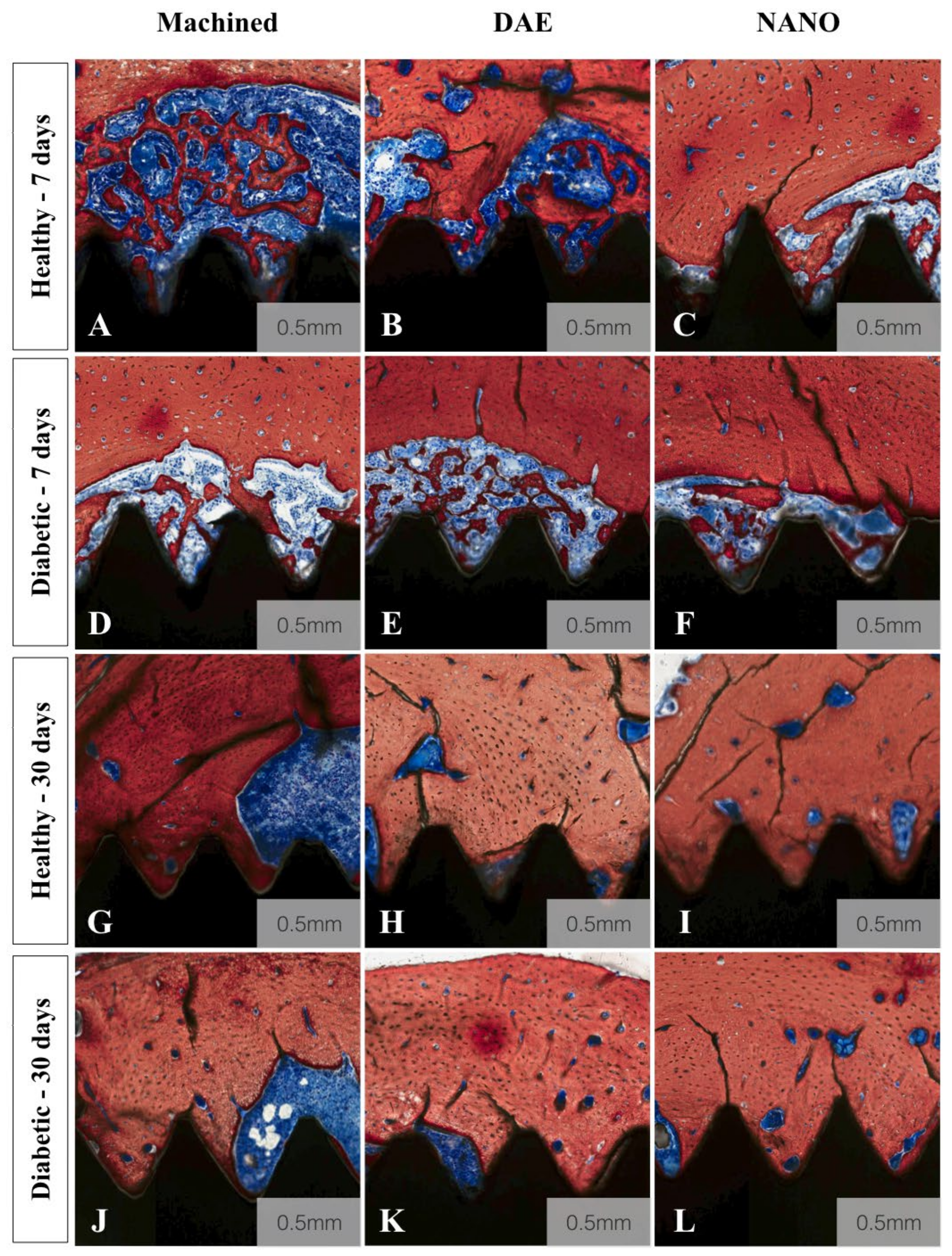
2.6. Histologic Sectioning and Histomorphometry
2.7. Nanoindentation Assay
2.8. Statistical Analysis
3. Results
3.1. Histomorphometric Analysis
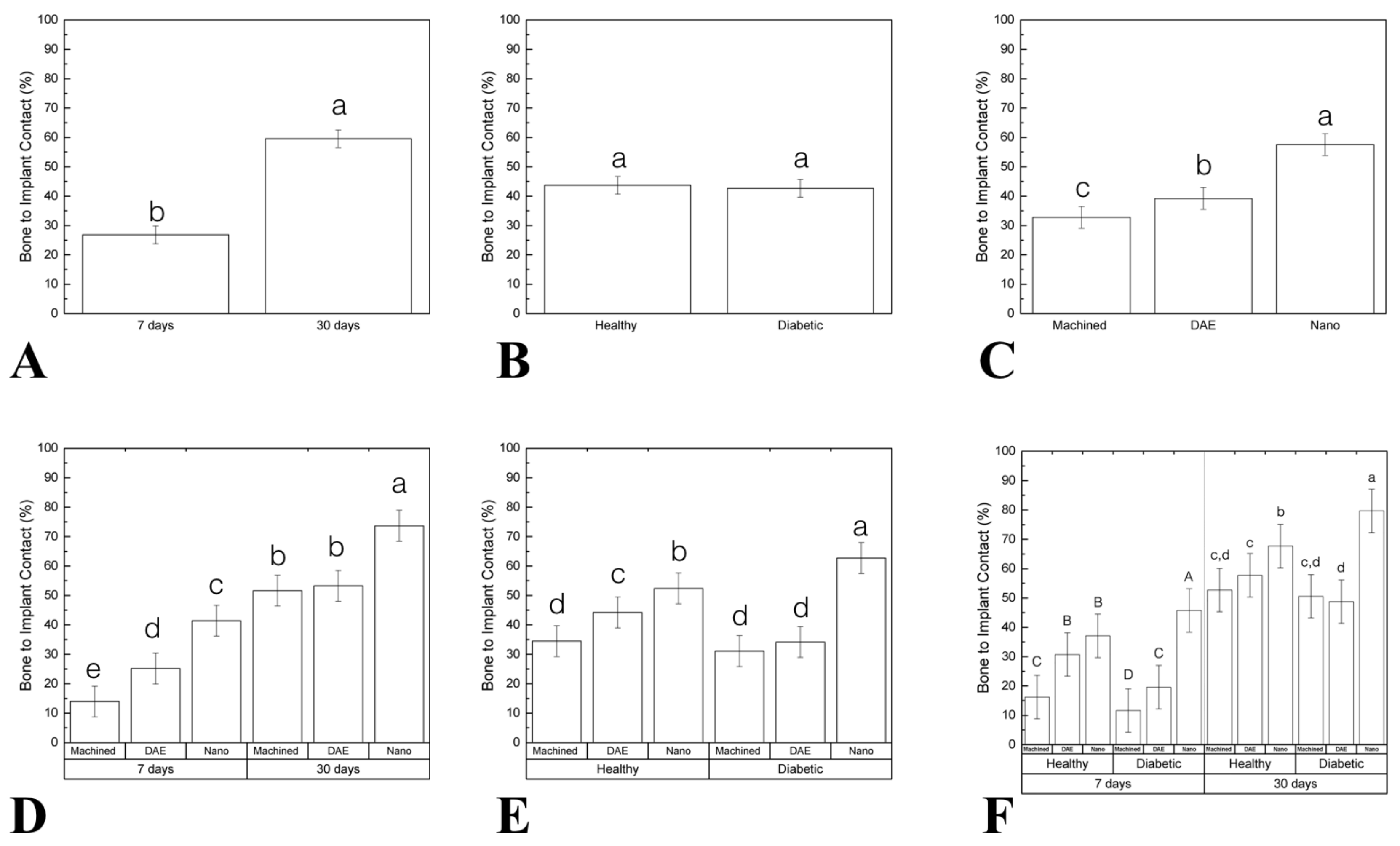
3.1.1. Bone to Implant Contact (%BIC)
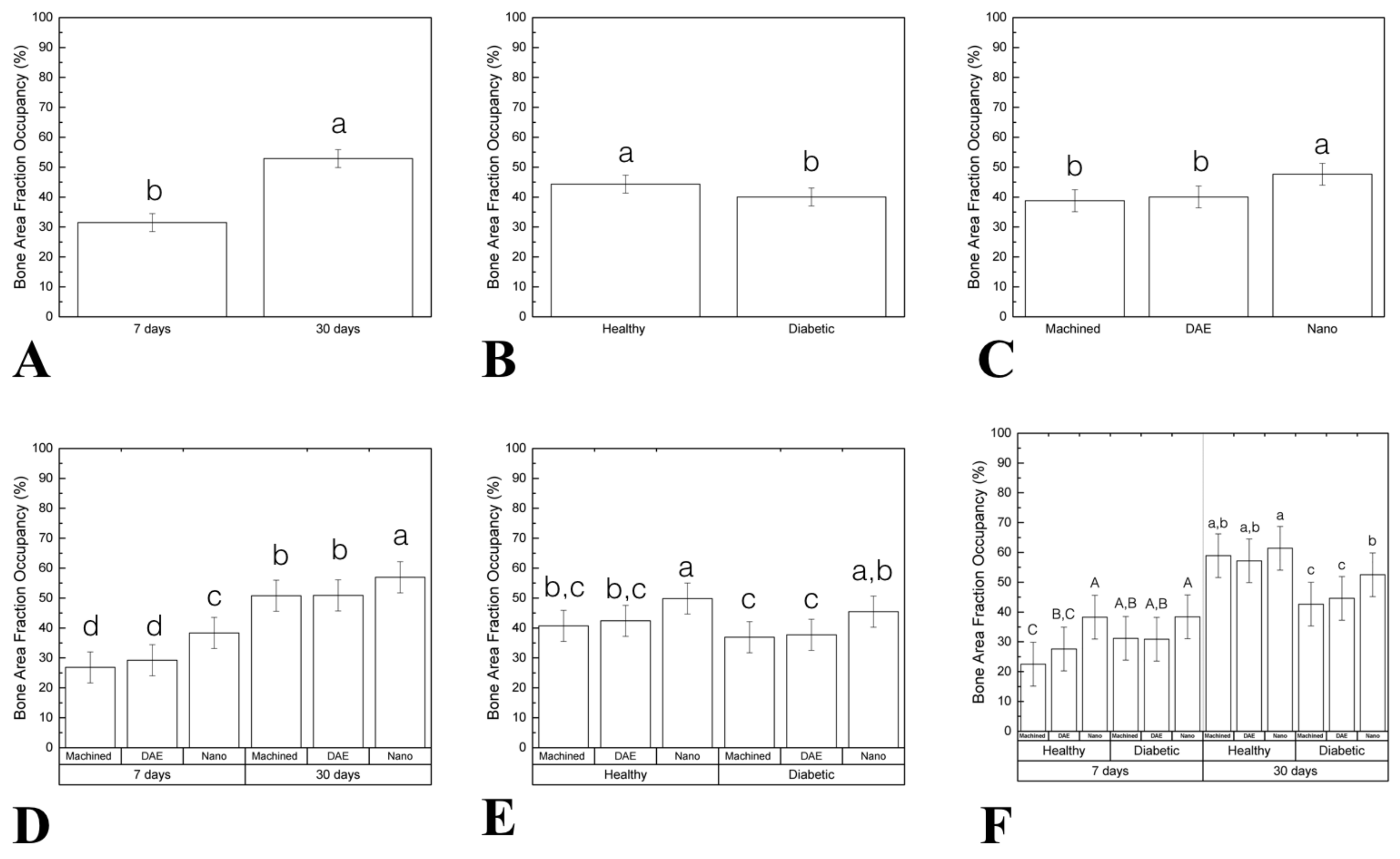
3.1.2. Bone Area Fraction Occupancy (%BAFO)
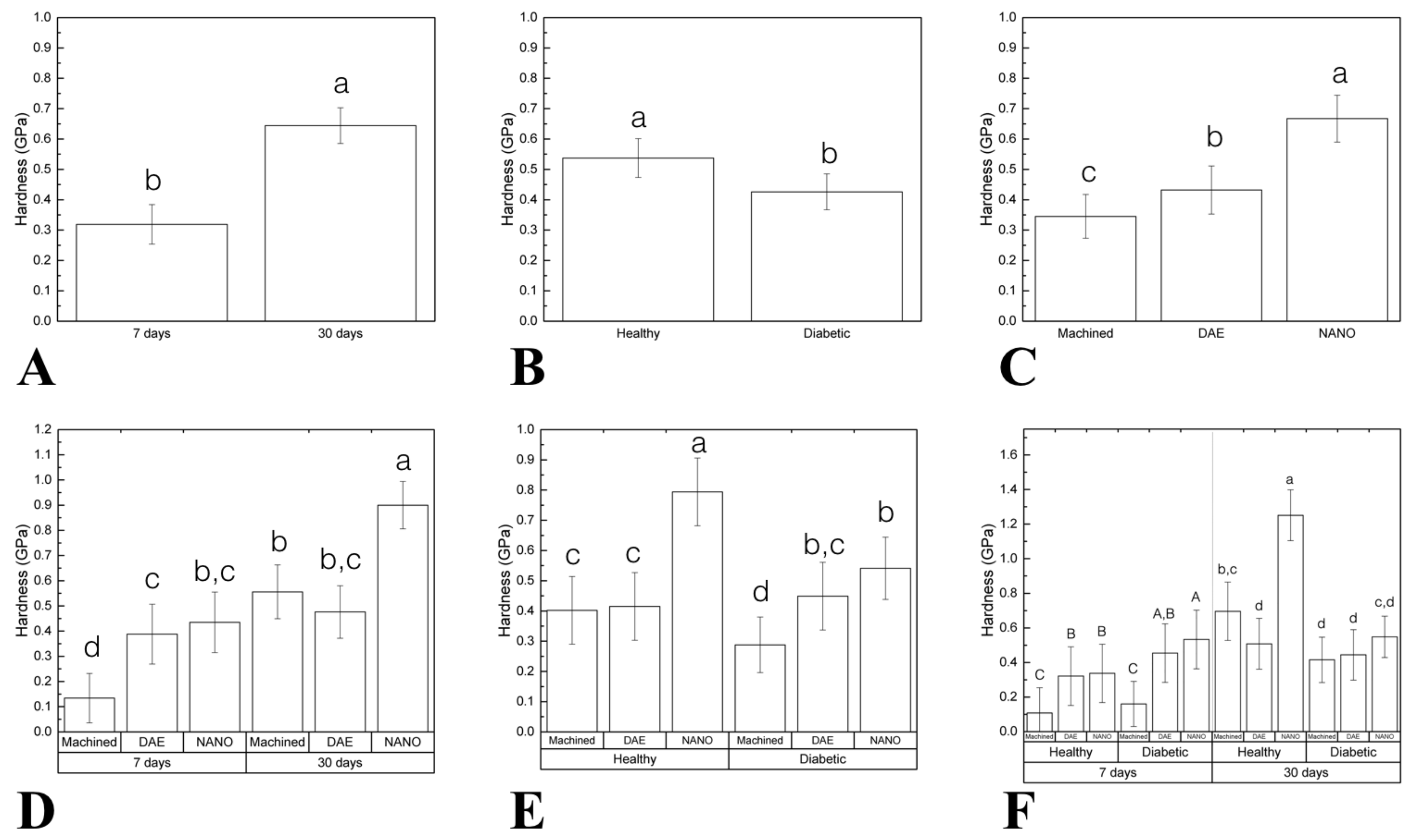
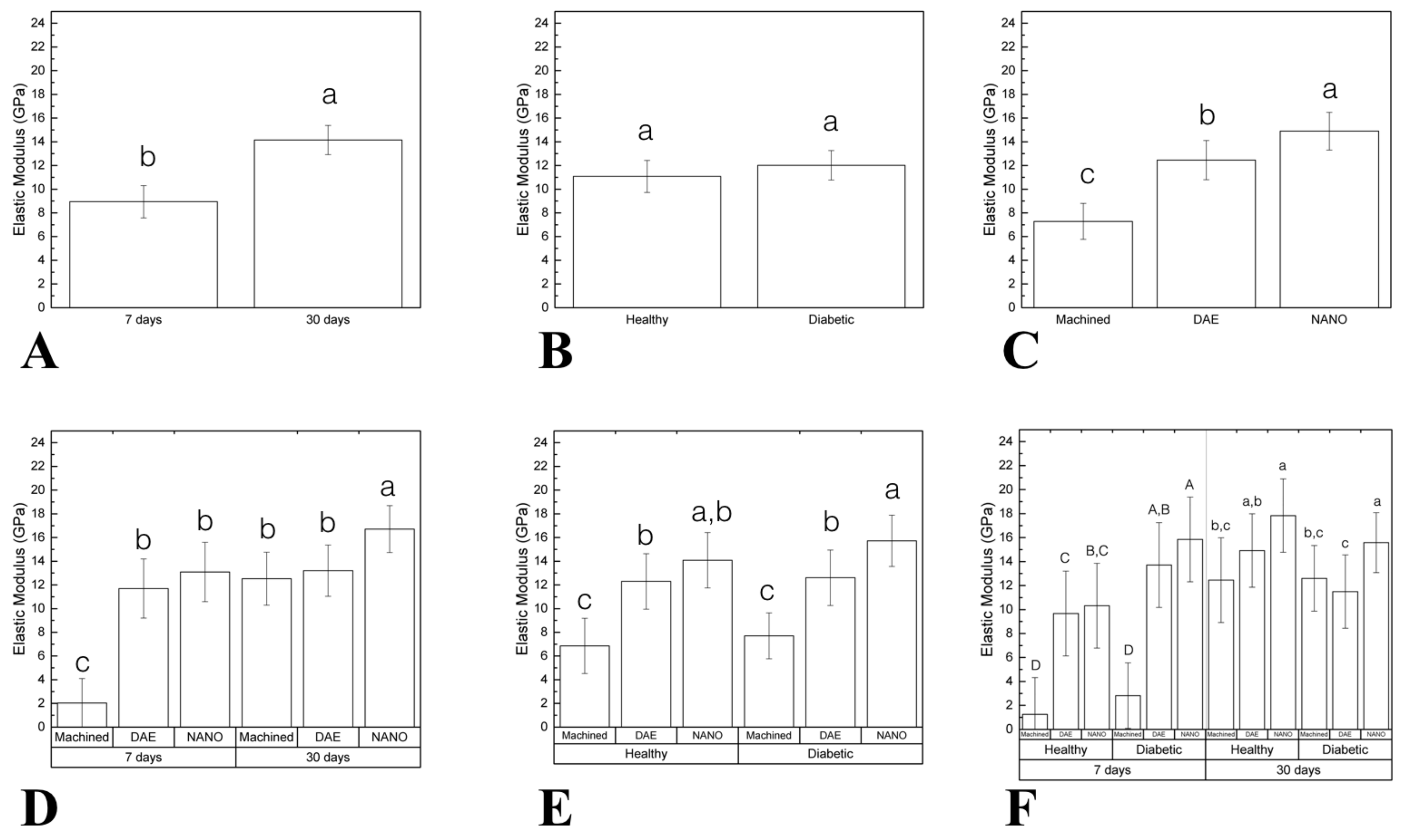
3.2. Nanomechanical Analysis
3.2.1. Elastic Modulus (EM)
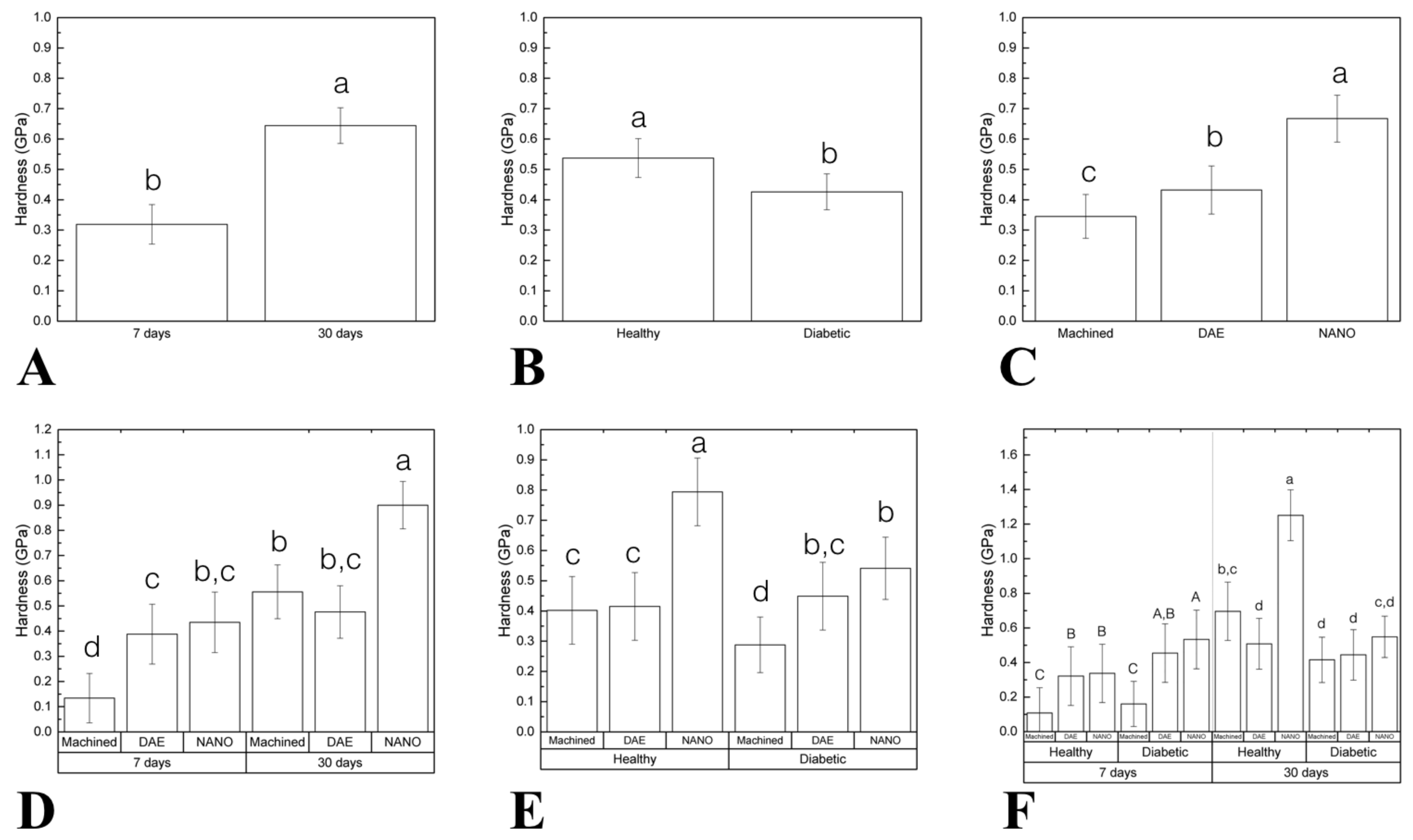
3.2.2. Hardness (H)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brånemark, P.-I.; Breine, U.; Adell, R.; Hansson, B.O.; Lindström, J.; Ohlsson, Å. Intra-osseous anchorage of dental prostheses: I. Experimental studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef]
- Geckili, O.; Bilhan, H.; Geckili, E.; Cilingir, A.; Mumcu, E.; Bural, C. Evaluation of possible prognostic factors for the success, survival, and failure of dental implants. Implant. Dent. 2014, 23, 44–50. [Google Scholar] [CrossRef]
- Albrektsson, T.; Branemark, P.I.; Hansson, H.A.; Lindstrom, J. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2005, 28, S37–S42. [Google Scholar] [CrossRef] [Green Version]
- King, H.; Aubert, R.E.; Herman, W.H. Global burden of diabetes, 1995–2025: Prevalence, numerical estimates, and projections. Diabetes Care 1998, 21, 1414–1431. [Google Scholar] [CrossRef]
- Oliver, R.C.; Tervonen, T. Periodontitis and tooth loss: Comparing diabetics with the general population. J. Am. Dent. Assoc. 1993, 124, 71–76. [Google Scholar] [CrossRef]
- Rothwell, B.R.; Richard, E.L. Diabetes mellitus: Medical and dental considerations. Spéc. Care Dent. 1984, 4, 58–65. [Google Scholar] [CrossRef]
- Frantzis, T.G.; Reeve, C.M.; Brown, A.L. The ultrastructure of capillary basement membranes in the attached gingiva of diabetic and nondiabetic patients with periodontal disease. J. Periodontol. 1971, 42, 406–411. [Google Scholar] [CrossRef]
- McMahon, M.M.; Bistrian, B.R. Host defenses and susceptibility to infection in patients with diabetes mellitus. Infect. Dis. Clin. North Am. 1995, 9, 1–9. [Google Scholar]
