Health Behavior and Cancer Prevention among Adults with Li-Fraumeni Syndrome and Relatives in Germany—A Cohort Description

 , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
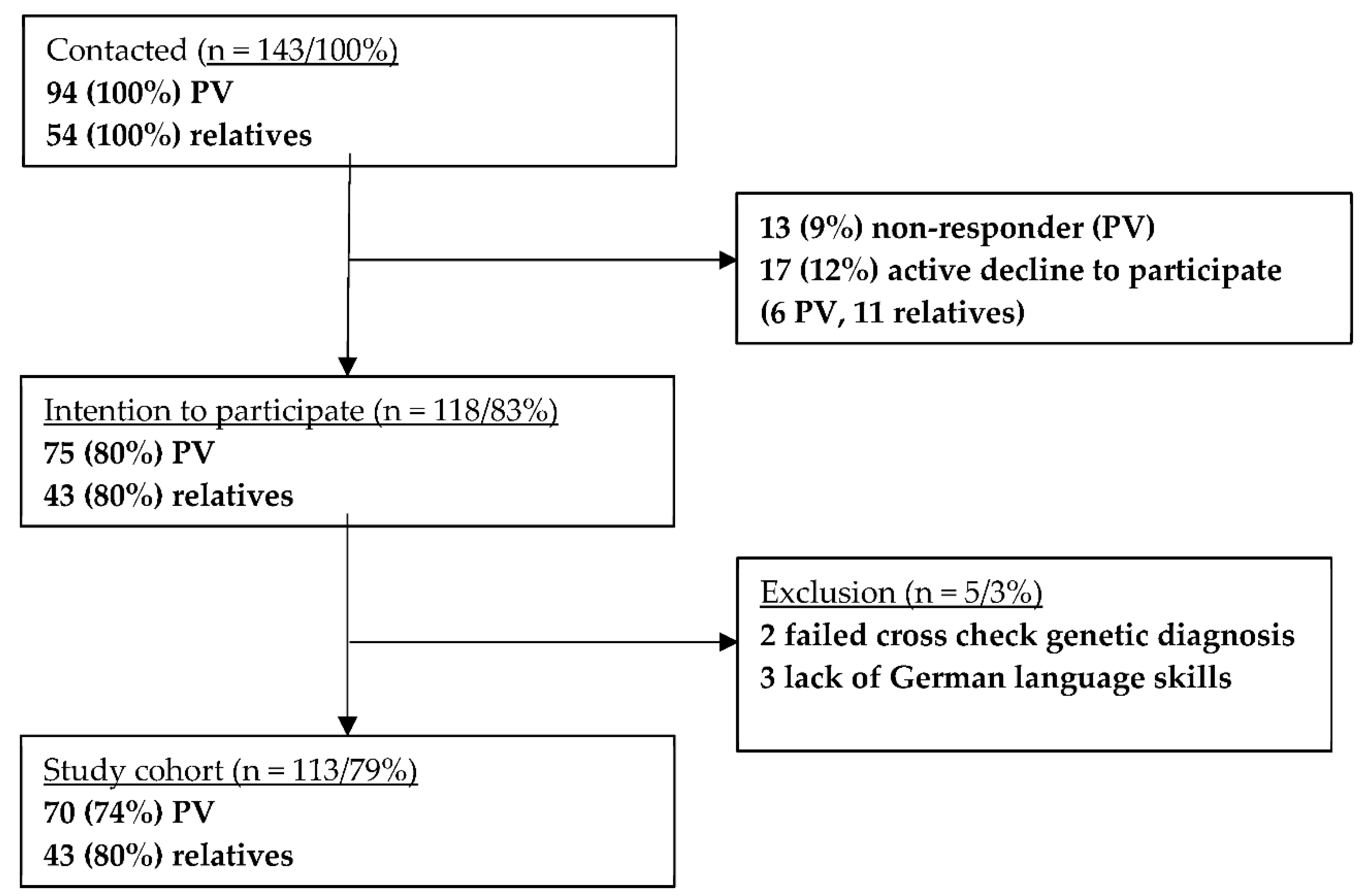
2.1. Study Population
2.2. Measurements
2.3. Statistical Analysis
3. Results
3.1. Study Cohort, Cancer Experiences
3.2. Lifestyle and Dietary Habits, Physical Activity, and Physical Wellbeing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kratz, C.P.; Achatz, M.I.; Brugières, L.; Frebourg, T.; Garber, J.E.; Greer, M.-L.C.; Hansford, J.R.; Janeway, K.A.; Kohlmann, W.K.; McGee, R.; et al. Cancer screening recommendations for individuals with li-fraumeni syndrome. Clin. Cancer Res. 2017, 23, e38–e45. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Shore, A.; Wasserman, J.D.; Stephens, D.; Kim, R.H.; Druker, H.; Gallinger, B.; Naumer, A.; Kohlmann, W.; Novokmet, A.; et al. Biochemical and imaging surveillance in germline TP53 mutation carriers with Li-Fraumeni syndrome: 11 year follow-up of a prospective observational study. Lancet Oncol. 2016, 17, 1295–1305. [Google Scholar] [CrossRef]
- Rippinger, N.; Fischer, C.; Haun, M.W.; Rhiem, K.; Grill, S.; Kiechle, M.; Cremer, F.W.; Kast, K.; Nguyen, H.P.; Ditsch, N.; et al. Cancer surveillance and distress among adult pathogenic TP53 germline variant carriers in Germany: A multicenter feasibility and acceptance survey. Cancer 2020, 126, 4032–4041. [Google Scholar] [CrossRef] [PubMed]
- Kratz, C.P.; Freycon, C.; Maxwell, K.N.; Nichols, K.E.; Schiffman, J.D.; Evans, D.G.; Achatz, M.I.; Savage, S.A.; Weitzel, J.N.; Garber, J.E.; et al. Analysis of the Li-Fraumeni spectrum based on an international germline TP53 variant data set: An international agency for research on cancer TP53 database analysis. JAMA Oncol. 2021, 7, 1800–1805. [Google Scholar] [CrossRef]
- Wang, P.-Y.; Ma, J.; Li, J.; Starost, M.F.; Wolfgang, M.J.; Singh, K.; Pirooznia, M.; Kang, J.-G.; Hwang, P.M. Reducing fatty acid oxidation improves cancer-free survival in a mouse model of li-fraumeni syndrome. Cancer Prev. Res. 2021, 14, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Whiteman, D.C.; Wilson, L.F. The fractions of cancer attributable to modifiable factors: A global review. Cancer Epidemiol. 2016, 44, 203–221. [Google Scholar] [CrossRef]
