
Teledermatology versus Face-to-Face Dermatology: An Analysis of Cost-Effectiveness from Eight Studies from Europe and the United States

 , and
, and 
Abstract
1. Introduction
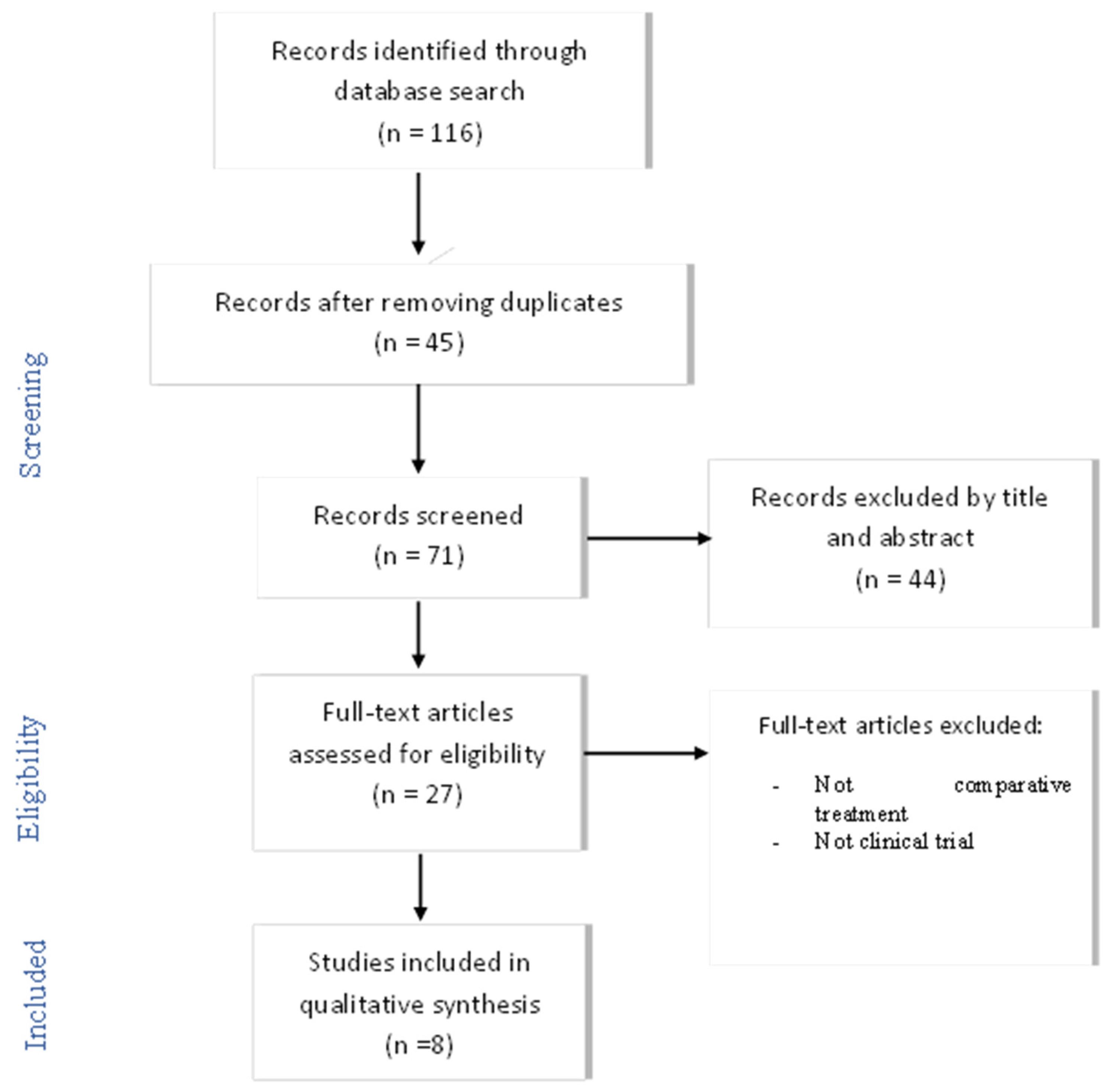
2. Materials and Methods
- Articles containing the MeSH terms: “Cost–Benefit Analysis”, “Dermatology”, “Telemedicine”, “Primary Health Care”. Other search terms included: “Cost–Utility Analysis”, “Economic Evaluation”, and “Cost-Effectiveness Analysis”, “Teledermatology”, “Skin Disease”, “Telehealth”, “Remote Consult” (conventional or “face-to-face” or standard or in-person).