- Michaeli, E.; Weinberg, I.; Nahlieli, O. Dental implants in the diabetic patient: Systemic and rehabilitative considerations. Quintessence Int. 2009, 40, 639–645. [Google Scholar]
- Oates, T.W.; Huynh-Ba, G.; Vargas, A.; Alexander, P.; Feine, J. A critical review of diabetes, glycemic control, and dental implant therapy. Clin. Oral Implant. Res. 2013, 24, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Santana, R.B.; Xu, L.; Chase, H.B.; Amar, S.; Graves, D.T.; Trackman, P.C. A role for advanced glycation end products in diminished bone healing in type 1 diabetes. Diabetes 2003, 52, 1502–1510. [Google Scholar] [CrossRef] [Green Version]
- Gooch, H.L.; Hale, J.E.; Fujioka, H.; Balian, G.; Hurwitz, S.R. Alterations of cartilage and collagen expression during fracture healing in experimental diabetes. Connect. Tissue Res. 2000, 41, 81–91. [Google Scholar] [CrossRef]
- He, H.; Liu, R.; Desta, T.; Leone, C.; Gerstenfeld, L.C.; Graves, D.T. Diabetes causes decreased osteoclastogenesis, reduced bone formation, and enhanced apoptosis of osteoblastic cells in bacteria stimulated bone loss. Endocrinology 2004, 145, 447–452. [Google Scholar] [CrossRef] [Green Version]
- Kayal, R.A.; Tsatsas, D.; Bauer, M.A.; Allen, B.; Al-Sebaei, M.O.; Kakar, S.; Leone, C.W.; Morgan, E.F.; Gerstenfeld, L.C.; Einhorn, T.A.; et al. Diminished bone formation during diabetic fracture healing is related to the premature resorption of cartilage associated with increased osteoclast activity. J. Bone Miner. Res. 2007, 22, 560–568. [Google Scholar] [CrossRef] [Green Version]
- Weiss, R.E.; Gorn, A.H.; Nimni, M.E. Abnormalities in the biosynthesis of cartilage and bone proteoglycans in experimental diabetes. Diabetes 1981, 30, 670–677. [Google Scholar] [CrossRef]
- Lu, H.; Kraut, D.; Gerstenfeld, L.C.; Graves, D.T. diabetes interferes with the bone formation by affecting the expression of transcription factors that regulate osteoblast differentiation. Endocrinology 2003, 144, 346–352. [Google Scholar] [CrossRef]
- Schlegel, K.A.; Prechtl, C.; Möst, T.; Seidl, C.; Lutz, R.; Von Wilmowsky, C. Osseointegration of SL Active implants in diabetic pigs. Clin. Oral Implant. Res. 2013, 24, 128–134. [Google Scholar] [CrossRef]
