



Determinants of Dietary Vitamin D Intake in Population-Based Cohort Sample of Polish Female Adolescents


Abstract
:1. Introduction
2. Materials and Methods
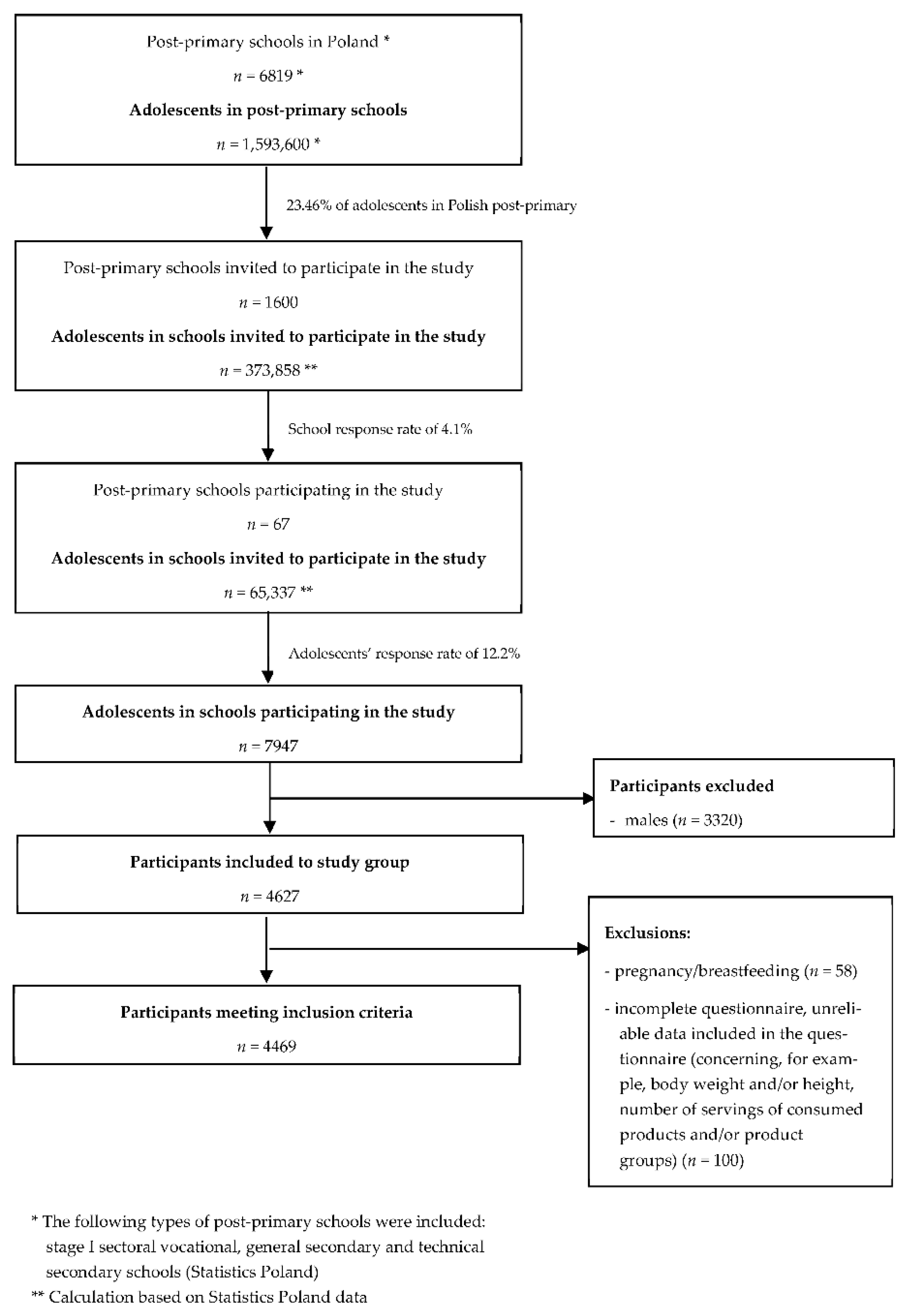
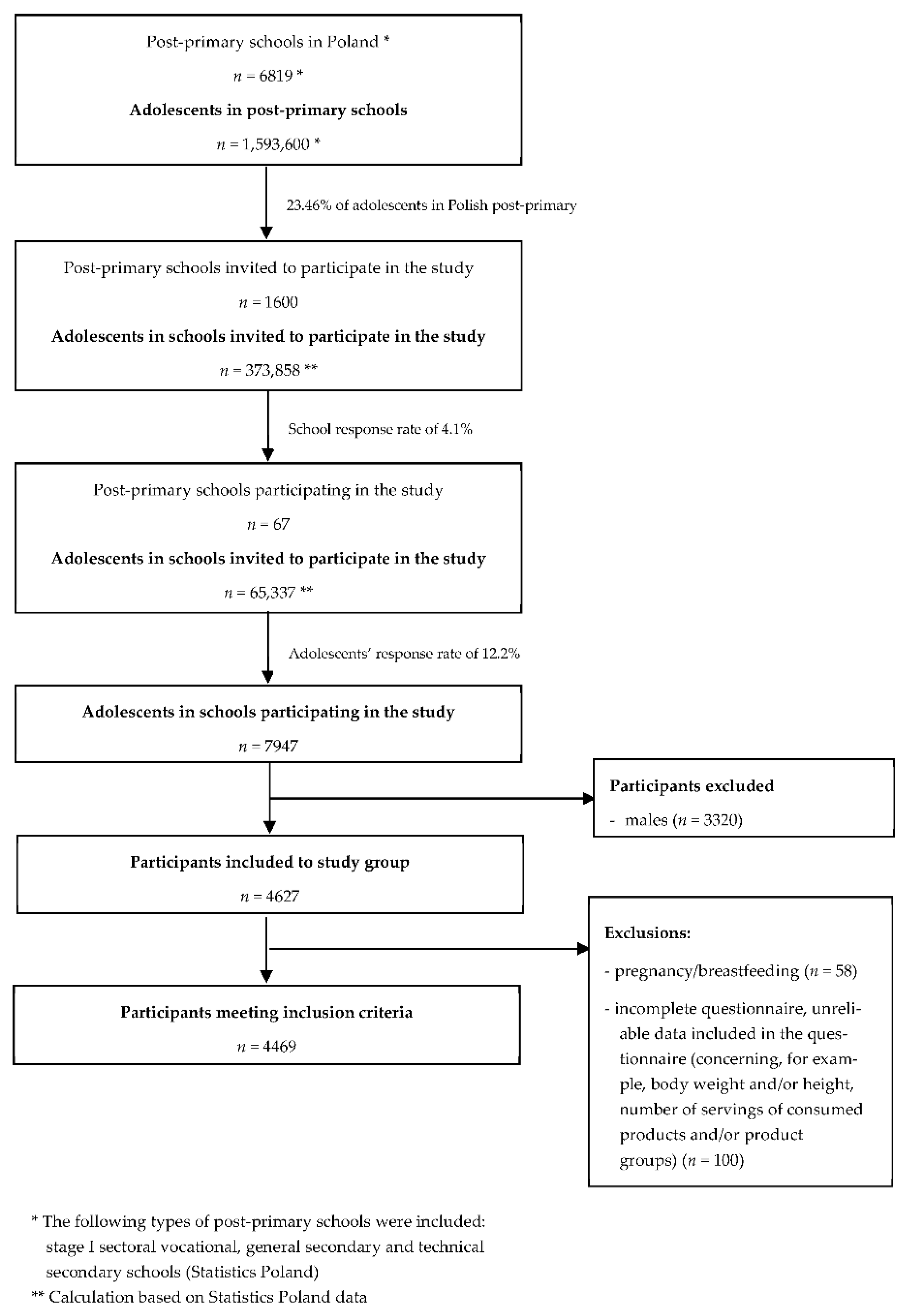
2.1. Study Population
2.2. Applied Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Study Group Characteristics
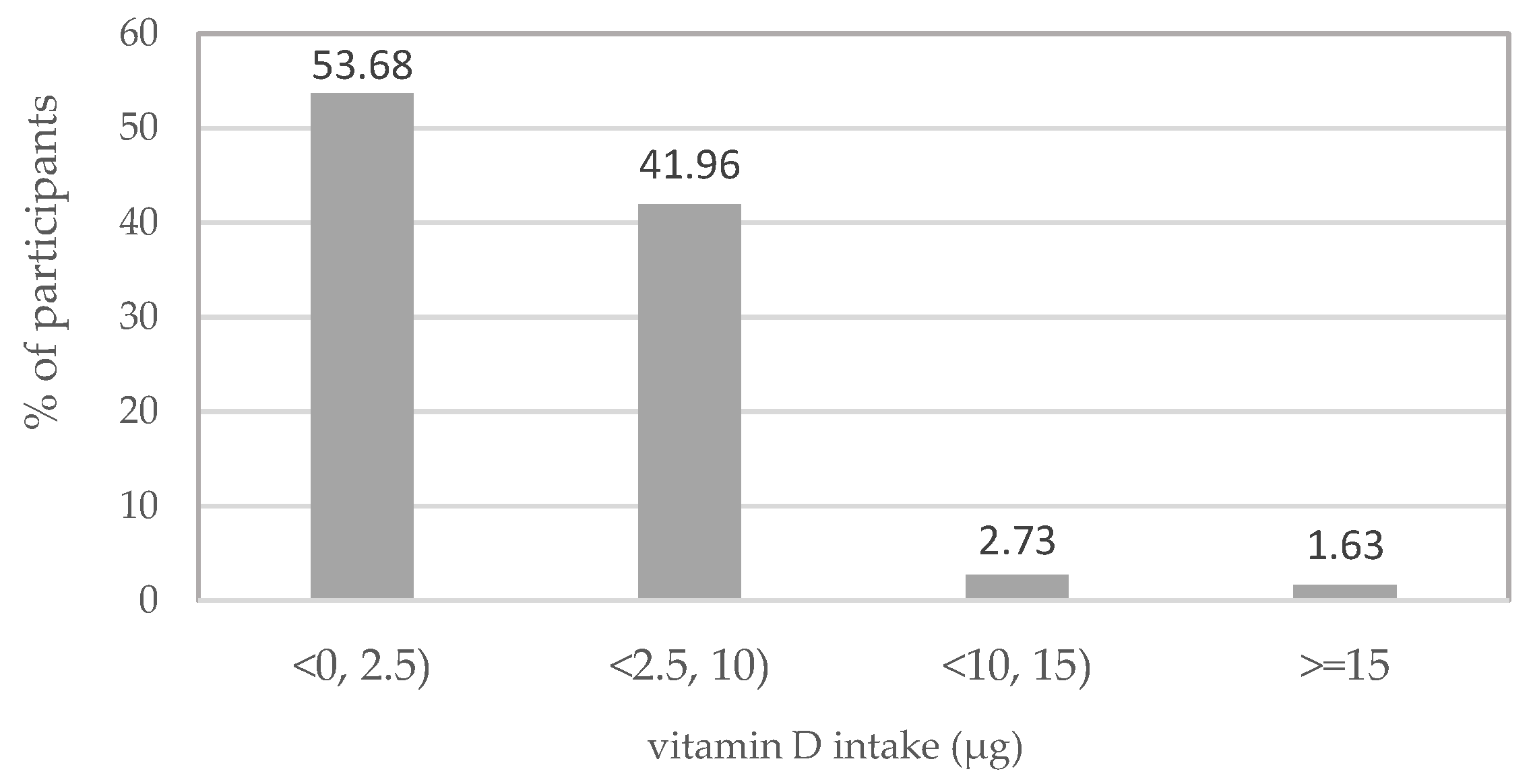
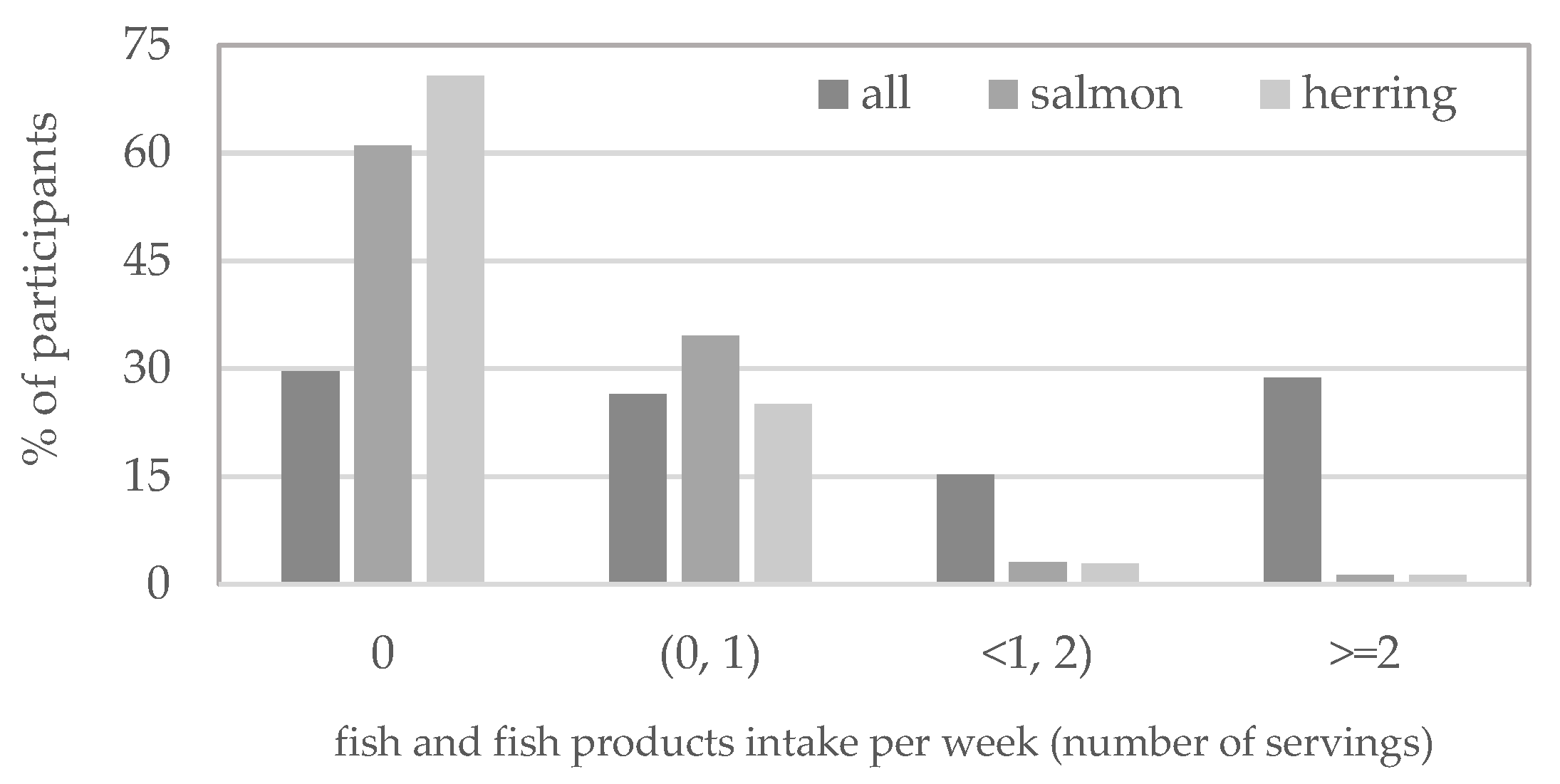
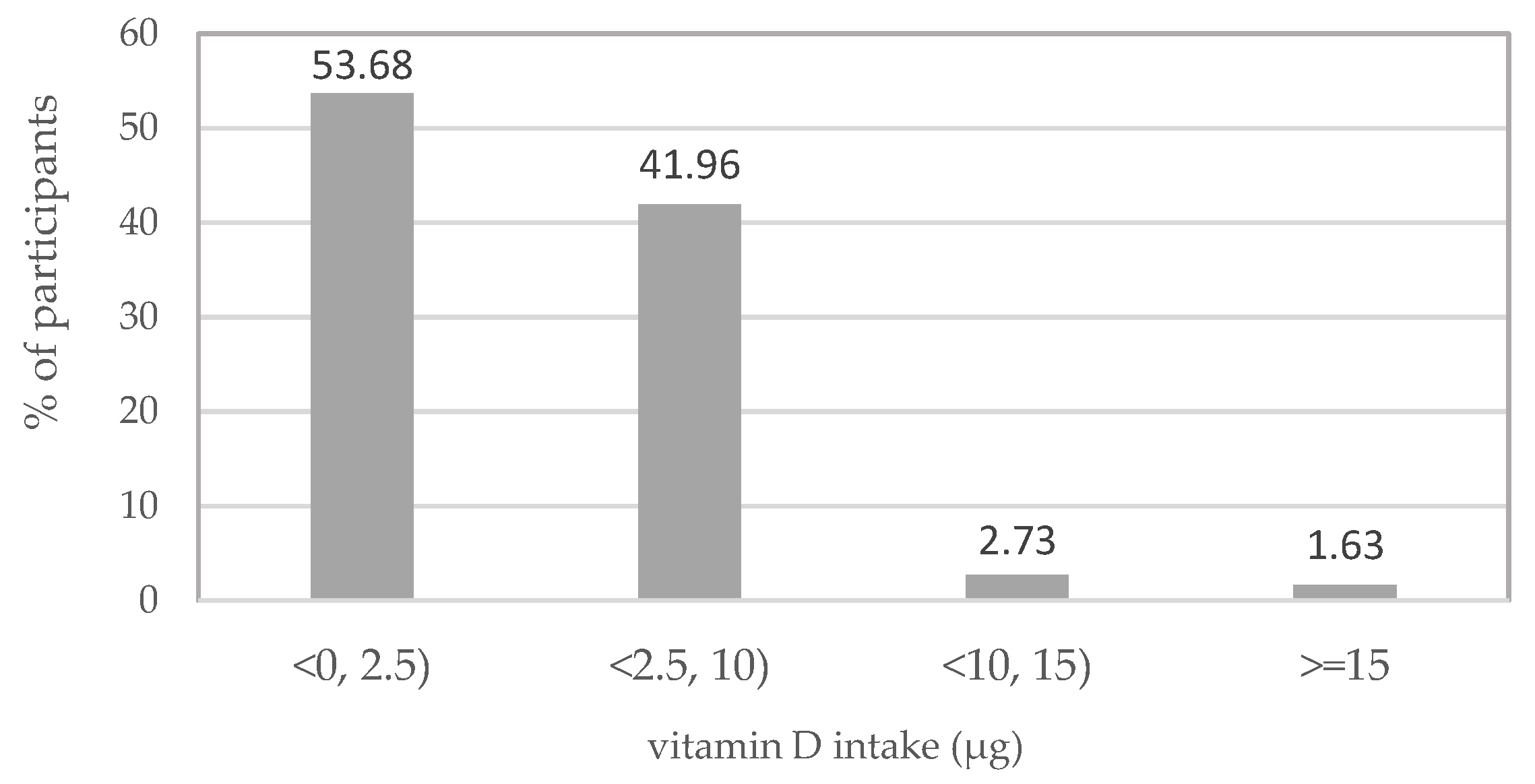
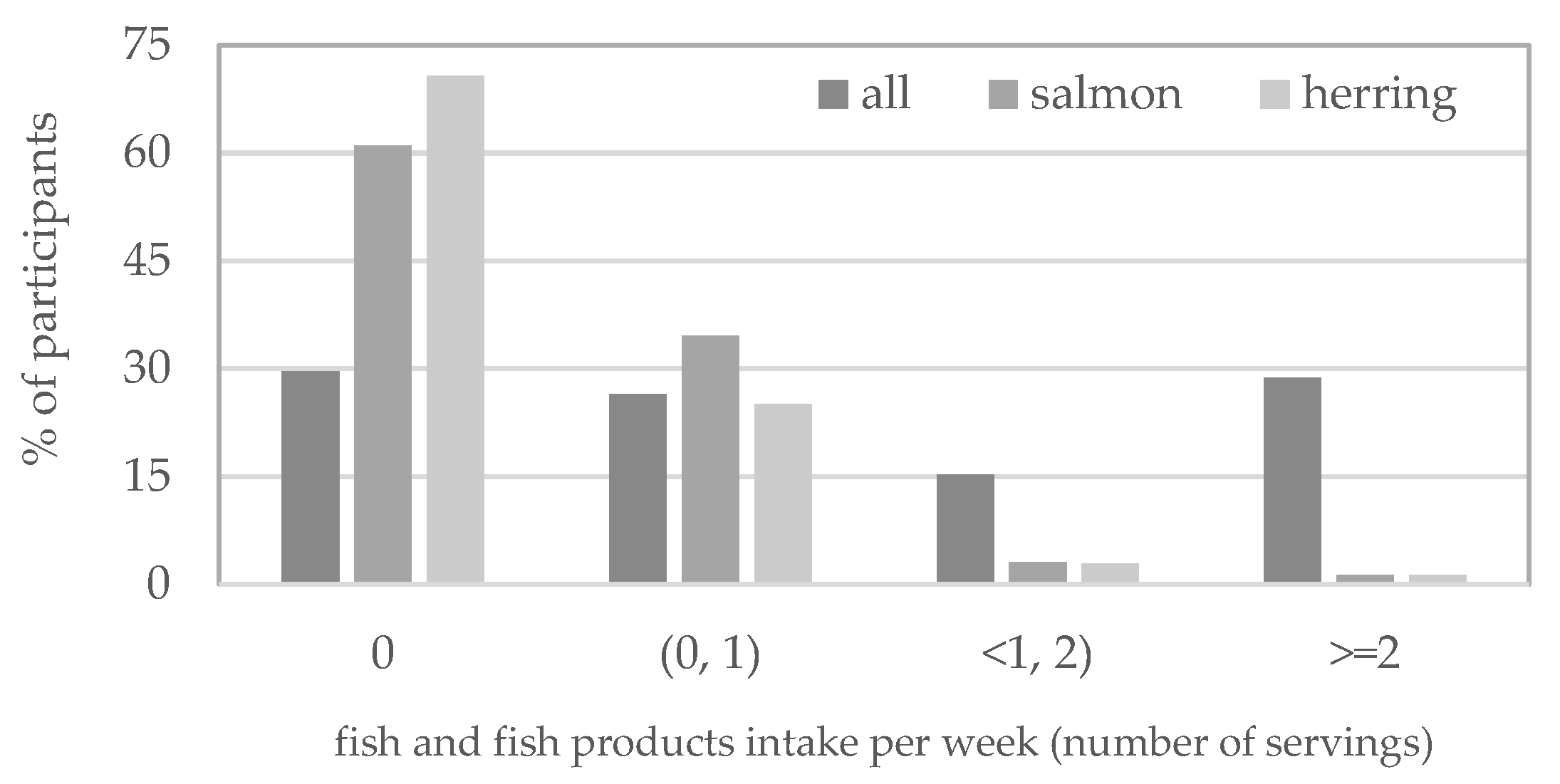
3.2. Dietary Vitamin D Intake and Its Sources
3.3. Dietary Vitamin D Intake in Subgroups
3.3.1. Regions of Poland and Vitamin D Intake
3.3.2. Age and Vitamin D Intake
3.3.3. BMI Classification and Vitamin D Intake
3.3.4. Vitamin D Supplementation and Vitamin D Intake
3.3.5. Vegetarian or Vegan Diet and Vitamin D Intake
3.4. Correlations
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef] [PubMed]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.-H.; Fang, T.-C. The Pleiotropic Effect of Vitamin D. ISRN Nephrol. 2013, 2013, 898125. [Google Scholar] [CrossRef] [PubMed]
- Stöcklin, E.; Eggersdorfer, M. Vitamin D, an Essential Nutrient with Versatile Functions in Nearly all Organs. Int. J. Vitam. Nutr. Res. 2013, 83, 92–100. [Google Scholar] [CrossRef]
- Caprio, M.; Infante, M.; Calanchini, M.; Mammi, C.; Fabbri, A. Vitamin D: Not just the bone. Evidence for beneficial pleiotropic extraskeletal effects. Eat. Weight. Disord. 2017, 22, 27–41. [Google Scholar] [CrossRef]
- Zmijewski, M.A.; Carlberg, C. Vitamin D receptor(s): In the nucleus but also at membranes? Exp. Dermatol. 2020, 29, 876–884. [Google Scholar] [CrossRef]
- Christodoulou, S.; Goula, T.; Ververidis, A.; Drosos, G. Vitamin D and Bone Disease. BioMed Res. Int. 2012, 2013, 396541. [Google Scholar] [CrossRef]
- Cannell, J.; Grant, W.B.; Holick, M.F. Vitamin D and inflammation. Dermato-Endocrinology 2014, 6, e983401. [Google Scholar] [CrossRef]
- Skrobot, A.; Demkow, U.; Wachowska, M. Immunomodulatory Role of Vitamin D: A Review. Adv. Exp. Med. Biol. 2018, 1108, 13–23. [Google Scholar] [CrossRef]