- Clinical trials or observational studies comparing the two follow-up methods (face-to-face versus TD).
- Description of a single method for intervention or follow-up, without comparison.
- Clinical guidelines, systematic reviews and meta-analyses.
3. Results
3.1. Description of TD Procedure versus Face-to-face Follow-Up
3.2. Variables That Measure Direct and Indirect Costs
3.3. Variables That Measure the Effectiveness of TD versus Face-to-Face Follow-Up
3.4. Comparison of Cost-Effectiveness in Each Method of Follow-Up
3.5. Level of Evidence and Quality of Articles Included
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Byamba, K.; Syed-Abdul, S.; Garcia-Romero, M.T.; Huang, C.-W.; Nergyi, S.; Nyamdorj, A.; Nguyen, P.-A.; Iqbal, U.; Paik, K.; Celi, L.; et al. Mobile teledermatology for a prompter and more efficient dermatological care in rural Mongolia. Br. J. Dermatol. 2014, 173, 265–267. [Google Scholar] [CrossRef]
- Andrees, V.; Klein, T.; Augustin, M.; Otten, M. Live interactive teledermatology compared to in-person care—A systematic review. J. Eur. Acad. Dermatol. Venereol. 2019, 34, 733–745. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; English, J.C. Teledermatology: A Review and Update. Am. J. Clin. Dermatol. 2017, 19, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Alonso, C.; Salerni, G.; Fernández-Bussy, R. Teledermatología: Aplicaciones actuales y futuras. Dermatol. Argent. 2017, 23, 29–33. [Google Scholar]
- Kumar, S.; Bishnoi, A.; Vinay, K. Changing paradigms of dermatology practice in developing nations in the shadow of COVID -19: Lessons learnt from the pandemic. Dermatol. Ther. 2020, 33, e13472. [Google Scholar] [CrossRef] [PubMed]
- Pasquali, P.; Romero-Aguilera, G.; Moreno-Ramírez, D. Teledermatología en tiempos de pandemia: El antes, el durante y el después. Dermatol. Práctica 2020, 112, 324–329. [Google Scholar] [CrossRef]
- Pearlman, R.L.; Le, P.B.; Brodell, R.T.; Nahar, V.K. Evaluation of patient attitudes towards the technical experience of synchronous teledermatology in the era of COVID-19. Arch. Dermatol. Res. 2021, 313, 769–772. [Google Scholar] [CrossRef] [PubMed]
- Ayen-Rodríguez, A.; Llamas-Molina, J.M.; Cabrerizo-Carvajal, A.M.; Leon-López, F.J.; Ruiz-Villaverde, R. Teledermatología en el Área Sanitaria Centro Oeste de Granada desde atención primaria a especializada. Semergen 2021, 4, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Coustasse, A.; Sarkar, R.; Abodunde, B.; Metzger, B.J.; Slater, C.M. Use of Teledermatology to Improve Dermatological Access in Rural Areas. Telemed. E-Health 2019, 25, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Trettel, A.; Eissing, L.; Augustin, M. Telemedicine in dermatology: Findings and experiences worldwide—A systematic literature review. J. Eur. Acad. Dermatol. Venereol. 2017, 32, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Maddukuri, S.; Patel, J.; Lipoff, J.B. Teledermatology Addressing Disparities in Health Care Access: A Review. Curr. Dermatol. Rep. 2021, 10, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Stadler, P.; Senner, S.; Frey, S.; Clanner-Engelshofen, B.M.; Frommherz, L.H.; French, L.E.; Reinholz, M. Teledermatology in times of COVID-19. J. Dermatol. 2021, 48, 620–624. [Google Scholar] [CrossRef] [PubMed]
- McKoy, K.; Halpern, S.; Mutyambizi, K. International Teledermatology Review. Curr. Dermatol. Rep. 2021, 10, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Kaunitz, G.; Yin, L.; Nagler, A.R.; Sicco, K.L.; Kim, R.H. Assessing Patient Satisfaction with Live-Interactive Teledermatology Visits During the COVID-19 Pandemic: A Survey Study. Telemed. E-Health 2021. [Google Scholar] [CrossRef] [PubMed]
- Edwards, H.A.; Shen, X.; Soyer, H.P. Teledermatology Adaptations in the COVID-19 Era. Front. Med. 2021, 8, 675383. [Google Scholar] [CrossRef] [PubMed]
- Schuster, B.; Ziehfreund, S.; Tizek, L.; Krause, J.; Biedermann, T.; Zink, A. Wie offen ist die bayerische Bevölkerung für Teledermatologie? Eine Querschnittsstudie in ländlichen und städtischen Regionen Bayerns. Das Gesundh. 2019, 83, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Rustad, A.M.; Lio, P.A. Pandemic Pressure: Teledermatology and Health Care Disparities. J. Patient Exp. 2021, 8. [Google Scholar] [CrossRef]
