
Process Design for Optimized Respiration Identification Based on Heart Rate Variability for Efficient Respiratory Sinus Arrhythmia Biofeedback



Abstract
:1. Introduction
2. Proposed Work
2.1. Overall Process Description
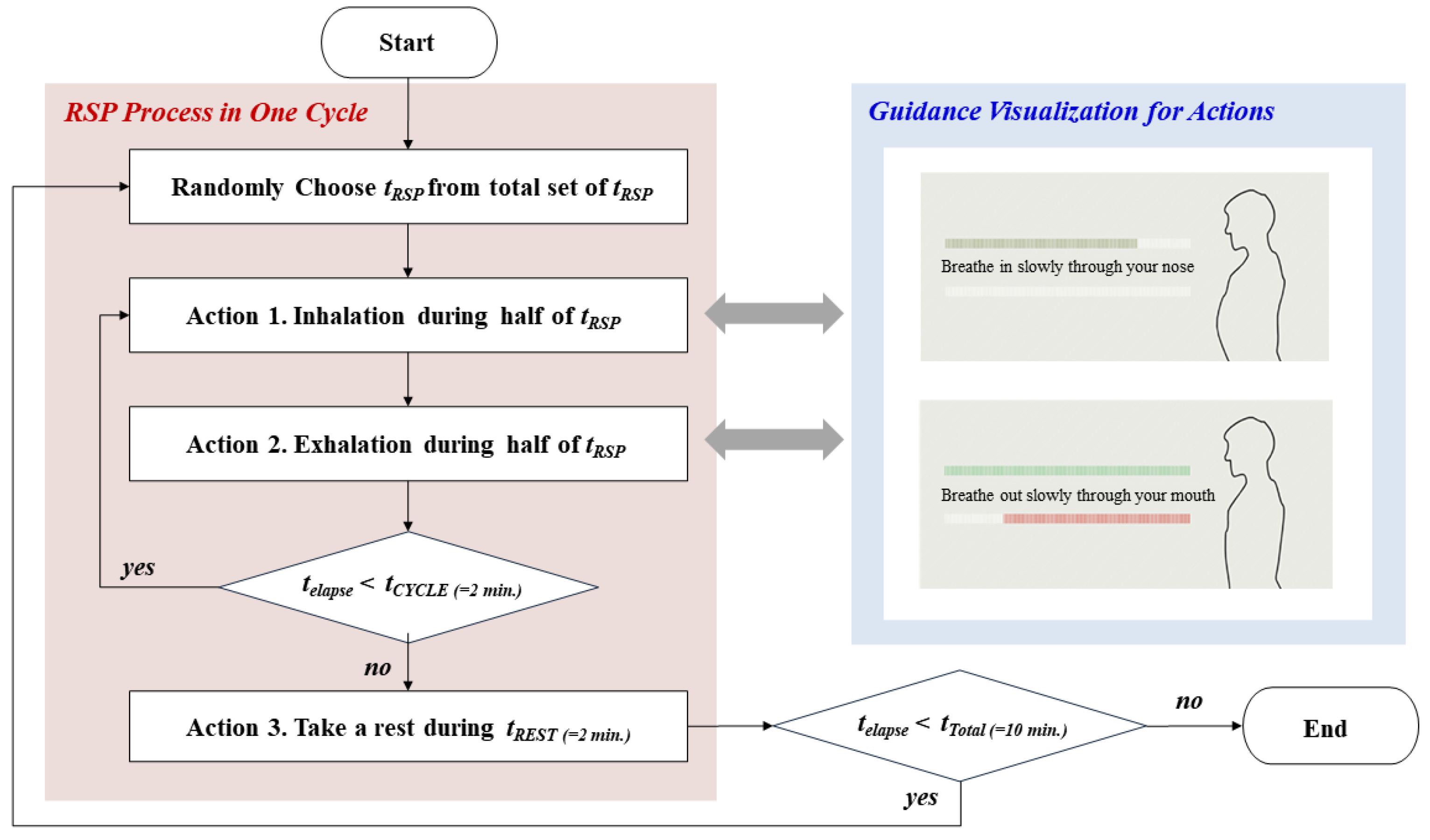
2.2. Description on Respiration Guidance
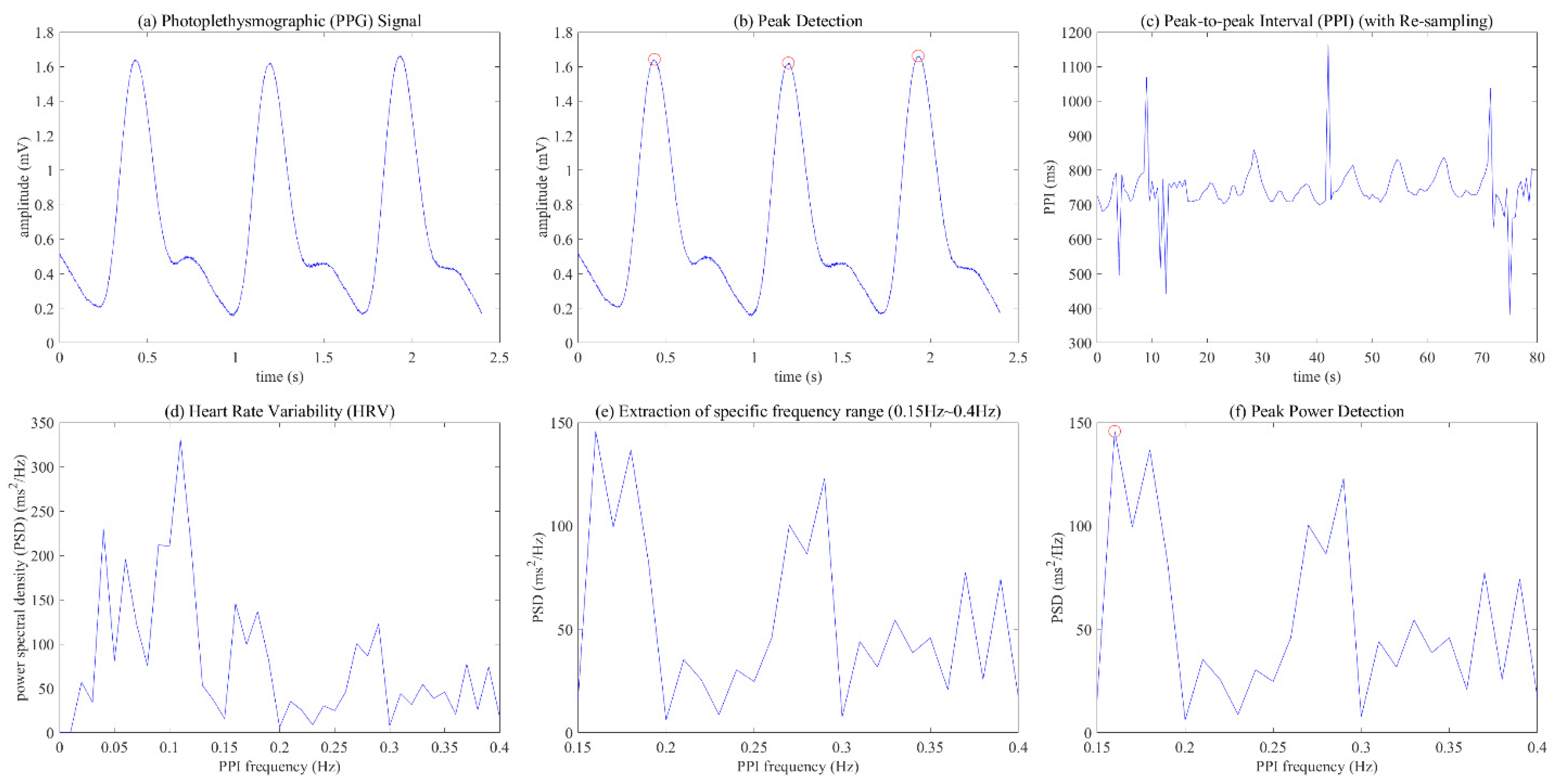
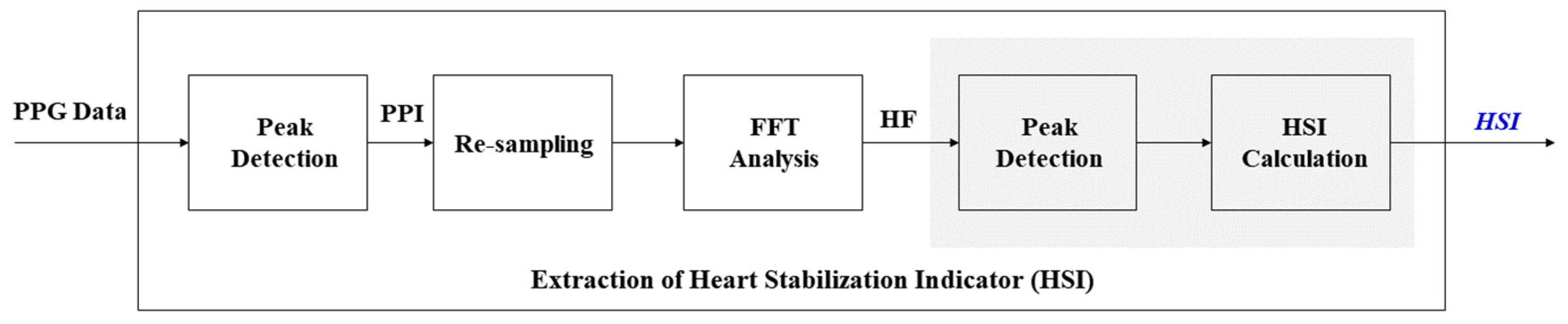
2.3. Description on Extraction HSI Process
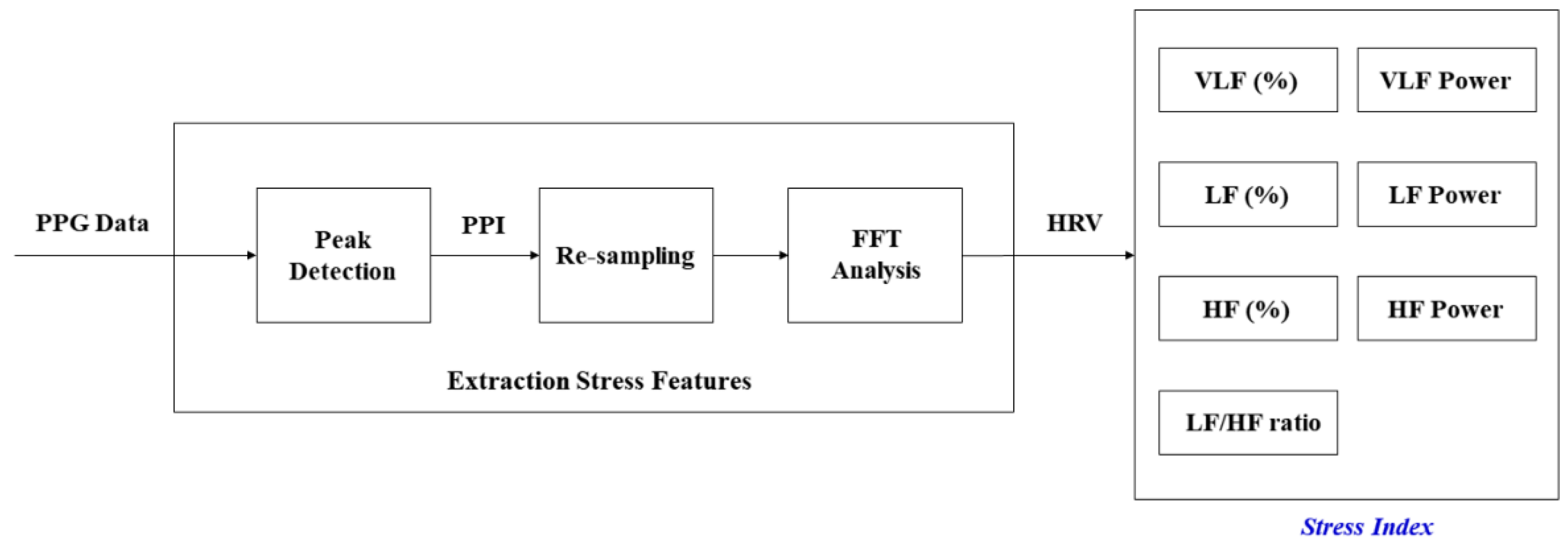
2.4. Description on Extraction Stress Features
3. Experimental Design
3.1. Participants and Experimental Device
3.2. Stimuli (Respiratory Cycles)
3.3. Dependent Variables
3.4. Statistical Analysis
4. Experimental Results
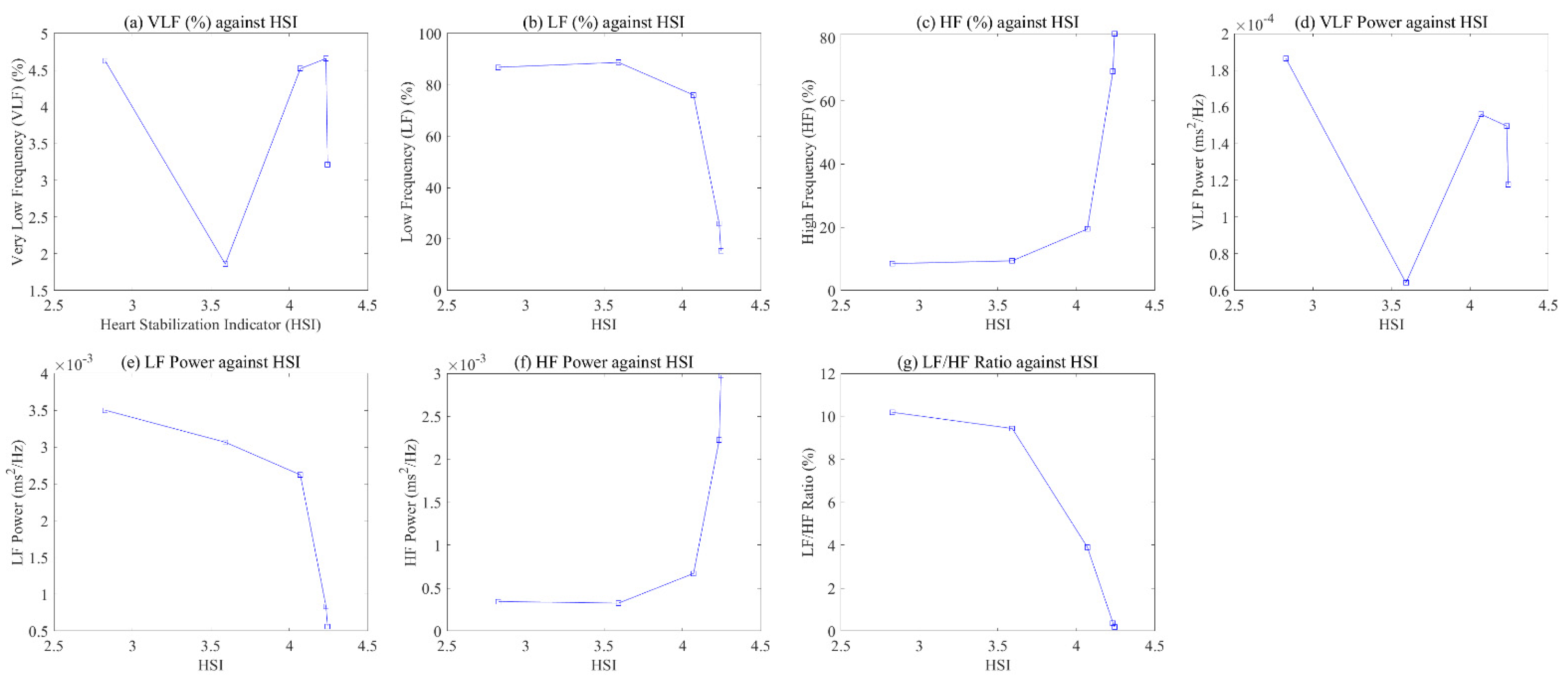
4.1. Relationship HSI and Stress Indices
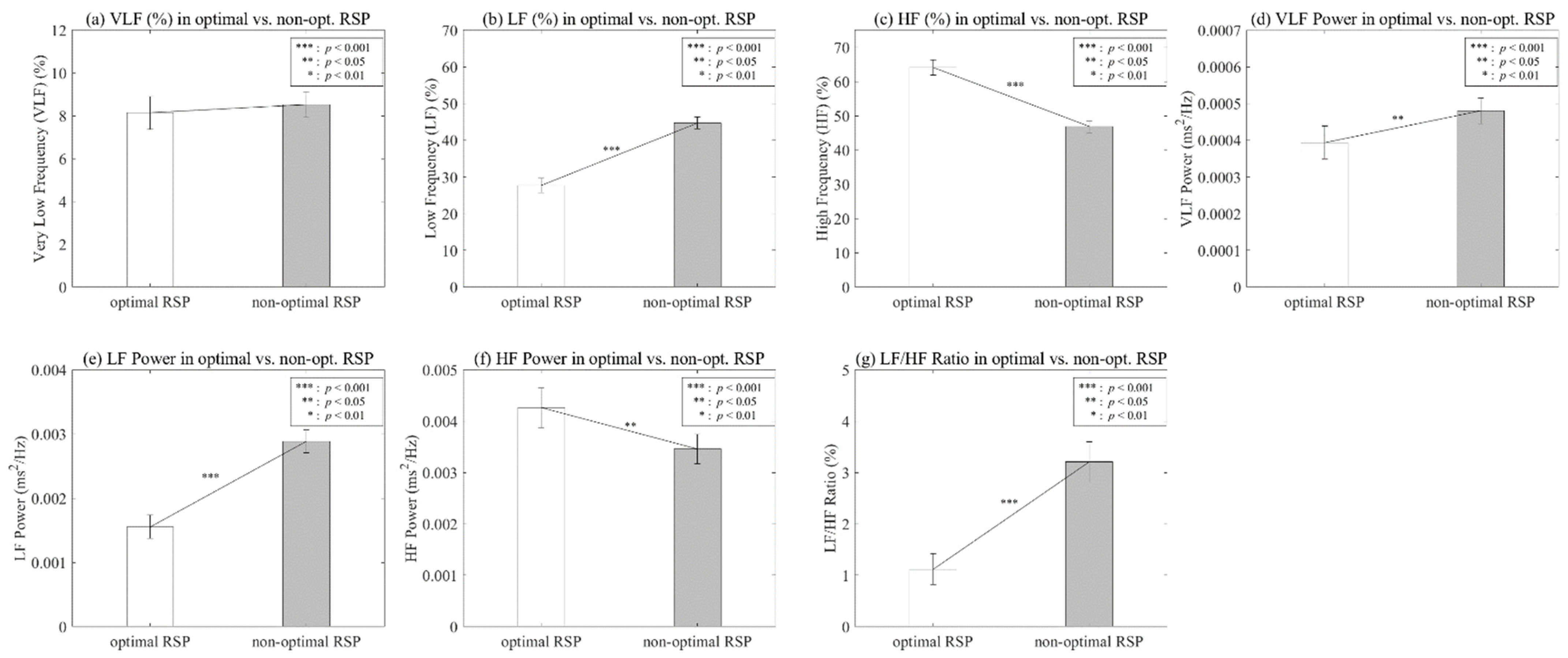
4.2. Difference of Optimal and Non-Optimal RSP
5. Discussion
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cannard, G. The effect of aromatherapy in promoting relaxation and stress reduction in a general hospital. Complement. Ther. Nurs. Midwifery 1996, 2, 38–40. [Google Scholar] [CrossRef]
- Malathi, A.; Damodaran, A. Stress due to exams in medical students-a role of Yoga. Indian J. Physiol. Pharmacol. 1999, 43, 218–224. [Google Scholar] [PubMed]
- Knight, W.E.; Rickard, N.S. Relaxing music prevents stress-induced increases in subjective anxiety, systolic blood pressure, and heart rate in healthy males and females. J. Music Ther. 2001, 38, 254–272. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, C. Breathing and the cardiovascular system. J. Bodyw. Mov. Ther. 1999, 3, 215–224. [Google Scholar] [CrossRef]
- Sovik, R. The science of breathing–The yogic view. Prog. Brain Res. 2000, 122, 491–505. [Google Scholar]
- Raghuraj, P.; Ramakrishnan, A.G.; Nagendra, H.R.; Telles, S. Effect of two selected yogic breathing techniques on heart rate variability. Indian J. Physiol. Pharmacol. 1998, 42, 467–472. [Google Scholar]
- Aysin, B.; Aysin, E. Effect of Respiration in Heart Rate Variability (HRV) Analysis. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 1776–1779. [Google Scholar]
