
Anorexia Nervosa, Body Image Perception and Virtual Reality Therapeutic Applications: State of the Art and Operational Proposal

 ,
,  ,
,  , ,
, ,  , and
, and 
Abstract
:1. Introduction
- −
- To review the literature on BI disturbances and VR clinical applications related to patients with AN;
- −
- To propose a new tool and a new application of VR, AN population therapy oriented, related to BI overestimation and dissatisfaction.
2. Materials and Methods
2.1. Search Strategy
2.2. Criteria for Eligibility
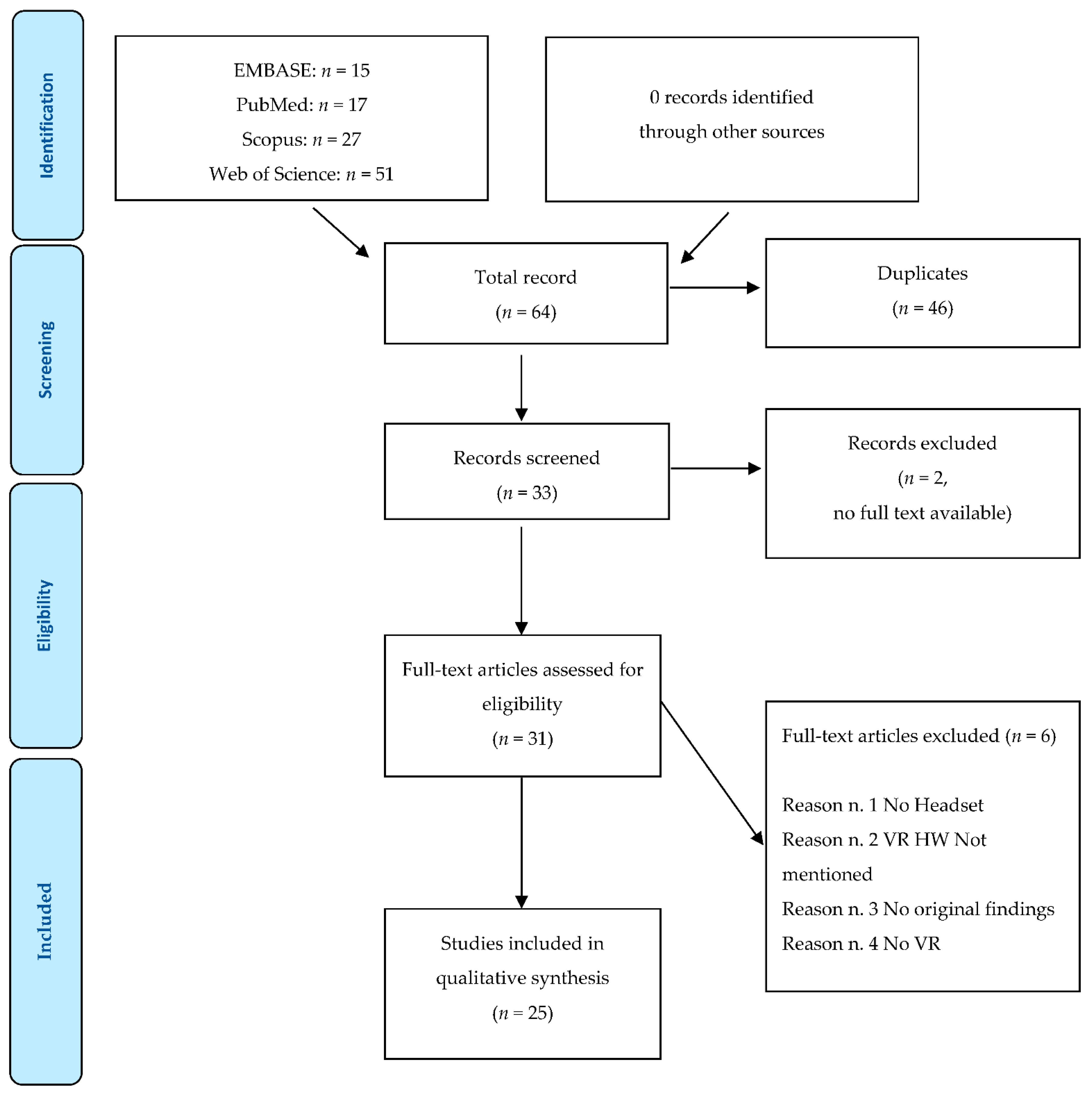
2.3. Study Selection
2.4. Data Extraction
2.5. Virtual Reality Conceptual Dimensions and Applications to Body Image
3. Results
3.1. Search Results and Study Characteristics
- Generic studies
- Editorials
- Studies without original findings
- Studies where there were no VR tools
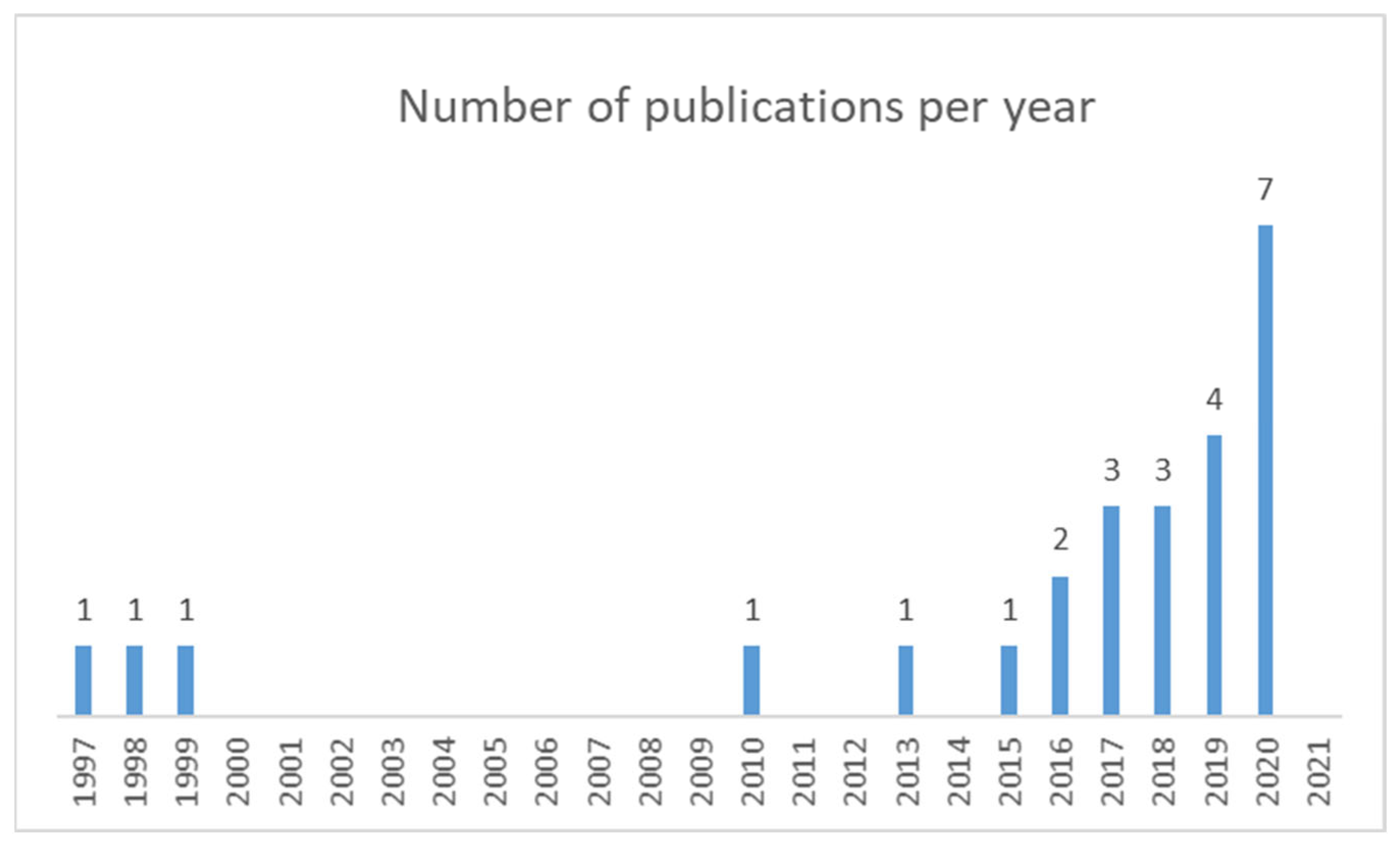
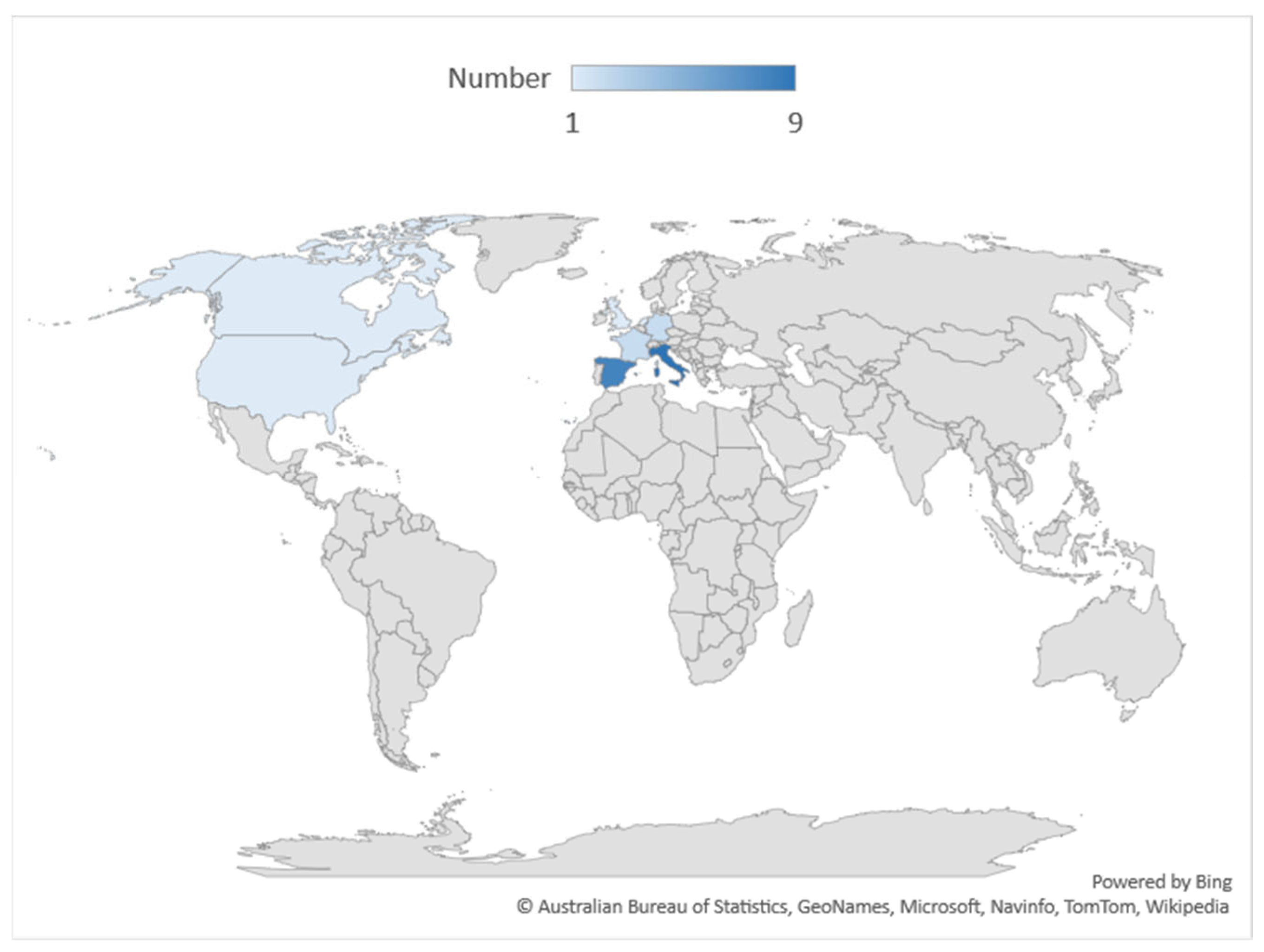
3.2. Geographical and Timeline Distribution
3.3. Study Design and Population
3.4. Avatar and Multisensory Integration: Stimulus Generation, Technical and Emotional Setup
3.5. Intervention Evaluation Studies
3.6. The VR Technologies
3.7. Technical Details on the Hardware/Software Used
3.7.1. VR Headset
3.7.2. Other Hardware/Software (HW/SW) Devices
4. Discussion
5. Implications/Proposal
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Clus, D.; Larsen, M.E.; Lemey, C.; Berrouiguet, S. The Use of Virtual Reality in Patients with Eating Disorders: Systematic Review. J. Med. Internet Res. 2018, 20, e157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan, T.F.; Hasan, H. Anorexia Nervosa: A Unified Neurological Perspective. Int. J. Med. Sci. 2011, 8, 679–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treasure, J.; Claudino, A.M.; Zucker, N. Eating Disorders. Lancet Lond. Engl. 2010, 375, 583–593. [Google Scholar] [CrossRef]
- Gillberg, I.C.; Gillberg, C.; Råstam, M.; Johansson, M. The Cognitive Profile of Anorexia Nervosa: A Comparative Study Including a Community-Based Sample. Compr. Psychiatry 1996, 37, 23–30. [Google Scholar] [CrossRef]
- Kingston, K.; Szmukler, G.; Andrewes, D.; Tress, B.; Desmond, P. Neuropsychological and Structural Brain Changes in Anorexia Nervosa before and after Refeeding. Psychol. Med. 1996, 26, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Gillberg, I.C.; Billstedt, E.; Wentz, E.; Anckarsäter, H.; Råstam, M.; Gillberg, C. Attention, Executive Functions, and Mentalizing in Anorexia Nervosa Eighteen Years after Onset of Eating Disorder. J. Clin. Exp. Neuropsychol. 2010, 32, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Russell, T.A.; Schmidt, U.; Doherty, L.; Young, V.; Tchanturia, K. Aspects of Social Cognition in Anorexia Nervosa: Affective and Cognitive Theory of Mind. Psychiatry Res. 2009, 168, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Tchanturia, K.; Anderluh, M.B.; Morris, R.G.; Rabe-Hesketh, S.; Collier, D.A.; Sanchez, P.; Treasure, J.L. Cognitive Flexibility in Anorexia Nervosa and Bulimia Nervosa. J. Int. Neuropsychol. Soc. 2004, 10, 513–520. [Google Scholar] [CrossRef]
- Lopez, C.; Tchanturia, K.; Stahl, D.; Treasure, J. Weak Central Coherence in Eating Disorders: A Step towards Looking for an Endophenotype of Eating Disorders. J. Clin. Exp. Neuropsychol. 2009, 31, 117–125. [Google Scholar] [CrossRef]
- Roberts, M.E.; Tchanturia, K.; Stahl, D.; Southgate, L.; Treasure, J. A Systematic Review and Meta-Analysis of Set-Shifting Ability in Eating Disorders. Psychol. Med. 2007, 37, 1075–1084. [Google Scholar] [CrossRef] [Green Version]
- Zastrow, A.; Kaiser, S.; Stippich, C.; Walther, S.; Herzog, W.; Tchanturia, K.; Belger, A.; Weisbrod, M.; Treasure, J.; Friederich, H.-C. Neural Correlates of Impaired Cognitive-Behavioral Flexibility in Anorexia Nervosa. Am. J. Psychiatry 2009, 166, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Lopez, C.; Tchanturia, K.; Stahl, D.; Treasure, J. Central Coherence in Eating Disorders: A Systematic Review. Psychol. Med. 2008, 38, 1393–1404. [Google Scholar] [CrossRef] [PubMed]
- Lena, S.M.; Fiocco, A.J.; Leyenaar, J.K. The Role of Cognitive Deficits in the Development of Eating Disorders. Neuropsychol. Rev. 2004, 14, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Kaye, W.H.; Bastiani, A.M.; Moss, H. Cognitive Style of Patients with Anorexia Nervosa and Bulimia Nervosa. Int. J. Eat. Disord. 1995, 18, 287–290. [Google Scholar] [CrossRef]
- Curzio, O.; Bastiani, L.; Scalese, M.; Cutrupi, V.; Romano, E.; Denoth, F.; Maestro, S.; Muratori, F.; Molinaro, S. Developing Anorexia Nervosa in Adolescence: The Role of Self-Image as a Risk Factor in a Prevalence Study. Adv. Eat. Disord. 2015, 3, 63–75. [Google Scholar] [CrossRef]
- Ziser, K.; Mölbert, S.C.; Stuber, F.; Giel, K.E.; Zipfel, S.; Junne, F. Effectiveness of Body Image Directed Interventions in Patients with Anorexia Nervosa: A Systematic Review. Int. J. Eat. Disord. 2018, 51, 1121–1127. [Google Scholar] [CrossRef]
- Butler, R.M.; Heimberg, R.G. Exposure Therapy for Eating Disorders: A Systematic Review. Clin. Psychol. Rev. 2020, 78, 101851. [Google Scholar] [CrossRef]
- Curzio, O.; Maestro, S.; Rossi, G.; Calderoni, S.; Giombini, L.; Scardigli, S.; Ragione, L.D.; Muratori, F. Transdiagnostic vs. Disorder-Focused Perspective in Children and Adolescents with Eating Disorders: Findings from a Large Multisite Exploratory Study. Eur. Psychiatry 2018, 49, 81–93. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association, Ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1. [Google Scholar]
- Ambrosecchia, M.; Ardizzi, M.; Russo, E.; Ditaranto, F.; Speciale, M.; Vinai, P.; Todisco, P.; Maestro, S.; Gallese, V. Interoception and Autonomic Correlates during Social Interactions. Implications for Anorexia. Front. Hum. Neurosci. 2017, 11, 219. [Google Scholar] [CrossRef] [Green Version]
- Curzio, O.; Calderoni, S.; Maestro, S.; Rossi, G.; De Pasquale, C.F.; Belmonti, V.; Apicella, F.; Muratori, F.; Retico, A. Lower Gray Matter Volumes of Frontal Lobes and Insula in Adolescents with Anorexia Nervosa Restricting Type: Findings from a Brain Morphometry Study. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2020, 63, e27. [Google Scholar] [CrossRef]