- Souza, A.T.P.; Bezerra, B.L.; Oliveira, F.S.; Freitas, G.P.; Trevisan, R.L.B.; Oliveira, P.T.; Rosa, A.L.; Beloti, M. Effect of bone morphogenetic protein 9 on osteoblast differentiation of cells grown on titanium with nanotopography. J. Cell. Biochem. 2018, 119, 8441–8449. [Google Scholar] [CrossRef]
- Junior, A.B.N.; De Souza, S.L.S.; De Barros, R.R.M.; Pereira, K.K.Y.; Iezzi, G.; Piattelli, A. Influence of implant surfaces on osseointegration. Braz. Dent. J. 2010, 21, 471–481. [Google Scholar] [CrossRef]
- Le Guéhennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Schulz, M.C.; Korn, P.; Stadlinger, B.; Range, U.; Möller, S.; Becher, J.; Schnabelrauch, M.; Mai, R.; Scharnweber, D.; Eckelt, U.; et al. Coating with artificial matrices from collagen and sulfated hyaluronan influences the osseointegration of dental implants. J. Mater. Sci. Mater. Med. 2013, 25, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Jimbo, R.; Coelho, P.; Bryington, M.; Baldassarri, M.; Tovar, N.; Currie, F.; Hayashi, M.; Janal, M.; Andersson, M.; Ono, D.; et al. Nano hydroxyapatite-coated implants improve bone nanomechanical properties. J. Dent. Res. 2012, 91, 1172–1177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, P.G.; Takayama, T.; Yoo, D.; Jimbo, R.; Karunagaran, S.; Tovar, N.; Janal, M.N.; Yamano, S. Nanometer-scale features on micrometer-scale surface texturing: A bone histological, gene expression, and nanomechanical study. Bone 2014, 65, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Giglio, M.J.; Giannunzio, G.; Olmedo, D.G.; Guglielmotti, M.B. Histomorphometric study of bone healing around laminar implants in experimental diabetes. Implant. Dent. 2000, 9, 143–149. [Google Scholar] [CrossRef]
- McCracken, M.; Lemons, J.E.; Rahemtulla, F.; Prince, C.W.; Feldman, D. Bone response to titanium alloy implants placed in diabetic rats. Int. J. Oral Maxillofac. Implant. 2000, 15, 345–354. [Google Scholar]
- Ajami, E.; Mahno, E.; Mendes, V.; Bell, S.; Moineddin, R.; Davies, J.E. Bone healing and the effect of implant surface topography on osteoconduction in hyperglycemia. Acta Biomater. 2014, 10, 394–405. [Google Scholar] [CrossRef]