- Jerath, R.; Edry, J.W.; Barnes, V.A.; Jerath, V. Physiology of long pranayamic breathing: Neural respiratory elements may provide a mechanism that explains how slow deep breathing shifts the autonomic nervous system. Med. Hypotheses 2006, 67, 566–571. [Google Scholar] [CrossRef] [Green Version]
- Gatti, P.J.; Johnson, T.A.; Massari, V.J. Can neurons in the nucleus ambiguus selectively regulate cardiac rate and atrio-ventricular conduction? J. Auton. Nerv. Syst. 1996, 57, 123–127. [Google Scholar] [CrossRef]
- Haselton, J.R.; Solomon, I.C.; Motekaitis, A.M.; Kaufman, M.P. Bronchomotor vagal preganglionic cell bodies in the dog: An anatomic and functional study. J. Appl. Physiol. 1992, 73, 1122–1129. [Google Scholar] [CrossRef]
- Porges, S.W. Cardiac vagal tone: A physiological index of stress. Neurosci. Biobehav. Rev. 1995, 19, 225–233. [Google Scholar] [CrossRef]
- Porges, S.W. The polyvagal theory: Phylogenetic contributions to social behavior. Physiol. Behav. 2003, 79, 503–513. [Google Scholar] [CrossRef]
- Porges, S.W. The polyvagal perspective. Biol. Psychol. 2007, 74, 116–143. [Google Scholar] [CrossRef] [PubMed]
- Porges, S.W. The polyvagal theory: New insights into adaptive reactions of the autonomic nervous system. Clevel. Clin. J. Med. 2009, 76 (Suppl. 2), S86–S90. [Google Scholar] [CrossRef]
- Frank, D.L.; Khorshid, L.; Kiffer, J.F.; Moravec, C.S.; McKee, M.G. Biofeedback in medicine: Who, when, why and how? Ment. Health Fam. Med. 2010, 7, 85–91. [Google Scholar]
- Saha, S.; Dey, D.; Bhattacharyya, I.M.; Das, A. An Investigation on Biofeedback Analysis and Psychosomatic Applications. In Proceedings of the 2015 International Conference on Recent Developments in Control, Automation and Power Engineering (RDCAPE), Noida, India, 12–13 March 2015; Volume 12, pp. 38–43. [Google Scholar]
- Steingrimsson, S.; Bilonic, G.; Ekelund, A.C.; Larson, T.; Stadig, I.; Svensson, M.; Vukovic, I.S.; Wartenberg, C.; Wrede, O.; Bernhardsson, S. Electroencephalography-based neurofeedback as treatment for post-traumatic stress disorder: A systematic review and meta-analysis. Eur. Psychiatry 2020, 63, e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunkin, H.; King, D.L.; Zajac, I.T. EEG neurofeedback during focused attention meditation: Effects on state mindfulness and meditation experiences. Mindfulness 2021, 12, 841–851. [Google Scholar] [CrossRef]