- Riva, G.; Malighetti, C.; Serino, S. Virtual Reality in the Treatment of Eating Disorders. Clin. Psychol. Psychother. 2021, 28, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Gaudio, S. Allocentric Lock in Anorexia Nervosa: New Evidences from Neuroimaging Studies. Med. Hypotheses 2012, 79, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Dakanalis, A.; Manzoni, G.M.; Castelnuovo, G.; Riva, G.; Clerici, M. Towards Novel Paradigms for Treating Dysfunctional Bodily Experience in Eating Disorders. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2017, 22, 373–375. [Google Scholar] [CrossRef]
- De Coster, L.; Sánchez-Herrero, P.; Aliaga, C.; Otaduy, M.A.; López-Moreno, J.; Tajadura-Jiménez, A. Perceived Match between Own and Observed Models’ Bodies: Influence of Face, Viewpoints, and Body Size. Sci. Rep. 2020, 10, 13991. [Google Scholar] [CrossRef] [PubMed]
- Botvinick, M.; Cohen, J. Rubber Hands “feel” Touch That Eyes See. Nature 1998, 391, 756. [Google Scholar] [CrossRef] [PubMed]
- Costantini, M. Body Perception, Awareness, and Illusions. Wiley Interdiscip. Rev. Cogn. Sci. 2014, 5, 551–560. [Google Scholar] [CrossRef]
- Normand, J.-M.; Giannopoulos, E.; Spanlang, B.; Slater, M. Multisensory Stimulation Can Induce an Illusion of Larger Belly Size in Immersive Virtual Reality. PLoS ONE 2011, 6, e16128. [Google Scholar] [CrossRef] [Green Version]
- Serino, S.; Pedroli, E.; Keizer, A.; Triberti, S.; Dakanalis, A.; Pallavicini, F.; Chirico, A.; Riva, G. Virtual Reality Body Swapping: A Tool for Modifying the Allocentric Memory of the Body. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 127–133. [Google Scholar] [CrossRef]
- Kilteni, K.; Maselli, A.; Kording, K.P.; Slater, M. Over My Fake Body: Body Ownership Illusions for Studying the Multisensory Basis of Own-Body Perception. Front. Hum. Neurosci. 2015, 9, 141. [Google Scholar] [CrossRef]
- Gaudio, S.; Brooks, S.J.; Riva, G. Nonvisual Multisensory Impairment of Body Perception in Anorexia Nervosa: A Systematic Review of Neuropsychological Studies. PLoS ONE 2014, 9, e110087. [Google Scholar] [CrossRef]
- Keizer, A.; van Elburg, A.; Helms, R.; Dijkerman, H.C. A Virtual Reality Full Body Illusion Improves Body Image Disturbance in Anorexia Nervosa. PLoS ONE 2016, 11, e0163921. [Google Scholar] [CrossRef]
- Repetto, C.; Gorini, A.; Vigna, C.; Algeri, D.; Pallavicini, F.; Riva, G. The Use of Biofeedback in Clinical Virtual Reality: The INTREPID Project. J. Vis. Exp. 2009, 33, e1554. [Google Scholar] [CrossRef] [Green Version]
- Pop-Jordanova, N. Psychological Characteristics and Biofeedback Mitigation in Preadolescents with Eating Disorders. Pediatr. Int. 2000, 42, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Pop-Jordanova, N.; Zorcec, T.; Demerdzieva, A. Anorexia: Anormal Phobia of Normal Weight. PRILOZI 2017, 38, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riva, G.; Dakanalis, A. Altered Processing and Integration of Multisensory Bodily Representations and Signals in Eating Disorders: A Possible Path Toward the Understanding of Their Underlying Causes. Front. Hum. Neurosci. 2018, 12, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological Quality and Synthesis of Case Series and Case Reports. BMJ Evid.-Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Serino, S.; Dakanalis, A.; Gaudio, S.; Carrà, G.; Cipresso, P.; Clerici, M.; Riva, G. Out of Body, out of Space: Impaired Reference Frame Processing in Eating Disorders. Psychiatry Res. 2015, 230, 732–734. [Google Scholar] [CrossRef]
- Marco, J.H.; Perpiñá, C.; Botella, C. Effectiveness of Cognitive Behavioral Therapy Supported by Virtual Reality in the Treatment of Body Image in Eating Disorders: One Year Follow-Up. Psychiatry Res. 2013, 209, 619–625. [Google Scholar] [CrossRef]
- Provenzano, L.; Porciello, G.; Ciccarone, S.; Lenggenhager, B.; Tieri, G.; Marucci, M.; Dazzi, F.; Loriedo, C.; Bufalari, I. Characterizing Body Image Distortion and Bodily Self-Plasticity in Anorexia Nervosa via Visuo-Tactile Stimulation in Virtual Reality. J. Clin. Med. 2019, 9, 98. [Google Scholar] [CrossRef] [Green Version]
- Mölbert, S.C.; Thaler, A.; Mohler, B.J.; Streuber, S.; Romero, J.; Black, M.J.; Zipfel, S.; Karnath, H.-O.; Giel, K.E. Assessing Body Image in Anorexia Nervosa Using Biometric Self-Avatars in Virtual Reality: Attitudinal Components Rather than Visual Body Size Estimation Are Distorted. Psychol. Med. 2018, 48, 642–653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubo, M.; Gamer, M. Visuo-Tactile Congruency Influences the Body Schema during Full Body Ownership Illusion. Conscious. Cogn. 2019, 73, 102758. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, S.; Malighetti, C.; Serino, S.; Riva, G.; Winter, D. Intrapersonal, Interpersonal, and Physical Space in Anorexia Nervosa: A Virtual Reality and Repertory Grid Investigation. Psychiatry Res. 2017, 252, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Malighetti, C.; Serino, S.; Riva, G.; Cipolletta, S. Inside and Outside the Self. Virtual Reality and Repertory Grids in the Spatial Analysis of Anorexic Patients’ Meanings. Annu. Rev. Ciber Ther. Telemed. 2016, 14, 78–83. [Google Scholar]
- Porras-Garcia, B.; Serrano-Troncoso, E.; Carulla-Roig, M.; Soto-Usera, P.; Ferrer-Garcia, M.; Figueras-Puigderrajols, N.; Yilmaz, L.; Onur Sen, Y.; Shojaeian, N.; Gutiérrez-Maldonado, J. Virtual Reality Body Exposure Therapy for Anorexia Nervosa. A Case Report With Follow-Up Results. Front. Psychol. 2020, 11, 956. [Google Scholar] [CrossRef] [PubMed]
- Serino, S.; Polli, N.; Riva, G. From Avatars to Body Swapping: The Use of Virtual Reality for Assessing and Treating Body-size Distortion in Individuals with Anorexia. J. Clin. Psychol. 2019, 75, 313–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Maldonado, J.; Ferrer-García, M.; Caqueo-Urízar, A.; Moreno, E. Body Image in Eating Disorders: The Influence of Exposure to Virtual-Reality Environments. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 521–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riva, G.; Bacchetta, M.; Baruffi, M.; Rinaldi, S.; Molinari, E. Experiential Cognitive Therapy in Anorexia Nervosa. Eat. Weight Disord. EWD 1998, 3, 141–150. [Google Scholar] [CrossRef]
- Riva, G.; Bacchetta, M.; Baruffi, M.; Rinaldi, S.; Molinari, E. Virtual Reality Based Experiential Cognitive Treatment of Anorexia Nervosa. J. Behav. Ther. Exp. Psychiatry 1999, 30, 221–230. [Google Scholar] [CrossRef]
