
Mapping the Vulnerability of Older-Adult Neighborhoods: An Ecological Study of New York State

 , ,
, ,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
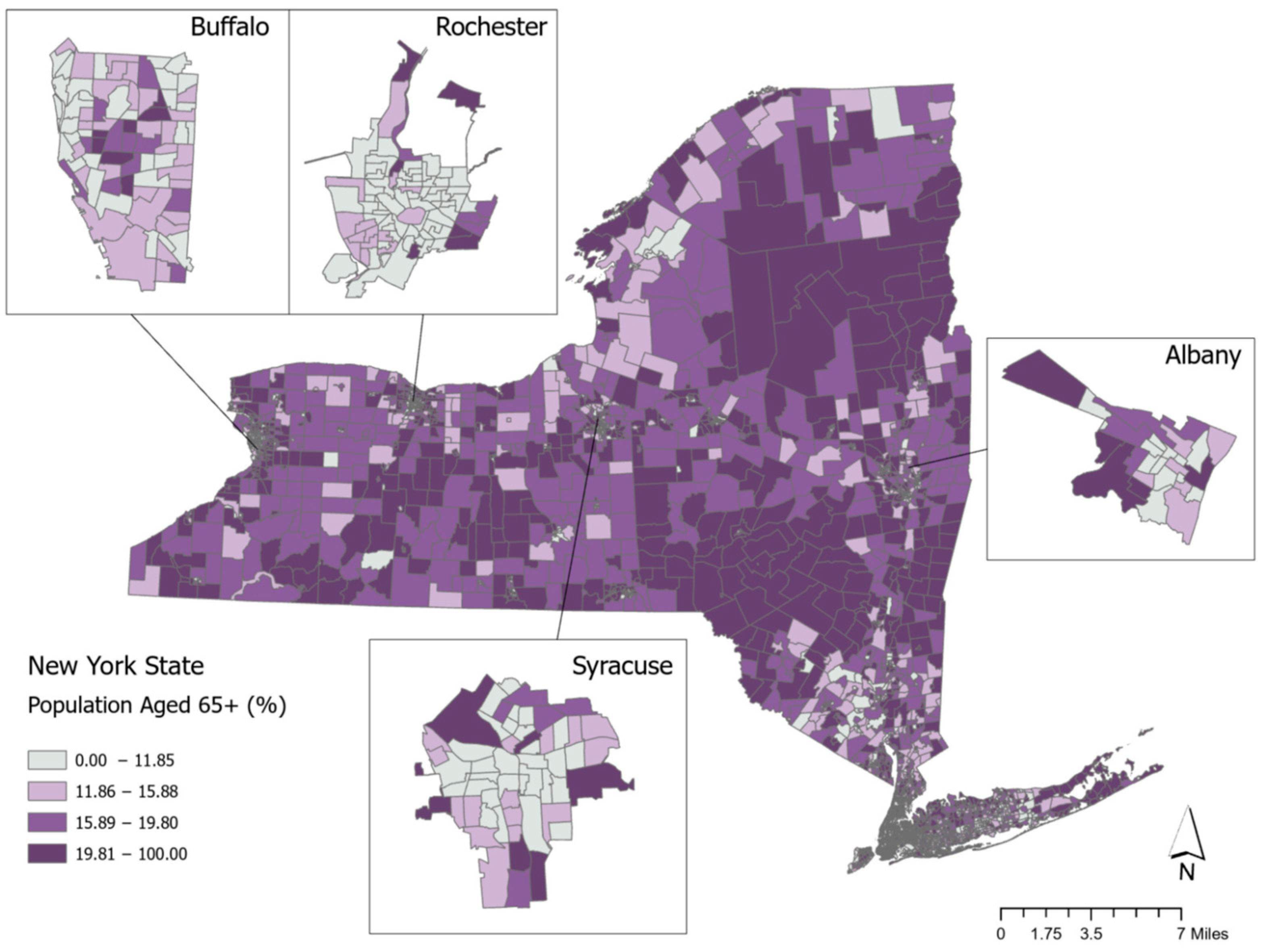
3.1. Spatial Variation in Older-Adult Neighborhoods
3.2. Demographic and Economic Characteristics of Older-Adult Neighborhoods
3.3. The Racial/Ethnic Composition and Redlining Status of Older-Adult Neighborhoods
3.4. Social Capital of Older-Adult Neighborhoods
3.5. Social Isolation of Older-Adult Neighborhoods
3.6. Retail Food Provider Access and Quality of Older-Adult Neighborhoods
3.7. Health Services of Older-Adult Neighborhoods
3.8. Summary of Key Findings
4. Discussion
4.1. Policy Implications
4.2. Study Limitations
4.3. Directions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- New York State Office for the Aging. 2021 Annual Report New York State Office for the Aging; New York State Office for the Aging: Albany, NY, USA, 2021.