- Margonar, R.; Sakakura, C.E.; Holzhausen, M.; Pepato, M.T.; Alba, J.R.C.; Marcantonio, J.E. The influence of diabetes mellitus and insulin therapy on biomechanical retention around dental implants: A study in rabbits. Implant. Dent. 2003, 12, 333–339. [Google Scholar] [CrossRef]
- Kjellin, P.; Andersson, M. Synthetic Nano-Sized Crystalline Calcium Phosphate and Method of Production. US Patent 8206813, 26 June 2012. [Google Scholar]
- Coelho, P.G.; Marin, C.; Granato, R.; Giro, G.; Suzuki, M.; Bonfante, E.A. Biomechanical and histologic evaluation of non-washed resorbable blasting media and alumina-blasted/acid-etched surfaces. Clin. Oral Implant. Res. 2011, 23, 132–135. [Google Scholar] [CrossRef]
- Jinno, Y.; Jimbo, R.; Tovar, N.; Teixeira, H.S.; Witek, L.; Coelho, P.G. In vivo evaluation of dual acid-etched and grit-blasted/acid-etched implants with identical macrogeometry in high-density bone. Implant. Dent. 2017, 26, 815–819. [Google Scholar] [CrossRef]
- Gil, L.; Sarendranath, A.; Neiva, R.; Marão, H.; Tovar, N.; Bonfante, E.A.; Janal, M.; Castellano, A.; Coelho, P. Bone healing around dental implants: Simplified vs conventional drilling protocols at speed of 400 rpm. Int. J. Oral Maxillofac. Implant. 2017, 32, 329–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldassarri, M.; Bonfante, E.; Suzuki, M.; Marin, C.; Granato, R.; Tovar, N.; Coelho, P.G. Mechanical properties of human bone surrounding plateau root form implants retrieved after 0.3–24 years of function. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100, 2015–2021. [Google Scholar] [CrossRef]
- Doerner, M.F.; Nix, W.D. A method for interpreting the data from depth-sensing indentation instruments. J. Mater. Res. 1986, 1, 601–609. [Google Scholar] [CrossRef]
- Butz, F.; Aita, H.; Wang, C.; Ogawa, T. Harder and stiffer bone Osseo integrated to roughened titanium. J. Dent. Res. 2006, 85, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Hoffler, C.E.; Guo, X.E.; Zysset, P.K.; Goldstein, S.A. An application of nanoindentation technique to measure bone tissue lamellae properties. J. Biomech. Eng. 2005, 127, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Hoffler, C.; Moore, K.; Kozloff, K.; Zysset, P.; Brown, M.; Goldstein, S.A. Heterogeneity of bone lamellar-level elastic moduli. Bone 2000, 26, 603–609. [Google Scholar] [CrossRef]