- Arias, P.G.; Arenas, E.A.; Blanco, M.A.; Sánchez, J.R.; Gutiérrez, M.G.; García-Nieto, A.V. Aspectos medicolegales de la práctica de la teledermatología en España. Actas Dermosifiliogr. 2020, 112, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Urrutia, G.; Bonfill, X. PRISMA declaration: A proposal to improve the publication of systematic reviews and meta-analyses. Med. Clín. 2010, 135, 507–511. [Google Scholar] [CrossRef]
- Hutton, B.; Catalá-López, F.; Moher, D. La extensión de la declaración PRISMA para revisiones sistemáticas que incorporan metaanálisis en red: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G.; International Stroke Trial Collaborative Group; European Carotid Surgery Trial Collaborative Group. Evaluating nonrandomized intervention studies. Health Technol. Assess 2003, 7, 1–173. [Google Scholar] [CrossRef]
- Saunders, L.D.; Soomro, G.M.; Buckingham, J.; Jamtvedt, G.; Raina, P. Assessing the Methodological Quality of Nonrandomized Intervention Studies. West. J. Nurs. Res. 2003, 25, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Zakaria, A.; Miclau, T.A.; Maurer, T.; Leslie, K.S.; Amerson, E. Cost Minimization Analysis of a Teledermatology Triage System in a Managed Care Setting. JAMA Dermatol. 2021, 157, 52–58. [Google Scholar] [CrossRef]
- Lopez-Villegas, A.; Bautista-Mesa, R.J.; Baena-Lopez, M.A.; Alvarez-Moreno, M.L.; Montoro-Robles, J.E.; Vega-Ramirez, F.A.; Ordoñez-Naranjo, I.; Hernandez-Montoya, C.J.; Leal-Costa, C.; Peiró, S. Economic impact and cost savings of teledermatology units compared to conventional monitoring at hospitals in southern Spain. J. Telemed. Telecare 2020. [Google Scholar] [CrossRef]
- Vidal-Alaball, J.; Garcia-Domingo, J.L.; Cuyàs, F.G.; Peña, J.M.; Flores-Mateo, G.; Rosanas, J.D.; Valmaña, G.S. A cost savings analysis of asynchronous teledermatology compared to face-to-face dermatology in Catalonia. BMC Heal. Serv. Res. 2018, 18, 650. [Google Scholar] [CrossRef]
- Yang, X.; Barbieri, J.S.; Kovarik, C.L. Cost analysis of a store-and-forward teledermatology consult system in Philadelphia. J. Am. Acad. Dermatol. 2018, 81, 758–764. [Google Scholar] [CrossRef]
- Zarca, K.; Charrier, N.; Mahé, E.; Guibal, F.; Carton, B.; Moreau, F.; Durand-Zaleski, I. Tele-expertise for diagnosis of skin lesions is cost-effective in a prison setting: A retrospective cohort study of 450 patients. PLoS ONE 2018, 13, e0204545. [Google Scholar] [CrossRef] [PubMed]
- Datta, S.K.; Warshaw, E.M.; Edison, K.; Kapur, K.; Thottapurathu, L.; Moritz, T.E.; Reda, D.J.; Whited, J.D. Cost and Utility Analysis of a Store-and-Forward Teledermatology Referral System. JAMA Dermatol. 2015, 151, 1323–1329. [Google Scholar] [CrossRef]
- Os-Medendorp, H.; Koffijberg, H.; Kok, P.C.M.E.; Zalm, A.; Bruin-Weller, M.S.; Pasmans, S.G.M.A.; Ros, W.J.G.; Thio, H.B.; Knol, M.J.; Bruijnzeel-Koomen, C.A.F.M. E-health in caring for patients with atopic dermatitis: A randomized controlled cost-effectiveness study of internet-guided monitoring and online self-management training. Br. J. Dermatol. 2012, 166, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Parsi, K.; Chambers, C.J.; Armstrong, A.W. Cost-effectiveness analysis of a patient-centered care model for management of psoriasis. J. Am. Acad. Dermatol. 2012, 66, 563–570. [Google Scholar] [CrossRef]
- Barbieri, J.S.; Kovarik, C.L. Inpatient and Tertiary Consultations in Teledermatology. Curr. Dermatol. Rep. 2016, 5, 83–89. [Google Scholar] [CrossRef]
- Tognetti, L.; Fiorani, D.; Russo, F.; Lazzeri, L.; Trovato, E.; Flori, M.L.; Moscarella, E.; Cinotti, E.; Rubegni, P. Teledermatology in 2020: Past, present and future per-spectives. Ital. J. Dermatol. Venerol. 2021, 156, 198–212. [Google Scholar] [CrossRef]
- Barbieri, J.S.; Nelson, C.A.; James, W.D.; Margolis, D.J.; Littman-Quinn, R.; Kovarik, C.L.; Rosenbach, M. The Reliability of Teledermatology to Triage Inpatient Dermatology Consultations. JAMA Dermatol. 2014, 150, 419. [Google Scholar] [CrossRef]