- Barnes, B.; Kraywinkel, K.; Nowossadeck, E.; Schönfeld, I.; Starker, A.; Wienecke, A.; Wolf, U. Bericht zum Krebsgeschehen in Deutschland 2016; Robert-Koch-Institut: Berlin, Germany, 2016; p. 185. [Google Scholar]
- Eng, L.; Pringle, D.; Su, J.; Shen, X.; Mahler, M.; Niu, C.; Charow, R.; Tiessen, K.; Lam, C.; Halytskyy, O.; et al. Patterns, perceptions, and perceived barriers to physical activity in adult cancer survivors. Support. Care Cancer 2018, 26, 3755–3763. [Google Scholar] [CrossRef] [PubMed]
- Steindorf, K.; Schmidt, M.E.; Klassen, O.; Ulrich, C.M.; Oelmann, J.; Habermann, N.; Beckhove, P.; Owen, R.; Debus, J.; Wiskemann, J.; et al. Randomized, controlled trial of resistance training in breast cancer patients receiving adjuvant radiotherapy: Results on cancer-related fatigue and quality of life. Ann. Oncol. 2014, 25, 2237–2243. [Google Scholar] [CrossRef]
- Depenbusch, J.; Haussmann, A.; Tsiouris, A.; Schmidt, L.; Wiskemann, J.; Ungar, N.; Sieverding, M.; Steindorf, K. The association between physicians’ exercise counseling and physical activity in patients with cancer: Which roles do patients’ satisfaction and previous physical activity levels play? Psychooncology 2020, 29, 1856–1863. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Winters-Stone, K.; Gerber, L.H.; George, S.M.; Fulton, J.E.; et al. American college of sports medicine roundtable report on physical activity, sedentary behavior, and cancer prevention and control. Med. Sci.Sports Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef] [PubMed]
- Kehm, R.D.; Genkinger, J.M.; MacInnis, R.J.; John, E.M.; Phillips, K.-A.; Dite, G.S.; Milne, R.L.; Zeinomar, N.; Liao, Y.; Knight, J.A.; et al. Recreational physical activity is associated with reduced breast cancer risk in adult women at high risk for breast cancer: A cohort study of women selected for familial and genetic risk. Cancer Res. 2020, 80, 116–125. [Google Scholar] [CrossRef]
- Pérez-López, F.R.; Chedraui, P.; Haya, J.; Cuadros, J.L. Effects of the Mediterranean diet on longevity and age-related morbid conditions. Maturitas 2009, 64, 67–79. [Google Scholar] [CrossRef]