- Fletcher, J.; Bishop, E.L.; Harrison, S.R.; Swift, A.; Cooper, S.C.; Dimeloe, S.K.; Raza, K.; Hewison, M. Autoimmune disease and interconnections with vitamin D. Endocr. Connect. 2022, 11, e210554. [Google Scholar] [CrossRef]
- De Almeida, L.F. Vitamin D Actions on Cell Differentiation, Proliferation and Inflammation. Int. J. Complement. Altern. Med. 2017, 6, 00201. [Google Scholar] [CrossRef]
- Manucha, W.; Juncos, L.I. The protective role of vitamin D on the heart and the kidney. Ther. Adv. Cardiovasc. Dis. 2017, 11, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Jorge, A.J.L.; Cordeiro, J.R.; Rosa, M.L.G.; Bianchi, D.B.C. Vitamin D Deficiency and Cardiovascular Diseases. Int. J. Cardiovasc. Sci. 2018, 31, 422–432. [Google Scholar] [CrossRef]
- Bivona, G.; Gambino, C.M.; Iacolino, G.; Ciaccio, M. Vitamin D and the nervous system. Neurol. Res. 2019, 41, 827–835. [Google Scholar] [CrossRef]
- Mpandzou, G.; Ben Haddou, E.A.; Regragui, W.; Benomar, A.; Yahyaoui, M. Vitamin D deficiency and its role in neurological conditions: A review. Rev. Neurol. 2016, 172, 109–122. [Google Scholar] [CrossRef]
- Pham, V.T.; Dold, S.; Rehman, A.; Bird, J.K.; Steinert, R.E. Vitamins, the gut microbiome and gastrointestinal health in humans. Nutr. Res. 2021, 95, 35–53. [Google Scholar] [CrossRef]
- Chen, Y.; Zhi, X. Roles of Vitamin D in Reproductive Systems and Assisted Reproductive Technology. Endocrinology 2020, 161, bqaa023. [Google Scholar] [CrossRef]
- Mahomed, A.G. Vitamin D in respiratory diseases. S. Afr. Respir. J. 2017, 23, 14–18. [Google Scholar] [CrossRef]
- Mondul, A.M.; Weinstein, S.J.; Layne, T.M.; Albanes, D. Vitamin D and Cancer Risk and Mortality: State of the Science, Gaps, and Challenges. Epidemiol. Rev. 2017, 39, 28–48. [Google Scholar] [CrossRef]
- Vranić, L.; Mikolašević, I.; Milić, S. Vitamin D Deficiency: Consequence or Cause of Obesity? Medicina 2019, 55, 541. [Google Scholar] [CrossRef] [Green Version]
- Ghozali, N.M.; Giribabu, N.; Salleh, N. Mechanisms Linking Vitamin D Deficiency to Impaired Metabolism: An Overview. Int. J. Endocrinol. 2022, 2022, 6453882. [Google Scholar] [CrossRef]