- Lee, K.-L.; Sobieraj, M.; Baldassarri, M.; Gupta, N.; Pinisetty, D.; Janal, M.N.; Tovar, N.; Coelho, P.G. The effects of loading conditions and specimen environment on the nanomechanical response of canine cortical bone. Mater. Sci. Eng. C 2013, 33, 4582–4586. [Google Scholar] [CrossRef]
- Anchieta, R.B.; Baldassarri, M.; Guastaldi, F.; Tovar, N.; Janal, M.N.; Gottlow, J.; Dard, M.; Jimbo, R.; Coelho, P. Mechanical property assessment of bone healing around a titanium-zirconium alloy dental implant. Clin. Implant. Dent. Relat. Res. 2014, 16, 913–919. [Google Scholar] [CrossRef]
- Jimbo, R.; Anchieta, R.; Baldassarri, M.; Granato, R.; Marin, C.; Teixeira, H.S.; Tovar, N.; Vandeweghe, S.; Janal, M.N.; Coelho, P.G. Histomorphometry and bone mechanical property evolution around different implant systems at early healing stages: An experimental study in dogs. Implant Dent. 2013, 22, 596–603. [Google Scholar] [CrossRef] [Green Version]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 2-Review focusing on clinical knowledge of different surfaces. Int. J. Prosthodont. 2004, 17, 544–564. [Google Scholar]
- Henry, P.J.; Laney, W.R.; Jemt, T.; Harris, D.; Krogh, P.H.; Polizzi, G.; Zarb, G.A.; Herrmann, I. Osseointegrated implants for single-tooth replacement: A prospective 5-year multicenter study. Int. J. Oral Maxillofac. Implant. 1996, 11, 450–455. [Google Scholar]
- Freitas, G.P.; Lopes, H.B.; Martins-Neto, E.C.; De Oliveira, P.T.; Beloti, M.M.; Rosa, A.L.; De Almeida, A.L. Effect of surface nanotopography on bone response to titanium implant. J. Oral Implant. 2016, 42, 240–247. [Google Scholar] [CrossRef] [PubMed]
- King, S.; Klineberg, I.; Levinger, I.; Brennan-Speranza, T.C. The effect of hyperglycaemia on osseointegration: A review of animal models of diabetes mellitus and titanium implant placement. Arch. Osteoporos. 2016, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Ramenzoni, L.L.; Bösch, A.; Proksch, S.; Attin, T.; Dds, P.R.S. Effect of high glucose levels and lipopolysaccharides-induced inflammation on osteoblast mineralization over sandblasted/acid-etched titanium surface. Clin. Implant. Dent. Relat. Res. 2020, 22, 213–219. [Google Scholar] [CrossRef]
