
WHOQOL-BREF in Measuring Quality of Life Among Sickle Cell Disease Patients with Leg Ulcers

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Inclusion and Exclusion Criteria
2.3. Ethical Requirements
2.4. Clinical, Sociodemographic, and Socioeconomic Data
2.5. Quality-of-Life Data
2.6. Statistical Analysis
3. Results
3.1. Social Relationships in SCD Patients with and Without SLU
3.2. Internal Consistency Reliability of the WHOQOL-BREF
3.3. Quality-of-Life Score Based on the WHOQOL-BREF Questionnaire
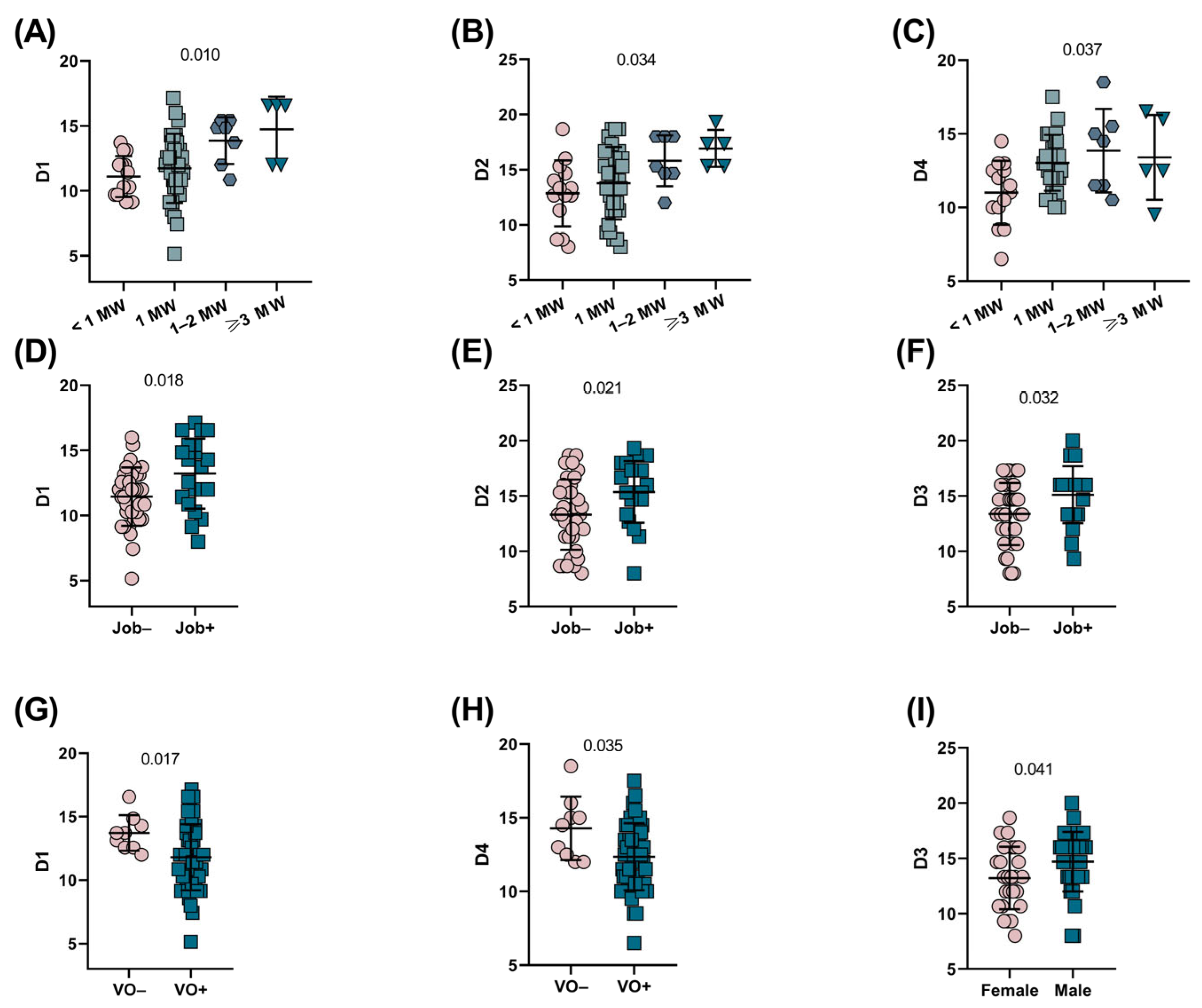
3.4. WHOQOL-BREF Domains Are Associated with Different Features of SCD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Al Saad, A.J.; Buhalim, R.A.; Al Jabr, F.A.; Al Dehailan, A.M.; Albahrani, A.A. The Correlation Between Surgical Procedures and Quality of Life Among Sickle Cell Disease Patients: A Perspective Saudi Study. Cureus 2022, 14, e21367. [Google Scholar] [CrossRef]
- Asnani, M.R.; Lipps, G.E.; Reid, M.E. Utility of WHOQOL-BREF in measuring quality of life in Sickle Cell Disease. Health Qual. Life Outcomes 2009, 7, 75. [Google Scholar] [CrossRef]
- Masese, R.V.; Bulgin, D.; Knisely, M.R.; Preiss, L.; Stevenson, E.; Hankins, J.S.; Treadwell, M.J.; King, A.A.; Gordeuk, V.R.; Kanter, J.; et al. Sex-based differences in the manifestations and complications of sickle cell disease: Report from the Sickle Cell Disease Implementation Consortium. PLoS ONE 2021, 16, e0258638. [Google Scholar] [CrossRef] [PubMed]
- Minniti, C.P.; Eckman, J.; Sebastiani, P.; Steinberg, M.H.; Ballas, S.K. Leg ulcers in sickle cell disease. Am. J. Hematol. 2010, 85, 831–833. [Google Scholar] [CrossRef] [PubMed]
- Monfort, J.B.; Senet, P. Leg Ulcers in Sickle-Cell Disease: Treatment Update. Adv. Wound Care 2020, 9, 348–356. [Google Scholar] [CrossRef]
- Serjeant, G.R. The natural history of sickle cell disease. Cold Spring Harb. Perspect. Med. 2013, 3, a011783. [Google Scholar] [CrossRef] [PubMed]
- Silva-Pinto, A.C.; Costa, F.F.; Gualandro, S.F.M.; Fonseca, P.B.B.; Grindler, C.M.; Souza Filho, H.C.R.; Bueno, C.T.; Cançado, R.D. Economic burden of sickle cell disease in Brazil. PLoS ONE 2022, 17, e0269703. [Google Scholar] [CrossRef]
- Silva Pinto, A.C.; Costa, F.F.; Gualandro, S.F.M.; Fonseca, P.B.B.; Bueno, C.T.; Cançado, R.D. Burden of Sickle Cell Disease: A Brazilian Societal Perspective Analysis. Blood 2020, 136, 10–11. [Google Scholar] [CrossRef]