- E Souza, C.L.; De Sá, L.B.P.C.; Rocha, D.R.T.W.; Arbex, A.K. Vitamin D and Diabetes Mellitus: A Review. Open J. Endocr. Metab. Dis. 2016, 6, 1–7. [Google Scholar] [CrossRef]
- Bollen, S.E.; Bass, J.J.; Fujita, S.; Wilkinson, D.; Hewison, M.; Atherton, P.J. The Vitamin D/Vitamin D receptor (VDR) axis in muscle atrophy and sarcopenia. Cell. Signal. 2022, 96, 110355. [Google Scholar] [CrossRef] [PubMed]
- Berridge, M.J. Vitamin D and Depression: Cellular and Regulatory Mechanisms. Pharmacol. Rev. 2017, 69, 80–92. [Google Scholar] [CrossRef]
- Dominguez, L.; Farruggia, M.; Veronese, N.; Barbagallo, M. Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment. Metabolites 2021, 11, 255. [Google Scholar] [CrossRef] [PubMed]
- Saponaro, F.; Saba, A.; Zucchi, R. An Update on Vitamin D Metabolism. Int. J. Mol. Sci. 2020, 21, 6573. [Google Scholar] [CrossRef]
- Hilger, J.; Friedel, A.; Herr, R.; Rausch, T.; Roos, F.; Wahl, D.A.; Pierroz, D.D.; Weber, P.; Hoffmann, K. A systematic review of vitamin D status in populations worldwide. Br. J. Nutr. 2014, 111, 23–45. [Google Scholar] [CrossRef]
- Cashman, K.D. Global differences in vitamin D status and dietary intake: A review of the data. Endocr. Connect. 2022, 11, e210282. [Google Scholar] [CrossRef]
- Spiro, A.; Buttriss, J.L. Vitamin D: An overview of vitamin D status and intake in Europe. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [Green Version]
- Lips, P.; Cashman, K.D.; Lamberg-Allardt, C.; Bischoff-Ferrari, H.A.; Obermayer-Pietsch, B.; Bianchi, M.L.; Stepan, J.; El-Hajj Fuleihan, G.; Bouillon, R. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: A position statement of the European Calcified Tissue Society. Eur. J. Endocrinol. 2019, 180, P23–P54. [Google Scholar] [CrossRef] [PubMed]