- Schultz, L. Introducing New York’s Rural Economies; Rockefeller Institute of Government: Albany, NY, USA, 2019. [Google Scholar]
- World Health Organization. Decade of Healthy Ageing: Baseline Report; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-001790-0. [Google Scholar]
- World Health Organization. Global Age-Friendly Cities: A Guide; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- World Health Organization. Measuring the Age-Friendliness of Cities: A Guide to Using Core Indicators; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-150969-5. [Google Scholar]
- Black, K.; Oh, P. Assessing Age-Friendly Community Progress: What Have We Learned? Gerontologist 2022, 62, 6–17. [Google Scholar] [CrossRef]
- Channer, N.S.; Hartt, M.; Biglieri, S. Aging-in-Place and the Spatial Distribution of Older Adult Vulnerability in Canada. Appl. Geogr. 2020, 125, 102357. [Google Scholar] [CrossRef]
- Hames, E.; Stoler, J.; Emrich, C.T.; Tewary, S.; Pandya, N. A GIS Approach to Identifying Socially and Medically Vulnerable Older Adult Populations in South Florida. Gerontologist 2016, 57, 1133–1141. [Google Scholar] [CrossRef]
- Rugel, E.J.; Chow, C.K.; Corsi, D.J.; Hystad, P.; Rangarajan, S.; Yusuf, S.; Lear, S.A. Developing Indicators of Age-Friendly Neighbourhood Environments for Urban and Rural Communities across 20 Low-, Middle-, and High-Income Countries. BMC Public Health 2022, 22, 87. [Google Scholar] [CrossRef] [PubMed]
- Cutter, S.L.; Boruff, B.J.; Shirley, W.L. Social Vulnerability to Environmental Hazards*. Soc. Sci. Q. 2003, 84, 242–261. [Google Scholar] [CrossRef]
- Cutter, S.L. The Origin and Diffusion of the Social Vulnerability Index (SoVI). Int. J. Disaster Risk Reduct. 2024, 109, 104576. [Google Scholar] [CrossRef]
- Park, G.; Xu, Z. The Constituent Components and Local Indicator Variables of Social Vulnerability Index. Nat. Hazards 2022, 110, 95–120. [Google Scholar] [CrossRef]
- Deziel, N.C.; Warren, J.L.; Bravo, M.A.; Macalintal, F.; Kimbro, R.T.; Bell, M.L. Assessing Community-Level Exposure to Social Vulnerability and Isolation: Spatial Patterning and Urban-Rural Differences. J. Expo. Sci. Environ. Epidemiol. 2023, 33, 198–206. [Google Scholar] [CrossRef]
- Mah, J.C.; Penwarden, J.L.; Pott, H.; Theou, O.; Andrew, M.K. Social Vulnerability Indices: A Scoping Review. BMC Public Health 2023, 23, 1253. [Google Scholar] [CrossRef]
- Shaharudin, A.; Van Loenen, B.; Janssen, M. Developing an Open Data Intermediation Business Model: Insights from the Case of Esri. Trans. GIS 2025, 29, e13304. [Google Scholar] [CrossRef]
- Yang, T.-C.; Kim, S.; Matthews, S.A. Unemployment and Opioid-Related Mortality Rates in U.S. Counties: Investigating Social Capital and Social Isolation-Smoking Pathways. Soc. Probl. 2023, 70, 533–553. [Google Scholar] [CrossRef]
- Deng, X.; Friedman, S.; Ryan, I.; Zhang, W.; Dong, G.; Rodriguez, H.; Yu, F.; Huang, W.; Nair, A.; Luo, G.; et al. The Independent and Synergistic Impacts of Power Outages and Floods on Hospital Admissions for Multiple Diseases. Sci. Total Environ. 2022, 828, 154305. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. American Community Survey [ACS] 2019, 5-Year Summary Data File. 2019. Available online: https://www2.census.gov/programs-surveys/acs/summary_file/2019/prototype/ (accessed on 30 September 2024).