- Yamawaki, I.; Taguchi, Y.; Komasa, S.; Tanaka, A.; Umeda, M. Effects of glucose concentration on osteogenic differentiation of type II diabetes mellitus rat bone marrow-derived mesenchymal stromal cells on a nano-scale modified titanium. J. Periodontal Res. 2017, 52, 761–771. [Google Scholar] [CrossRef]
- Burgos, P.M.; Rasmusson, L.; Meirelles, L.; Sennerby, L. Early bone tissue responses to turned and oxidized implants in the rabbit tibia. Clin. Implant. Dent. Relat. Res. 2008, 10, 181–190. [Google Scholar] [CrossRef]
- Jiang, H.; Ma, X.; Zhou, W.; Dong, K.; Rausch-Fan, X.; Liu, S.; Li, S. The effects of hierarchical micro/nano-structured titanium surface on osteoblast proliferation and differentiation under diabetic conditions. Implant. Dent. 2017, 26, 263–269. [Google Scholar] [CrossRef]
- Coelho, P.G.; Bonfante, E.A.; Pessoa, R.S.; Marin, C.; Granato, R.; Giro, G.; Witek, L.; Suzuki, M. Characterization of five different implant surfaces and their effect on osseointegration: A study in dogs. J. Periodontol. 2011, 82, 742–750. [Google Scholar] [CrossRef]
- Coelho, P.G.; Jimbo, R.; Tovar, N.; Bonfante, E.A. Osseointegration: Hierarchical designing encompassing the macrometer, micrometer, and nanometer length scales. Dent. Mater. 2015, 31, 37–52. [Google Scholar] [CrossRef]
- Hayashi, M.; Jimbo, R.; Lindh, L.; Sotres, J.; Sawase, T.; Mustafa, K.; Andersson, M.; Wennerberg, A. In vitro characterization and osteoblast responses to nanostructured photocatalytic TiO2 coated surfaces. Acta Biomater. 2012, 8, 2411–2416. [Google Scholar] [CrossRef]
- Tomsia, A.P.; Lee, J.S.; Wegst, U.G.; Saiz, E. Nanotechnology for dental implants. Int. J. Oral Maxillofac. Implant. 2013, 28, e535–e546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webster, T.J.; Ahn, E.S. Nanostructured biomaterials for tissue engineering bone. Process. Integr. Biochem. Eng. 2007, 103, 275–308. [Google Scholar] [CrossRef]
- Rupp, F.; Liang, L.; Geis-Gerstorfer, J.; Scheideler, L.; Huettig, F. Surface characteristics of dental implants: A review. Dent. Mater. 2018, 34, 40–57. [Google Scholar] [CrossRef] [PubMed]
