Effects of an Exercise Intervention on Gait Function in Young Survivors of Osteosarcoma with Megaendoprosthesis of the Lower Extremity—Results from the Pilot Randomized Controlled Trial proGAIT

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Population and Surgery
2.3. Intervention
2.4. Assessments
2.5. Data Analysis and Statistics
3. Results
3.1. Patient Characteristics
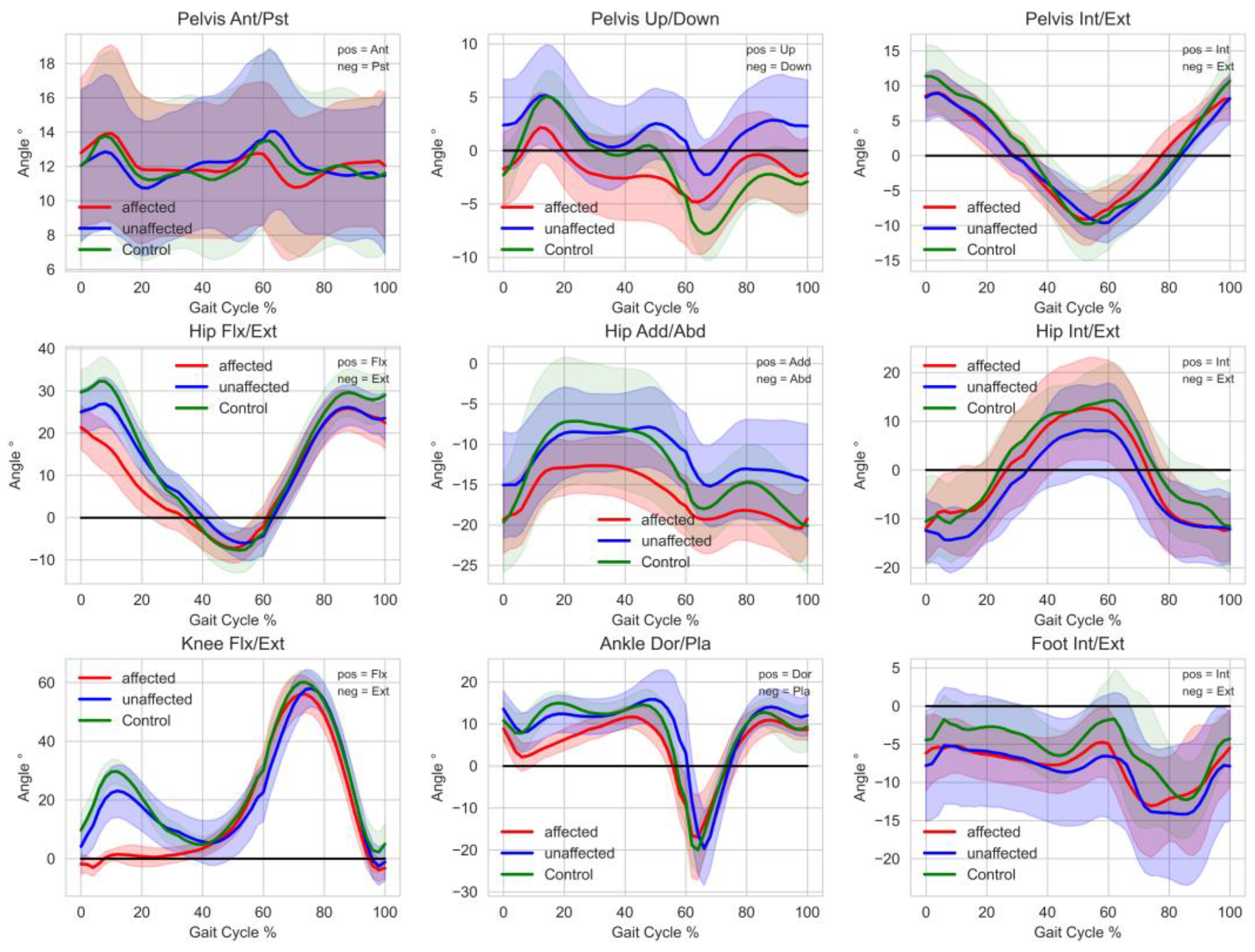
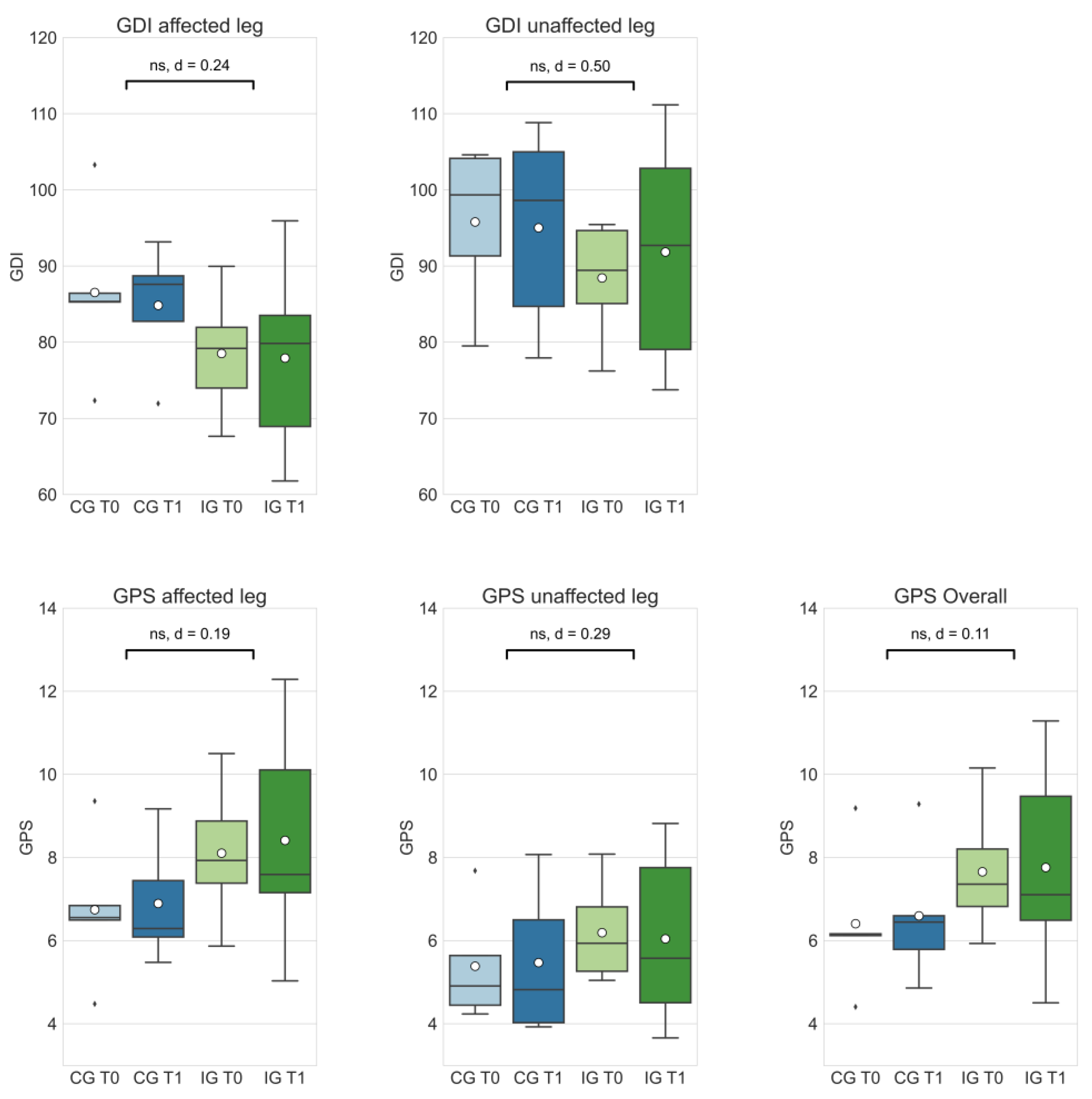
3.2. Gait Function at Baseline and Change during the Intervention
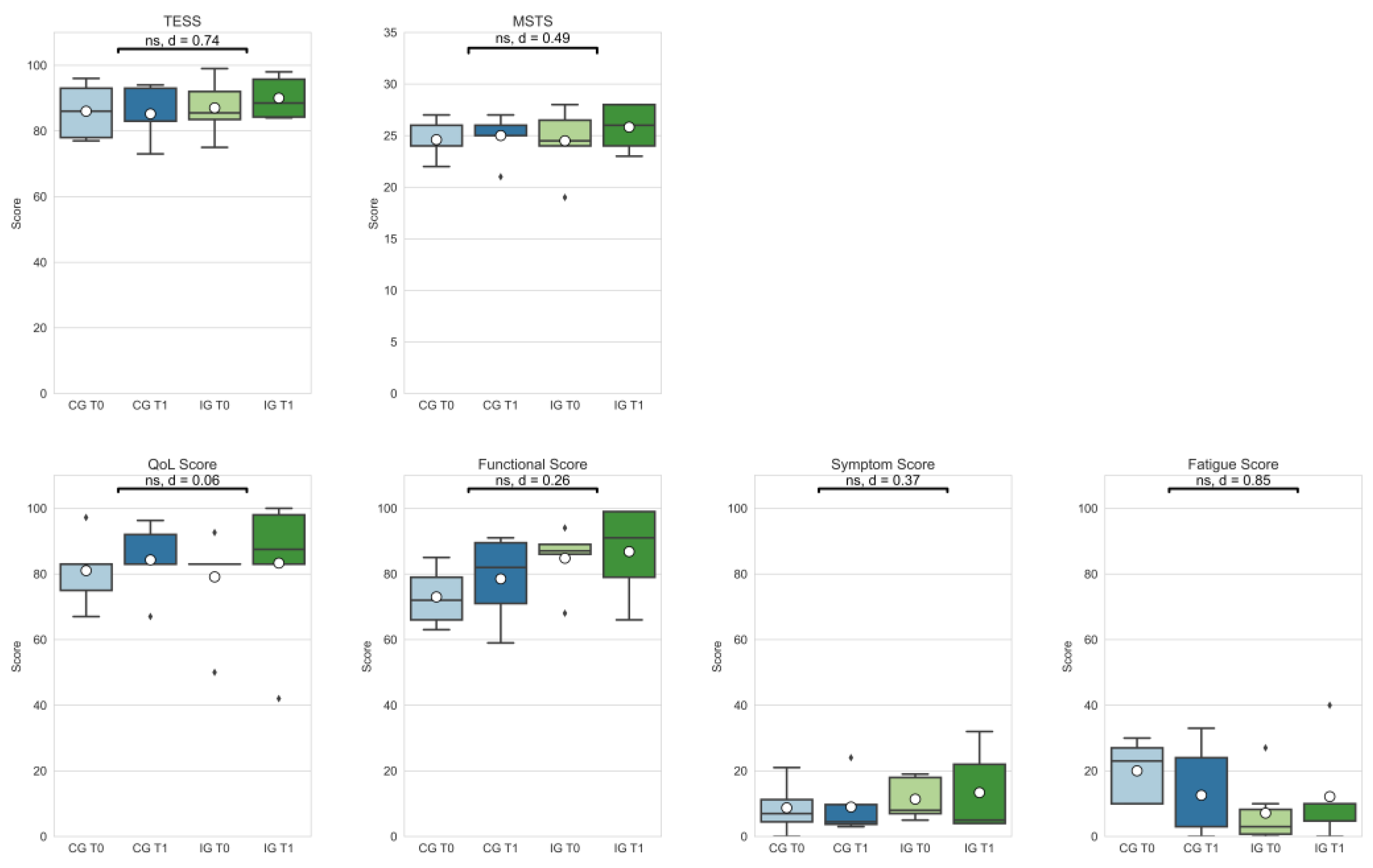
3.3. TESS and MSTS
3.4. Physical Function
3.5. Quality of Life and Fatigue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, K.D.; Fidler-Benaoudia, M.; Keegan, T.H.; Hipp, H.S.; Jemal, A.; Siegel, R.L. Cancer statistics for adolescents and young adults, 2020. CA A Cancer J. Clin. 2020, 70, 443–459. [Google Scholar] [CrossRef]
- Meltzer, P.S.; Helman, L.J. New Horizons in the Treatment of Osteosarcoma. N. Engl. J. Med. 2021, 385, 2066–2076. [Google Scholar] [CrossRef] [PubMed]
- Bölling, T.; Hardes, J.; Dirksen, U. Management of bone tumours in paediatric oncology. Clin. Oncol. (R. Coll. Radiol.) 2013, 25, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Grünewald, T.G.P.; Cidre-Aranaz, F.; Surdez, D.; Tomazou, E.M.; de Álava, E.; Kovar, H.; Sorensen, P.H.; Delattre, O.; Dirksen, U. Ewing sarcoma. Nat. Rev. Dis. Primers 2018, 4, 5. [Google Scholar] [CrossRef]
- Pugh, G.; Gravestock, H.L.; Hough, R.E.; King, W.M.; Wardle, J.; Fisher, A. Health Behavior Change Interventions for Teenage and Young Adult Cancer Survivors: A Systematic Review. J. Adolesc. Young Adult Oncol. 2016, 5, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Pugh, G.; Hough, R.; Gravestock, H.; Davies, C.; Horder, R.; Fisher, A. The development and user evaluation of health behaviour change resources for teenage and young adult Cancer survivors. Res. Involv. Engagem. 2019, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, C.; Rechnitzer, C.; Andersen, E.A.W.; Kenborg, L.; Norsker, F.N.; Bautz, A.; Baad-Hansen, T.; Tryggvadottir, L.; Madanat-Harjuoja, L.-M.; Holmqvist, A.S.; et al. Somatic Disease in Survivors of Childhood Malignant Bone Tumors in the Nordic Countries. Cancers 2021, 13, 4505. [Google Scholar] [CrossRef] [PubMed]
