
Burnout and Health Issues among Prehospital Personnel in Taiwan Fire Departments during a Sudden Spike in Community COVID-19 Cases: A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participant Characteristics
3.2. Characteristics and Mental Health-Related Status
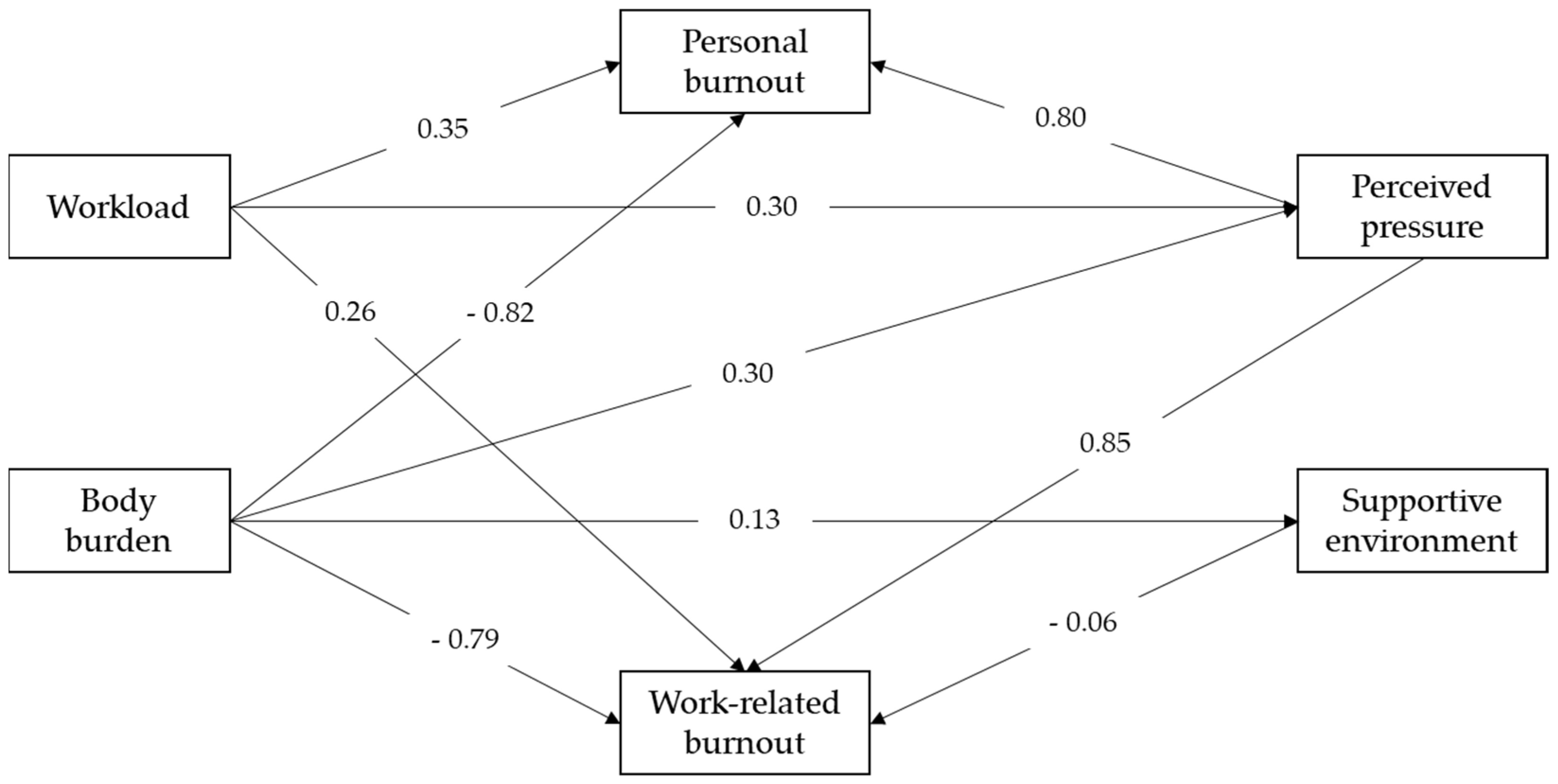
3.3. Association of Burnout and Observed Factors
3.4. Qualitative Feedback from Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, Y.T.; Chen, G.; Tang, C. Countermeasures for EMS personnel to reduce heat stress when wearing PPE during COVID-19 pandemic. J. Paramed. Emerg. Response 2021, 2, 6–12. [Google Scholar]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Dell’Oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A.; et al. Professional Quality of Life and Mental Health Outcomes among Health Care Workers Exposed to SARS-CoV-2 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 6180. [Google Scholar] [CrossRef] [PubMed]
- De Brier, N.; Stroobants, S.; Vandekerckhove, P.; De Buck, E. Factors affecting mental health of health care workers during coronavirus disease outbreaks (SARS, MERS & COVID-19): A rapid systematic review. PLoS ONE 2020, 15, e0244052. [Google Scholar] [CrossRef]
- Pappa, S.; Barnett, J.; Berges, I.; Sakkas, N. Tired, Worried and Burned Out, but Still Resilient: A Cross-Sectional Study of Mental Health Workers in the UK during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4457. [Google Scholar] [CrossRef] [PubMed]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef] [PubMed]
- ElGindi, H.; Shalaby, R.; Gusnowski, A.; Vuong, W.; Surood, S.; Hrabok, M.; Greenshaw, A.J.; Agyapong, V. Mental health impact of COVID-19 pandemic among physicians, nurses, and other healthcare providers, in the province of Alberta (Preprint). JMIR Form. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Vanhaecht, K.; Seys, D.; Bruyneel, L.; Cox, B.; Kaesemans, G.; Cloet, M.; Broeck, K.V.D.; Cools, O.; De Witte, A.; Lowet, K.; et al. COVID-19 is having a destructive impact on health-care workers’ mental well-being. Int. J. Qual. Health Care 2021, 33, mzaa158. [Google Scholar] [CrossRef]
- Wong, L.P.; Hung, C.-C.; Alias, H.; Lee, T.S.-H. Anxiety symptoms and preventive measures during the COVID-19 outbreak in Taiwan. BMC Psychiatry 2020, 20, 376. [Google Scholar] [CrossRef]
- Robles, R.; Rodríguez, E.; Vega-Ramírez, H.; Álvarez-Icaza, D.; Madrigal, E.; Durand, S.; Morales-Chainé, S.; Astudillo, C.; Real-Ramírez, J.; Medina-Mora, M.-E.; et al. Mental health problems among healthcare workers involved with the COVID-19 outbreak. Rev. Bras. Psiquiatr. 2021, 43, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Evanoff, B.A.; Strickland, J.R.; Dale, A.M.; Hayibor, L.; Page, E.; Duncan, J.G.; Kannampallil, T.; Gray, D.L. Work-Related and Personal Factors Associated with Mental Well-Being During the COVID-19 Response: Survey of Health Care and Other Workers. J. Med. Internet Res. 2020, 22, e21366. [Google Scholar] [CrossRef] [PubMed]
- Awais, S.B.; Martins, R.S.; Khan, M.S. Paramedics in pandemics: Protecting the mental wellness of those behind enemy lines. Br. J. Psychiatry 2021, 218, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Buick, J.E.; Cheskes, S.; Feldman, M.; Verbeek, P.R.; Hillier, M.; Leong, Y.C.; Drennan, I.R. COVID-19: What paramedics need to know. Can. J. Emerg. Med. 2020, 22, 426–430. [Google Scholar] [CrossRef] [Green Version]
- National Fire Agency of Taiwan. 2020 Total Number of EMTs in Fire Departments in Taiwan. 2020. Available online: https://www.nfa.gov.tw/cht/index.php?code=list&flag=detail&ids=221&article_id=9543 (accessed on 31 August 2021).