- Hsieh, H.F.; Huang, I.; Liu, Y.; Chen, W.L.; Lee, Y.W.; Hsu, H.T. The effects of biofeedback training and smartphone-delivered biofeedback training on resilience, occupational stress, and depressive symptoms among abused psychiatric nurses. Int. J. Environ. Res. Public Health 2020, 17, 2905. [Google Scholar] [CrossRef]
- Wu, W.; Zhang, H.; Pirbhulal, S.; Mukhopadhyay, S.C.; Zhang, Y.T. Assessment of biofeedback training for emotion management through wearable textile physiological monitoring system. IEEE Sens. J. 2015, 15, 7087–7095. [Google Scholar] [CrossRef]
- Lehrer, P.M.; Vaschillo, E.; Vaschillo, B. Resonant frequency biofeedback training to increase cardiac variability: Rationale and manual for training. Appl. Psychophysiol. Biofeedback 2000, 25, 177–191. [Google Scholar] [CrossRef]
- Lisspers, J.; Ost, L.G. BVP-Biofeedback in the treatment of migraine: The effects of constriction and dilatation during different phases of the migraine attack. Behav. Modif. 1990, 14, 200–221. [Google Scholar] [CrossRef]
- Schoenberg, P.L.; Hepark, S.; Kan, C.C.; Barendregt, H.P.; Buitelaar, J.K.; Speckens, A.E. Effects of mindfulness-based cognitive therapy on neurophysiological correlates of performance monitoring in adult attention-deficit/hyperactivity disorder. Clin. Neurophysiol. 2014, 125, 1407–1416. [Google Scholar] [CrossRef] [PubMed]
- Enriquez-Geppert, S.; Smit, D.; Pimenta, M.G.; Arns, M. Neurofeedback as a treatment intervention in ADHD: Current evidence and practice. Curr. Psychiatry Rep. 2019, 21, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerjee, S.; Argáez, C. Neurofeedback and Biofeedback for Mood and Anxiety Disorders: A Review of Clinical Effectiveness and Guidelines; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 2017; pp. 1–26. [Google Scholar]