- United Health Foundation. America’s Health Rankings Senior Report 2018; 2018. Available online: https://assets.americashealthrankings.org/app/uploads/ahrsenior18-finalv1.pdf (accessed on 30 September 2024).
- Nelson, R.K.; Winling, L. Mapping Inequality: Redlining in New Deal America. Available online: https://dsl.richmond.edu/panorama/redlining/ (accessed on 30 September 2024).
- Richardson, J.; Mitchell, B.; Edlebi, J.; Meier, H.; Lynch, E. The Lasting Impact of Historic “Redlining” on Neighborhood Health: Higher Prevalence of COVID-19 Risk Factors; National Community Reinvestment Coalition: Washington, DC, USA, 2020. [Google Scholar]
- U.S. Department of Agriculture. Food Access Research Atlas: Documentation; Economic Research Service: Washington, DC, USA, 2019.
- Centers for Disease Control and Prevention. Census Tract Level State Maps of the Modified Food Environment Index (mRFEI) 2012. Available online: https://stacks.cdc.gov/view/cdc/61367 (accessed on 30 September 2024).
- ESRI ArcGIS Pro–Business Analyst Data 2020. Available online: https://pro.arcgis.com/en/pro-app/latest/help/analysis/business-analyst/data-overview.htm (accessed on 30 September 2024).
- Agency for Healthcare Research and Quality AHRQ. Social Determinants of Health (SDOH) Database: Data Source Documentation; 2021. Available online: https://www.ahrq.gov/sdoh/data-analytics/sdoh-data.html (accessed on 30 September 2024).
- Fraser, T.; Page-Tan, C.; Aldrich, D.P. Social Capital’s Impact on COVID-19 Outcomes at Local Levels. Sci. Rep. 2022, 12, 6566. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.; Lee, Y. Where Will Older Adults Reside? Evidence from Calgary, Canada. Cities 2024, 149, 104924. [Google Scholar] [CrossRef]
- Dao, T.H.D.; Dao, K.A.; Barboza-Salerno, G. Uncovering Spatial Patterns of Residential Settlements, Segregation, and Vulnerability of Urban Seniors Using Geospatial Analytics and Modeling Techniques. Urban Sci. 2024, 8, 81. [Google Scholar] [CrossRef]
- Golant, S.M. Residential Concentrations of the Future Elderly. Gerontologist 1975, 15, 16–23. [Google Scholar] [CrossRef]
- Wiseman, R.F. Why Older People Move: Theoretical Issues. Res. Aging 1980, 2, 141–154. [Google Scholar] [CrossRef]
- Gardner, P.J. Natural Neighborhood Networks—Important Social Networks in the Lives of Older Adults Aging in Place. J. Aging Stud. 2011, 25, 263–271. [Google Scholar] [CrossRef]
- Litwak, E.; Longino, F., Jr. Migration Patterns among the Elderly: A Developmental Perspective. Gerontologist 1987, 27, 266–272. [Google Scholar] [CrossRef]
- Crenshaw, K. Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics. In Feminist Legal Theories; Routledge: London, UK, 2013; pp. 23–51. [Google Scholar]