- Ranft, A.; Seidel, C.; Hoffmann, C.; Paulussen, M.; Warby, A.-C.; Berg, H.V.D.; Ladenstein, R.; Rossig, C.; Dirksen, U.; Rosenbaum, D.; et al. Quality of Survivorship in a Rare Disease: Clinicofunctional Outcome and Physical Activity in an Observational Cohort Study of 618 Long-Term Survivors of Ewing Sarcoma. J. Clin. Oncol. 2017, 35, 1704–1712. [Google Scholar] [CrossRef] [PubMed]
- Tan, P.; Yong, B.; Wang, J.; Huang, G.; Yin, J.; Zou, C.; Xie, X.; Tang, Q.; Shen, J. Analysis of the efficacy and prognosis of limb-salvage surgery for osteosarcoma around the knee. Eur. J. Surg. Oncol. 2012, 38, 1171–1177. [Google Scholar] [CrossRef] [PubMed]
- Pesenti, S.; Peltier, E.; Pomero, V.; Authier, G.; Roscigni, L.; Viehweger, E.; Jouve, J.-L. Knee function after limb salvage surgery for malignant bone tumor: Comparison of megaprosthesis and distal femur allograft with epiphysis sparing. Int. Orthop. 2018, 42, 427–436. [Google Scholar] [CrossRef]
- Mester, B.; Guder, W.; Streitbürger, A.; Schoepp, C.; Nottrott, M.; Podleska, L.; Dudda, M.; Hardes, J. Wiederkehr zu körperlicher Aktivität und Sport in der Tumororthopädie. [Return to Sports and Activity in Tumor Orthopaedics]. Z. Orthop. Unfall. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Gerber, L.H.; Hoffman, K.; Chaudhry, U.; Augustine, E.; Parks, R.; Bernad, M.; Mackall, C.; Steinberg, S.; Mansky, P. Functional outcomes and life satisfaction in long-term survivors of pediatric sarcomas. Arch. Phys. Med. Rehabil. 2006, 87, 1611–1617. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hu, A.; Zhang, M.; Shi, C.; Zhang, X.; Zhang, J. Correlation between functional status and quality of life after surgery in patients with primary malignant bone tumor of the lower extremities. Orthop. Nurs. 2014, 33, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Bekkering, W.P.; Vlieland, T.V.; Koopman, H.M.; Schaap, G.R.; Schreuder, H.B.; Beishuizen, A.; Tissing, W.J.; Hoogerbrugge, P.M.; Anninga, J.K.; Taminiau, A.H. Quality of life in young patients after bone tumor surgery around the knee joint and comparison with healthy controls. Pediatr. Blood Cancer 2010, 54, 738–745. [Google Scholar] [CrossRef]
- Müller, D.A.; Beltrami, G.; Scoccianti, G.; Cuomo, P.; Capanna, R. Allograft-prosthetic composite versus megaprosthesis in the proximal tibia-What works best? Injury 2016, 47 (Suppl. S4), S124–S130. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Winters-Stone, K.; Gerber, L.H.; George, S.M.; Fulton, J.E.; et al. American College of Sports Medicine Roundtable Report on Physical Activity, Sedentary Behavior, and Cancer Prevention and Control. Med. Sci. Sports Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef]
- Winter, C.C.; Müller, C.; Hardes, J.; Gosheger, G.; Boos, J.; Rosenbaum, D. The effect of individualized exercise interventions during treatment in pediatric patients with a malignant bone tumor. Support. Care Cancer 2013, 21, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.; Becker, H.; Kim, S. Unmet needs in adolescents and young adults with cancer: A mixed-method study using social media. J. Pediatr. Nurs. 2022, 64, 31–41. [Google Scholar] [CrossRef]
- Saghaei, M.; Saghaei, S. Implementation of an open-source customizable minimization program for allocation of patients to parallel groups in clinical trials. JBiSE 2011, 04, 734–739. [Google Scholar] [CrossRef]
- Westlake, B.; Pipitone, O.; Tedesco, N.S. Time to Functional Outcome Optimization After Musculoskeletal Tumor Resection. Cureus 2022, 14, e27317. [Google Scholar] [CrossRef] [PubMed]
- Kask, G.; Barner-Rasmussen, I.; Repo, J.P.; Kjäldman, M.; Kilk, K.; Blomqvist, C.; Tukiainen, E.J. Functional Outcome Measurement in Patients with Lower-Extremity Soft Tissue Sarcoma: A Systematic Literature Review. Ann. Surg. Oncol. 2019, 26, 4707–4722. [Google Scholar] [CrossRef]