- Alexandergehrke, S.; Martínez, C.P.-A.; Piattelli, A.; Shibli, J.A.; Markovic, A.; Guirado, J.L.C. The influence of three different apical implant designs at stability and osseointegration process: Experimental study in rabbits. Clin. Oral Implant. Res. 2016, 28, 355–361. [Google Scholar] [CrossRef]
- Ajami, E.; Bell, S.; Liddell, R.S.; Davies, J.E. Early bone anchorage to micro-and nano-topographically complex implant surfaces in hyperglycemia. Acta Biomater. 2016, 39, 169–179. [Google Scholar] [CrossRef]
- Coelho, P.G.; Teixeira, H.S.; Marin, C.; Witek, L.; Tovar, N.; Janal, M.N.; Jimbo, R. The in vivo effect of P-15 coating on early osseointegration. J. Biomed. Mater. Res. Part. B Appl. Biomater. 2013, 102, 430–440. [Google Scholar] [CrossRef]
- Coelho, P.G.; Freire, J.N.; Granato, R.; Marin, C.; Bonfante, E.A.; Gil, J.N.; Chuang, S.-K.; Suzuki, M. Bone mineral apposition rates at early implantation times around differently prepared titanium surfaces: A study in beagle dogs. Int. J. Oral Maxillofac. Implant. 2011, 26, 63–69. [Google Scholar]
- Van De Weghe, S.; Coelho, P.G.; Vanhove, C.; Wennerberg, A.; Jimbo, R. Utilizing micro-computed tomography to evaluate bone structure surrounding dental implants: A comparison with histomorphometry. J. Biomed. Mater. Res. Part. B Appl. Biomater. 2013, 101, 1259–1266. [Google Scholar] [CrossRef] [Green Version]
- Beck, G.R.; Sullivan, E.C.; Moran, E.; Zerler, B. Relationship between alkaline phosphatase levels, osteopontin expression, and mineralization in differentiating MC3T3-E1 osteoblasts. J. Cell. Biochem. 1998, 68, 269–280. [Google Scholar] [CrossRef]
- Stein, G.S.; Lian, J.B.; Stein, J.L.; Van Wijnen, A.J.; Montecino, M. Transcriptional control of osteoblast growth and differentiation. Physiol. Rev. 1996, 76, 593–629. [Google Scholar] [CrossRef]
- De Oliveira, P.; De Melo Soares, M.S.; Silveira, E.S.A.M.M.; Taba, M., Jr.; Palioto, D.B.; Messora, M.R.; Ghiraldini, B.; Nunes, F.A.S.; De Souza, S.L.S. Influence of nano-hydroxyapatite coating implants on gene expression of osteogenic markers and micro-CT parameters. An in vivo study in diabetic rats. J. Biomed. Mater. Res. A 2020. [Google Scholar]