- Vickery, J. Using an Intersectional Approach to Advance Understanding of Homeless Persons’ Vulnerability to Disaster. Environ. Sociol. 2018, 4, 136–147. [Google Scholar] [CrossRef]
- Pope, N.E.; Greenfield, E.A.; Keyes, L.; Russell, E. A Review of Public Sector Engagement in Age-Friendly Community Initiatives. J. Aging Soc. Policy 2024, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Forsyth, A.; Lyu, Y. Making Communities Age-Friendly: Lessons from Implemented Programs. J. Plan. Lit. 2024, 39, 3–24. [Google Scholar] [CrossRef]
- Hansmann, K.J.; Deemer, D.A.; Robert, S. Measuring Age-Friendliness of Transportation and Mobility Characteristics in Communities: A Scoping Review. Gerontologist 2024, 64, gnad106. [Google Scholar] [CrossRef] [PubMed]
- Van Hoof, J.; Marston, H.R.; Kazak, J.K.; Buffel, T. Ten Questions Concerning Age-Friendly Cities and Communities and the Built Environment. Build. Environ. 2021, 199, 107922. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Mean/(SD) | Percentage of Older Adults (65+) | Percentage of Older Adults Living Alone | Percentage of Older Adults Living Below Poverty Line | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | High (1) | Low (2) | 95% CI (3) | p-Value (4) | High (5) | Low (6) | 95% CI (7) | p-Value (8) | High (9) | Low (10) | 95% CI (11) | p-Value (12) | ||
| Education BA or higher (%) | 40 (18) | 33 (19) | 5.7, 8.1 | <0.001 | 41 (21) | 39 (17) | −0.50, 4.6 | 0.11 | 34 (17) | 41 (18) | −10, −4.0 | <0.001 | ||
| N | 1213 | 3636 | 316 | 897 | 156 | 1057 | ||||||||
| Median income | 40,223 (16,122) | 35,330 (16,970) | 3829, 5958 | <0.001 | 40,236 (19,640) | 40,218 (14,701) | −2365, 2401 | >0.9 | 29,160 (15,007) | 41,839 (15,643) | −15,246, −10,113 | <0.001 | ||
| N | 1208 | 3628 | 314 | 894 | 154 | 1054 | ||||||||
| Own house (%) | 72 (22) | 53 (29) | 17, 21 | <0.001 | 56 (24) | 77 (18) | −25, −19 | <0.001 | 39 (26) | 77 (16) | −42, −33 | <0.001 | ||
| N | 1212 | 3616 | 316 | 896 | 155 | 1057 | ||||||||
| Older adults with disabilities (%) | 32 (11) | 34 (13) | −3.3, −1.8 | <0.001 | 37 (12) | 30 (10) | 5.2, 8.2 | <0.001 | 42 (14) | 30 (9) | 9.4, 14 | <0.001 | ||
| N | 1213 | 3598 | 316 | 897 | 156 | 1057 | ||||||||
| Unemployment Rate | 2.70 (1.66) | 3.81 (2.92) | −1.2, −0.98 | <0.001 | 2.84 (1.83) | 2.66 (1.60) | −0.05, 0.41 | 0.12 | 3.30 (2.10) | 2.62 (1.57) | 0.34, 1.0 | <0.001 | ||
| N | 1213 | 3639 | 316 | 897 | 156 | 1057 | ||||||||
| Percentage of Older Adults (65+) | Percentage of Older Adults Living Alone | Percentage of Older Adults Living Below Poverty Line | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High (1) | Low (2) | 95% CI (3) | p-Value (4) | High (5) | Low (6) | 95% CI (7) | p-Value (8) | High (9) | Low (10) | 95% CI (11) | p-Value (12) | |||