- Rusińska, A.; Płudowski, P.; Walczak, M.; Borszewska-Kornacka, M.K.; Bossowski, A.; Chlebna-Sokół, D.; Czech-Kowalska, J.; Dobrzańska, A.; Franek, E.; Helwich, E.; et al. Vitamin D Supplementation Guidelines for General Population and Groups at Risk of Vitamin D Deficiency in Poland—Recommendations of the Polish Society of Pediatric Endocrinology and Diabetes and the Expert Panel With Participation of National Specialist Consultants and Representatives of Scientific Societies—2018 Update. Front. Endocrinol. 2018, 9, 246. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Berisha, A.T.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Niedermaier, T.; Gredner, T.; Kuznia, S.; Schöttker, B.; Mons, U.; Lakerveld, J.; Ahrens, W.; Brenner, H.; On behalf of the PEN-Consortium. Vitamin D food fortification in European countries: The underused potential to prevent cancer deaths. Eur. J. Epidemiol. 2022, 37, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; März, W.; Cashman, K.D.; Kiely, M.E.; Whiting, S.J.; Holick, M.F.; Grant, W.B.; Pludowski, P.; Hiligsmann, M.; Trummer, C.; et al. Rationale and Plan for Vitamin D Food Fortification: A Review and Guidance Paper. Front. Endocrinol. 2018, 9, 373. [Google Scholar] [CrossRef]
- Tomaszewska, A.; Rustecka, A.; Lipińska-Opałka, A.; Piprek, R.P.; Kloc, M.; Kalicki, B.; Kubiak, J.Z. The Role of Vitamin D in COVID-19 and the Impact of Pandemic Restrictions on Vitamin D Blood Content. Front. Pharmacol. 2022, 13, 836738. [Google Scholar] [CrossRef]
- Rustecka, A.; Maret, J.; Drab, A.; Leszczyńska, M.; Tomaszewska, A.; Lipińska-Opałka, A.; Będzichowska, A.; Kalicki, B.; Kubiak, J. The Impact of COVID-19 Pandemic during 2020–2021 on the Vitamin D Serum Levels in the Paediatric Population in Warsaw, Poland. Nutrients 2021, 13, 1990. [Google Scholar] [CrossRef]
- Kołota, A.; Głąbska, D. COVID-19 Pandemic and Remote Education Contributes to Improved Nutritional Behaviors and Increased Screen Time in a Polish Population-Based Sample of Primary School Adolescents: Diet and Activity of Youth during COVID-19 (DAY-19) Study. Nutrients 2021, 13, 1596. [Google Scholar] [CrossRef]
- Mancini, C. Research Methods: Web Survey (CAWI). 2020. Available online: https://www.idsurvey.com/en/methods-web-survey-cawi/ (accessed on 25 August 2022).