- Scarano, A.; Lorusso, F.; Orsini, T.; Morra, M.; Iviglia, G.; Valbonetti, L. Biomimetic surfaces coated with covalently immobilized collagen type i: An x-ray photoelectron spectroscopy, atomic force microscopy, micro-CT and histomorphometrical study in rabbits. Int. J. Mol. Sci. 2019, 20, 724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yıldırım, T.T.; Dündar, S.; Bozoğlan, A.; Karaman, T.; Kahraman, O.E.; Özcan, E.C. The effects of metformin on the bone filling ration around of TiAl6Va4 implants in non diabetic rats. J. Oral Biol. Craniofacial Res. 2020, 10, 474–477. [Google Scholar] [CrossRef] [PubMed]
- Guimaraes, R.P.; De Oliveira, P.A.D.; Oliveira, A.M.S.D. Effects of induced diabetes and the administration of aminoguanidine in the biomechanical retention of implants: A study in rats. J. Periodontal Res. 2011, 46, 691–696. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, P.G.F.P.; Coelho, P.G.; Bergamo, E.T.P.; Witek, L.; Borges, C.A.; Bezerra, F.B.; Novaes, A.B., Jr.; Souza, S.L.S. Histological and Nanomechanical Properties of a New Nanometric Hydroxiapatite Implant Surface. An In Vivo Study in Diabetic Rats. Materials 2020, 13, 5693. https://doi.org/10.3390/ma13245693
Oliveira PGFP, Coelho PG, Bergamo ETP, Witek L, Borges CA, Bezerra FB, Novaes AB Jr., Souza SLS. Histological and Nanomechanical Properties of a New Nanometric Hydroxiapatite Implant Surface. An In Vivo Study in Diabetic Rats. Materials. 2020; 13(24):5693. https://doi.org/10.3390/ma13245693
Chicago/Turabian StyleOliveira, Paula G. F. P., Paulo G. Coelho, Edmara T. P. Bergamo, Lukasz Witek, Cristine A. Borges, Fábio B. Bezerra, Arthur B. Novaes, Jr., and Sergio L. S. Souza. 2020. "Histological and Nanomechanical Properties of a New Nanometric Hydroxiapatite Implant Surface. An In Vivo Study in Diabetic Rats" Materials 13, no. 24: 5693. https://doi.org/10.3390/ma13245693
APA StyleOliveira, P. G. F. P., Coelho, P. G., Bergamo, E. T. P., Witek, L., Borges, C. A., Bezerra, F. B., Novaes, A. B., Jr., & Souza, S. L. S. (2020). Histological and Nanomechanical Properties of a New Nanometric Hydroxiapatite Implant Surface. An In Vivo Study in Diabetic Rats. Materials, 13(24), 5693. https://doi.org/10.3390/ma13245693