- Markiewcz, R. The use of EEG Biofeedback/Neurofeedback in psychiatric rehabilitation. Psychiatr. Pol. 2017, 51, 1095–1106. [Google Scholar] [CrossRef] [PubMed]
- Vaschillo, E.; Lehrer, P.; Rishe, N.; Konstantinov, M. Heart rate variability biofeedback as a method for assessing baroreflex function: A preliminary study of resonance in the cardiovascular system. Appl. Psychophysiol. Biofeedback 2002, 27, 1–27. [Google Scholar] [CrossRef]
- Chernigovskaya, N.V.; Vashchillo, E.G.; Petrash, V.V.; Rusanovskii, V.V. Voluntary control of the heart rate as a method of correcting the functional state in neurosis. Hum. Physiol. 1990, 16, 105–111. [Google Scholar]
- Eckberg, D.L.; Sleight, P. Human Baroreflexes in Health and Disease; Oxford University Press: Oxford, UK, 1992. [Google Scholar]
- Tiinanen, S.; Tulppo, M.; Seppanen, T. Reducing the effect of respiration in baroreflex sensitivity estimation with adaptive filtering. IEEE Trans. Biomed. Eng. 2007, 55, 51–59. [Google Scholar] [CrossRef]
- Porges, S.W.; Doussard-Roosevelt, J.A.; Maiti, A.K. Vagal tone and the physiological regulation of emotion. Monogr. Soc. Res. Child Dev. 1994, 59, 167–186. [Google Scholar] [CrossRef]
- Carney, R.M.; Blumenthal, J.A.; Stein, P.K.; Watkins, L.; Catellier, D.; Berkman, L.F.; Czajkowski, S.M.; O’Connor, C.; Stone, P.H. Freedland KE. Depression, heart rate variability, and acute myocardial infarction. Circulation 2001, 104, 2024–2028. [Google Scholar] [CrossRef]
- Bonnet, M.H.; Arand, D.L. Heart rate variability in insomniacs and matched normal sleepers. Psychosom. Med. 1998, 60, 610–615. [Google Scholar] [CrossRef]
- Karavidas, M.K.; Lehrer, P.M.; Vaschillo, E.; Vaschillo, B.; Marin, H.; Buyske, S.; Malinovsky, I.; Radvanski, D.; Hassett, A. Preliminary results of an open label study of heart rate variability biofeedback for the treatment of major depression. Appl. Psychophysiol. Biofeedback 2007, 32, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Nickel, P.; Nachreiner, F. Sensitivity and diagnosticity of the 0.1-Hz component of heart rate variability as an indicator of mental workload. Hum. Factors 2003, 45, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, P. Respiratory sinus arrhythmia as a function of state anxiety in healthy individuals. Int. J. Psychophysiol. 