- Głąbska, D.; Guzek, D.; Sidor, P.; Włodarek, D. Vitamin D Dietary Intake Questionnaire Validation Conducted among Young Polish Women. Nutrients 2016, 8, 36. [Google Scholar] [CrossRef]
- National Cancer Institute/National Institutes of Health (NCI/NIH). Register of NCI-Developed Short Diet Assessment Instruments. Available online: https://epi.grants.cancer.gov/diet/shortreg/instruments/ (accessed on 27 July 2022).
- Kunachowicz, H.; Nadolna, I.; Przygoda, B.; Iwanow, K. Tables of Composition and Nutritional Value of Food; PZWL: Warsaw, Poland, 2005. (In Polish) [Google Scholar]
- Jarosz, M.; Rychlik, E.; Stoś, K.; Wierzejska, R.; Wojtasik, A.; Charzewska, J.; Mojska, H.; Szponar, L.; Sajór, I.; Kłosiewicz-Latoszek, L.; et al. Nutrition Standards for the Polish Population; Polish National Food and Nutrition Institute: Warsaw, Poland, 2017; ISBN 978-83-86060-89-4. (In Polish) [Google Scholar]
- OLAF Calculator from OLAF Study. Available online: http://olaf.czd.pl/index.php?option=com_content&view=article&id=103:kalkulator (accessed on 29 July 2022).
- Kulaga, Z.; Litwin, M.; Tkaczyk, M.; Różdżyńska, A.; Barwicka, K.; Grajda, A.; Świąder, A.; Gurzkowska, B.; Napieralska, E.; Pan, H. The height-, weight-, and BMI-for-age of Polish school-aged children and adolescents relative to international and local growth references. BMC Public Health 2010, 10, 109. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Body Mass Index—BMI. Available online: http://www.euro.who.int/en/healthtopics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 29 July 2022).
- Płudowski, P.; Ducki, C.; Konstantynowicz, J.; Jaworski, M. Vitamin D status in Poland. Pol. Arch. Med. Wewn. 2016, 126, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Tripkovic, L.; Lanham-New, S.A.; Hart, K.H. Vitamin D in adolescence: Evidence-based dietary requirements and implications for public health policy. Proc. Nutr. Soc. 2017, 77, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Grant, W.; Bhattoa, H.P.; Bayer, M.; Povoroznyuk, V.; Rudenka, E.; Ramanau, H.; Varbiro, S.; Rudenka, A.; Karczmarewicz, E.; et al. Vitamin D Status in Central Europe. Int. J. Endocrinol. 2014, 2014, 589587. [Google Scholar] [CrossRef] [PubMed]
- Utri, Z.; Głąbska, D. Vitamin D Intake in a Population-Based Sample of Young Polish Women, Its Major Sources and the Possibility of Meeting the Recommendations. Foods 2020, 9, 1482. [Google Scholar] [CrossRef]
- Ponder, A.; Włodarek, D.; Krusiec, J. Evaluation of Nutrition in Women Who Attend Fitness Classes. Pol. J. Sports Med. 2016, 32, 231–239. [Google Scholar] [CrossRef]
- Kamińska, S.; Pikala, M.; Dziankowska-Zaborszczyk, E.; Bielecki, W.; Rębowska, E.; Kozakiewicz, K.; Nadrowski, P.; Drygas, W.; Kwaśniewska, M. Vitamin D—Dietary intake, supplementation and metabolic status of Polish adults. Int. J. Occup. Med. Environ. Health 2020, 33, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Lebiedzińska, A.; Rypina, M.; Czaja, J.; Petrykowska, K.; Szefer, P. Assessment of vitamin D content in daily food rations of adult Poles. Bromat. Chem. Toksykol. 2010, 43, 255–259. (In Polish) [Google Scholar]
- Ejsymont, J.; Zegan, M.; Michota-Katulska, E. Influence of vitamin D, B6, calcium and magnesium intake on premenstrual symptoms incidence. Probl. Hig. Epidemiol. 2014, 95, 765–771. (In Polish) [Google Scholar]
- Przysławski, J.; Bolesławska, I.; Kaźmierczak, A. Assessment of the level of consumption of selected vitamins among academic youth from the city of Poznań in comparison with the results of other studies. Bromat. Chem. Toksykol. 2012, 45, 183–1189. (In Polish) [Google Scholar]
- Mensink, G.B.M.; Fletcher, R.; Gurinović, M.; Huybrechts, I.; Lafay, L.; Serra-Majem, L.; Szponar, L.; Tetens, I.; Verkaik-Kloosterman, J.; Baka, A.; et al. Mapping low intake of micronutrients across Europe. Br. J. Nutr. 2013, 110, 755–773. [Google Scholar] [CrossRef]
- Elmadfa, I.; Meyer, A.; Nowak, V.; Hasenegger, V.; Putz, P.; Verstraeten, R.; Remaut-DeWinter, A.M.; Kolsteren, P.; Dostálová, J.; Dlouhý, P.; et al. European Nutrition and Health Report 2009. Forum Nutr. 2009, 62, 1–405. [Google Scholar] [CrossRef] [PubMed]
- Lichthammer, A.; Nagy, B.; Orbán, C.; Tóth, T.; Csajbók, R.; Molnár, S.; Tátrai-Németh, K.; Bálint, M.V. A comparative study of eating habits, calcium and Vitamin D intakes in the population of Central-Eastern European countries. New Med. 2015, 19, 66–70. [Google Scholar]
- Hribar, M.; Hristov, H.; Lavriša, Ž.; Seljak, B.K.; Gregorič, M.; Blaznik, U.; Žmitek, K.; Pravst, I. Vitamin D Intake in Slovenian Adolescents, Adults, and the Elderly Population. Nutrients 2021, 13, 3528. [Google Scholar] [CrossRef] [PubMed]
- Parel, N.; Bochud, M.; Rezzi, S.; Chatelan, A.; Chaparro, C.J. Vitamin D dietary intake and status in a sample of adolescents. Clin. Nutr. Open Sci. 2022, 43, 56–66. [Google Scholar] [CrossRef]
- Lehmann, U.; Gjessing, H.R.; Hirche, F.; Mueller-Belecke, A.; Gudbrandsen, O.A.; Ueland, P.M.; Mellgren, G.; Lauritzen, L.; Lindqvist, H.; Hansen, A.L.; et al. Efficacy of fish intake on vitamin D status: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2015, 102, 837–847. [Google Scholar] [CrossRef]
- Jarosz, M. Pyramid of Healthy Nutrition and Physical Activity for Children and Adolescents—Expert Comments. In-Stitute of Food and Nutrition. Available online: https://ncez.pzh.gov.pl/wp-content/uploads/2021/03/piramida-dla-dzieci-i-mlodziezy-opis.pdf (accessed on 4 August 2022). (In Polish)
- Myszkowska-Ryciak, J.; Harton, A.; Lange, E.; Laskowski, W.; Gajewska, D. Nutritional Behaviors of Polish Adolescents: Results of the Wise Nutrition—Healthy Generation Project. Nutrients 2019, 11, 1592. [Google Scholar] [CrossRef] [PubMed]
- Szczepańska, E.; Janota, B.; Janion, K. Selected lifestyle elements in adolescents attending high schools. Rocz. Panstw. Zakl. Hig. 2020, 71, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Przysławski, J.; Stelmach, M.; Grygiel-Górniak, B.; Mardas, M.; Walkowiak, J. Dietary Habits and Nutritional Status of Female Adolescents from the Great Poland Region. Pol. J. Food Nutr. Sci. 2011, 61, 73–78. [Google Scholar] [CrossRef]
- Pieniak, Z.; Verbeke, W.; Perez-Cueto, F.J.; Brunsø, K.; De Henauw, S. Fish consumption and its motives in households with versus without self-reported medical history of CVD: A consumer survey from five European countries. BMC Public Health 2008, 8, 306. [Google Scholar] [CrossRef]
- Hryszko, K. Rynek Ryb [Fish market] Nr 29/2018. Available online: https://www.ierigz.waw.pl/publikacje/analizy-rynkowe/rynek-ryb/23234,3,3,0,nr-29-2018-rynek-ryb.html (accessed on 4 August 2022). (In Polish).