- Irvine, K.R.; Irvine, A.R.; Maalin, N.; McCarty, K.; Cornelissen, K.K.; Tovée, M.J.; Cornelissen, P.L. Using Immersive Virtual Reality to Modify Body Image. Body Image 2020, 33, 232–243. [Google Scholar] [CrossRef]
- Porras-Garcia, B.; Ferrer-Garcia, M.; Ghita, A.; Moreno, M.; López-Jiménez, L.; Vallvé-Romeu, A.; Serrano-Troncoso, E.; Gutiérrez-Maldonado, J. The Influence of Gender and Body Dissatisfaction on Body-related Attentional Bias: An Eye-tracking and Virtual Reality Study. Int. J. Eat. Disord. 2019, 52, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Neyret, S.; Bellido Rivas, A.I.; Navarro, X.; Slater, M. Which Body Would You Like to Have? The Impact of Embodied Perspective on Body Perception and Body Evaluation in Immersive Virtual Reality. Front. Robot. AI 2020, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Fisher, S.; Abdullah, A.; Charvin, I.; Da Fonseca, D.; Bat-Pitault, F. Comparison of Body Image Evaluation by Virtual Reality and Paper-Based Figure Rating Scales in Adolescents with Anorexia Nervosa: Retrospective Study. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2020, 25, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Hudson, G.M.; Lu, Y.; Zhang, X.; Hahn, J.; Zabal, J.E.; Latif, F.; Philbeck, J. The Development of a BMI-Guided Shape Morphing Technique and the Effects of an Individualized Figure Rating Scale on Self-Perception of Body Size. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 579–594. [Google Scholar] [CrossRef] [Green Version]
- Fonseca-Baeza, S.; Corno, G.; Baños, R.M. An Intervention Protocol Proposal to Modify the Body Image Disturbance Using Virtual Reality. Calid. Vida Salud 2018, 11, 48–61. [Google Scholar]
- Corno, G.; Serino, S.; Cipresso, P.; Baños, R.M.; Riva, G. Assessing the Relationship Between Attitudinal and Perceptual Component of Body Image Disturbance Using Virtual Reality. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 679–686. [Google Scholar] [CrossRef]
- Buche, C.; Bigot, N.L. REVAM: A Virtual Reality Application for Inducing Body Size Perception Modifications. In Proceedings of the 2018 International Conference on Cyberworlds (CW), Singapore, 3–5 October 2018; pp. 229–236. [Google Scholar]
- Ferrer-Garcia, M.; Porras-Garcia, B.; González-Ibañez, C.; Gracia-Blanes, M.; Vilalta-Abella, F.; Plasanjuanelo, J.; Riva, G.; Dakanalis, A.; Achoteguil-Oizate, J.; Talarn-Caparró, A.S.; et al. Does Owning a “Fatter” Virtual Body Increase Body Anxiety in College Students? Annu. Rev. Ciber Ther. Telemed. 2017, 15, 147–153. [Google Scholar]
- Serino, S.; Dakanalis, A. Bodily Illusions and Weight-Related Disorders: Clinical Insights from Experimental Research. Ann. Phys. Rehabil. Med. 2017, 60, 217–219. [Google Scholar] [CrossRef]
- Porras-Garcia, B.; Ferrer-García, M.; Serrano-Troncoso, E.; Carulla-Roig, M.; Soto-Usera, P.; Fernández-Del Castillo Olivares, L.; Figueras-Puigderajols, N.; Gutiérrez-Maldonado, J. Virtual reality body exposure therapy for anorexia nervosa. A single case study. In HCI International 2020—Posters; Communications in Computer and Information Science; Stephanidis, C., Antona, M., Eds.; Springer International Publishing: Cham, Switzerland, 2020; Volume 1225, pp. 108–115. ISBN 978-3-030-50728-2. [Google Scholar]
- Armel, K.C.; Ramachandran, V.S. Projecting Sensations to External Objects: Evidence from Skin Conductance Response. Proc. R. Soc. Lond. B Biol. Sci. 2003, 270, 1499–1506. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Vives, M.V.; Spanlang, B.; Frisoli, A.; Bergamasco, M.; Slater, M. Virtual Hand Illusion Induced by Visuomotor Correlations. PLoS ONE 2010, 5, e10381. [Google Scholar] [CrossRef] [Green Version]
- Salagean, A.; Hadnett-Hunter, J.; Finnegan, D.J.; De Sousa, A.A.; Proulx, M.J. A Virtual Reality Application of the Rubber Hand Illusion Induced by Ultrasonic Mid-Air Haptic Stimulation. ACM Trans. Appl. Percept. 2022, 19, 1–19. [Google Scholar] [CrossRef]
- Denis, P. Methodology of Biofeedback. Eur. J. Gastroenterol. Hepatol. 1996, 8, 530–533. [Google Scholar] [CrossRef] [PubMed]
- McCleary, R.A. The Nature of the Galvanic Skin Response. Psychol. Bull. 1950, 47, 97–117. [Google Scholar] [CrossRef]
- Sharma, M.; Kacker, S.; Sharma, M. A Brief Introduction and Review on Galvanic Skin Response. Int. J. Med. Res. Prof. 2016, 2, 13–17. [Google Scholar] [CrossRef]
- Brown, T.; Nauman Vogel, E.; Adler, S.; Bohon, C.; Bullock, K.; Nameth, K.; Riva, G.; Safer, D.L.; Runfola, C.D. Bringing Virtual Reality From Clinical Trials to Clinical Practice for the Treatment of Eating Disorders: An Example Using Virtual Reality Cue Exposure Therapy. J. Med. Internet Res. 2020, 22, e16386. [Google Scholar] [CrossRef]
- Gregg, L.; Tarrier, N. Virtual Reality in Mental Health: A Review of the Literature. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 343–354. [Google Scholar] [CrossRef]
- Rebenitsch, L.; Owen, C. Review on Cybersickness in Applications and Visual Displays. Virtual Real. 2016, 20, 101–125. [Google Scholar] [CrossRef]
- Gutiérrez-Maldonado, J.; Ferrer-García, M.; Dakanalis, A.; Riva, G. Virtual Reality; Agras, W.S., Robinson, A., Eds.; Oxford University Press: Oxford, UK, 2017; Volume 1. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year, Institution, Title, Journal | Population | Method | VR, Hardware and Software (HW/SW), Tools and View | Objective | Results | Quality Score |
|---|---|---|---|---|---|---|
| Irvine–2020 Department of Psychology, Faculty of Health and Life Sciences, Northumbria University, Newcastle upon Tyne, UK Using Immersive Virtual Reality to Modify Body Image Body Image Journal | 60 female volunteers with high body image concerns. | The participants, divided into two groups, completed a 4-day program, in which they classified a series of 3D models as thin or fat; stimuli were presented to one group briefly, while no time limits were imposed on the other group. Both intervention groups received inflationary feedback to shift their model ratings towards higher BMIs. | VR HW tool: Oculus Rift. Additional HW, notes on SW: Unreal Engine. View: TPV. | Intervening on the perceptual boundary of the classification of a fat body versus a lean body with the use of a VR application. | Both intervention groups experienced statistically significant reductions in their concerns about their body shape, weight, and eating habits. These reductions had clinically significant effects in the group with longer stimulus presentation times. | 9/9 |