- Ferrándiz, L.; Ojeda-Vila, T.; Corrales, A.; Martín-Gutiérrez, F.J.; Ruíz-De-Casas, A.; Galdeano, R.; Álvarez-Torralba, I.; Sánchez-Ibáñez, F.; Domínguez-Toro, J.M.; Encina, F.; et al. Internet-based skin cancer screening using clinical images alone or in conjunction with dermoscopic images: A randomized teledermoscopy trial. J. Am. Acad. Dermatol. 2017, 76, 676–682. [Google Scholar] [CrossRef]
- Nelson, C.A.; Takeshita, J.; Wanat, K.A.; Bream, K.; Holmes, J.H.; Koenig, H.C.; Roth, R.R.; Vuppalapati, A.; James, W.D.; Kovarik, C.L. Impact of store-and-forward (SAF) teledermatology on outpatient dermatologic care: A prospective study in an underserved urban primary care setting. J. Am. Acad. Dermatol. 2016, 74, 484–490.e1. [Google Scholar] [CrossRef]
- Cutler, L.; Ross, K.; Withers, M.; Chiu, M.; Cutler, D. Teledermatology: Meeting the Need for Specialized Care in Rural Haiti. J. Health Care Poor Underserved 2019, 30, 1394–1406. [Google Scholar] [CrossRef]
- Tran, K.; Ayad, M.; Weinberg, J.; Cherng, A.; Chowdhury, M.; Monir, S.; El Hariri, M.; Kovarik, C. Mobile teledermatology in the developing world: Implications of a feasibility study on 30 Egyptian patients with common skin diseases. J. Am. Acad. Dermatol. 2011, 64, 302–309. [Google Scholar] [CrossRef]
- Kozera, E.K.; Yang, A.; Murrell, D.F. Patient and practitioner satisfaction with tele-dermatology including Australia’s indigenous population: A systematic review of the literature. Int. J. Women’s Dermatol. 2016, 2, 70–73. [Google Scholar] [CrossRef]
- Snoswell, C.; Finnane, A.; Janda, M.; Soyer, H.P.; Whitty, J.A. Cost-effectiveness of Store-and-Forward Teledermatology. JAMA Dermatol. 2016, 152, 702–708. [Google Scholar] [CrossRef]
- Hadeler, E.; Gitlow, H.; Nouri, K. Definitions, survey methods, and findings of patient satisfaction studies in teledermatology: A systematic review. Arch. Dermatol. Res. 2020, 313, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Vyas, K.S.; Hambrick, H.R.; Shakir, A.; Morrison, S.; Tran, D.C.; Pearson, K.; Vasconez, H.C.; Mardini, S.; Gosman, A.A.; Dobke, M.; et al. A Systematic Review of the Use of Telemedicine in Plastic and Reconstructive Surgery and Dermatology. Ann. Plast. Surg. 2017, 78, 736–768. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Databases and Search Terms | Results | Selected Articles |
|---|---|---|
SCOPUS, SCIELO, MEDLINE
| 100 | 26 |
PUBMED
| 16 | 1 |
| Author, Year Country | Type of Study Participants Diagnosis | Dermatology Follow-Up Method | Main Results |
|---|---|---|---|
| Zakaria, 2020 [24] United States | A retrospective cost-minimization analysis In TD:
| Compared dermatology patients within a TD triage system vs. a conventional dermatology care model Asynchronous 1st PC consultation + TD consultation Follow-up: 6 months | Average cost/patient TD: $559.84 Average cost/patient conventional consultation: $699.96 TD reduces costs by $140.12 ($11.01) per patient, representing approximately $441,378 per year. |
| López-Villegas, 2020 [25] Spain | Inter-level multicentre retrospective study n = 7030 patients
2 excluded, software error 3507 diagnosed and treated by dermatologist using the platform 730 received recommendations from PC doctor Diagnoses: non-benign pathologies (basal-cell carcinoma, melanoma, squamous-cell carcinoma, other types of skin cancer) and Benign pathologies (actinic keratosis) | Teledermatology units compared to conventional monitoring at hospitals Asynchronous 1st PC consultation + TD consultation Follow-up: 1 year | Savings of 61.86% of hospital visits There was a cost savings of 31.68% in the TD group (€18.59 TD vs. €27.20 CM) during the follow-up period. The number of CM visits to the hospital reduced by 38.14%. From the patients’ perspective, the costs were lower, and the cost savings was 73.53% (€5.45 TD vs. €20.58 CM). TD is an economic solution in comparison with conventional dermatology, both from the perspective of the public healthcare system and the patient, obtaining clear cost savings The results cannot be extrapolated to countries with different healthcare systems |