- Knap, R.; Włodarczyk, K. Health and environmental determinants of consumer decisions and development trends in the consumption of fish products. Studia i Prace WNEiZ US 2016, 3, 165–175. [Google Scholar] [CrossRef]
- Kosicka-Gębska, M.; Ładecka, Z. Conditions and trends of fish consumption in Poland. Rocz. Nauk. Stowarzyszenia Ekon. Rol. I Agrobiz. 2012, XIV, 238–244. (In Polish) [Google Scholar]
- Tkaczewska, J.; Migdał, W.; Kulawik, P. Fish consumption consumer preferences. Komun. Ryb. 2014, 1, 10–14. (In Polish) [Google Scholar]
- Resolution No. 6/2021 of the Management Commission of the Fish Promotion Fund, Dated 29 July 2021, on the Adoption of the Promotion Strategy for the Fish Industry for 2022. Available online: https://bip.kowr.gov.pl/uploads/pliki/fundusze/fpr/strategia_prom_fp_ryb_2022_uchw6_2021.pdf (accessed on 19 September 2022). (In Polish)
- Welch, A.; Lund, E.; Amiano, P.; Dorronsoro, M.; Brustad, M.; Kumle, M.; Rodriguez, M.; Lasheras, C.; Janzon, L.; Jansson, J.; et al. Variability of fish consumption within the 10 European countries participating in the European Investigation into Cancer and Nutrition (EPIC) study. Public Health Nutr. 2002, 5, 1273–1285. [Google Scholar] [CrossRef] [PubMed]
- Cieślik, E.; Siembida, A.; Cieślik, I.; Zaglaniczna, K. Nutritional awareness of the consumption of fish and preserves among the Malopolska voivodeship‘s residents. Bromat. Chem. Toksykol. 2014, XLVII, 49–56. (In Polish) [Google Scholar]
- Sygnowska, E.; Waśkiewicz, A.; Głuszek, J.; Kwaśniewska, M.; Stepaniak, U.; Kozakiewicz, K.; Zdrojewski, T.; Rywik, S. Intake of consumed products by adults in the Polish population. Results of the WOBASZ program. Kardiol. Pol. 2005, 63 (Suppl. S4), S670–S676. (In Polish) [Google Scholar]
- Jeżewska-Zychowicz, M. The use of supplements among adolescents with the control of their use. Zyw. Człowieka Metab. 2007, 34, 481–485. (In Polish) [Google Scholar]
- Gil, M.; Ciszek, P.; Głodek, E. Evaluation of dietary supplements usage and knowledge on supplementation among secondary school students from Dębica. Bromat. Chem. Toksykol. 2013, XLVI, 194–199. [Google Scholar]
- Krejpcio, Z.; Staniek, H.; Chmielewska, A. Evaluation of the prevalence of dietary supplement consumption in selected groups of students. Probl. Hig. Epidemiol. 2013, 94, 622–625. [Google Scholar]
- Black, L.J.; Walton, J.; Flynn, A.; Kiely, M. Adequacy of vitamin D intakes in children and teenagers from the base diet, fortified foods and supplements. Public Health Nutr. 2013, 17, 721–731. [Google Scholar] [CrossRef]
- Del Ciampo, L.A.; Del Ciampo, I.R.L. Vegetarianism and veganism in adolescence: Benefits and risks. Integr. Food Nutr. Metab. 2019, 6, 1–4. [Google Scholar] [CrossRef]
- Patelakis, E.; Lage Barbosa, C.; Haftenberger, M.; Brettschneider, A.-K.; Lehmann, F.; Heide, K.; Frank, M.; Perlitz, H.; Richter, A.; Mensink, G.B.M. Prevalence of vegetarian diet among children and adolescents in Germany. Results from EsKiMo II. Ernahr. Umsch. 2019, 66, 85–91. [Google Scholar] [CrossRef]
- Alexy, U.; Fischer, M.; Weder, S.; Längler, A.; Michalsen, A.; Sputtek, A.; Keller, M. Nutrient Intake and Status of German Children and Adolescents Consuming Vegetarian, Vegan or Omnivore Diets: Results of the VeChi Youth Study. Nutrients 2021, 13, 1707. [Google Scholar] [CrossRef]
- Neufingerl, N.; Eilander, A. Nutrient Intake and Status in Adults Consuming Plant-Based Diets Compared to Meat-Eaters: A Systematic Review. Nutrients 2020, 14, 29. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Number (%) of Participants | p Value * | ||||
|---|---|---|---|---|---|---|
| Total | Quartiles of Vitamin D Intake from Food (µg/day) | |||||
| Q1 (0.01–1.32) | Q2 (1.33–2.32) | Q3 (2.33–4.03) | Q4 (4.04–29.34) | |||
| Total | 4469 (100.00) | 1117 (24.99) | 1116 (24.97) | 1118 (25.02) | 1118 (25.02) | |
| Region of Poland: | ||||||
| Central | 567 (12.67) | 149 (13.34) | 132 (11.83) | 144 (12.88) | 142 (12.70) | 0.00042 |
| Eastern | 914 (20.45) | 283 (25.34) | 197 (17.65) | 220 (19.68) | 214 (19.14) | |
| Northern | 1350 (30.21) | 299 (26.77) | 342 (30.64) | 325 (29.07) | 384 (34.35) | |
| North-Western | 396 (8.86) | 99 (8.86) | 110 (9.86) | 99 (8.86) | 88 (7.87) | |
| Southern | 993 (22.22) | 228 (20.41) | 266 (23.83) | 268 (23.97) | 231 (20.66) | |
| South-Western | 249 (5.57) | 59 (5.18) | 69 (6.18) | 62 (5.54) | 59 (5.28) | |
| Age: | 0.14204 | |||||
| 14–17 | 3131 (70.06) | 812 (72.69) | 764 (68.46) | 768 (68.69) | 787 (70.39) | |
| 18–20 | 1338 (29.94) | 305 (27.31) | 352 (31.54) | 350 (31.31) | 331 (29.61) | |
| Body Mass Index (BMI) classification: | ||||||
| Underweight | 445 (9.96) | 122 (10.92) | 108 (9.768) | 110 (9.84) | 105 (9.39) | 0.90188 |
| Normal weight | 3234 (72.36) | 796 (71.26) | 816 (73.12) | 805 (72.00) | 817 (73.08) | |
| Overweight | 927 (10.78) | 119 (10.65) | 125 (11.20) | 119 (10.64) | 119 (10.64) | |
| Obesity | 308 (6.89) | 80 (7.16) | 67 (6.00) | 84 (7.51) | 77 (6.88) | |
| Vitamin D supplementation: | ||||||
| No | 2222 (49.72) | 630 (56.40) | 555 (49.73) | 508 (45.44) | 529 (47.32) | <0.00001 |
| Yes | 2247 (50.28) | 487 (43.60) | 561 (50.27) | 610 (54.56) | 589 (52.68) | |
| Vegetarian or vegan diet: | ||||||
| No | 4113 (92.03) | 964 (86.30) | 1051 (94.18) | 1046 (93.56) | 1052 (94.10) | <0.00001 |
| Yes | 356 (7.97) | 153 (3.70) | 65 (5.82) | 72 (6.44) | 66 (5.90) | |