| Neyret–2020 Event Lab, Department of Clinical Psychology and Psychobiology, University of Barcelona, Barcelona, Spain. Which Body Would You Like to Have? The Impact of Embodied Perspective on Body Perception and Body Evaluation in Immersive Virtual Reality Frontiers in Robotics and AI Journal | Female participants | Participants’ bodies are scanned and generated as avatars. For each body, two more are generated by increasing or decreasing their size. After that, the participants must choose which is their body among the three proposed, both an FPV and TPV mode. | VR HW tool: nVision SX11. Additional HW, notes on SW: Optitrack Motion capture System (a Velcro suit with 28 reflective markers tracked by 12 infrared cameras); tactile feedback through four vibrators controlled by an Arduino board. View: FPV & TPV. | Measure the internal conscious representation of one’s body aspect, comparing it with one’s ideal body aspect and with the real aspect. | Female participants rated their real body as more attractive when they viewed it from a third-person perspective. Their level of dissatisfaction with the body decreased after the experimental procedure. It is hypothesized that the third-person perspective allowed them to perceive their real body shape without applying the previous negative beliefs associated with the self. | 9/9 |
| Provenzano–2020 Department of Psychology, “Sapienza” University of Rome, 00185 Rome, Italy and IRCCS, Santa Lucia Foundation, 00142 Rome, Italy Characterizing Body Image Distortion and Bodily Self-Plasticity in Anorexia Nervosa via Visuo-Tactile Stimulation in Virtual Reality Journal of Clinical Medicine | 20 anorexics, 20 healthy controls. | For each participant, customized avatars were created, one reproducing their real body size, and two others with increased and decreased weight. Body overestimation and dissatisfaction were measured by asking participants to choose the avatar, presented in FPV, they felt most closely resembled their own body. The activity is completed by a synchronous and asynchronous stimulation with the three versions of the avatar. | VR HW tool: Oculus Rift Developers Kit Dk1. Additional HW, notes on SW: Makehuman (for character creation), Photoshop 7 for skin and dresses, 3dsMax for generation of an avatar with different weights starting from the ones created with Makehuman. View: FPV. | Combining virtual reality and multisensory body illusion to characterize and reduce body overestimation and body dissatisfaction. | Upper body dissatisfaction was found in subjects with AN. The embodiment was stronger with synchronous stimulation in both groups but still did not reduce BI disorder in participants with AN. Subjects with AN reported more negative emotions after embodying the fatter avatar. The cognitive-emotional component, rather than perceptive, of the BID, was severely altered in AN. | 9/9 |
| Porras-Garcia–2020 Department of Clinical Psychology and Psychobiology, University of Barcelona, Barcelona, Spain Virtual Reality Body Exposure Therapy for Anorexia Nervosa. A Case Report with Follow-Up Results Frontiers in Psychology | A case study with a patient diagnosed with AN. | The activity included 5 VR therapy sessions. The sessions included exposure in TPV of the patient to a virtual representation of his own body, with the body mass index of the avatar progressively increasing. The virtual environment consists of a room with a large mirror capable of reflecting the image of the body. During the sessions, the participants received synchronous visual-motor and visual-tactile stimulation. Fear of gaining weight (FGW), body anxiety, thinness drive, body image disturbances, body mass index, and attention bias were assessed before and after treatment, as well as 5 months after. | VR HW tool: HTC-VIVE. Additional HW, notes on SW: VR HMD FOVE Eye Tracking to detect and register eye movements, Unity 3D and Blender for avatar creation. View: FPV. | This study aimed to provide preliminary evidence of the usefulness of VR body exposure therapy. | After the treatment, there was a reduction in typical AN symptoms such as FGW, thinness drive, body-related anxiety, and dissatisfaction. There was a noticeable change in body-related dysfunctional attention bias. Thanks to the intervention, the values of the body mass index have increased and reached healthy levels. Most of all these improvements were maintained after 5 months. | 8/8 |
| Porras-Garcia–2020 Department of Clinical Psychology and Psychobiology, University of Barcelona, Barcelona, Spain Virtual Reality Body Exposure Therapy for Anorexia Nervosa. A Single Case Study In: Stephanidis C., Antona M. (eds) HCI International 2020–Posters. HCII 2020. Communications in Computer and Information Science | A case study on a 14-year-old female adolescent with AN. | A virtual representation of the patient’s body was reconstructed, whose weight was progressively increased in 5 sessions. The avatar was displayed to the patient in a simple VR setting. FGW, Body Anxiety, and Full Body Illusion (FBI) were assessed at the start of each session. Fear of gaining weight (FGW), body anxiety, thinness drive, body image disorder (BID), and body mass index (BMI) were assessed before, after treatment, and 3 months after follow-up. -up of 3 months. | VR HW tool: HTC-VIVE. Additional HW, notes on SW: VR HMD FOVE Eye Tracking to detect and register eye movements, Unity 3D and Blender for avatar creation. View: FPV. | Traditional exposure-based therapies have significant limitations (for example, the negative initial reaction in patients or increased risk of abandonment). The use of VR-based exposure techniques can overcome these limitations. | After the treatment they decreased in FGW, push to thinness, body-related anxiety, and BID. BMI slightly increased throughout the surgery. FBI levels also increased progressively with each exposure session. However, these changes were not fully maintained at follow-up. | 8/8 |
