An Alternative Route for Entrapped Inferior Orbital Nerve in Orbital Floor Fracture
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
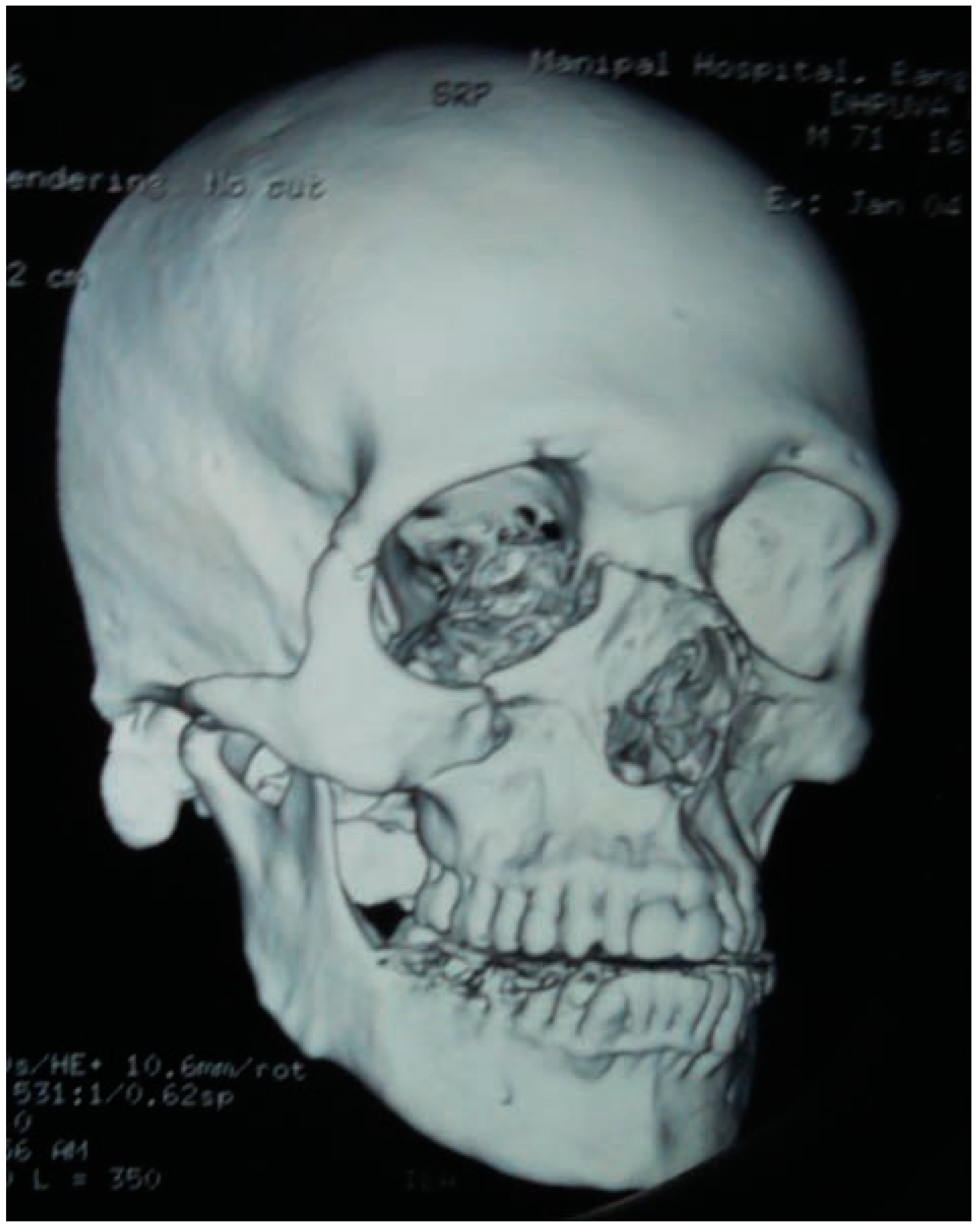
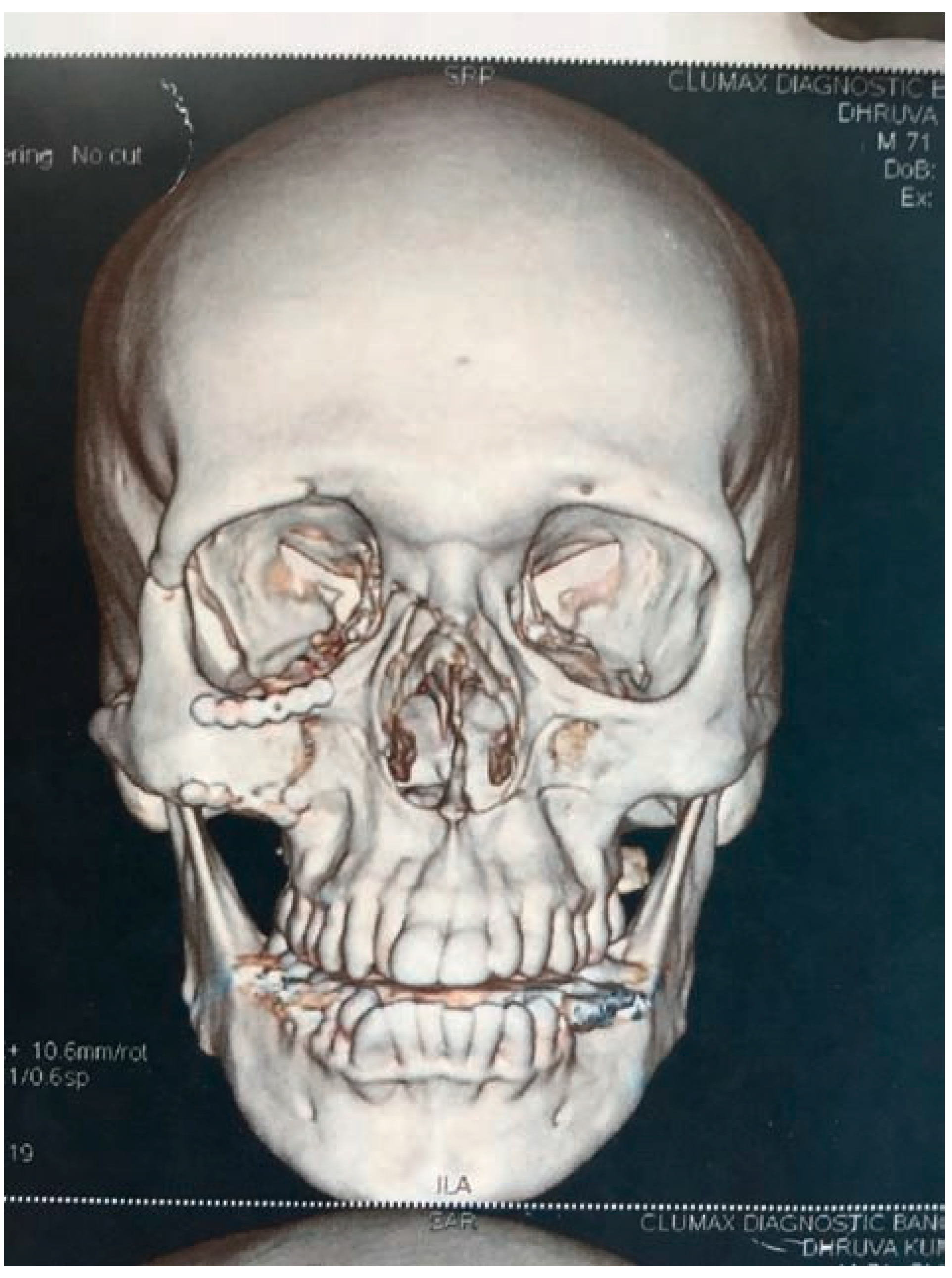
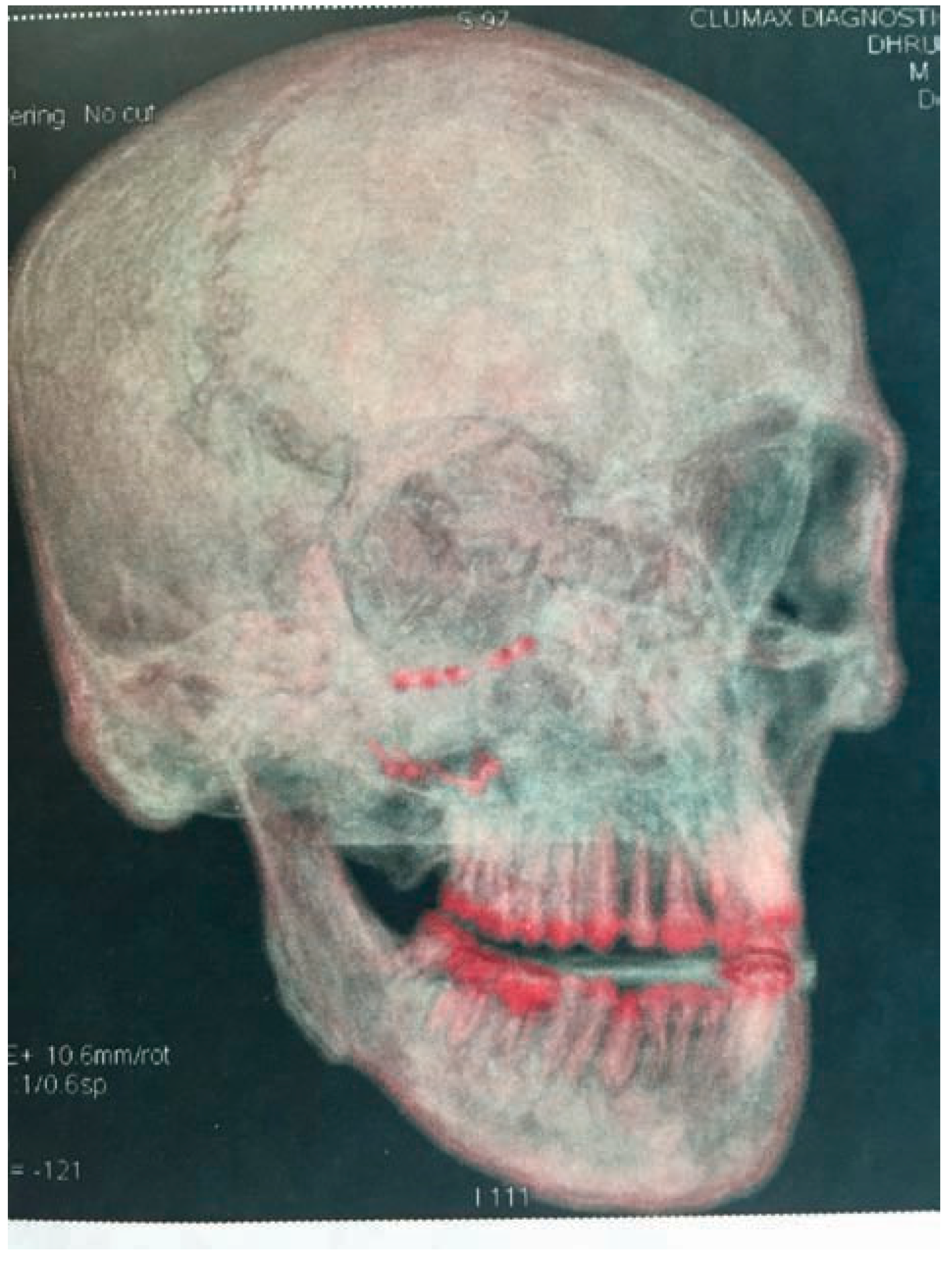
:Case History
- Both nasal bones
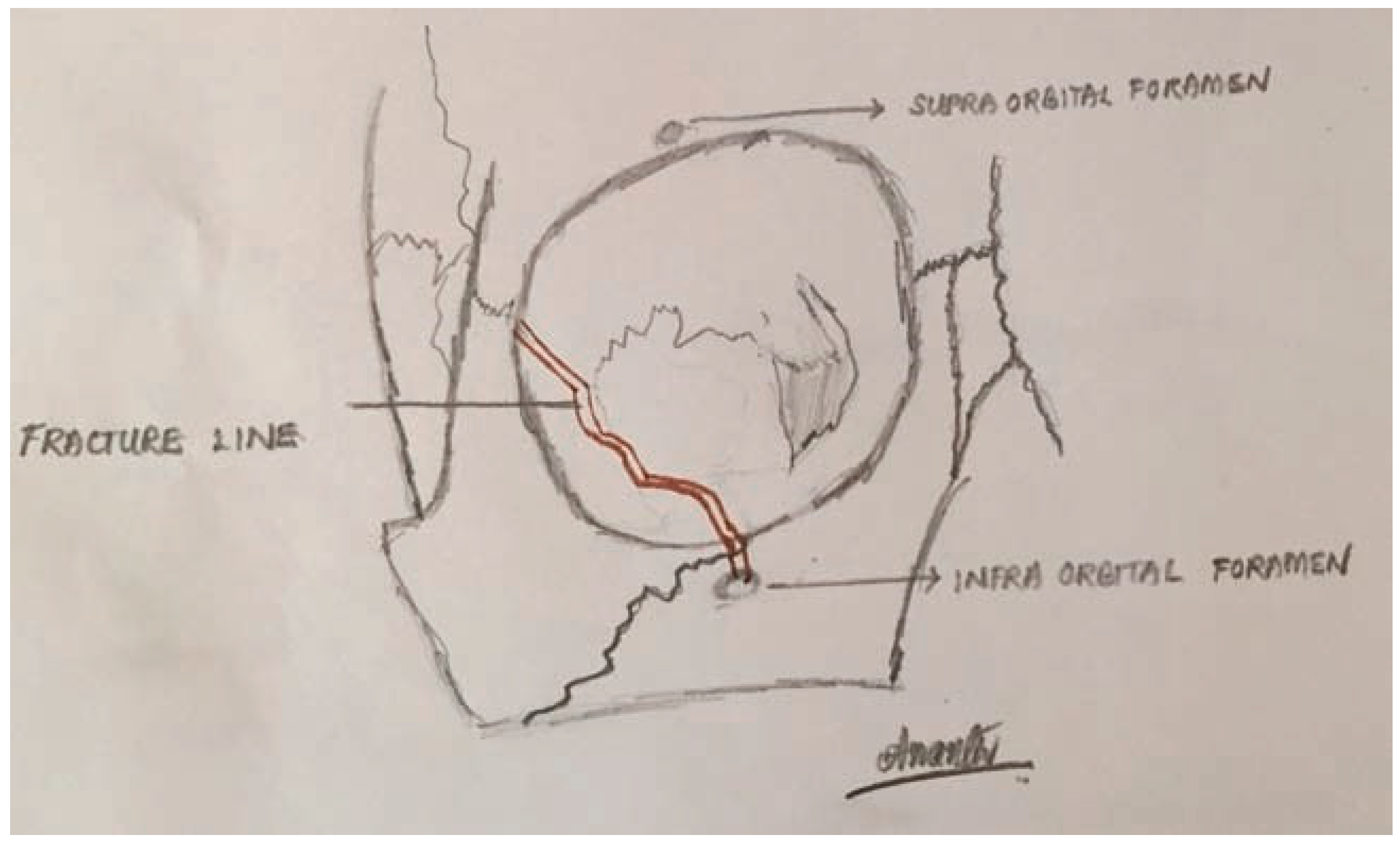
- Anterior, medial, and lateral wall of the right maxillary sinus with displaced fragments with hemosinus, fracture line passing through the right infraorbital foramen
- Lateral wall of right orbit
- Right zygomatic process



Discussion


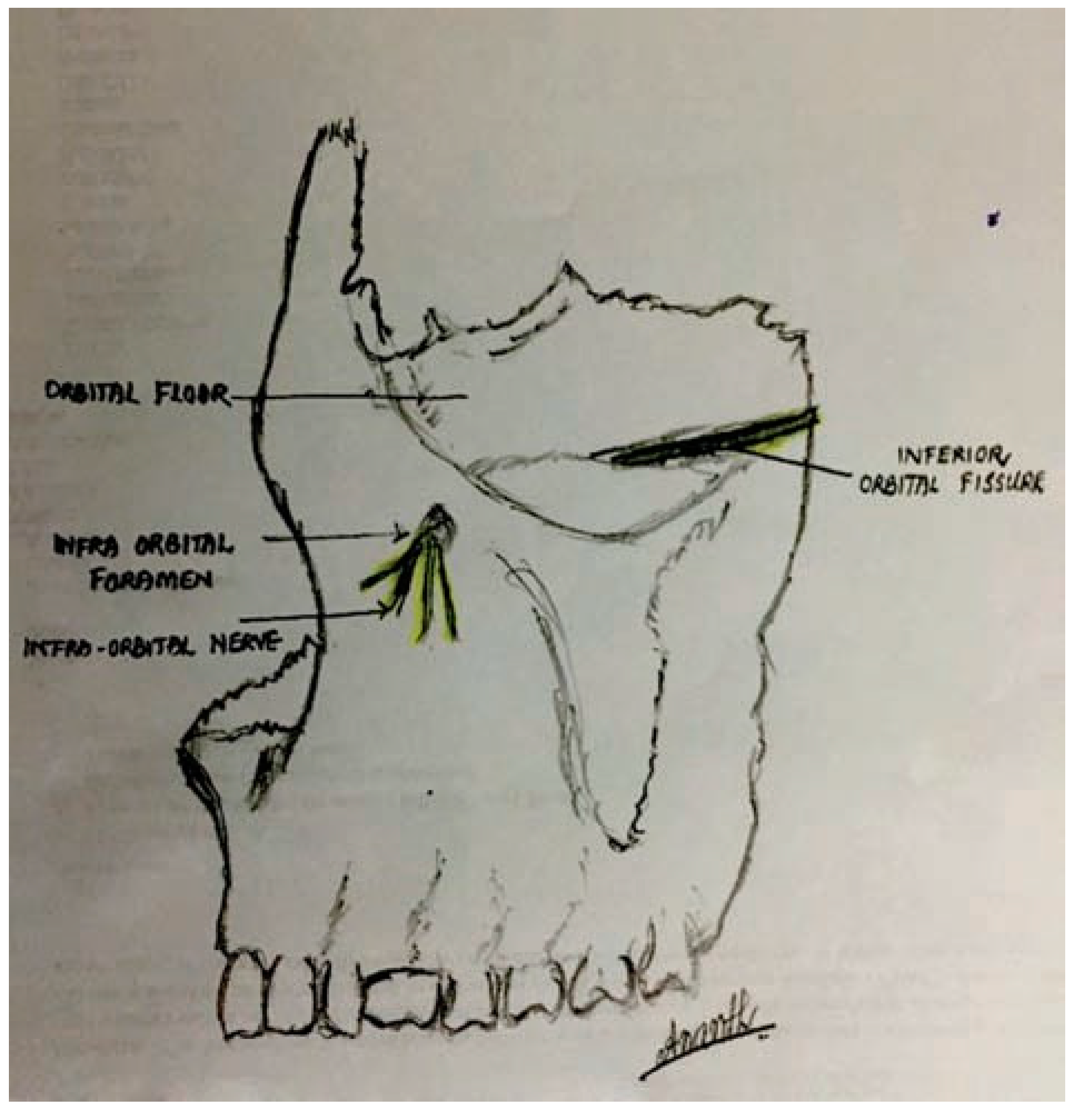
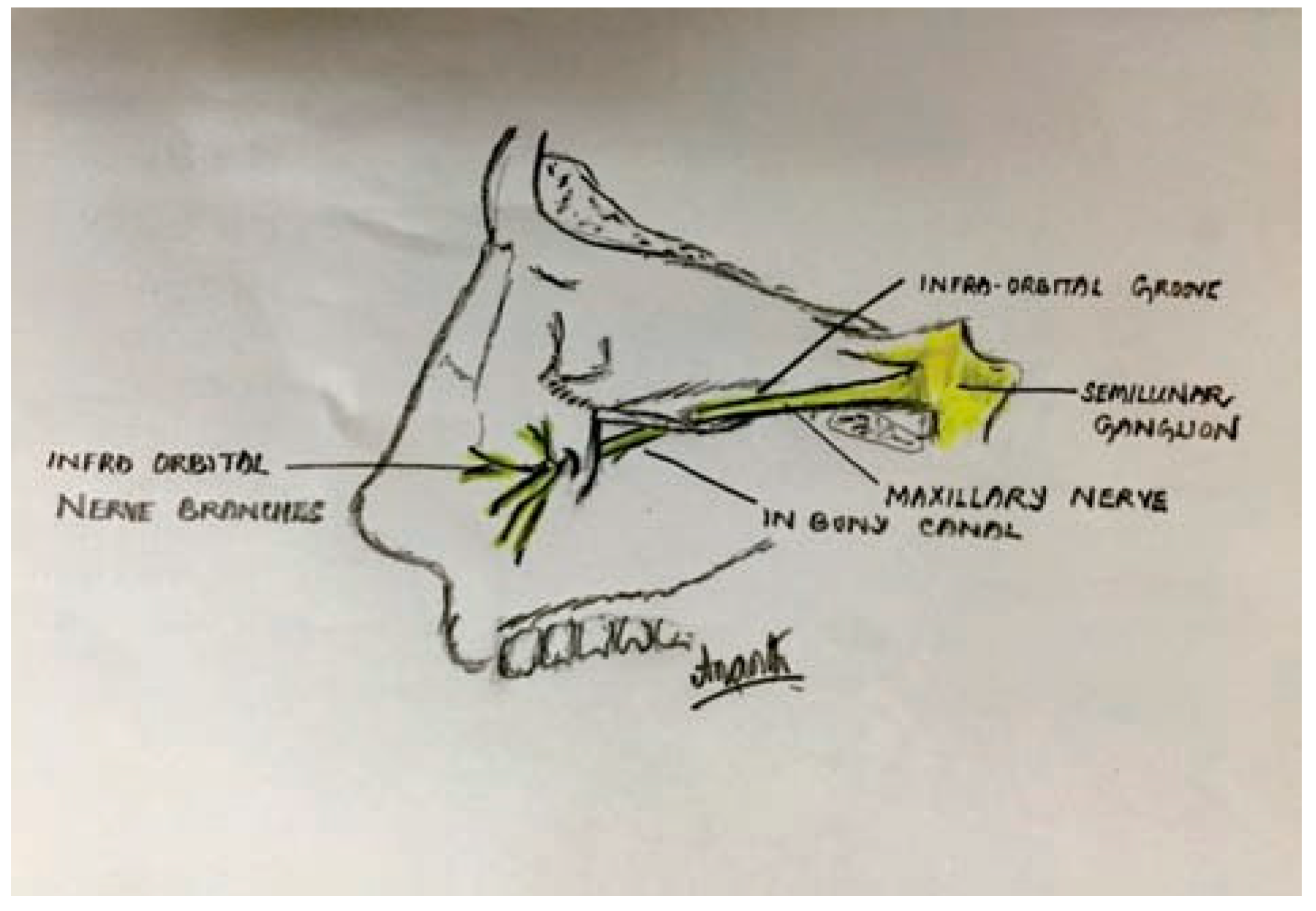
Infraorbital Nerve Anatomy


- A bifurcated nerve running in two separate osseous canals and emerging out of two separate infraorbital foramina [15].