- Grosso, G.; Buscemi, S.; Galvano, F.; Mistretta, A.; Marventano, S.; La Vela, V.; Drago, F.; Gangi, S.; Basile, F.; Biondi, A. Mediterranean diet and cancer: Epidemiological evidence and mechanism of selected aspects. BMC Surg. 2013, 13, S14. [Google Scholar] [CrossRef] [PubMed]
- Coletta, A.M.; Peterson, S.K.; Gatus, L.A.; Krause, K.J.; Schembre, S.M.; Gilchrist, S.C.; Arun, B.; You, Y.N.; Rodriguez-Bigas, M.A.; Strong, L.L.; et al. Diet, weight management, physical activity and Ovarian & Breast Cancer Risk in women with BRCA1/2 pathogenic Germline gene variants: Systematic review. Hered. Cancer Clin. Pract. 2020, 18, 5. [Google Scholar] [PubMed]
- Boffetta, P.; Hashibe, M. Alcohol and cancer. Lancet Oncol. 2006, 7, 149–156. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-item Mediterranean diet assessment tool and obesity indexes among high-risk subjects: The PREDIMED trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [PubMed]
- Hebestreit, K.; Yahiaoui-Doktor, M.; Engel, C.; Vetter, W.; Siniatchkin, M.; Erickson, N.; Halle, M.; Kiechle, M.; Bischoff, S.C. Validation of the German version of the Mediterranean Diet Adherence Screener (MEDAS) questionnaire. BMC Cancer 2017, 17, 341. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and MET intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef]
- Drixler, K.; Morfeld, M.; Glaesmer, H.; Brähler, E.; Wirtz, M.A. Validation of the Short-Form-Health-Survey-12 (SF-12 Version 2.0) assessing health-related quality of life in a normative German sample. Z. Fur Psychosom. Med. Psychother. 2020, 66, 272–286. [Google Scholar]
- Glenn, B.A.; Hamilton, A.S.; Nonzee, N.J.; Maxwell, A.E.; Crespi, C.M.; Ryerson, A.B.; Chang, L.C.; Deapen, D.; Bastani, R. Obesity, physical activity, and dietary behaviors in an ethnically-diverse sample of cancer survivors with early onset disease. J. Psychosoc. Oncol. 2018, 36, 418–436. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and mediterranean diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [PubMed]
- Raparelli, V.; Romiti, G.F.; Spugnardi, V.; Borgi, M.; Cangemi, R.; Basili, S.; Proietti, M.; the EVA Collaborative Group. Gender-related determinants of adherence to the mediterranean diet in adults with ischemic heart disease. Nutrients 2020, 12, 759. [Google Scholar] [CrossRef] [PubMed]