| Fisher–2020 Child and Adolescent Psychopathology Unit, Salvator University Hospital, Public Assistance-Marseille Hospitals, Aix-Marseille University, 249 Boulevard Sainte-Marguerite, 13009 Marseille, France Comparison of body image evaluation by virtual reality and paper-based figure rating scales in adolescents with anorexia nervosa: retrospective study Eating and Weight Disorders–Studies on Anorexia, Bulimia and Obesity Journal | 31 female adolescents with AN. | Ten 3D avatars are created, with different builds, arranged in a circle. The participant observes the scene in VR while the observation time of each of the avatars is measured. Next, the participant has to choose the avatar that best matches their current image and the avatar that matches their desired shape. Paired data of perceived and desired body shapes were compared as well as body perception index (BPI) (p = 0.2) and body dissatisfaction (p = 0.6). The correlation of the data found with validated psychometric questionnaires was measured. | VR HW tool: Oculus Rift. Additional HW, notes on SW: C2CARE PSY (application realized with Unity). View: TPV. | The objective of the study is to demonstrate that VR systems with standardized avatars would improve the perception of the body image and therefore the evaluation of the body image by subjects with AN, compared to the evaluation scales of the figures on paper (FRS). | Participants with AN overestimated their body size regardless of the assessment tool used. BPI and body dissatisfaction did not differ significantly between FRS and VR. The results of the BID evaluation by VR standardized 3D avatars are comparable to those obtained by paper FRS. | 7/8 |
| Hudson–2020 Department of Health, Kinesiology and Sport, University of South Alabama, USA The Development of a BMI-Guided Shape Morphing Technique and the Effects of an Individualized Figure Rating Scale on Self-Perception of Body Size European Journal of Investigation in Health Psychology and Education | Young adult women | A corresponding avatar was created for each subject, along with 3 others with slightly different apparent weights. The avatars were then shown, in a 2D and 3D version, in a VR setting in TPV mode. | VR HW tool: Oculus Rift. Additional HW, notes on SW: Two Microsoft Kinect v2 for body scanning. View: TPV. | The study aimed to assess the effects of an Individualized Figure Rating Scale on Self-Perception of Body Size | Assessments of body perception using generalized line drawings (2D) were often superior to responses using individualized visualization methods. The realism of representation, therefore, does not seem to be of much importance, except in helping to identify. Using scales based on custom textures and limb sizes seems beneficial, but immersive VR presentation may not be essential. | 7/9 |
| Mölbert–2019 Department of Psychosomatic Medicine and Psychotherapy, Medical University Hospital Tübingen, Germany. Assessing Body Image in Anorexia Nervosa Using Biometric Self-Avatars in Virtual Reality: Attitudinal Components Rather than Visual Body Size Estimation Are Distorted Psychological Medicine | 24 women with AN and n = 24 controls. | Realistic avatars were created for each participant based on a 3D scan. The apparent weight of the avatars was then varied within a range of ±20%. The avatars were then presented to the subjects in a mirror-like scenario, in virtual reality. | VR HW tool: Not specified. Additional HW, notes on SW: 3D scan for avatar generation. View: FPV. | The study, using AR technologies, aimed to separate the perceptual and attitudinal components of the BID into AN. | Women with AN underestimated their weight more than controls. The target mean bodyweight of the controls had normal weight while the target mean weight of the women with AN corresponded to the extreme AN (DSM-5). Desired body weight was found to be associated with eating disorder symptoms. | 9/9 |
| Rubo and Gamer–2019 Marcusstr. 9–11, D-97080 Wuerzburg, Germany Visuo-Tactile Congruency Influences the Body Schema during Full Body Ownership Illusion Consciousness and Cognition | 24 women with AN diagnosed according to DSM-5 and n = 24 age and gender-matched normal weight control. | A corresponding avatar has been created for each subject. The apparent weight of the avatar has therefore been slightly increased. After the calibration phase, the participant observes himself through a VR mirror and has to perform simple tasks such as touching his hips and stomach and walking around a table. | VR HW tool: HTC Vive. Additional HW, notes on SW: TPCAST Wireless Adapter instead of a standard cable to allow participants to move more freely. Unity 3D. Unity Humanoid AdjustProportion and Unity Vertex Displacements (two in-house software to adjust human body proportions and to apply distortion to the Euclidean space of the virtual scene. View: FPV&TPV. | The aim was to assess if visuotactile congruency influences the body schema during VR-based full body ownership illusion. | Participants who took possession of a more corpulent virtual body with visual-tactile congruence set at the normal level increased safety distances to the laboratory walls compared to participants who experienced the same illusion with limited visual-tactile congruence. | 9/9 |
| Porras-Garcia–2019 Department of Clinical Psychology and Psychobiology, University of Barcelona, Barcelona, Spain The Influence of Gender and Body Dissatisfaction on body-related Attentional Bias: An Eye-Tracking and Virtual Reality Study International Journal of Eating Disorders | Forty-five women (23 with high BD and 22 with low BD) and 40 men (20 with high BD and 20 with low BD). | Participants were represented in three virtual avatars, the first based on the participant’s actual measurements, the second larger than the participant, and the third with an apparent weight similar to the first avatar. The number of fixations and full fixation time on weight-related areas of interest (W-AOI) and no weight-related areas of interest (NW-AOI) were recorded for the three assessment times/avatars. | VR HW tool: HTC-VIVE. Additional HW, notes on SW: VR HMD FOVE Eye Tracking to detect and register eye movements, Unity 3D and Blender for avatar creation. View: TPV | The aim was to assess gender differences in attentional bias (AB) towards weight-related and non-weight-related body parts, using virtual reality and eye-tracking techniques. | The results showed an interaction between sex, total time, and several fixations. BD levels did not significantly affect the results. Overall, women paid more attention to weight-related areas of interest (W-AOI) than men. Additionally, preliminary evidence was found for increased attention to muscle-related areas of the body in male subjects. | 9/9 |