| Vidal-Alaball, 2018 [26] Spain | Observational Study n = 5606 patients 1104 patients sent to in-person consultation No specific mention of main diagnoses | A cost–savings analysis comparing teledermatology with traditional dermatology consultations (face-to-face) Asynchronous 1st PC consultation + TD consultation Follow-up: 3 months | TD saved 4502 in-person visits. The use of TD versus face-to-face consultations generates savings of 51,164.00 euros/year (11.40 euros/patient) Societal savings are the most significant Cannot be extrapolated to countries with different healthcare systems |
| Yang, 2018 [27] United States | A retrospective study of the cases n = 700 patients 189 patients required in-person consultation 23 required urgent care 86% of patients were assisted via TD | Analysis compared the cost of each patient case with use of the TD consultation model vs. conventional care Asynchronous 1st PC consultation + TD consultation Follow-up: 5 years | Compared with conventional care, TD had an average expected cost savings of $10.00 to $52.65 per TD consultation Providing access to high-quality care, this program reduced unnecessary in-person dermatology clinical visits as well as urgent care Significantly reduces the costs of dermatological care, increases access and improves patient satisfaction and clinical results |
| Zarca, 2018 [28] France | Retrospective cohort study n = 450 prisoners 82% (368/450) of the patients with tele-expertise had a complete treatment plan The most frequent lesions were acnea and atopic dermatitis | Evaluate the effectiveness and costs of tele-expertise in dermatology Follow-up: 1 year | For 368 patients every year, the average cost is €184 for completed treatment plans distributed as follows: 34% investment, 66% operating cost (30% human resource, 36% software) Tele-expertise was found to be effective, increasing the proportion of patients with completed treatment plans and the overall satisfaction of physicians, at a cost far lower than a dermatologist consultation in a hospital |
| Datta, 2015 [29] United States | Randomized clinical trial Conventional n = 196 patients TD: n = 195 patients 1 patient excluded, assignment error Ambulatory skin conditions | To assess the costs and utility of a store-and-forward teledermatology referral process compared with conventional referral process. Asynchronous 1st PC consultation PC + TD consultation Follow-up: 9 months | The TD cost per patient was $30 lower and, from a societal perspective, saved $82 The differences in effectiveness for both groups were not significant Compared with conventional referrals, store-and-forward teledermatology referrals were performed at a comparable cost (VA perspective) or at a lower cost (societal perspective) with no evidence of a difference in utility as measured by the time trade-off method |
| Os-Medendorp, 2012 [30] Netherlands | Randomized controlled study with economic evaluation n = 199 patients with atopic dermatitis CG: n = 98 IG n = 101 | Determine the cost-effectiveness of individualized e-health compared with usual face-to-face care Asynchronous 1st appointment with dermatologist + TD Follow-up: 3 months and after 1 year | Both interventions proved effective regarding quality of life and severity of illness, but there were no significant differences. The difference in total costs between the CG and the IG is €594 per patient during the first year of treatment IG: average 3378 € per patient CG: 3972 € per patient It is possible that telemedicine is more economical because it involves fewer days of work absenteeism; although the results may not be consistent due to the heterogeneity of the interventions Uncertainty analyses revealed that the probability of e-health reducing costs was estimated to be around 73% |