- Mensink, G.; Burger, M.; Beitz, R.; Henschel, Y.; Hintzpeter, B. Was essen wir heute? In Ernährungsverhalten in Deutschland; Beiträge zur Gesundheitsberichterstattung des Bundes; Robert Koch-Institut: Berlin, Germany, 2002. [Google Scholar]
- Arthur, R.S.; Wang, T.; Xue, X.; Kamensky, V.; E Rohan, T. Genetic factors, adherence to healthy lifestyle behavior, and risk of invasive breast cancer among women in the UK biobank. J. Natl. Cancer Inst. 2020, 112, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Kotsopoulos, J.; I Olopade, O.; Ghadirian, P.; Lubinski, J.; Lynch, H.T.; Isaacs, C.; Weber, B.; Kim-Sing, C.; Ainsworth, P.; Foulkes, W.; et al. Changes in body weight and the risk of breast cancer in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. 2005, 7, R833–R843. [Google Scholar] [CrossRef] [PubMed]
- Statista. 2017. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Gesundheitszustand-Relevantes-Verhalten/Tabellen/liste-koerpermasse.html (accessed on 22 December 2021).
- Kolb, R.; Sutterwala, F.S.; Zhang, W. Obesity and cancer: Inflammation bridges the two. Curr. Opin. Pharmacol. 2016, 29, 77–89. [Google Scholar] [CrossRef]
- Walcott, F.L.; Wang, P.-Y.; Bryla, C.M.; Huffstutler, R.D.; Singh, N.; Pollak, M.N.; Khincha, P.P.; A Savage, S.; Mai, P.L.; Dodd, K.W.; et al. Pilot study assessing tolerability and metabolic effects of metformin in patients with li-fraumeni syndrome. JNCI Cancer Spectr. 2020, 4, pkaa063. [Google Scholar] [CrossRef] [PubMed]
- World-Health-Organization. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 26 January 2022).
- Ginsburg, O.; Ghadirian, P.; Lubinski, J.; Cybulski, C.; Lynch, H.; Neuhausen, S.; Kim-Sing, C.; Robson, M.; Domchek, S.; Isaacs, C.; et al. Smoking and the risk of breast cancer in BRCA1 and BRCA2 carriers: An update. Breast Cancer Res. Treat. 2009, 114, 127–135. [Google Scholar] [CrossRef]
- Statista: Rauchen - Statistiken und Zahlen 2021. Available online: https://de.statista.com/themen/150/rauchen/ (accessed on 22 December 2021).
- Statista: Umfrage zur Häufigkeit des Alkoholkonsums in Deutschland bis 2021. Available online: https://de.statista.com/statistik/daten/studie/1200222/umfrage/haeufigkeit-alkoholkonsum-deutschland/ (accessed on 22 December 2021).