| Serino–2019 IRCCS Istituto Auxologico Italiano-Catholic University of the Sacred Heart From Avatars to Body Swapping: The Use of Virtual Reality for Assessing and Treating Body-Size Distortion in Individuals with Anorexia Journal of Clinical Psychology | A patient with a diagnosis of AN (DSM-5) underwent intensive multidisciplinary outpatient treatment. | The protocol was composed of three sessions on the body-exchange paradigm in VR, obtained through synchronous and asynchronous visual-tactile stimulations. | VR HW tool: Oculus Rift SDK2. Additional HW, notes on SW: Makehuman to generate the avatar. Unity 3D to generate the virtual scene. View: FPV. | This case study aimed to use body illusion techniques in a VR protocol within a multidisciplinary treatment of AN. | The Full Body Illusion (FBI) in VR environment has proven effective in monitoring changes in multisensory body integration. The study also demonstrates how the FBI can help foster these changes. | 8/8 |
| Fonseca-Baeza–2018 Universitat de València, Valencia, España An Intervention Protocol Proposal to Modify the Body Image Disturbance Using Virtual Reality Calidad de Vida y Salud | A community sample of young women (18–35 years old), having a BMI between 18.5 and 24.99. | A standard female virtual body (with hidden hair and face) was developed for all participants, shown in VR in FPV and TPV modes. The avatar is initially proposed with an apparent BMI similar to that of the subject. The participant is then asked to change the avatar until the avatar’s abdomen matches her real abdomen. | VR HW tool: Oculus Rift. Additional HW, notes on SW: TANITA to measure the weight and analyze the body composition. Makehuman was used to generate the avatar. View: FPV and TPV. | The study aimed to present a study protocol of virtual reality (VR) multisensory paradigm to evaluate and treat BID. | This protocol appears to be an effective tool for developing a more realistic body representation of oneself. | 8/9 |
| Corno–2018 Université du Québec en Outaouais Gatineau, Québec, Canada Assessing the Relationship Between Attitudinal and Perceptual Component of Body Image Disturbance Using Virtual Reality Cyberpsychology Behavior and Social Networking | A sample of 27 community women. | Starting with a body with standard BMI, (presented in VR in both FPV and TPV modes) subjects must indicate how to modify it to make it look like their body. The women were able to choose from a wide range of three-dimensional bodies with a body mass index between 12.5 and 42.5 kg/m2. Standard indices such as body dissatisfaction, body discomfort, and avoidance of body image were assessed through questionnaires. | VR HW tool: Oculus Rift SDK2. Additional HW, notes on SW: Makehuman for avatar generation. Unity 3D for scene generation. Kinect V2 to detect participant movement. View: FPVandTPV. | This study aimed to explore the attitudinal and perceptual components of the BID using VR technologies. | The study showed that the attitudinal components predicted the BID only in the TPV mode. Overestimation was predicted by body image avoidance, while underestimation was predicted by body discomfort. Furthermore, a common predictor of underestimation and overestimation was body dissatisfaction. | 8/9 |
| Buche and Le Bigot–2018 LAB-STICC, ENIB and LAB-STICC, UBO REVAM: A Virtual Reality Application for Inducing Body Size Perception Modifications In Proceedings-2018 International Conference on Cyberworlds | 16 female participants. | The REVAM application proposes to couple a tactile stimulation while viewing a TPV avatar. In addition, the application offers the possibility to choose between avatars of different sizes and to morph between them. The experiment consists in estimating the affordance, in a basic situation and in another 4 in which visual-tactile stimulation is present. | VR HW tool: Oculus Rift Dk2. Additional HW, notes on SW: Kinect, Razer Hydra. View: TPV. | The study aims to propose a 3D virtual environment to induce the illusion of body ownership (whole body illusion). | It was noted that the average width of a door represented in VR, through which participants estimate they can pass with the avatar representing them, was significantly reduced when morphing was present. Simultaneous tactile stimulation does not appear to affect this result. The study speculates that exposing people to a smaller virtual body in this way could be an effective way to change the perception of body size, at least temporarily. | 8/9 |
| Serino–2017 IRCCS Istituto Auxologico Italiano-Catholic University of the Sacred Heart Two-phases innovative treatment for anorexia nervosa: The potential of virtual reality body-swap Annual Review of Cyber Therapy and Telemedicine | A group of23 female participants suffering from Anorexia Nervosa. | Participants observed in VR, in FPV mode, a virtual body with a lean belly representing their physical body in two experimental conditions: synchronous and asynchronous visual-tactile stimulation. | VR HW tool: Oculus Rift DK2. Additional HW, notes on SW: Razer Hydra Portal 2. View: FPV. | The goal is to investigate whether a treatment based on VR-based full-body illusion can induce variations in the representation of the body. | The study showed that the treatment can reduce the decrease in body distortions in the abdomen. This VR-based approach, if further developed, may be useful for anorexic patients to specifically improve body representation disorders. | 8/9 |