- Enneking, W.F.; Dunham, W.; Gebhardt, M.C.; Malawar, M.; Pritchard, D.J. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin. Orthop. Relat. Res. 1993, 286, 241–246. [Google Scholar] [CrossRef]
- Davis, A.M.; Wright, J.G.; Williams, J.I.; Bombardier, C.; Griffin, A.; Bell, R.S. Development of a measure of physical function for patients with bone and soft tissue sarcoma. Qual. Life Res. 1996, 5, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Reijers, S.J.; Husson, O.; Soomers, V.L.; Been, L.B.; Bonenkamp, J.J.; van de Sande, M.A.; Verhoef, C.; van der Graaf, W.T.; van Houdt, W.J. Health-related quality of life after isolated limb perfusion compared to extended resection, or amputation for locally advanced extremity sarcoma: Is a limb salvage strategy worth the effort? Eur. J. Surg. Oncol. 2022, 48, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Saebye, C.; Fugloe, H.M.; Nymark, T.; Safwat, A.; Petersen, M.M.; Baad-Hansen, T.; Krarup-Hansen, A.; Keller, J. Factors associated with reduced functional outcome and quality of life in patients having limb-sparing surgery for soft tissue sarcomas—A national multicenter study of 128 patients. Acta Oncol. 2017, 56, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Burwinkle, T.M.; Katz, E.R.; Meeske, K.; Dickinson, P. The PedsQL in pediatric cancer: Reliability and validity of the Pediatric Quality of Life Inventory Generic Core Scales, Multidimensional Fatigue Scale, and Cancer Module. Cancer 2002, 94, 2090–2106. [Google Scholar] [CrossRef] [PubMed]
- Söntgerath, R.; Däggelmann, J.; Kesting, S.V.; Rueegg, C.S.; Wittke, T.-C.; Reich, S.; Eckert, K.G.; Stoessel, S.; Chamorro-Viña, C.; Wiskemann, J.; et al. Physical and functional performance assessment in pediatric oncology: A systematic review. Pediatr. Res. 2021, 91, 743–756. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; McGinley, J.L.; Schwartz, M.H.; Beynon, S.; Rozumalski, A.; Graham, H.K.; Tirosh, O. The gait profile score and movement analysis profile. Gait Posture 2009, 30, 265–269. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Rozumalski, A. The Gait Deviation Index: A new comprehensive index of gait pathology. Gait Posture 2008, 28, 351–357. [Google Scholar] [CrossRef]