- The nerve may run in a canal (complete roof present) or canal plus groove.
- The foramen may be oval, round, or semilunar.
- There may be accessory or supernumerary infraorbital foramina. Kazkayasi et al. found them to be doubled in 5%, tripled in 5%, and more than three times in 0.3% [16].


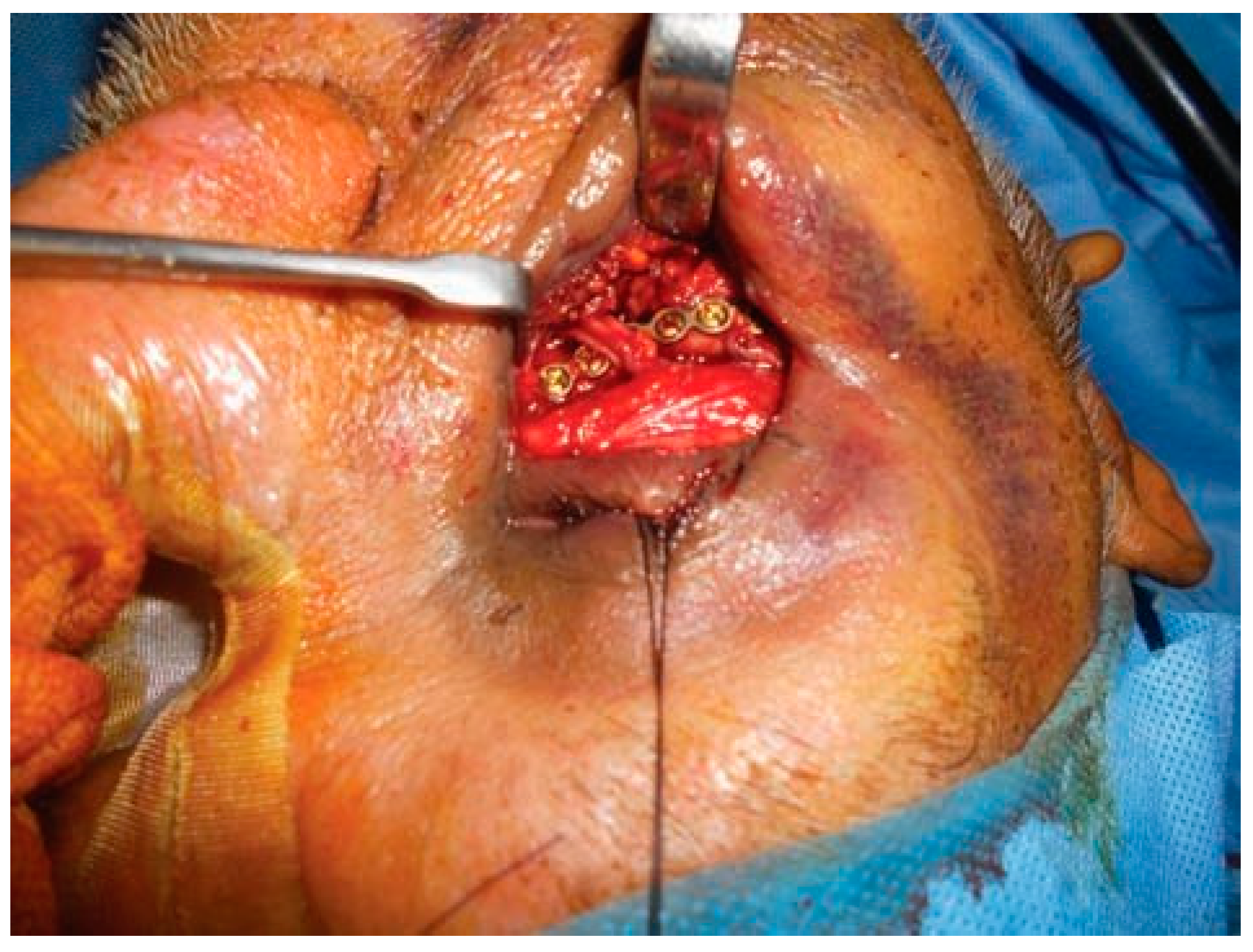
Surgical Management of Orbital Floor Fractures
- Enophthalmos of more than 2 mm at any time during first 6 weeks
- Diplopia persisting for more than 2 weeks
- Large orbital floor defect of 1 cm2 and above
- Significant hypoglobus




Conclusion
References
- Trindade, P.A.K.; Vieira, E.H.; Gabrielli, M.A.C.; Gabrielli, M.F.R.; Filho, V.A.P. Treatment and complications of orbito-zygomatico fractures. Int J Odontostomat 2012, 6, 255–262. [Google Scholar] [CrossRef]