| Ferrer-Garcia–2017 Department of Clinical Psychology and Psychobiology, Universitat de Barcelona, Barcelona, Spain Does Owning a ‘Fatter’ Virtual Body Increase Body Anxiety in College Students? Annual Review of CyberTherapy and Telemedicine | 23 college students (5 male). | The subjects were exposed to an immersive VR environment in FPV and TPV modes. For each participant, an avatar with compatible apparent body measurements was reconstructed, plus two other avatars, respectively, one heavier by 20% and one lighter by 20%. Before exposure, BMI, drive to thinness (EDI 3-DT) and body dissatisfaction (EDI3-BD) were assessed. Body anxiety (PASTAS), fear of gaining weight, and delusion property (VAS 0 to 100) were assessed after exposure to each avatar. The illusion of ownership of a virtual body was induced through visual-motor synchronization. | VR HW tool: HTC-Vive. View: FPV and TPV. | Evaluate the ability of virtual reality (VR) based software to produce body anxiety responses in a non-clinical sample. | The study showed that the virtual body illusion with measurements larger than the subject’s causes body anxiety and fear of gaining weight in subjects with higher body dissatisfaction. BMI did not affect the results. | 8/9 |
| Cipolletta–2017 Department of General Psychology, University of Padua Intrapersonal, interpersonal, and physical space in anorexia nervosa: a virtual reality and repertory grid investigation Psychiatry Research | A sample of 12 AN patients and 12 HCs (controls) participated in the study. | The Eating Disorder Inventory (EDI), a procedure based on virtual reality, traditional measures of spatial skills, and repertoire grids were used in the protocol. | VR HW tool: -Additional HW, notes on SW: Logitech 940-000114 F510. NeuroVirtual 3D. View: FPV and TPV | This study, based on VR technologies, aimed to verify the differences between the spatial perception of patients with AN from healthy controls, and are these differences related to the severity of the anorexic symptoms. | The study showed that AN subjects showed significant impairments in spatial abilities, more unidimensional construing, and more extreme construing of the present self and the self as seen by others when compared to controls. | 9/9 |
| Keizer–2016 Experimental Psychology/Helmholtz Institute, Utrecht University, Utrecht, The Netherlands A Virtual Reality Full Body Illusion Improves Body Image Disturbance in Anorexia Nervosa Plos One | AN patient (n = 30) and HC group (n = 29). | Participants were asked to estimate their body size (shoulders, abdomen, hips) before Full Body Illusion (FBI) was induced, immediately after induction, and approximately 2 h and 45 min of follow-up. Full Body Illusion in VR was induced through synchronous visual-tactile stimulation. | VR HW tool: Oculus Rift DK2. Additional HW, notes on SW: Razer Hydra Portal 2. Unity 3D, MakeHuman. View: FPV | The study aimed to investigate whether a virtual reality-based full-body illusion affects the body size estimate of various body parts. | AN patient decreased the overestimation of their shoulders, abdomen, and hips directly after the FBI was induced. The effect was noted also in controls, although with a different pattern. | 9/9 |
| Malighetti–2016 Department of General Psychology, University of Padua Inside and outside the self. Virtual reality and repertory grids in the spatial analysis of anorexic patients’ meanings Annual Review of Cyber Therapy and Telemedicine | A sample composed of 12 AN patients and 12 healthy controls. | In a first task, the participants were asked to find a hidden object and memorize its position in a virtual city. After they have found the object, the second task participants were invited to retrieve the position of the object, which was absent, after entering the virtual city from another starting point. | VR HW tool: Oculus Rift DK2. Additional HW, notes on SW: Razer Hydra Portal 2. View: FPV. | The general objective of this study was to investigate, through a system based on VR technologies, the presence of deficits in the elaboration of the egocentric and allocentric frame of reference in AN patients. | The AN patient showed deficits in the spatial ability to retrieve and update a long-term memorized representation. It is hypothesized that the deficit in processing spatial information could be related to a distorted body representation. | 8/9 |
| Serino–2015 Applied Technology for Neuro-Psychology Lab, IRCCS Istituto Auxologico Italiano, Via Magnasco 2, 20149 Milan, Italy Out of Body, out of Space: Impaired Reference Frame Processing in Eating Disorders Psychiatry Research | Healthy controls/ED (eating disorder) patients | In a preliminary phase, the Corsi Block Test- Span and Supraspan (Corsi, 1972), and the Judgment of Line Orientation (Benton et al., 1978) were used to assess visuospatial abilities. Participants were then invited to retrieve the position of a hidden object they had discovered in the virtual city and memorized it on a real map (an aerial view of the virtual city) with a pen (allocentric view). In a second phase, they have to indicate the position of that object (which was absent) entering the virtual city from another starting point (egocentric view). | VR HW tool: Oculus Rift DK2. Additional HW, notes on SW: Razer Hydra Portal 2. View: FPV. | The aim was to investigate the relationship between ED and spatial abilities. | Employing a well-validated virtual reality-based procedure related to healthy controls, patients with eating disorders showed deficits in the ability to reference and update a long-term stored allocentric representation (TPV) with egocentric input (FPV). | 8/9 |
| Conxa Perpiñá and Botella–2013 San Vicente Mártir Catholic University of Valencia Effectiveness of Cognitive Behavioral Therapy Supported by Virtual Reality in the Treatment of Body Image in Eating Disorders: One Year Follow-Up Psychiatry Research | 34 participants diagnosed with eating disorders. | The treatment consisted of 15 sessions divided into 3 stages. The virtual environment consisted of 5 different areas. Area 1: Virtual scale and kitchen. Area 2: Photograph area, Here the patient’s tendency to compare themselves with other bodies is addressed. Area 3: Mirror room. The patient has to manipulate a 3D avatar until it matches a 2D image representing his/her real body. Area 4: a sort of adjustable door, the user has to set it so that he/her can pass through it. Area 5: several versions of one’s body are here presented. The is invited to compare them. | VR HW tool: Virtual Research V6. View: FPV/TPV. | Testing effectiveness of cognitive behavioral therapy supported by virtual reality. | Patients who received the described treatment improved their body image. The improvement was also maintained in the follow-up. | 8/9 |