| Vitamin D Source | Median (Min–Max) ** in µg/day | p Value *** | ||||
|---|---|---|---|---|---|---|
| Total | Quartiles of Vitamin D Intake from Food (µg/day) | |||||
| Q1 | Q2 | Q3 | Q4 | |||
| Vitamin intake from all food sources | 2.33 (0.01–29.34) | 0.87 (0.01–1.32) A | 1.81 (1.33–2.32) B | 3.00 (2.33–4.03) C | 5.96 (4.04–29.34) D | <0.001 |
| Intake from fish and fish products | 0.52 (0.00–27.28) | 0.00 (0.00–1.18) A | 0.27 (0.00–2.30) B | 1.18 (0.00–3.92) C | 3.32 (0.00–27.28) D | <0.001 |
| Salmon, rainbow trout, herring, eel | 0.25 (0.00–21.25) | 0.00 (0.00–1.07) A | 0.00 (0.00–1.88) B | 0.63 (0.00–3.17) C | 2.24 (0.00–21.25) D | <0.001 |
| • Salmon | 0.23 (0.00–9.5) | 0.00 (0.00–0.95) A | 0.00 (0.00–1.58) B | 0.00 (0.00–3.17) C | 0.63 (0.00–9.5) D | <0.001 |
| • Herring | 0.18 (0.00–7.5) | 0.00 (0.00–0.75) A | 0.00 (0.00–1.25) B | 0.00 (0.00–3.00) C | 0.25 (0.00–7.5) D | <0.001 |
| Halibut, mackerel, brook trout, sole, tuna | 0.00 (0.00–5.88) | 0.00 (0.00–0.67) A | 0.00 (0.00–1.33) B | 0.08 (0.00–3.33) C | 0.33 (0.00–5.88) D | <0.001 |
| Cod, flounder, plaice, pollock, hake | 0.00 (0.00–1.25) | 0.00 (0.00–0.50) A | 0.00 (0.00–0.50) B | 0.00 (0.00–0.87) C | 0.03 (0.00–1.25) D | <0.001 |
| Herring, sardine, and tuna products | 0.00 (0.00–12.36) | 0.00 (0.00–0.41) A | 0.00 (0.00–1.24) B | 0.00 (0.00–1.65) C | 0.41 (0.00–12.36) D | <0.001 |
| Other fish products | 0.00 (0.00–0.93) | 0.00 (0.00–0.62) A | 0.00 (0.00–0.31) B | 0.00 (0.00–0.31) C | 0.00 (0.00–0.93) D | <0.001 |
| Dairy products | 0.31 (0.00–4.93) | 0.19 (0.00–1.04) A | 0.30 (0.00–2.29) B | 0.36 (0.00–2.05) C | 0.50 (0.00–4.93) D | <0.001 |
| Eggs | 0.38 (0.00–8.71) | 0.12 (0.00–1.21) A | 0.37 (0.00–1.71) B | 0.50 (0.00–2.94) C | 0.75 (0.00–8.71) D | <0.001 |
| Meat and meat products | 0.39 (0.00–4.33) | 0.13 (0.00–1.14) A | 0.39 (0.00–2.00) B | 0.48 (0.00–2.83) C | 0.68 (0.00–4.33) D | <0.001 |
| Cereals | 0.12 (0.00–2.48) | 0.07 (0.00–0.86) A | 0.11 (0.00–0.86) B | 0.14 (0.00–2.04) C | 0.17 (0.00–2.48) D | <0.001 |
| Fats | 0.04 (0.00–3.20) | 0.01 (0.00–0.48) A | 0.04 (0.00–1.33) B | 0.05 (0.00–1.58) C | 0.07 (0.00–3.20) D | <0.001 |
| Vitamin D Source | Median (Min–Max) ** in Servings/Week | p Value *** | ||||
|---|---|---|---|---|---|---|
| Total | Quartiles of Vitamin D Intake from Food (µg/day) | |||||
| Q1 | Q2 | Q3 | Q4 | |||
| Total fish and fish products | 0.70 (0.00–34.53) | 0.00 (0.00–7.00) A | 0.47 (0.00–7.00) B | 1.40 (0.00–12.83) C | 3.73 (0.00–34.53) D | <0.001 |
| Salmon, rainbow trout, herring, eel | 0.23 (0.00–14.00) | 0.00 (0.00–0.93) A | 0.00 (0.00–1.52) B | 0.47 (0.00–2.80) C | 1.63 (0.00–14.00) D | <0.001 |
| • Salmon | 0.23 (0.00–7.00) | 0.00 (0.00–0.70) A | 0.00 (0.00–1.17) B | 0.00 (0.00–2.80) C | 0.47 (0.00–7.00) D | <0.001 |
| • Herring | 0.21 (0.00–7.00) | 0.00 (0.00–0.70) A | 0.00 (0.00–1.17) B | 0.00 (0.00–2.33) C | 0.45 (0.00–7.00) D | <0.001 |
| Halibut, mackerel, brook trout, sole, tuna | 0.00 (0.00–12.13) | 0.00 (0.00–2.10) A | 0.00 (0.00–2.33) B | 0.23 (0.00–5.8) C | 0.70 (0.00–12.13) D | <0.001 |
| Cod, flounder, plaice, pollock, hake | 0.00 (0.00–19.13) | 0.00 (0.00–7.00) A | 0.00 (0.00–7.00) B | 0.00 (0.00–12.83) C | 0.47 (0.00–19.13) D | <0.001 |
| Herring, sardine, and tuna products | 0.00 (0.00–7.00) | 0.00 (0.00–0.23) A | 0.00 (0.00–0.70) B | 0.00 (0.00–0.93) C | 0.23 (0.00–7.00) D | <0.001 |
| Other fish products | 0.00 (0.00–7.00) | 0.00 (0.00–4.47) A | 0.00 (0.00–2.33) B | 0.00 (0.00–2.33) C | 0.00 (0.00–7.00) D | <0.001 |
| Vitamin D Source | Regions of Poland | p Value *** | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Central (n = 567) | Eastern (n = 914) | Northern (n = 1350) | North-Western (n = 396) | Southern (n = 993) | South-Western (n = 249) | ||||||||
| Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | ||
| Total intake from food | 100.00 | 2.35 (0.01–25.18) | 100.00 | 2.20 A (0.01–29.34) | 100.00 | 2.41 B (0.04–29.26) | 100.00 | 2.22 (0.05–28.17) | 100.00 | 2.33 (0.07–24.27) | 100.00 | 2.24 (0.13–23.68) | 0.0008 |
| Intake from fish and fish products Salmon, rainbow trout, herring, and eel Halibut, mackerel, brook trout, sole, and tuna Cod, flounder, plaice, pollock, and hake Herring, sardine, and tuna products Other fish products | 32.08 | 0.60 (0.00–21.10) 0.26 (0.00–18.47) 0.03 AC (0.00–5.60) 0.00 (0.00–1.25) 0.00 (0.00–8.24) 0.00 (0.00–0.62) | 34.33 | 0.58 (0.00–17.89) 0.25 (0.00–12.95) 0.03 AC (0.00–5.32) 0.00 (0.00–0.50) 0.00 (0.00–12.36) 0.00 (0.00–0.93) | 27.87 | 0.43 A (0.00–27.28) 0.25 (0.00–21.25) 0.00 BC (0.00–5.88) 0.00 (0.00–0.78) 0.00 A (0.00–6.18) 0.00 (0.00–0.62) | 29.93 | 0.49 (0.00–21.47) 0.25 (0.00–21.19) 0.00 C (0.00–2.56) 0.00 (0.00–1.14) 0.00 (0.00–8.24) 0.00 (0.00–0.31) | 32.01 | 0.63 B (0.00–18.39) 0.25 (0.00–13.31) 0.08 A (0.00–5.42) 0.00 (0.00–0.89) 0.00 B (0.00–8.24) 0.00 (0.00–0.31) | 28.83 | 0.43 (0.00–19.90) 0.25 (0.00–17.00) 0.00 (0.00–4.00) 0.00 (0.00–0.62) 0.00 (0.00–3.30) 0.00 (0.00–0.25) | 0.0329 0.6626 <0.0001 0.102 <0.0001 0.4128 |