| Panel A. Racial/ethnic composition—percentages | ||||||||||||||
| NH Black Racial composition | 8 (18) | 18 (24) | −11, −8.5 | <0.001 | 11 (19) | 7 (18) | 1.8, 6.7 | <0.001 | 17 (24) | 7 (17) | 6.6, 14 | <0.001 | ||
| NH White Racial composition | 73 (27) | 49 (34) | 22, 25 | <0.001 | 68 (27) | 75 (27) | −11, −3.8 | <0.001 | 45 (31) | 77 (24) | −38, −27 | <0.001 | ||
| Asian Racial composition | 8 (13) | 9 (13) | −1.9, −0.19 | 0.017 | 7 (10) | 8 (14) | −2.3, 0.68 | 0.3 | 16 (22) | 6 (11) | 6.5, 14 | <0.001 | ||
| Hispanic Racial composition | 9 (11) | 21 (21) | −13, −11 | <0.001 | 11 (13) | 8 (10) | 1.5, 4.7 | <0.001 | 19 (19) | 8 (8) | 8.0, 14 | <0.001 | ||
| N (census tracts) | 1213 | 3640 | 316 | 897 | 156 | 1057 | ||||||||
| Source: Tabulations of American Community Survey 2019 5-year data | ||||||||||||||
| Panel B. Redlining score | <0.001 | <0.001 | <0.001 | |||||||||||
| 0 <= Average redlining < 3 | 1014 (95%) | 2620 (80%) | 260 (91%) | 755 (97%) | 119 (82%) | 895 (97%) | ||||||||
| 3 <= Average redlining < 4 | 47 (4.4%) | 563 (17%) | 23 (8.0%) | 24 (3.1%) | 25 (17%) | 22 (2.4%) | ||||||||
| Average redlining score = 4 | 5 (0.5%) | 100 (3.0%) | 3 (1.0%) | 2 (0.3%) | 2 (1.4%) | 3 (0.3%) | ||||||||
| N (census tracts) | 1066 | 3283 | 286 | 780 | 146 | 920 | ||||||||
| Percentage of Older Adults (65+) | Percentage of Older Adults Living Alone | Percentage of Older Adults Living Below Poverty Line | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High (1) | Low (2) | 95% CI (3) | p-Value (4) | High (5) | Low (6) | 95% CI (7) | p-Value (8) | High (9) | Low (10) | 95% CI (11) | p-Value (12) | |||
| Social Capital | 0.56 (0.09) | 0.50 (0.10) | 0.05, 0.06 | <0.001 | 0.53 (0.08) | 0.56 (0.09) | −0.04, −0.02 | <0.001 | 0.48 (0.09) | 0.57 (0.08) | −0.11, −0.08 | <0.001 | ||
| Bonding | 0.51 (0.09) | 0.50 (0.10) | 0.01, 0.02 | <0.001 | 0.47 (0.09) | 0.52 (0.09) | −0.06, −0.04 | <0.001 | 0.41 (0.10) | 0.52 (0.08) | −0.13, −0.10 | <0.001 | ||
| Bridging | 0.52 (0.19) | 0.42 (0.20) | 0.09, 0.11 | <0.001 | 0.50 (0.18) | 0.52 (0.19) | −0.04, 0.01 | 0.14 | 0.41 (0.21) | 0.53 (0.18) | −0.15, −0.08 | <0.001 | ||
| Linking | 0.64 (0.10) | 0.59 (0.12) | 0.05, 0.06 | <0.001 | 0.63 (0.11) | 0.65 (0.10) | −0.04, −0.01 | 0.002 | 0.60 (0.12) | 0.65 (0.10) | −0.07, −0.03 | <0.001 | ||
| N | 1213 | 3640 | 316 | 897 | 156 | 1057 | ||||||||
| Percentage of Older Adults (65+) | Percentage of Older Adults Living Alone | Percentage of Older Adults Living Below Poverty Line | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Social Isolation | High (1) | Low (2) | 95% CI (3) | p-Value (4) | High (5) | Low (6) | 95% CI (7) | p-Value (8) | High (9) | Low (10) | 95% CI (11) | p-Value (12) | ||