- Ormond, G.; Murphy, R. The effect of alcohol consumption on household income in Ireland. Alcohol 2016, 56, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Smarandescu, L.; Walker, D.; Wansink, B. Mindless drinking: How gender and BMI relate to the consumption of alcohol. Int. J. Drug Policy 2014, 25, 1131–1134. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The physical activity guidelines for americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef]
- Ancellin, R. Benefits of physical activity for cancer patients. Rev. Prat. 2019, 69, 438–443. [Google Scholar]
- Dorri, S.; Asadi, F.; Olfatbakhsh, A.; Kazemi, A. A systematic review of electronic health (eHealth) interventions to improve physical activity in patients with breast cancer. Breast Cancer 2020, 27, 25–46. [Google Scholar] [CrossRef] [PubMed]
- Van Duijnhoven, F.J.; Botma, A.; Winkels, R.; Nagengast, F.M.; Vasen, H.F.; Kampman, E. Do lifestyle factors influence colorectal cancer risk in Lynch syndrome? Fam. Cancer 2013, 12, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Mancebo, A.; González-Diéguez, M.L.; Navascués, C.A.; Cadahía, V.; Varela, M.; Pérez, R.; Rodrigo, L.; Rodríguez, M. Adherence to a semiannual surveillance program for hepatocellular carcinoma in patients with liver cirrhosis. J. Clin. Gastroenterol. 2017, 51, 557–563. [Google Scholar] [CrossRef]
- Wärnberg, J.; Pérez-Farinós, N.; Benavente-Marín, J.C.; Gómez, S.F.; Labayen, I.; G. Zapico, A.; Gusi, N.; Aznar, S.; Alcaraz, P.E.; González-Valeiro, M.; et al. Screen time and parents’ education level are associated with poor adherence to the mediterranean diet in spanish children and adolescents: The PASOS study. J. Clin. Med. 2021, 10, 795. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, B.; Lampert, T. Smoking and passive smoke exposure among adolescents in Germany. Dtsch. Arztebl. Int. 2016, 113, 23–30. [Google Scholar] [CrossRef]
- Statista. Bildungsstand: Verteilung der Bevölkerung in Deutschland nach höchstem Schulabschluss (Stand 2019). 2019. Available online: https://de.statista.com/statistik/daten/studie/1988/umfrage/bildungsabschluesse-in-deutschland/ (accessed on 7 January 2022).
- Statista: Durchschnittlicher Netto-Jahresarbeitslohn von ledigen Arbeitnehmern ohne Kinder¹ in Deutschland von 1960 bis 2022. 2021. Available online: https://de.statista.com/statistik/daten/studie/164047/umfrage/jahresarbeitslohn-in-deutschland-seit-1960/#:~:text=Im%20Jahr%202021%20betr%C3%A4gt%20der%20durchschnittliche%20Netto-Arbeitslohn%20-,Vergleich%20zum%20Vorjahr%20um%20rund%20vier%20Prozent%20gestiegen (accessed on 7 January 2022).
- Statista. Anzahl der Mitglieder und Versicherten der gesetzlichen und privaten Krankenversicherung in den Jahren 2014 bis 2020. 2020. Available online: https://de.statista.com/statistik/daten/studie/155823/umfrage/gkv-pkv-mitglieder-und-versichertenzahl-im-vergleich/ (accessed on 7 January 2022).
- Conley, C.C.; Agnese, D.M.; Vadaparampil, S.T.; Andersen, B.L. Factors associated with intentions for breast cancer risk management: Does risk group matter? Psychooncology 2019, 28, 1119–1126. [Google Scholar] [CrossRef]