- Gonçalves, M.S.; Bomfim, G.C.; Maciel, E.; Cerqueira, I.; Lyra, I.; Zanette, A.; Bomfim, G.; Adorno, E.V.; Albuquerque, A.L.; Pontes, A.; et al. ß S-Haplotypes in Sickle Cell Anemia Patients From Salvador, Bahia, Northeastern Brazil. Braz. J. Med. Biol. Res. 2003, 36, 1283–1288. [Google Scholar] [CrossRef]
- Verger. Flux et Reflux de la Traite des Nègres Entre le Golfe de Benin et Bahia de Todos os Santos; Sorbonne, Mouton & Co.: Paris, France, 1968. [Google Scholar]
- Florentino, M. Em Costas Negras, 1st ed.; Editora Unesp: São Paulo, Brazil, 2015; pp. 1–312. [Google Scholar]
- Carroll, P.C.; Haywood, C., Jr.; Hoot, M.R.; Lanzkron, S. A preliminary study of psychiatric, familial, and medical characteristics of high-utilizing sickle cell disease patients. Clin. J. Pain 2013, 29, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Spira, J.A.O.; Borges, E.L.; Guedes, A.C.M.; Andrade, P.G.R.; Lima, V.L.A.N. Prevalence of people with sickle cell disease and leg ulcers in Brazil: Socioeconomic and clinical overview. PLoS ONE 2022, 17, e0274254. [Google Scholar] [CrossRef] [PubMed]
- Mucalo, L.; Field, J.J.; Highland, J.; Khan, H.; Hankins, J.S.; Singh, A.; Brandow, A.M. Preliminary construct validity of patient-reported outcomes to assess chronic pain in adults with sickle cell disease. Blood Adv. 2023, 7, 3658–3665. [Google Scholar] [CrossRef]
- dos Santos, L.F.O.; Guimarães, M.W.; Baptista, A.F.; Sá, K.N. Impact of neuropathic pain on quality of life in adults with sickle cell disease: Observational study. Hematol. Transfus. Cell Ther. 2021, 43, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Umeh, N.I.; Ajegba, B.; Buscetta, A.J.; Abdallah, K.E.; Minniti, C.P.; Bonham, V.L. The psychosocial impact of leg ulcers in patients with sickle cell disease: I don’t want them to know my little secret. PLoS ONE 2017, 12, e0186270. [Google Scholar] [CrossRef] [PubMed]
- Ilić, I.; Šipetić-Grujičić, S.; Grujičić, J.; Živanović Mačužić, I.; Kocić, S.; Ilić, M. Psychometric properties of the world health organization’s quality of life (WHOQOL-BREF) questionnaire in medical students. Medicina 2019, 55, 772. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | SLU+ (N = 13) N (%) | SLU− (N = 42) N (%) |
|---|---|---|
| Age (years) | 33.8 | 34.8 |
| Gender | ||
| Female | 4 (30.8) | 22 (52.4) |
| Male | 9 (69.2) | 20 (47.6) |