| Social isolation index | −0.14 (0.60) | 0.05 (0.68) | −0.23, −0.15 | <0.001 | 0.43 (0.59) | −0.35 (0.45) | 0.71, 0.85 | <0.001 | 0.74 (0.71) | −0.27 (0.46) | 0.90, 1.1 | <0.001 | ||
| N (census tracts) | 1213 | 3598 | 316 | 897 | 156 | 1057 | ||||||||
| Percentage 65+ | 25 (7) | 13 (4) | 11, 12 | <0.001 | 25.8 (8.6) | 24.4(5.7) | 0.33, 2.4 | 0.01 | 26.0 (7.4) | 24.6 (6.4) | 0.20, 2.7 | 0.023 | ||
| N (census tracts) | 1213 | 3640 | 316 | 897 | 156 | 1057 | ||||||||
| Percentage of Older Adults (65+) | Percentage of Older Adults Living Alone | Percentage of Older Adults Living Below Poverty Line | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High (1) | Low (2) | 95% CI (3) | p-Value (4) | High (5) | Low (6) | 95% CI (7) | p-Value (8) | High (9) | Low (10) | 95% CI (11) | p-Value (12) | |||
| Panel A. Food Access | ||||||||||||||
| Low-access tract at 1 and 10 miles | 328 (27%) | 608 (17%) | 7.5%, 13% | <0.001 | 72 (23%) | 256 (29%) | −11%, −0.05% | 0.057 | 12 (7.7%) | 316 (30%) | −28%, −17% | <0.001 | ||
| Low-access tract at one-half and 10 miles | 573 (47%) | 1395 (38%) | 5.6%, 12% | <0.001 | 153 (48%) | 420 (47%) | −5.0%, 8.2% | 0.7 | 33 (21%) | 540 (51%) | −37%, −22% | <0.001 | ||
| Low-access tract using vehicle access and at 20 miles | 242 (20%) | 543 (15%) | 2.4%, 7.6% | <0.001 | 96 (30%) | 146 (16%) | 8.3%, 20% | <0.001 | 27 (17%) | 215 (20%) | −9.8%, 3.7% | 0.4 | ||
| N (census tracts) | 1213 | 3637 | 316 | 897 | 156 | 1057 | ||||||||
| Source: USDA data on food access (see https://www.ers.usda.gov/data-products/food-access-research-atlas/documentation/ (accessed on 30 September 2024) for definitions) | ||||||||||||||
| Panel B. Quality of food retailers | ||||||||||||||
| Modified Retail Food Environment Index (%)—mRFEI | 12 (13) | 9 (9) | 2.1, 3.9 | <0.001 | 11 (11) | 13 (13) | −3.2, 0.21 | 0.086 | 10 (10) | 12 (13) | −4.3, −0.44 | 0.017 | ||
| N (census tracts) | 990 | 3146 | 261 | 729 | 131 | 859 | ||||||||
| Percentage of Older Adults (65+) | Percentage of Older Adults Living Alone | Percentage of Older Adults Living Below Poverty Line | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High (1) | Low (2) | 95% CI (3) | p-Value (4) | High (5) | Low (6) | 95% CI (7) | p-Value (8) | High (9) | Low (10) | 95% CI (11) | p-Value (12) | |||
| Panel A. Health Services Availability and Spending | ||||||||||||||
| Number of health services (mean) | 12 (8) | 8 (14) | 2.8, 5.2 | <0.001 | 16 (22) | 10 (16) | <0.001 | 12 (14) | 12 (18) | 0.9 | ||||
| Percentage of health services out of all businesses (mean) | 7.4 (7.1) | 5.3 (5.8) | 1.6, 2.5 | <0.001 | 9 (7) | 7 (7) | <0.001 | 9 (8) | 7 (7) | 0.011 | ||||
| Total spending on health services including insurance (in millions USD$) (mean) | 13.24 (10.2) | 10.47 (8.6) | 2.1, 3.5 | <0.001 | 14.88 (13.9) | 12.64 (8.4) | 0.011 | 9.52 (9.4) | 13.83 (10.2) | <0.001 | ||||