- Jungell, P.; Lindqvist, C. Paraesthesia of the infraorbital nerve following fracture of the zygomatic complex. Int J Oral Maxillofac Surg 1987, 16, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Kersey, J.P.; Beigi, B. Infraorbital nerve decompression for infraorbital neuralgia following orbital fracture. British Oculoplastic Surg Soc 1999, 10, 24–27. [Google Scholar]
- Fogaça, W.C.; Fereirra, M.C.; Dellon, A.L. Infraorbital nerve injury associated with zygoma fractures: Documentation with neurosensory testing. Plast Reconstr Surg 2004, 113, 834–838. [Google Scholar] [CrossRef] [PubMed]
- Peltomaa, J.; Rihkanen, H. Infraorbital nerve recovery after minimally dislocated facial fractures. Eur Arch Otorhinolaryngol 2000, 257, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Vriens, J.P.; Moos, K.F. Morbidity of the infraorbital nerve following orbitozygomatic complex fractures. J Craniomaxillofac Surg 1995, 23, 363–368. [Google Scholar] [CrossRef]
- Bailey, K.; Ng, J.D.; Hwang, P.H.; Saulny, S.M.; Holck, D.E.; Rubin, P.A. Infraorbital nerve surgical decompression for chronic infraorbital nerve hyperesthesia. Ophthal Plast Reconstr Surg 2007, 23, 49–51. [Google Scholar] [CrossRef] [PubMed]
- Sakavicius, D.; Juodzbalys, G.; Kubilius, R.; Sabalys, G.P. Investigation of infraorbital nerve injury following zygomaticomaxillary complex fractures. J Oral Rehabil 2008, 35, 903–916. [Google Scholar] [CrossRef] [PubMed]
- Taicher, S.; Ardekian, L.; Samet, N.; Shoshani, Y.; Kaffe, I. Recovery of the infraorbital nerve after zygomatic complex fractures: A preliminary study of different treatment methods. Int J Oral Maxillofac Surg 1993, 22, 339–341. [Google Scholar] [CrossRef] [PubMed]