- Cervera, S.; Aubá, E. Calidad de vida y dinámica familiar tras el diagnóstico de cáncer de mama. Boletín Psicol. 2005, 85, 7–29. [Google Scholar]
- Nübling, M.; Andersen, H.; Mühlbacher, A. Entwicklung eines Verfahrens zur Berechnung der Körperlichen und psychischen Summenskalen auf Basis der SOEP-Version des SF 12 (Algorithmus). In DIW Data Documentation; German Institute for Economic Research: Berlin Germany, 2006. [Google Scholar]
- Hoskins, L.M.; Roy, K.M.; Greene, M.H. Toward a new understanding of risk perception among young female BRCA1/2 “previvors”. Fam. Syst. Health 2012, 30, 32–46. [Google Scholar] [CrossRef]
- Katapodi, M.C.; Northouse, L.; Pierce, P.; Milliron, K.J.; Liu, G.; Merajver, S.D. Differences between women who pursued genetic testing for hereditary breast and ovarian cancer and their at-risk relatives who did not. Oncol. Nurs. Forum 2011, 38, 572–581. [Google Scholar] [CrossRef][Green Version]
- Erdmann, F.; Spix, C.; Katalinic, A.; Christ, M.; Folkerts, J.; Hansmann, J.; Kranzhöfer, K.; Kunz, B.; Manegold, K.; Penzkofer, A.; et al. Krebs in Deutschland für 2017/2018; Robert-Koch-Institut: Berlin, Germany, 2021; Volume 13. [Google Scholar]
- McCann, S.; MacAuley, D.; Barnett, Y.; Bunting, B.; Bradley, A.; Jeffers, L.; Morrison, P.J. Family communication, genetic testing and colonoscopy screening in hereditary non-polyposis colon cancer: A qualitative study. Psychooncology 2009, 18, 1208–1215. [Google Scholar] [CrossRef]
- Young, J.L.; Pantaleao, A.; Zaspel, L.; Bayer, J.; Peters, J.A.; Khincha, P.P.; Bremer, R.C.; Loud, J.T.; Greene, M.H.; Achatz, M.I.; et al. Couples coping with screening burden and diagnostic uncertainty in Li-Fraumeni syndrome: Connection versus independence. J. Psychosoc. Oncol. 2019, 37, 178–193. [Google Scholar] [CrossRef]
- Lammens, C.R.; Bleiker, E.M.; Verhoef, S.; Ausems, M.G.; Majoor-Krakauer, D.; Sijmons, R.H.; Hes, F.J.; Gómez-García, E.B.; Van Os, T.A.; Spruijt, L.; et al. Distress in partners of individuals diagnosed with or at high risk of developing tumors due to rare hereditary cancer syndromes. Psychooncology 2011, 20, 631–638. [Google Scholar] [CrossRef]


{kind=link}
| P/LP TP53 Variant Carriers (n = 70) | Relatives (n = 43) | p-Value | |
|---|---|---|---|
| Sex | <0.01 | ||
| Male n (%) | 12 (17.14) | 20 (46.51) | |
| Female n (%) | 58 (82.86) | 23 (53.49) | |
| Age (years) | 0.27 | ||
| Mean ± SD [range] | 41.52 ± 12.11 [20–54] | 38 ± 8.73 [22–66] | |
| Median | 38 | 36 | |
| Years since P/LP TP53 variant Diagnosis | |||
| Mean ± SD [range] | 3.43 ± 3.28 [0–16] | 4.95 ± 5.99 [0–25] | |
| Median | 2.0 | 3.0 | |
| 0 (%) | 3 (4) | 1 (2) | |
| >10 (%) | 2 (3) | 3 (7) | |
| Marital Status | 0.21 | ||
| Single (%) | 14 (20) | 5 (12) | |
| In a relationship (%) | 11 (16) | 8 (19) | |
| Married (%) | 41 (59) | 24 (56) | |
| Divorced (%) | 3 (4) | 2 (5) | |
| Widowed (%) | 1 (1) | 4 (9) | |
| Insurance Status | 1 | ||
| State (%) | 65 (93) | 40 (93) | |
| Private (%) | 5 (7) | 3 (7) | |
| Highest School-Leaving Qualification | 0.62 | ||
| High school (%) | 24 (35) | 15 (35) | |
| College (%) | 16 (23) | 9 (21) | |
| University (%) | 24 (35) | 18 (42) | |
| Other (%) | 5 (7) | 1 (2) | |