- Kim, S.; Ryu, C.; Jung, S.-T. Differences in Kinematic and Kinetic Patterns According to the Bone Tumor Location after Endoprosthetic Knee Replacement Following Bone Tumor Resection: A Comparative Gait Analysis between Distal Femur and Proximal Tibia. J. Clin. Med. 2021, 10, 4100. [Google Scholar] [CrossRef] [PubMed]
- Rompen, J.C.; Ham, S.J.; Halbertsma, J.P.K.; van Horn, J.R. Gait and function in patients with a femoral endoprosthesis after tumor resection: 18 patients evaluated 12 years after surgery. Acta Orthop. Scand. 2002, 73, 439–446. [Google Scholar] [CrossRef]
- Winter, C.; Müller, C.; Brandes, M.; Brinkmann, A.; Hoffmann, C.; Hardes, J.; Gosheger, G.; Boos, J.; Rosenbaum, D. Level of activity in children undergoing cancer treatment. Pediatr. Blood Cancer 2009, 53, 438–443. [Google Scholar] [CrossRef]
- Bamdad, K.; Hudson, S.; Briggs, T. Factors associated with functional outcome in patients having limb salvage surgery for primary malignant bone sarcoma using TESS. J. Clin. Orthop. Trauma 2019, 10, 986–990. [Google Scholar] [CrossRef] [PubMed]
- Heaver, C.; Isaacson, A.; Gregory, J.J.; Cribb, G.; Cool, P. Patient factors affecting the Toronto extremity salvage score following limb salvage surgery for bone and soft tissue tumors. J. Surg. Oncol. 2016, 113, 804–810. [Google Scholar] [CrossRef]
- Bisschop, C.N.S.; Courneya, K.S.; Velthuis, M.J.; Monninkhof, E.M.; Jones, L.W.; Friedenreich, C.; van der Wall, E.; Peeters, P.H.M.; May, A.M. Control group design, contamination and drop-out in exercise oncology trials: A systematic review. PLoS ONE. 2015, 10, e0120996. [Google Scholar] [CrossRef]
- Wilson, P.J.; Steadman, P.; Beckman, E.M.; Connick, M.J.; Carty, C.P.; Tweedy, S.M. Fitness, Function, and Exercise Training Responses after Limb Salvage with a Lower Limb Megaprosthesis: A Systematic Review. PM&R 2019, 11, 533–547. [Google Scholar] [CrossRef]