| Parsi, 2011 [31] United States | Randomized Controlled Trial Cost-effectiveness Analyses n = 64 patients with psoriasis. | Compare cost-effectiveness of conventional in-office care with a patient-centered, online model for follow-up treatment Asynchronous. Remote monitoring by the patient (previous training) Follow-up: 24 weeks | Both improved patient quality of life and proved effective: patients gained 23.3 weeks of quality of life with TD and 24.1 with in-person care The online model is equally effective but less expensive than face-to-face: The cost of follow-up care with online visits was 1.7 times less than the cost of in-person visits ($315 vs. $576). TD costs $261.10 less per patient. Users also expressed their preference for TD. TD appears to be an innovative and profitable healthcare model for follow-up and treatment of patients with psoriasis |
| Author, Year | Direct Costs | Indirect Costs | Exclusion of Costs | Effectiveness Variables |
|---|---|---|---|---|
| Zakaria, 2020 [24] | Costs associated with PC, dermatology and TD visits (number of visits) Personal costs: salary and time Technological costs: installation of licensed software, software support, maintenance services, equipment and training for professionals | No reference made to indirect costs | Exclusion of rent costs, clinical supplies, public services and social costs | Does not include effectiveness |
| López-Villegas, 2020 [25] | Costs from PHS perspective: Number of both conventional and TD visits PC and hospital costs: labour costs and specific costs of TD equipment and materials (Canon EOS camera and dermascopy lens); every 5 years | Patient Cost Perspective: Transport costs, travel time, waiting time and time of visit | Exclusion of structural costs (electricity, telecommunications, construction and maintenance) Exclusion of number of trips and wages lost by companions | Effectiveness was not measured |
| Vidal-Alaball, 2018 [26] | Number of PC, dermatological and TD visits. Direct costs: cameras, hardware and personnel Equipment costs: iPad Air with WIFI and a mobile phone with 32 GB; every 5 years. | Costs included building maintenance, IT services, gas, electricity, telephone–internet connections and medical insurance Patient costs: Loss of productive time, salary and transport costs (time and fuel) | Exclusion of costs incurred by companions, loss of free time, technical and maintenance costs, training costs for professionals and medical insurance | Effectiveness was not measured |
| Yang, 2018 [27] | Direct medical costs of health care: average cost of an in-person dermatology visit, an emergency dermatology visit, and the dermatologist for a TD visit | Indirect costs were not included | Separate costs for medications, patient travel, laboratory work and/or imaging or procedures outside of the visits were not included in the analysis | PC doctors were asked about their satisfaction with using TD |
| Zarca, 2018 [28] | Evaluates image quality but not diagnostic precision Costs of transport, facilities and hospitals Investment costs Operational costs: maintenance and human resources | The proportion of patients with a completed treatment plan for skin lesions, the proportion of technical problems, the quality of the pictures, the investment and operating costs and the satisfaction of the professionals Average cost of a complete treatment plan: investment costs + operational costs | They could not evaluate the diagnostic accuracy of telemedicine; the causes of “failed upload, unanswered requests and unsatisfactory requests”; unable to measure patient satisfaction | Satisfaction survey for doctors. |
| Datta, 2015 [29] | The cost elements from the VA perspective included: TD intervention or referral; referral and follow-up visits to the dermatology clinic; dermatological medications prescribed; travel cost reimbursement to patients paid by the VA; and dermatology-related hospitalizations | Dermatological care sought outside of the VA system; travel costs in seeking health care if not reimbursed by the VA; and work or productivity loss owing to the patient | They did not include the equipment cost in TD | Time trade-off determines the quality of life one experiences in a given state of health by assessing the equivalence point between living a longer life with the given medical condition vs. a shorter life in perfect health |