- Yeh, W.Y.; Cheng, Y.; Chen, C.J.; Hu, P.; Kristensen, T.S. Psychometric properties of the Chinese version of the Copenhagan Burnout Inventory among Taiwanese employees from two enterprises. Int. J. Behav. Med. 2007, 14, 1–8. [Google Scholar] [CrossRef]
- Feng, M.-C.; Wu, H.-C.; Lin, H.-T.; Lei, L.; Chao, C.-L.; Lu, C.-M.; Yang, W.-P. Exploring the Stress, Psychological Distress, and Stress-relief Strategies of Taiwan Nursing Staffs Facing the Global Outbreak of COVID-19. Hu Li Za Zhi J. Nurs. 2020, 67, 64–74. [Google Scholar]
- Fernandez, R.; Lord, H.; Halcomb, E.; Moxham, L.; Middleton, R.; Alananzeh, I.; Ellwood, L. Implications for COVID-19: A systematic review of nurses’ experiences of working in acute care hospital settings during a respiratory pandemic. Int. J. Nurs. Stud. 2020, 111, 103637. [Google Scholar] [CrossRef] [PubMed]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Athanasiou, N.; Sakkas, N.; Patrinos, S.; Sakka, E.; Barmparessou, Z.; Tsikrika, S.; Adraktas, A.; Pataka, A.; Migdalis, I.; et al. From Recession to Depression? Prevalence and Correlates of Depression, Anxiety, Traumatic Stress and Burnout in Healthcare Workers during the COVID-19 Pandemic in Greece: A Multi-Center, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 2390. [Google Scholar] [CrossRef] [PubMed]
- Lovreglio, P.; Leso, V.; Riccardi, E.; Stufano, A.; Pacella, D.; Cagnazzo, F.; Ercolano, M.L.; Iavicoli, I. Coronavirus Disease (COVID-19) Pandemic: The Psychological Well-Being in a Cohort of Workers of a Multinational Company. Saf. Health Work 2021. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Frequency (%) | Mean ± SD |
|---|---|---|
| Age | 35.4 ± 6.5 | |
| Working experience (years) | 11.8 ± 6.8 | |
| Number of dependents | 2.1 ± 1.3 | |
| Gender | ||
| Male | 173 (92.5) | |
| Female | 14 (7.5) | |
| Marriage | ||
| Not married | 66 (35.3) | |
| Married | 118 (63.1) | |
| Divorced | 3 (1.6) | |
| Education | ||
| Diploma | 67 (35.8) | |
| Undergraduate | 76 (40.6) | |
| Postgraduate | 44 (23.5) | |
| EMTs Level | ||
| EMTs-2 | 112 (59.9) | |
| Paramedic | 75 (40.1) | |
| Service Unit | ||
| COVID-19 response units | 93 (49.8) | |
| Non-COVID-19 response units | 94 (50.2) | |
| Jurisdictions | ||
| New Taipei City | 73 (39.0) | |
| Taichung City | 31 (16.6) | |
| Kaohsiung City | 21 (11.2) | |
| Hsinchu City | 13 (7.0) | |
| Tainan City | 12 (6.4) | |
| Taipei City | 11 (5.9) | |
| Taoyuan City | 8 (4.3) | |
| Hsinchu County | 6 (3.2) | |
| Others | 12 (6.4) | |
| Financial status | ||
| Below the poverty line | 9 (4.8) | |
| Middle class | 151 (80.7) | |
| Upper class | 27 (14.4) | |
| Religion | ||
| No religion | 101 (54.0) | |
| Buddhist | 25 (13.4) | |
| Taoist | 48 (25.7) | |