- Van Egmond-van Dam, J.C.; Bekkering, W.P.; Bramer, J.A.M.; Beishuizen, A.; Fiocco, M.; Dijkstra, P.D.S. Functional outcome after surgery in patients with bone sarcoma around the knee; results from a long-term prospective study. J. Surg. Oncol. 2017, 115, 1028–1032. [Google Scholar] [CrossRef] [PubMed]
- Wurz, A.; McLaughlin, E.; Lategan, C.; Viña, C.C.; Grimshaw, S.L.; Hamari, L.; Götte, M.; Kesting, S.; Rossi, F.; van der Torre, P.; et al. The international Pediatric Oncology Exercise Guidelines (iPOEG). Transl. Behav. Med. Soc. Behav. Med. 2021, 11, 1915–1922. [Google Scholar] [CrossRef]
- Götte, M.; Gauß, G.; Dirksen, U.; Driever, P.H.; Basu, O.; Baumann, F.T.; Wiskemann, J.; Boos, J.; Kesting, S.V. Multidisciplinary Network ActiveOncoKids guidelines for providing movement and exercise in pediatric oncology—Consensus-based recommendations. Pediatr. Blood Cancer 2022, 69, e29953. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IG | CG | |||||
|---|---|---|---|---|---|---|
| Characteristic | Mean | SD | Range | Mean | SD | Range |
| Number of patients | 6 | - | - | 5 | - | - |
| Male/female | 3/3 | - | - | 3/2 | - | - |
| Tumor location | ||||||
| (Proximal tibia/distal femur) | 3/3 | - | - | 1/4 | - | - |
| Age at gait analysis (years) | 26.3 | 8.0 | 15–34 | 27.0 | 9.8 | 17–41 |
| Age at surgery (years) | 19.8 | 7.5 | 12–31 | 24.0 | 11.2 | 10–39 |
| Follow-up (years) | 6.5 | 6.1 | 1–16 | 3.0 | 2.3 | 1–7 |
| Weight (kg) | 69 | 12.4 | 52.0–82.0 | 76.1 | 25.9 | 60.0–122.0 |
| Height (cm) | 172.2 | 7.7 | 163–182 | 179.0 | 4.7 | 172.0–185.0 |
| BMI (kg/m2) | 23.4 | 4.7 | 18.0–29.1 | 23.4 | 6.8 | 20.0–35.6 |
| Leg Length Discrepancy (mm) | 23.7 | 30.5 | 1.6–83.2 | 13.6 | 13.3 | 3.9–36.9 |