2007, 63, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, P.; Carr, R.E.; Smetankine, A.; Vaschillo, E.; Peper, E.; Porges, S.; Edelberg, R.; Hamer, R.; Hochron, S. Respiratory sinus arrhythmia versus neck/trapezius EMG and incentive inspirometry biofeedback for asthma: A pilot study. Appl. Psychophysiol. Biofeedback 1997, 22, 95–109. [Google Scholar] [CrossRef]
- Lehrer, P.M.; Vaschillo, E.; Vaschillo, B.; Lu, S.E.; Eckberg, D.L.; Edelberg, R.; Shih, W.J.; Lin, Y.; Kuusela, T.A.; Tahvanainen, K.U.; et al. Heart rate variability biofeedback increases baroreflex gain and peak expiratory flow. Psychosom. Med. 2003, 65, 796–805. [Google Scholar] [CrossRef] [Green Version]
- Yucha, C.B.; Tsai, P.S.; Calderon, K.S.; Tian, L. Biofeedback-assisted relaxation training for essential hypertension: Who is most likely to benefit? J. Cardiovasc. Nurs. 2005, 20, 198–205. [Google Scholar] [CrossRef]
- Lehrer, P.M.; Vaschillo, E.G.; Vidali, V. Heart rate and breathing are not always in phase during resonance frequency breathing. Appl. Psychophysiol. Biofeedback 2020, 45, 145–152. [Google Scholar] [CrossRef]
- Steffen, P.R.; Austin, T.; DeBarros, A.; Brown, T. The impact of resonance frequency breathing on measures of heart rate variability, blood pressure, and mood. Front. Public Health 2017, 5, 222. [Google Scholar] [CrossRef] [Green Version]
- Zautra, A.J.; Fasman, R.; Davis, M.C.; Arthur, D. The effects of slow breathing on affective responses to pain stimuli: An experimental study. Pain 2010, 149, 12–18. [Google Scholar] [CrossRef]
- Cullins, S.W.; Gevirtz, R.N.; Poeltler, D.M.; Cousins, L.M.; Harpin, R.E.; Muench, F. An exploratory analysis of the utility of adding cardiorespiratory biofeedback in the standard care of pregnancy-induced hypertension. Appl. Psychophysiol. Biofeedback 2013, 38, 161–170. [Google Scholar] [CrossRef]