| Age at 1st SCD diagnosis | ||
| <6 months | 1 (7.7) | 7 (16.7) |
| 6 months–4 years | 5 (38.5) | 6 (14.3) |
| 5–9 years | 2 (15.4) | 5 (11.9) |
| 10–14 years | 1 (7.7) | 4 (9.5) |
| 15–17 years | 2 (15.4) | 2 (4.8) |
| ≥18 years | 2 (15.4) | 18 (42.9) |
| Self-declared ethnicity | ||
| Black | 7 (53.8) | 22 (52.4) |
| Brown | 6 (46.2) | 17 (40.5) |
| Yellow | 0 | 1 (2.4) |
| Indigenous | 0 | 2 (4.8) |
| Income per capita | ||
| <1 minimum wage | 4 (30.8) | 10 (23.8) |
| 1 minimum wage | 8 (61.5) | 22 (52.4) |
| 1–2 times minimum wage | 0 | 7 (16.7) |
| ≥3 times minimum wages | 1 (7.7) | 3 (7.1) |
| Education | ||
| Illiterate/elementary school unfinished | 1 (7.7) | 5 (12.5) |
| Elementary school completed/middle school unfinished | 1 (7.7) | 2 (5) |
| Middle school completed/high school unfinished | 5 (38.5) | 14 (35) |
| High school completed/college degree unfinished | 5 (38.5) | 18 (45) |
| Graduated | 1 (7.7) | 1 (2.5) |
| Relatives with SCD | ||
| Siblings | 5 (38.5) | 22 (52.4) |
| Parents and siblings | 1 (7.7) | 2 (4.8) |
| Other relatives | 2 (15.4) | 6 (14.3) |
| None | 5 (38.5) | 12 (28.6) |
| Hydroxyurea | ||
| Yes | 10 (76.9) | 23 (54.7) |
| No | 3 (23.1) | 19 (45.3) |
| Occupation | ||
| Yes | 3 (23.1) | 17 (40.5) |
| No | 10 (76.9) | 25 (59.5) |
| Consumption of alcoholic beverages | ||
| Yes | 1 (11.1) | 13 (30.9) |
| No | 8 (88.9) | 29 (69.1) |
| Smoking | ||
| Yes | 0 (0) | 2 (4.8) |
| No | 9 (100) | 40 (95.2) |
| Vaccination schedule completed | ||
| Yes | 9 (69.2) | 35 (85.4) |
| No | 4 (30.8) | 6 (14.6) |
| Social Characteristics | SLU+ (N = 13) N (%) | SLU− (N = 42) N (%) |
|---|---|---|
| Friends | ||
| 0 | 4 (30.7) | 8 (22.9) |
| 1 | 2 (15.4) | 2 (5.7) |
| 2–3 | 1 (7.7) | 8 (22.9) |
| 4–6 | 3 (23.1) | 11 (31.4) |
| 7–10 | 3 (23.1) | 6 (17.1) |
| Close to family members | ||
| 0 | 1 (7.7) | 2 (5.7) |
| 1 | 0 (0) | 0 (0) |
| 2–3 | 1 (7.7) | 7 (20) |
| 4–6 | 4 (30.7) | 11 (31.5) |
| 7–10 | 7 (53.9) | 15 (42.8) |
| Frequency of social meetings | ||
| Daily or almost daily | 4 (30.7) | 10 (28.6) |
| Many times/week | 1 (7.7) | 6 (17.1) |
| Many times/month | 2 (15.4) | 9 (25.7) |
| Many times/year | 1 (7.7) | 5 (14.3) |
| Rarely | 5 (38.5) | 5 (14.3) |
| Sports practice | ||
| Yes | 2 (15.4) | 5 (14.3) |
| No | 11 (84.6) | 30 (85.7) |
| D1 Mean ± SD (Median, IQR) | D2 Mean ± SD (Median, IQR) | D3 Mean ± SD (Median, IQR) | D4 Mean ± SD (Median, IQR) | Cronbach’s Alpha Coefficient (All Domains) |