| Monthly Net Household Income (EUR ) | 0.16 | ||
| Mean ± SD [range] | 3270 ± 2103 [600–9167] | 3550 ± 1749 [450–7500] | |
| Median | 2545 | 3200 | |
| Current Occupation | 0.56 | ||
| Scholar/Student (%) | 6 (9) | 4 (9) | |
| Freelancer (%) | 2 (3) | 4 (9) | |
| Housewife (%) | 3 (7) | 2 (5) | |
| Employee (%) | 42 (60) | 24 (56) | |
| Public servant (%) | 6 (9) | 6 (14) | |
| Retired (%) | 6 (9) | 1 (2) | |
| Other (%) | 5 (7) | 2 (5) | |
| Family (Question 1.9, 1.11, 1.12 1) | |||
| Having children (%) | 39 (56) | 29 (67) | 0.3 |
| Child with cancer (%) | 9 (13) | 10 (23) | 0.45 |
| Child deceased due to cancer (%) | 1 (1) | 3 (7) | 0.19 |
| Sibling with P/LP TP53 variant (%) | 25 (36) | 1 (2) | <0.001 |
| Sibling deceased due to cancer (%) | 4 (6) | 0 (0) | n.a. + |
| Parent deceased due to cancer (%) | 13 (30) | 1 (2) | 0.07 |
| Own Cancer History (%) | 47 (67) | 4 (9) | <0.001 |
| Cancer Risk Estimation (%) | |||
| Own mean ± SD [range] | 71.78 ± 22.74 [15–100] | 37.71 ± 21.27 [5–100] | <0.001 |
| General mean ± SD [range] | 37.89 ± 18.42 [1–90] | 69.93 ± 29.88 [0–100] | <0.001 |
| Adherence to Surveillance Programm | 0.474 | ||
| Yes, totally (%) | 37 (53) | 27 (63) | |
| Yes, partially (%) | 24 (34) | 12 (28) | |
| Not anymore (%) | 0 (0) | 1 (2) | |
| Never have (%) | 4 (6) | 1 (2) | |
| Do not know (%) | 2 (3) | 1 (2) |
| P/LP TP53 Variant Carriers (n = 70) | Relatives (n = 43) | p-Value | |
|---|---|---|---|
| BMI (kg/m²) | 0.66 | ||
| Mean ± SD [range] | 26.82 ± 7.31 [18.52–66.21] | 25.83 ± 5.17 [18.22–40.72] | |
| Median | 24.97 | 24.44 | |
| BMI Distribution (%) | |||
| <25 kg/m² | 51 | 52 | |
| 25–<30 kg/m² | 29 | 31 | |
| 30–<35 kg/m² | 12 | 10 | |
| 35–<40 kg/m² | 6 | 2 | |
| >40 kg/m² | 3 | 5 | |
| MEDAS score | 6.59 | 5.51 | 0.01 |
| Pack years | 1.93 | 4.51 | 0.14 |
| Physical Activity (metabolic equivalents) | 22.63 | 18.99 | 0.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nees, J.; Kiermeier, S.; Struewe, F.; Keymling, M.; Maatouk, I.; Kratz, C.P.; Schott, S. Health Behavior and Cancer Prevention among Adults with Li-Fraumeni Syndrome and Relatives in Germany—A Cohort Description. Curr. Oncol. 2022, 29, 7768-7778. https://doi.org/10.3390/curroncol29100614
Nees J, Kiermeier S, Struewe F, Keymling M, Maatouk I, Kratz CP, Schott S. Health Behavior and Cancer Prevention among Adults with Li-Fraumeni Syndrome and Relatives in Germany—A Cohort Description. Current Oncology. 2022; 29(10):7768-7778. https://doi.org/10.3390/curroncol29100614
Chicago/Turabian StyleNees, Juliane, Senta Kiermeier, Farina Struewe, Myriam Keymling, Imad Maatouk, Christian P. Kratz, and Sarah Schott. 2022. "Health Behavior and Cancer Prevention among Adults with Li-Fraumeni Syndrome and Relatives in Germany—A Cohort Description" Current Oncology 29, no. 10: 7768-7778. https://doi.org/10.3390/curroncol29100614
APA StyleNees, J., Kiermeier, S., Struewe, F., Keymling, M., Maatouk, I., Kratz, C. P., & Schott, S. (2022). Health Behavior and Cancer Prevention among Adults with Li-Fraumeni Syndrome and Relatives in Germany—A Cohort Description. Current Oncology, 29(10), 7768-7778. https://doi.org/10.3390/curroncol29100614