| Os-Medendorp, 2012 [30] | Costs of primary care, e-health service and outpatient clinics Care at the dermatology department Telephone consultation with a dermatologist Combined visit to dermatology nurse and dermatologist Day of hospitalization Number of e-consultations with dermatology nurse Care at other hospital departments Care by the general practitioner | Two modules online of the ‘Health and Labour Questionnaire’ Written diary to gather data regarding days on leave from work Visits with transportation and parking costs to a medical specialist or nurse in a hospital; a general practitioner; days of work absenteeism; hours with loss of productivity during work; hours with loss of productivity in unpaid work | Equipment costs not included | Quality of life, itch intensity and severity of atopic dermatitis *DLQI *IDQOL *VAS Two parts of the online questionnaire “Impact of Chronic Skin Disease on Daily Life” (shortened version) |
| Parsi, 2011 [31] | Social perspective: Online costs: Medical: clinic and facility fees, morbidity and mortality Non-medical: loss of productivity, cost of patient’s time, equipment (camera, computer) In-office costs: Medical: clinic and facility fees, morbidity and mortality Non-medical: loss of productivity, cost of patient’s time (including travel costs) | Costs of patient’s time: patient wages/minute, duration of visit, cost of patient’s time/visit | Not included | Quality-adjusted life expectancy *HLQOL *QALY *DLQI *QALE *EQ-5D |
| Study Quality | External Validity | Study Bias | Confounding and Selection Bias | Study Power | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author (Year) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | Total | Quality |
| Zakaria, 2020 [24] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 23 | Good |
| López-Villegas, 2020 [25] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 21 | Good |
| Vidal-Alaball, 2018 [26] | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 17 | Fair |
| Yang, 2018 [27] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 22 | Good |
| Zarca, 2018 [28] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 21 | Good |
| Datta, 2015 [29] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 25 | Good |
| Os-Medendorp, 2012 [30] | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 25 | Good |
| Parsi, 2011 [31] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 22 | Good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Liria, R.; Valverde-Martínez, M.Á.; López-Villegas, A.; Bautista-Mesa, R.J.; Vega-Ramírez, F.A.; Peiró, S.; Leal-Costa, C. Teledermatology versus Face-to-Face Dermatology: An Analysis of Cost-Effectiveness from Eight Studies from Europe and the United States. Int. J. Environ. Res. Public Health 2022, 19, 2534. https://doi.org/10.3390/ijerph19052534
López-Liria R, Valverde-Martínez MÁ, López-Villegas A, Bautista-Mesa RJ, Vega-Ramírez FA, Peiró S, Leal-Costa C. Teledermatology versus Face-to-Face Dermatology: An Analysis of Cost-Effectiveness from Eight Studies from Europe and the United States. International Journal of Environmental Research and Public Health. 2022; 19(5):2534. https://doi.org/10.3390/ijerph19052534
Chicago/Turabian StyleLópez-Liria, Remedios, María Ángeles Valverde-Martínez, Antonio López-Villegas, Rafael Jesús Bautista-Mesa, Francisco Antonio Vega-Ramírez, Salvador Peiró, and Cesar Leal-Costa. 2022. "Teledermatology versus Face-to-Face Dermatology: An Analysis of Cost-Effectiveness from Eight Studies from Europe and the United States" International Journal of Environmental Research and Public Health 19, no. 5: 2534. https://doi.org/10.3390/ijerph19052534
APA StyleLópez-Liria, R., Valverde-Martínez, M. Á., López-Villegas, A., Bautista-Mesa, R. J., Vega-Ramírez, F. A., Peiró, S., & Leal-Costa, C. (2022). Teledermatology versus Face-to-Face Dermatology: An Analysis of Cost-Effectiveness from Eight Studies from Europe and the United States. International Journal of Environmental Research and Public Health, 19(5), 2534. https://doi.org/10.3390/ijerph19052534