- Schultze-Mosgau, S.; Erbe, M.; Rudolph, D.; Ott, R.; Neukam, F.W. Prospective study on post-traumatic and postoperative sensory disturbances of the inferior alveolar nerve and infraorbital nerve in mandibular and midfacial fractures. J Craniomaxillofac Surg 1999, 27, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Godhi, S.; Lall, A.B.; Ram, C.S. Evaluation of neurosensory changes in the infraorbital nerve following zygomatic fractures. J Maxillofac Oral Surg 2012, 11, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Lone, P.A.; Singh, R.K.; Pal, U.S. Treatment of traumatic infra orbital nerve paresthesia. Natl J Maxillofac Surg 2012, 3, 218–219. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.S.; Kwak, H.H.; Song, W.C.; et al. Branching patterns of the infraorbital nerve and topography within the infraorbital space. J Craniofac Surg 2006, 17, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Lokanayaki, V. Anatomic variations of infraorbital foramen. CIB Tech J Surgery 2013, 2, 30–36. [Google Scholar]
- Tubbas, R.S.; Loukas, M.; May, W.R.; Cohen-Gadol, A.A. A variation of the infraorbital nerve: Its potential clinical consequence especially the treatment of trigeminal neuralgia: Case report. Neurosugery 2010, 67, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Kazkayasi, M.; Ergin, A.; Ersoy, M.; Tekdemir, I.; Elhan, A. Microscopic anatomy of the infraorbital canal, nerve, and foramen. Otolaryngol Head Neck Surg 2003, 129, 692–697. [Google Scholar] [CrossRef] [PubMed]
- Kotrashetti, S.M.; Kale, T.P.; Bhandage, S.; Kumar, A. Infraorbital nerve transpositioning into orbital floor: A modified technique to minimize nerve injury following zygomaticomaxillary complex fractures. J Korean Assoc Oral