- Berntson, G.G.; Cacioppo, J.T.; Quigley, K.S. Respiratory sinus arrhythmia: Autonomic origins, physiological mechanisms, and psychophysiological implications. Psychophysiology 1993, 30, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Halámek, J.; Kára, T.; Jurák, P.; Souček, M.; Francis, D.P.; Davies, L.C.; Shen, W.K.; Coats, A.J.; Novák, M.; Nováková, Z.; et al. Variability of phase shift between blood pressure and heart rate fluctuations: A marker of short-term circulation control. Circulation 2003, 108, 292–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammer, P.E.; Saul, J.P. Resonance in a mathematical model of baroreflex control: Arterial blood pressure waves accompanying postural stress. Am. J. Physiol. Integr. Comp. Physiol. 2005, 288, R1637–R1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenza, G.; Lanata, A.; Scilingo, E.P. The role of nonlinear dynamics in affective valence and arousal recognition. IEEE Trans. Affect. Comput. 2011, 3, 237–249. [Google Scholar] [CrossRef]
- Shea, S.A.; Walter, J.; Murphy, K.; Guz, A. Evidence for individuality of breathing patterns in resting healthy man. Respir. Physiol. 1987, 68, 331–344. [Google Scholar] [CrossRef]
- Benchetrit, G.; Shea, S.A.; Dinh, T.P.; Bodocco, S.; Baconnier, P.; Guz, A. Individuality of breathing patterns in adults assessed over time. Respir. Physiol. 1989, 75, 199–209. [Google Scholar] [CrossRef]
- Cysarz, D.; Büssing, A. Cardiorespiratory synchronization during Zen meditation. Eur. J. Appl. Physiol. 2005, 95, 88–95. [Google Scholar] [CrossRef]
- Khng, K.H. A better state-of-mind: Deep breathing reduces state anxiety and enhances test performance through regulating test cognitions in children. Cogn. Emot. 2017, 31, 1502–1510. [Google Scholar] [CrossRef]
- Perciavalle, V.; Blandini, M.; Fecarotta, P.; Buscemi, A.; Di Corrado, D.; Bertolo, L.; Fichera, F.; Coco, M. The role of deep breathing on stress. Neurol. Sci. 2017, 38, 451–458. [Google Scholar] [CrossRef]
- Priyanka, K. A Study to Assess the Effectiveness of Deep Breathing Exercise on Reduction of Anger Expression Among Adolescent Girls in Selected School at Vallioor. Ph.D. Thesis, Nehru Nursing College, Vallioor, India, 2016. [Google Scholar]