| GDI (aff) | GDI (unaff.) | GPS (aff.) | GPS (unaff.) | GPS (Overall) | TESS | MSTS | QoL | Function | Symptom | Fatigue | TUG (sec) | TUDS (sec) | Knee Flexion Active (°) | Knee Flexion Passive (°) | Knee Extension Active (°) | Knee Extension Passive (°) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CG (n = 5) | T0 | Mean | 86.5 | 95.8 | 6.7 | 5.4 | 6.4 | 86.0 | 24.6 | 81.0 | 73.0 | 8.75 | 20.0 | 6.4 | 18.2 | 90.7 | 92.4 | 13.3 | 0.0 |
| Min | 72.3 | 79.5 | 4.5 | 4.2 | 4.4. | 77.0 | 22.0 | 67.0 | 63.0 | 0.0 | 10.0 | 5.1 | 9.5 | 80.0 | 85.0 | 5.0 | 0.0 | ||
| Max | 103.3 | 104.6 | 9.4 | 7.7 | 9.2 | 96.0 | 27.0 | 97.2 | 85.0 | 21.0 | 30.0 | 8.4 | 32.9 | 105.0 | 110.0 | 30.0 | 0.0 | ||
| 95%-CI | 72.9–100.2 | 82.7–108.9 | 4.6–8.9 | 3.6–7.1 | 4.3–8.6 | 75.4–96.6 | 22.2–27.0 | 67.1–95.0 | 57.2–88.8 | 0.0–22.8 | 8.3–31.7 | 4.7–8.2 | 6.3–30.0 | 58.6–122.7 | 79.9–104.9 | 0.0–49.2 | - | ||
| T1 | Mean | 84.8 | 95.0 | 6.9 | 5.5 | 6.6 | 85.2 | 25.0 | 84.3 | 78.5 | 9.0 | 12.6 | 5.9 | 17.1 | 86.0 | 95.2 | 14.0 | 2.0 | |
| Min | 71.9 | 78.0 | 5.5 | 3.9 | 4.9 | 73.0 | 21.0 | 67.0 | 59.0 | 3.0 | 0.0 | 4.0 | 7.9 | 70.0 | 85.0 | 0.0 | 0.0 | ||
| Max | 93.2 | 108.8 | 9.1 | 8.1 | 9.3 | 94. | 27.0 | 96.3 | 91.0 | 24.0 | 33.0 | 8.2 | 31.2 | 108.0 | 115.0 | 45.0 | 10.0 | ||
| 95%-CI | 74.8–94.9 | 78.6–111.5 | 5.1–8.7 | 3.3–7.7 | 4.5–8.6 | 74.5–95.9 | 22.1–28.0 | 70.3–98.2 | 54.9–100.0 | 0.0–25.0 | 0.0–31.1 | 3.7–8.1 | 6.2–28.1 | 68.9–103.1 | 79.7–110.7 | 0.0–36.1 | 0.0–7.6 | ||
| IG (n = 6) | T0 | Mean | 78.5 | 88.4 | 8.1 | 6.2 | 7.7 | 87.0 | 24.5 | 79.1 | 84.8 | 11.4 | 7.2 | 6.5 | 16.5 | 87.5 | 97.5 | 26.3 | 1.7 |
| Min | 67.6 | 76.2 | 5.9 | 5.0 | 5.9 | 75.0 | 19.0 | 50.0 | 68.0 | 5.0 | 0.0 | 4.1 | 9.9 | 66.0 | 70.0 | 10.0 | 0.0 | ||
| Max | 90.0 | 95.4 | 10.5 | 8.1 | 10.2 | 99.0 | 28.0 | 92.6 | 94.0 | 19.0 | 27.0 | 8.8 | 33.6 | 110.0 | 120.0 | 50.0 | 10.0 | ||
| 95%-CI | 70.4–86.7 | 80.5–96.4 | 6.4–9.8 | 5.0–7.4 | 6.1–9.2 | 78.1–95.9 | 21.2–27.8 | 63.6–94.6 | 72.5–97.1 | 3.2–19.6 | 0.0–18.1 | 4.8–8.1 | 7.4–25.6 | 72.3–102.7 | 78.2–116.8 | 7.6–45.1 | 0.0–6.0 | ||
| T1 | Mean | 77.9 | 91.8 | 8.4 | 6.0 | 7.8 | 90.0 | 25.8 | 83.3 | 86.8 | 13.4 | 12.2 | 5.6 | 14.7 | 82.5 | 98.3 | 16.0 | 0.8 | |