| Maldonado–2010 Department of Personality, Assessment and Psychological Treatments, University of Barcelona, Barcelona, Spain Body Image in Eating Disorders: The Influence of Exposure to Virtual-Reality Environments Cyberpsychology Behavior And Social Networking | 85 ED patients and 108 non-ED students. | VEs to simulate real-life situations that were emotionally significant for ED patients, to produce or enhance body-image distortion and body-image dissatisfaction. The subjects have been exposed to high-calorie food, as well as situations in which their body is on display or in which they come into contact with other people. | VR HW tool: HTC-Vive. View: FPV and TPV. | The study aimed to evaluate the effect of virtual-reality exposure to situations that are emotionally significant for patients with eating disorders (ED) on the stability of body-image distortion and body-image dissatisfaction. | The study shows the presence of a distorted body image in patients compared to controls and highlights the fact that, in the patient group, these body images vary according to the emotional and social situation. | 8/9 |
| Riva–1999 Applied Technology for Neuro-Psychology Lab., Istituto Auxologico Italiano, Verbania, Italy. Virtual reality-based experiential cognitive treatment of anorexia nervosa Journal of Behavior Therapy and Experimental Psychiatry | Case study on a 22-year old female diagnosed with AN. | The study used experiential cognitive therapy (ECT), with the use of VR technologies. The treatment consisted of 5 sessions with the VEBIM virtual reality system. The first session was used to assess any stimuli that could elicit abnormal eating behaviour. The next four sessions were used to assess and modify: the symptoms of anxiety-related to food exposure and the body experience of the subject. All the sessions were guided by a therapist. | VR HW tool: Thunder 400/C virtual reality system by Virtual Engineering of Milano-Italy. View: FPV | The work describes the treatment, with VR technologies, of a 22-year-old university student diagnosed with Anorexia Nervosa | The patient had a high degree of motivation to change. The subject increased his body awareness coupled with a reduction in his level of body dissatisfaction. | 8/8 |
| Riva–1998 Applied Technology for Neuro-Psychology Lab., Istituto Auxologico Italiano, Verbania, Italy. Experiential Cognitive Therapy in Anorexia Nervosa Eating and Weight Disorders | Case study on a 22-year old female diagnosed with AN. | The study used experiential cognitive therapy (ECT), with the use of VR technologies (see 24). | VR HW tool: Thunder 400/C virtual reality system by Virtual Engineering of Milano-Italy. Additional HW, notes on SW: two-button joystick-type motion-input device. View: FPV | The article describes the characteristics of experiential cognitive therapy (ECT): a short-term, integrated and patient-oriented approach that focuses on individual discovery. | The patient had a high degree of motivation to change. The subject increased his body awareness coupled with a reduction in his level of body dissatisfaction. | 8/8 |
| Riva–1997 Applied Technology for Neuro-Psychology Lab., Istituto Auxologico Italiano, Verbania, Italy. The Virtual Environment for Body-Image Modification (VEBIM): Development and Preliminary EvaluationPresence-Teleoperators And Virtual Environments | 72 normal subjects. | The treatment uses a VR environment built with a VEBIM system. It consisted of a visit to 6 zones, guided by a therapist. Zone 1: a virtual balance. Zone: interaction with food. To move to zone 3 subjects had to weigh again. Zone 3: a corridor with male and female models. Zone 4: a room with the subject’s digitized picture. Zone 5: a room with four doors of different dimensions. The subject can only move into the by choosing the door corresponding exactly to his width and height. Zone 6: a room with the image of the subject’s real body, plus an image that can be modified to use to last zone create its ideal body. | VR HW tool: Thunder 400/C virtual reality system by Virtual Engineering of Milano-Italy. Additional HW, notes on SW: two-button joystick-type motion-input device. View: FPV | The purpose of the article is to describe the VEBIM (Virtual Environment for Body-Image Modification) theoretical approach and its characteristics. | The results report significantly lower values for FRS (Figure Rating Scale, Thompson, and Altabe, 1991) and CDRS (The Contour Drawing Rating Scale, Thompson, and Gray, 1995) after the experience in the virtual environment. | 8/9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magrini, M.; Curzio, O.; Tampucci, M.; Donzelli, G.; Cori, L.; Imiotti, M.C.; Maestro, S.; Moroni, D. Anorexia Nervosa, Body Image Perception and Virtual Reality Therapeutic Applications: State of the Art and Operational Proposal. Int. J. Environ. Res. Public Health 2022, 19, 2533. https://doi.org/10.3390/ijerph19052533
Magrini M, Curzio O, Tampucci M, Donzelli G, Cori L, Imiotti MC, Maestro S, Moroni D. Anorexia Nervosa, Body Image Perception and Virtual Reality Therapeutic Applications: State of the Art and Operational Proposal. International Journal of Environmental Research and Public Health. 2022; 19(5):2533. https://doi.org/10.3390/ijerph19052533
Chicago/Turabian StyleMagrini, Massimo, Olivia Curzio, Marco Tampucci, Gabriele Donzelli, Liliana Cori, Maria Cristina Imiotti, Sandra Maestro, and Davide Moroni. 2022. "Anorexia Nervosa, Body Image Perception and Virtual Reality Therapeutic Applications: State of the Art and Operational Proposal" International Journal of Environmental Research and Public Health 19, no. 5: 2533. https://doi.org/10.3390/ijerph19052533
APA StyleMagrini, M., Curzio, O., Tampucci, M., Donzelli, G., Cori, L., Imiotti, M. C., Maestro, S., & Moroni, D. (2022). Anorexia Nervosa, Body Image Perception and Virtual Reality Therapeutic Applications: State of the Art and Operational Proposal. International Journal of Environmental Research and Public Health, 19(5), 2533. https://doi.org/10.3390/ijerph19052533