- Hayama, Y.; Inoue, T. The effects of deep breathing on ‘tension–anxiety’and fatigue in cancer patients undergoing adjuvant chemotherapy. Complement. Ther. Clin. Pract. 2012, 18, 94–98. [Google Scholar] [CrossRef]
- Malliani, A.; Pagani, M.; Lombardi, F.; Cerutti, S. Cardiovascular neural regulation explored in the frequency domain. Circulation 1991, 84, 482–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montano, N.; Ruscone, T.G.; Porta, A.; Lombardi, F.; Pagani, M.; Malliani, A. Power spectrum analysis of heart rate variability to assess the changes in sympathovagal balance during graded orthostatic tilt. Circulation 1994, 90, 1826–1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berntson, G.G.; Thomas Bigger, J., Jr.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef] [PubMed]
- Phongsuphap, S.; Pongsupap, Y.; Chandanamattha, P.; Lursinsap, C. Changes in heart rate variability during concentration meditation. Int. J. Cardiol. 2008, 130, 481–484. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Huh, H.J.; Kim, B.G.; Ryu, H.; Lee, H.S.; Kim, J.M.; Chung, H.T. Effects of Qi-training on heart rate variability. Am. J. Chin. Med. 2002, 30, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Vaschillo, E.G.; Vaschillo, B.; Lehrer, P.M. Characteristics of resonance in heart rate variability stimulated by biofeedback. Appl. Psychophysiol. Biofeedback 2006, 31, 129–142. [Google Scholar] [CrossRef]
- Castaldo, R.; Melillo, P.; Bracale, U.; Caserta, M.; Triassi, M.; Pecchia, L. Acute mental stress assessment via short term HRV analysis in healthy adults: A systematic review with meta-analysis. Biomed. Signal Process Control 2015, 18, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Seong, H.M.; Lee, J.S.; Shin, T.M.; Kim, W.S.; Yoon, Y.R. The Analysis of Mental Stress Using Time-Frequency Distribution of Heart Rate Variability Signal. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004; Volume 1, pp. 283–285. [Google Scholar]
- Borchini, R.; Veronesi, G.; Bonzini, M.; Gianfagna, F.; Dashi, O.; Ferrario, M.M. Heart rate variability frequency domain alterations among healthy nurses exposed to prolonged work stress. Int. J. Environ. Res. Public Health 2018, 15, 113. [Google Scholar] [CrossRef] [Green Version]