| Christian | 8 (4.3) | |
| Others | 5 (2.7) | |
| Smoking habit | … | |
| Non-smoker | 156 (83.4) | |
| Less than 1 pack per week | 14 (7.5) | |
| 1–2 packs per week | 12 (6.4) | |
| More than 1 pack per day | 5 (2.7) | |
| Alcohol consumption habit | … | |
| No drinking habit | 63 (33.7) | |
| Drink occasionally | 113 (60.4) | |
| Drink more than 3 times per week | 11 (5.9) | |
| Exercise habit | ||
| No exercise habit | 36 (19.3) | |
| 1–2 times per week | 100 (53.5) | |
| More than 3 times per week | 51 (27.3) |
| Variables | Mean ± SD |
|---|---|
| Personal-related burnout | 55.9 ± 22.4 |
| Work-related burnout | 51.3 ± 22.0 |
| Workload | 83.1 ± 11.2 |
| Body burden | 64.7 ± 6.5 |
| Perceived pressure | 72.6 ± 13.4 |
| Supportive environment | 69.7 ± 11.5 |
| Variables | n | Workload | p | Body Burden | p | Personal Burnout | p | Work Burnout | p | Perceived Pressure | p | Supportive Environment | p |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | |||||||||||||
| Male | 173 | 83.17 ± 11.4 | 0.742 | 64.8 ± 6.6 | 0.617 | 56.6 ± 21.8 | 0.149 | 51.9 ± 21.5 | 0.189 | 72.9 ± 13.5 | 0.383 | 70.0 ± 11.4 | 0.249 |
| Female | 14 | 82.1 ± 9.5 | 63.8 ± 6.2 | 47.6 ± 28.1 | 43.8 ± 26.7 | 69.6 ± 11.6 | 66.3 ± 11.8 | ||||||
| Marriage | |||||||||||||
| Not married | 66 | 84.4 ± 9.3 | 0.456 | 64.1 ± 4.8 | 0.619 | 53.3 ± 22.3 | 0.303 | 48.5 ± 21.3 | 0.096 | 71.0 ± 10.8 | 0.088 | 67.3 ± 11.8 | 0.088 |
| Married | 118 | 82.4 ± 12.2 | 65.1 ± 7.4 | 57.6 ± 22.3 | 53.3 ± 22.0 | 73.9 ± 14.4 | 70.9 ± 11.2 | ||||||
| Divorced | 3 | 80.0 ± 8.8 | 64.8 ± 5.5 | 44.4 ± 20.9 | 30.9 ± 26.8 | 59.6 ± 14.4 | 74.8 ± 5.1 | ||||||
| Education | |||||||||||||
| Diploma | 67 | 85.3 ± 9.8 | 0.093 | 64.5 ± 6.0 | 0.136 | 56.5 ± 19.4 | 0.608 | 52.8 ± 17.5 | 0.398 | 73.2 ± 10.9 | 0.335 | 69.9 ± 9.7 | 0.366 |
| Undergraduate | 76 | 81.2 ± 12.7 | 65.7 ± 6.8 | 57.1 ± 22.8 | 52.2 ± 23.6 | 73.6 ± 14.7 | 68.5 ± 11.7 | ||||||
| Postgraduate | 44 | 82.8 ± 10.3 | 63.3 ± 6.7 | 53.0 ± 25.8 | 47.4 ± 25.0 | 70.0 ± 14.4 | 71.6 ± 13.3 | ||||||
| EMTs level | |||||||||||||
| (1) EMTs-2 | 112 | 83.8 ± 11.4 | 0.257 | 64.8 ± 6.9 | 0.846 | 58.5 ± 22.9 | 0.048 * (1) > (2) | 53.3 ± 21.5 | 0.118 | 74.2 ± 13.0 | 0.055 | 70.1 ± 10.8 | 0.572 |
| (2) Paramedic | 75 | 81.9 ± 11.0 | 64.6 ± 6.0 | 52.0 ± 21.1 | 48.2 ± 22.3 | 70.3 ± 13.6 | 69.1 ± 12.4 | ||||||
| Service units | |||||||||||||
| (1) COVID-19 Units | 93 | 84.4 ± 10.1 | 0.008 * (1) > (2) | 66.2 ± 6.45 | 0.002 * (1) > (2) | 56.6 ± 21.0 | 0.113 | 51.4 ± 21.4 | 0.299 | 72.4 ± 13.1 | 0.112 | 70.9 ± 11.7 | 0.017 * (1) > (2) |
| (2) Non- COVID-19 Units | 94 | 82.6 ± 10.5 | 63.8 ± 9.0 | 56.7 ± 22.4 | 52.4 ± 21.7 | 73.9 ± 13.1 | 69.5 ± 10.3 | ||||||
| Jurisdictions | |||||||||||||