| Min | 61.8 | 73.8 | 5.0 | 3.7 | 4.5 | 84.0 | 23.0 | 42.0 | 66.0 | 4.0 | 0.0 | 3.8 | 8.3 | 55.0 | 70.0 | 0.0 | 0.0 | ||
| Max | 96.0 | 111.2 | 12.3 | 8.8 | 11.3 | 98.0 | 28.0 | 100.0 | 99.0 | 32.0 | 40.0 | 8.6 | 31.8 | 120.0 | 125.0 | 45.0 | 5.0 | ||
| 95%-CI | 64.8–91.0 | 75.8–107.9 | 5.6–11.2 | 3.8–8.3 | 5.1–10.4 | 83.1–96.9 | 23.3–28.4 | 60.6–100.0 | 69.1–100.0 | 0.0–29.4 | 0.0–27.2 | 4.0–7.3 | 5.5–23.9 | 59.8–105.2 | 75.2–121.4 | 0.0–37.2 | 0.0–3.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basteck, S.; Guder, W.K.; Dirksen, U.; Krombholz, A.; Streitbürger, A.; Reinhardt, D.; Götte, M. Effects of an Exercise Intervention on Gait Function in Young Survivors of Osteosarcoma with Megaendoprosthesis of the Lower Extremity—Results from the Pilot Randomized Controlled Trial proGAIT. Curr. Oncol. 2022, 29, 7754-7767. https://doi.org/10.3390/curroncol29100613
Basteck S, Guder WK, Dirksen U, Krombholz A, Streitbürger A, Reinhardt D, Götte M. Effects of an Exercise Intervention on Gait Function in Young Survivors of Osteosarcoma with Megaendoprosthesis of the Lower Extremity—Results from the Pilot Randomized Controlled Trial proGAIT. Current Oncology. 2022; 29(10):7754-7767. https://doi.org/10.3390/curroncol29100613
Chicago/Turabian StyleBasteck, Simon, Wiebke K. Guder, Uta Dirksen, Arno Krombholz, Arne Streitbürger, Dirk Reinhardt, and Miriam Götte. 2022. "Effects of an Exercise Intervention on Gait Function in Young Survivors of Osteosarcoma with Megaendoprosthesis of the Lower Extremity—Results from the Pilot Randomized Controlled Trial proGAIT" Current Oncology 29, no. 10: 7754-7767. https://doi.org/10.3390/curroncol29100613
APA StyleBasteck, S., Guder, W. K., Dirksen, U., Krombholz, A., Streitbürger, A., Reinhardt, D., & Götte, M. (2022). Effects of an Exercise Intervention on Gait Function in Young Survivors of Osteosarcoma with Megaendoprosthesis of the Lower Extremity—Results from the Pilot Randomized Controlled Trial proGAIT. Current Oncology, 29(10), 7754-7767. https://doi.org/10.3390/curroncol29100613