- Tu, P.C.; Cheng, W.C.; Hou, P.C.; Chang, Y.S. Effects of types of horticultural activity on the physical and mental state of elderly individuals. Int. J. Environ. Res. Public Health 2020, 17, 5225. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Optimal RSP | Non-Optimal RSP | Z | p |
|---|---|---|---|---|
| M (SD) | M (SD) | |||
| VLF (%) | 8.1359 (7.6382) | 8.5199 (5.9367) | −1.062 | 0.288 |
| LF (%) | 27.7045 (19.4434) | 44.6741 (16.2995) | −6.505 | 0.000 |
| HF (%) | 64.1596 (22.2799) | 46.806 (17.6863) | −6.316 | 0.000 |
| VLF Power | 0.0004 (0.0004) | 0.0005 (0.0003) | −3.246 | 0.001 |
| LF Power | 0.0016 (0.0018) | 0.0029 (0.0018) | −6.203 | 0.000 |
| HF Power | 0.0043 (0.0038) | 0.0035 (0.0029) | −2.644 | 0.008 |
| LF/HF ratio | 1.1185 (3.021) | 3.2043 (3.9283) | −6.791 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-N.; Whang, M.-C.; Kang, B.-G. Process Design for Optimized Respiration Identification Based on Heart Rate Variability for Efficient Respiratory Sinus Arrhythmia Biofeedback. Int. J. Environ. Res. Public Health 2022, 19, 2087. https://doi.org/10.3390/ijerph19042087
Lee J-N, Whang M-C, Kang B-G. Process Design for Optimized Respiration Identification Based on Heart Rate Variability for Efficient Respiratory Sinus Arrhythmia Biofeedback. International Journal of Environmental Research and Public Health. 2022; 19(4):2087. https://doi.org/10.3390/ijerph19042087
Chicago/Turabian StyleLee, Jung-Nyun, Min-Cheol Whang, and Bong-Gu Kang. 2022. "Process Design for Optimized Respiration Identification Based on Heart Rate Variability for Efficient Respiratory Sinus Arrhythmia Biofeedback" International Journal of Environmental Research and Public Health 19, no. 4: 2087. https://doi.org/10.3390/ijerph19042087
APA StyleLee, J.-N., Whang, M.-C., & Kang, B.-G. (2022). Process Design for Optimized Respiration Identification Based on Heart Rate Variability for Efficient Respiratory Sinus Arrhythmia Biofeedback. International Journal of Environmental Research and Public Health, 19(4), 2087. https://doi.org/10.3390/ijerph19042087