| (1) New Taipei City | 73 | 85.9 ± 9.1 | 0.004 * (1) > (2) (6) > (5) | 65.7 ± 6.9 | 0.130 | 58.9 ± 21.4 | 0.393 | 54.2 ± 22.2 | 0.758 | 73.2 ± 14.8 | 0.345 | 72.9 ± 10.3 | 0.002 * (1) > (2) (1) > (4) |
| (2) Taichung City | 31 | 78.3 ± 13.6 | 62.2 ± 5.4 | 50.8 ± 25.7 | 48.7 ± 21.7 | 69.1 ± 14.5 | 65.2 ± 11.5 | ||||||
| (3) Kaohsiung City | 21 | 83.0 ± 11.7 | 65.0 ± 5.5 | 59.1 ± 21.2 | 52.0 ± 22.0 | 77.3 ± 12.0 | 69.4 ± 12.1 | ||||||
| (4) Hsinchu City | 13 | 79.2 ± 10.3 | 64.1 ± 3.8 | 43.9 ± 17.1 | 43.4 ± 19.2 | 67.5 ± 8.1 | 61.5 ± 11.9 | ||||||
| (5) Tainan City | 12 | 75.0 ± 13.6 | 63.0 ± 4.7 | 61.1 ± 24.1 | 56.5 ± 21.4 | 78.2 ± 12.4 | 64.2 ± 8.5 | ||||||
| (6) Taipei City | 11 | 90.0 ± 9.7 | 68.5 ± 8.8 | 57.9 ± 22.6 | 47.0 ± 25.3 | 71.2 ± 14.9 | 73.1 ± 16.3 | ||||||
| (7) Taoyuan City | 8 | 83.3 ± 9.7 | 64.0 ± 6.5 | 50.0 ± 31.9 | 46.4 ± 31.1 | 73.3 ± 9.9 | 72.5 ± 6.4 | ||||||
| (8) Hsinchu County | 6 | 85.0 ± 4.0 | 66.3 ± 7.5 | 54.1 ± 12.3 | 52.9 ± 12.8 | 71.5 ± 7.9 | 76.6 ± 10.0 | ||||||
| (9) Others | 12 | 83.0 ± 13.5 | 62.8 ± 8.4 | 56.2 ± 19.5 | 48.8 ± 19.6 | 71.9 ± 10.1 | 68.8 ± 8.3 | ||||||
| Financial status | |||||||||||||
| (1) Below the poverty line | 9 | 78.5 ± 16.9 | 0.183 | 65.0 ± 10.3 | 0.709 | 66.6 ± 28.3 | 0.101 | 67.4 ± 25.2 | 0.028 * (1) > (3) | 81.2 ± 13.8 | 0.031 * (1) > (3) | 71.1 ± 14.0 | 0.698 |
| (2) Middle class | 151 | 83.8 ± 10.8 | 64.9 ± 6.0 | 56.5 ± 21.7 | 51.49 ± 21.0 | 73.0 ± 12.6 | 69.4 ± 11.8 | ||||||
| (3) Upper class | 27 | 80.6 ± 11.0 | 63.7 ± 8.0 | 49.2 ± 23.1 | 44.9 ± 24.2 | 68.0 ± 16.0 | 71.2 ± 8.7 | ||||||
| Religion | |||||||||||||
| No religion | 101 | 82.4 ± 11.5 | 0.643 | 64.5 ± 7.1 | 0.304 | 54.6 ± 21.5 | 0.065 | 50.4 ± 22.2 | 0.072 | 71.4 ± 13.9 | 0.054 | 70.1 ± 10.3 | 0.146 |
| Buddhist | 25 | 83.0 ± 10.5 | 64.0 ± 4.8 | 49.8 ± 18.1 | 45.0 ± 18.4 | 68.7 ± 9.0 | 73.9 ± 13.5 | ||||||
| Taoism | 48 | 84.3 ± 11.7 | 64.9 ± 6.4 | 61.6 ± 23.8 | 56.5 ± 20.9 | 77.0 ± 13.8 | 67.8 ± 12.2 | ||||||
| Christian | 8 | 80.8 ± 8.8 | 64.5 ± 2.7 | 47.9 ± 29.4 | 41.9 ± 28.1 | 71.2 ± 10.1 | 68.3 ± 8.1 | ||||||
| Others | 5 | 88.6 ± 9.3 | 70.9 ± 4.6 | 71.6 ± 20.7 | 65.7 ± 23.2 | 78.6 ± 13.2 | 62.6 ± 16.9 | ||||||
| Smoking habit | |||||||||||||
| Non-smoker | 156 | 83.0 ± 11.3 | 0.608 | 64.6 ± 6.6 | 0.774 | 55.8 ± 22.5 | 0.480 | 51.6 ± 22.0 | 0.217 | 72.2 ± 13.6 | 0.394 | 69.6 ± 11.2 | 0.505 |
| Less than 1 pack per week | 14 | 82.3 ± 11.2 | 64.1 ± 6.1 | 54.7 ± 21.4 | 49.7 ± 21.9 | 75.6 ± 12.9 | 68.4 ± 16.7 | ||||||
| 1–2 packs per week | 12 | 86.3 ± 10.7 | 66.3 ± 6.8 | 52.7 ± 22.0 | 42.8 ± 20.9 | 77.4 ± 11.8 | 74.0 ± 8.2 | ||||||
| More than 1 pack per day | 5 | 78.6 ± 13.2 | 66.1 ± 8.1 | 70.8 ± 21.2 | 67.1 ± 20.4 | 68.0 ± 7.8 | 66.2 ± 5.7 | ||||||