|---|---|---|---|---|
| 12.11 ± 2.54 (12.00, 10.28–13.71) | 14.08 ± 3.17 (14.66, 12.00–16.66) | 14.02 ± 2.83 (14.66, 12.00–16.00) | 12.66 ± 2.34 (12.50, 11.00–14.50) | 0.88 |
| Cronbach’s alpha coefficient of each domain | ||||
| 0.67 | 0.84 | 0.51 | 0.67 | |
| Domain | SCD N = 55 Mean ± SD | SLU+ N = 13 Mean ± SD | SLU− N = 42 Mean ± SD | p-Value |
|---|---|---|---|---|
| D1 | 12.11 ± 2.54 | 11.86 ± 2.59 | 12.08 ± 2.49 | 0.758 |
| D2 | 14.08 ± 3.17 | 14.76 ± 3.06 | 13.79 ± 3.20 | 0.404 |
| D3 | 14.02 ± 2.83 | 14.35 ± 3.31 | 13.87 ± 2.71 | 0.554 |
| D4 | 12.66 ± 2.34 | 12.50 ± 2.76 | 12.63 ± 2.20 | 0.706 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Guarda, C.C.; de Carvalho Silva, J.E.; Melo, G.I.V.; Santana, P.V.B.; Pacheco, J.A.; Correa, B.T.; Santos, E.d.C.; Adorno, E.V.; Spier, A.; Fonseca, T.C.C.; et al. WHOQOL-BREF in Measuring Quality of Life Among Sickle Cell Disease Patients with Leg Ulcers. Int. J. Environ. Res. Public Health 2025, 22, 108. https://doi.org/10.3390/ijerph22010108
da Guarda CC, de Carvalho Silva JE, Melo GIV, Santana PVB, Pacheco JA, Correa BT, Santos EdC, Adorno EV, Spier A, Fonseca TCC, et al. WHOQOL-BREF in Measuring Quality of Life Among Sickle Cell Disease Patients with Leg Ulcers. International Journal of Environmental Research and Public Health. 2025; 22(1):108. https://doi.org/10.3390/ijerph22010108
Chicago/Turabian Styleda Guarda, Caroline Conceição, Jéssica Eutímio de Carvalho Silva, Gabriela Imbassahy Valentim Melo, Paulo Vinícius Bispo Santana, Juliana Almeida Pacheco, Bruno Terra Correa, Edvan do Carmo Santos, Elisângela Vitória Adorno, Andrea Spier, Teresa Cristina Cardoso Fonseca, and et al. 2025. "WHOQOL-BREF in Measuring Quality of Life Among Sickle Cell Disease Patients with Leg Ulcers" International Journal of Environmental Research and Public Health 22, no. 1: 108. https://doi.org/10.3390/ijerph22010108
APA Styleda Guarda, C. C., de Carvalho Silva, J. E., Melo, G. I. V., Santana, P. V. B., Pacheco, J. A., Correa, B. T., Santos, E. d. C., Adorno, E. V., Spier, A., Fonseca, T. C. C., Goncalves, M. S., & Aleluia, M. M. (2025). WHOQOL-BREF in Measuring Quality of Life Among Sickle Cell Disease Patients with Leg Ulcers. International Journal of Environmental Research and Public Health, 22(1), 108. https://doi.org/10.3390/ijerph22010108