| N (census tracts) | 1066 | 3239 | 286 | 780 | 146 | 920 | ||||||||
| Source: ESRI Business Summary Data | ||||||||||||||
| Panel B. Accessibility and Distance to Health Services | ||||||||||||||
| Medically Underserved Areas | ||||||||||||||
| Yes (%) | 7.6% (92) | 22% (798) | −16%, −12% | <0.001 | 17% (54) | 4.3% (38) | 8.3%, 17% | <0.001 | 34% (53) | 3.7% (39) | 22%, 38% | <0.001 | ||
| Distance in miles to the nearest: | ||||||||||||||
| Emergency department | 3.8 (4.4) | 2.5 (3.1) | 1.1, 1.6 | <0.001 | 2.3 (2.7) | 4.3 (4.7) | −2.5, −1.6 | <0.001 | 1.3 (1.5) | 4.2 (4.5) | −3.3, −2.6 | <0.001 | ||
| Medical-surgical ICU | 4.1 (4.9) | 2.6 (3.4) | 1.2, 1.8 | <0.001 | 2.3 (2.7) | 4.8 (5.3) | −2.9, −2.0 | <0.001 | 1.3 (1.7) | 4.6 (5.1) | −3.7, −2.9 | <0.001 | ||
| Designated trauma center | 11 (13) | 7 (10) | 3.9, 5.6 | <0.001 | 8 (11) | 12 (14) | −6.1, −3.0 | <0.001 | 4 (7) | 12 (14) | −9.4, −6.5 | <0.001 | ||
| Health clinic | 4.4 (4.9) | 2.5 (3.7) | 1.7, 2.3 | <0.001 | 3.0 (4.2) | 5.0 (5.1) | −2.6, −1.5 | <0.001 | 1.4 (2.3) | 4.9 (5.1) | −4.0, −3.0 | <0.001 | ||
| Hospital with alcohol and drug abuse inpatient care | 6.4 (7.4) | 4.1 (5.7) | 1.9, 2.8 | <0.001 | 4 (5) | 7 (8) | −3.9, −2.3 | <0.001 | 2 (3) | 7 (8) | −5.5, −4.1 | <0.001 | ||
| N (census tracts) | 1209 | 3632 | 316 | 893 | 156 | 1053 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friedman, S.; Fang, C.; Yang, T.-C.; Li, R.; Mithu, I.H.; Manganello, J.A.; Romeiko, X.; Lin, S. Mapping the Vulnerability of Older-Adult Neighborhoods: An Ecological Study of New York State. Int. J. Environ. Res. Public Health 2025, 22, 332. https://doi.org/10.3390/ijerph22030332
Friedman S, Fang C, Yang T-C, Li R, Mithu IH, Manganello JA, Romeiko X, Lin S. Mapping the Vulnerability of Older-Adult Neighborhoods: An Ecological Study of New York State. International Journal of Environmental Research and Public Health. 2025; 22(3):332. https://doi.org/10.3390/ijerph22030332
Chicago/Turabian StyleFriedman, Samantha, Chunxu Fang, Tse-Chuan Yang, Rui Li, Imran Hossain Mithu, Jennifer A. Manganello, Xiaobo Romeiko, and Shao Lin. 2025. "Mapping the Vulnerability of Older-Adult Neighborhoods: An Ecological Study of New York State" International Journal of Environmental Research and Public Health 22, no. 3: 332. https://doi.org/10.3390/ijerph22030332
APA StyleFriedman, S., Fang, C., Yang, T.-C., Li, R., Mithu, I. H., Manganello, J. A., Romeiko, X., & Lin, S. (2025). Mapping the Vulnerability of Older-Adult Neighborhoods: An Ecological Study of New York State. International Journal of Environmental Research and Public Health, 22(3), 332. https://doi.org/10.3390/ijerph22030332