Maxillofac Surg 2015, 41, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Lee, J.H. Orbital floor restoration with traction of the infraorbital nerve using a vessel loop in posterior orbital floor fractures. J Craniomaxillofac Surg 2014, 42, 2069–2075. [Google Scholar] [CrossRef] [PubMed]
- Mok, D.; Lessard, L.; Cordoba, C.; Harris, P.G.; Nikolis, A. A review of materials currently used in orbital floor reconstruction. Can J Plast Surg 2004, 12, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Zheng, H.F.; Chen, X.H.; Shen, X.C.; Hao, J.C. A comparison of early and late reconstruction and repositioning of orbital blow-out fracture. Zhonghua Zheng Xing Wai Ke Za Zhi 2003, 19, 436–438. [Google Scholar] [PubMed]
© 2016 by the author. The Author(s) 2016.
Share and Cite
Rao, A.Y.N.; Jesudas, J. An Alternative Route for Entrapped Inferior Orbital Nerve in Orbital Floor Fracture. Craniomaxillofac. Trauma Reconstr. 2017, 10, 230-238. https://doi.org/10.1055/s-0036-1592090
Rao AYN, Jesudas J. An Alternative Route for Entrapped Inferior Orbital Nerve in Orbital Floor Fracture. Craniomaxillofacial Trauma & Reconstruction. 2017; 10(3):230-238. https://doi.org/10.1055/s-0036-1592090
Chicago/Turabian StyleRao, Anantheswar Y. N., and Joyce Jesudas. 2017. "An Alternative Route for Entrapped Inferior Orbital Nerve in Orbital Floor Fracture" Craniomaxillofacial Trauma & Reconstruction 10, no. 3: 230-238. https://doi.org/10.1055/s-0036-1592090
APA StyleRao, A. Y. N., & Jesudas, J. (2017). An Alternative Route for Entrapped Inferior Orbital Nerve in Orbital Floor Fracture. Craniomaxillofacial Trauma & Reconstruction, 10(3), 230-238. https://doi.org/10.1055/s-0036-1592090