| Alcohol consumption habit | |||||||||||||
| No drinking habit | 63 | 84.0 ± 11.6 | 0.251 | 62.8 ± 6.8 | 0.022 * | 52.5 ± 24.3 | 0.319 | 47.9 ± 24.2 | 0.320 | 69.6 ± 14.0 | 0.039 * | 70.6 ± 10.6 | 0.503 |
| Drink occasionally | 113 | 83.0 ± 10.6 | 65.6 ± 6.2 | 57.8 ± 21.2 | 53.1 ± 20.9 | 74.7 ± 13.1 | 69.0 ± 12.1 | ||||||
| Drink more than 3 times per week | 11 | 77.8 ± 15.0 | 65.9 ± 6.8 | 56.0 ± 21.4 | 51.2 ± 18.2 | 69.6 ± 8.2 | 72.3 ± 9.2 | ||||||
| Exercise habit | |||||||||||||
| (1) No exercise habit | 36 | 82.5 ± 12.8 | 0.762 | 65.0 ± 7.0 | 0.200 | 53.4 ± 21.1 | 0.001 * (2) > (3) | 48.9 ± 22.7 | 0.001 * (2) > (3) | 70.1 ± 12.9 | 0.005 * (2) > (3) | 70.0 ± 10.3 | 0.703 |
| (2) 1–2 times per week | 100 | 83.6 ± 11.1 | 65.3 ± 6.9 | 61.2 ± 21.7 | 56.5 ± 20.2 | 75.6 ± 13.3 | 69.1 ± 12.5 | ||||||
| (3) More than 3 times per week | 51 | 51 ± 82.3 | 63.3 ± 5.3 | 47.3 ± 21.9 | 42.7 ± 22.2 | 68.7 ± 12.7 | 70.8 ± 10.1 |
| Dependent Variable | Personal Burnout | ||||
|---|---|---|---|---|---|
| Independent Variable | Coefficient | Standardized Coefficient | T | p Value | |
| B | SE | β | |||
| Constant | −32.35 | 12.39 | |||
| Work experience | −0.42 | 0.19 | −0.13 | −2.15 | 0.03 |
| Workload | 0.19 | 0.07 | 0.09 | 2.68 | 0.008 |
| Work-related burnout | 0.83 | 0.04 | 0.82 | 17.30 | <0.001 |
| Dependent Variable | Work-Related Burnout | ||||
| Independent Variable | Coefficient | Standardized Coefficient | T | p Value | |
| B | SE | β | |||
| Constant | 10.36 | 12.12 | |||
| Perceived pressure | 0.25 | 0.07 | 0.15 | 3.43 | 0.001 |
| Personal burnout | 0.77 | 0.04 | 0.78 | 17.30 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.-T.; Hu, Y.-J. Burnout and Health Issues among Prehospital Personnel in Taiwan Fire Departments during a Sudden Spike in Community COVID-19 Cases: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 2257. https://doi.org/10.3390/ijerph19042257
Chang Y-T, Hu Y-J. Burnout and Health Issues among Prehospital Personnel in Taiwan Fire Departments during a Sudden Spike in Community COVID-19 Cases: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(4):2257. https://doi.org/10.3390/ijerph19042257
Chicago/Turabian StyleChang, Yu-Tung, and Yih-Jin Hu. 2022. "Burnout and Health Issues among Prehospital Personnel in Taiwan Fire Departments during a Sudden Spike in Community COVID-19 Cases: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 4: 2257. https://doi.org/10.3390/ijerph19042257
APA StyleChang, Y.-T., & Hu, Y.-J. (2022). Burnout and Health Issues among Prehospital Personnel in Taiwan Fire Departments during a Sudden Spike in Community COVID-19 Cases: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(4), 2257. https://doi.org/10.3390/ijerph19042257