| Dairy products Eggs Meat and meat products Cereals Fats | 16.39 23.12 18.07 6.93 3.41 | 0.31 (0.00–3.29) 0.37 A (0.00–7.43) 0.36 A (0.00–3.47) 0.11 A (0.00–2.04) 0.03 ACD (0.00–2.03) | 23.82 16.56 15.64 6.25 3.40 | 0.31 (0.00–3.84) 0.25 B (0.00–7.50) 0.30 B (0.00–3.94) 0.10 B (0.00–2.48) 0.03 B (0.00–2.11) | 17.02 22.00 22.42 6.68 4.00 | 0.32 (0.00–4.93) 0.49 A (0.00–8.71) 0.47 C (0.00–4.33) 0.12 A (0.00–1.99) 0.04 C (0.00–2.88) | 18.17 21.18 20.13 7.60 2.99 | 0.34 (0.00–3.13) 0.49 A (0.00–5.00) 0.43 AC (0.00–3.60) 0.12 A (0.00–1.82) 0.03 CD (0.00–1.86) | 16.60 21.16 18.66 7.21 4.37 | 0.30 (0.00–3.16) 0.49 A (0.00–6.79) 0.37 A (0.00–4.01) 0.12 A (0.00–1.06) 0.05 BD (0.00–3.20) | 17.54 21.34 20.81 7.30 4.18 | 0.32 (0.00–2.30) 0.49 A (0.00–6.29) 0.45 AC (0.00–3.6) 0.12 A (0.00–1.69) 0.05 BD (0.00–2.93) | 0.19 <0.0001 <0.0001 <0.0001 <0.0001 |
| Vitamin D Source | Age of Participants | p Value *** | |||
|---|---|---|---|---|---|
| 14–17 Years (n = 3131) | 18–20 Years (n = 1338) | ||||
| Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | ||
| Total intake from food | 100.00 | 2.36 (0.02–29.34) | 100.00 | 2.41 (0.01–29.26) | 0.2935 |
| Intake from fish and fish products Salmon, rainbow trout, herring, and eel Halibut, mackerel, brook trout, sole, and tuna Cod, flounder, plaice, pollock, and hake Herring, sardine, and tuna products Other fish products | 29.31 | 0.50 (0.00–27.23) 0.25 (0.00–21.25) 0.00 (0.00–5.60) 0.00 (0.00–1.25) 0.00 (0.00–12.36) 0.00 (0.00–0.93) | 30.54 | 0.61 (0.00–27.28) 0.26 (0.00–20.93) 0.00 (0.00–5.88) 0.00 (0.00–0.56) 0.00 (0.00–8.24) 0.00 (0.00–0.62) | 0.1038 0.0800 06081 0.3913 0.3335 0.1275 |
| Dairy products Eggs Meat and meat products Cereals Fats | 17.61 21.52 20.54 7.14 3.88 | 0.32 (0.00–3.84) 0.49 (0.00–8.71) 0.39 (0.00–4.20) 0.12 (0.00–2.04) 0.04 (0.00–3.20) | 16.61 21.98 19.46 7.22 4.19 | 0.31 (0.00–4.93) 0.49 (0.00–7.43) 0.43 (0.00–4.33) 0.13 (0.00–2.48) 0.05 (0.00–2.68) | 0.1091 0.1778 0.7289 0.0081 0.0121 |
| Vitamin D Source | Body Mass Index (BMI) Classification | p Value *** | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Underweight (n = 445) | Normal Weight (n = 3234) | Overweight (n = 482) | Obesity (n = 308) | ||||||
| Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | ||
| Total intake from food | 100.00 | 2.24 (0.01–23.14) | 100.00 | 2.33 (0.02–29.3) | 100.00 | 2.30 (0.04–24.98) | 100.00 | 2.42 (0.01–25.97) | 0.7471 |
| Intake from fish and fish products Salmon, rainbow trout, herring, and eel Halibut, mackerel, brook trout, sole, and tuna Cod, flounder, plaice, pollock, and hake Herring, sardine, and tuna products Other fish products | 29.53 | 0.46 (0.00–19.18) 0.25 (0.00–15.20) 0.00 (0.00–3.20) 0.00 (0.00–0.56) 0.00 (0.00–8.24) 0.00 (0.00–0.37) | 31.04 | 0.53 (0.00–27.28) 0.25 (0.00–21.25) 0.00 (0.00–5.90) 0.00 (0.00–1.25) 0.00 (0.00–12.36) 0.00 (0.00–0.93) | 30.71 | 0.50 (0.00–18.79) 0.25 (0.00–17.50) 0.00 (0.00–4.00) 0.00 (0.00–0.63) 0.00 (0.00–4.94) 0.00 (0.00–0.62) | 31.45 | 0.47 (0.00–21.47) 0.25 (0.00–15.53) 0.00 (0.00–4.20) 0.00 (0.00–0.80) 0.00 (0.00–0.62) 0.00 (0.00–0.31) | 0.7428 0.723 0.7571 0.5637 0.7054 0.7914 |
| Dairy products Eggs Meat and meat products Cereals Fats | 18.48 20.78 19.80 7.10 4.32 | 0.30 (0.00–3.84) 0.36 (0.00–8.71) 0.40 (0.00–3.60) 0.12 (0.00–0.98) 0.04 (0.00–1.01) | 18.43 20.67 19.07 6.98 3.82 | 0.32 (0.00–4.93) 0.38 (0.00–8.11) 0.37 (0.00–4.20) 0.12 (0.00–2.48) 0.04 (0.00–3.20) | 17.56 21.62 20.43 6.04 3.63 | 0.30 (0.00–3.16) 0.49 (0.00–7.50) 0.40 (0.00–4.09) 0.14 (0.00–0.98) 0.04 (0.00–2.93) | 18.82 19.94 20.05 6.53 3.20 | 0.31 (0.00–3.33) 0.43 (0.00–3.71) 0.42 (0.00–4.33) 0.10 (0.00–2.04) 0.03 (0.00–1.85) | 0.1302 0.5984 0.7790 0.364 0.1844 |
| Vitamin D Source | Vitamin D Supplementation | Vegetarian or Vegan Diet | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No (n = 2222) | Yes (n = 2247) | p Value *** | No (n = 4113) | Yes (n = 356) | p Value *** | |||||
| Intake (%) | Median ** (Min-Max) | Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | Intake (%) | Median ** (Min–Max) | |||
| Total intake from food | 100.00 | 2.19 (0.02–28.17) | 100.00 | 2.47 (0.01–29.34) | <0.0001 | 100.00 | 2.37 (0.01–29.34) | 100.00 | 1.70 (0.01–28.75) | <0.0001 |
| Intake from fish and fish products Salmon, rainbow trout, herring, and eel Halibut, mackerel, brook trout, sole, and tuna Cod, flounder, plaice, pollock, and hake Herring, sardine, and tuna products Other fish products | 29.03 | 0.42 (0.00–27.22) 0.25 (0.00–21.25) 0.00 (0.00–5.60) 0.00 (0.00–1.25) 0.00 (0.00–12.36) 0.00 (0.00–0.93) | 32.72 | 0.61 (0.00–27.28) 0.32 (0.00–21.19) 0.08 (0.00–5.88) 0.00 (0.00–1.14) 0.00 (0.00–8.24) 0.00 (0.00–0.93) | <0.0001 0.0001 <0.0001 0.0002 0.0647 0.1163 | 31.33 | 0.55 (0.00–27.28) 0.00 (0.00–21.25) 0.00 (0.00–5.88) 0.00 (0.00–1.25) 0.00 (0.00–12.36) 0.00 (0.00–0.93) | 28.20 | 0.09 (0.00–19.66) 0.00 (0.00–13.76) 0.00 (0.00–2.42) 0.00 (0.00–0.50) 0.00 (0.00–8.24) 0.00 (0.00–0.31) | <0.0001 0.0002 0.0001 0.0174 0.0059 0.0015 |
| Dairy products Eggs Meat and meat products Cereals Fats | 18.77 20.58 20.64 7.02 3.95 | 0.30 (0.00–4.93) 0.37 (0.00–7.43) 0.39 (0.00–4.33) 0.11 (0.00–1.99) 0.04 (0.00–3.20) | 17.97 20.88 18.08 6.69 3.67 | 0.33 (0.00–3.84) 0.49 (0.00–8.71) 0.38 (0.00–4.09) 0.12 (0.00–2.48) 0.04 (0.00–2.93) | 0.0002 0.0026 0.2341 0.1837 0.8308 | 17.68 20.30 20.31 6.65 3.72 | 0.31 (0.00–4.93) 0.38 (0.00–8.12) 0.42 (0.00–4.33) 0.12 (0.00–2.48) 0.04 (0.00–3.20) | 28.41 28.19 0.00 10.09 5.11 | 0.29 (0.00–2.00) 0.36 (0.00–8.71) 0.00 (0.00–0.00) 0.11 (0.00–1.33) 0.03 (0.00–2.30) | 0.5086 0.206 <0.0001 0.0889 0.0007 |
| Variable | Correlations | ||
|---|---|---|---|
| r | p | ||
| Number of servings of fish and fish products per week | Total fish and fish products | 0.74 | <0.01 |
| Salmon, rainbow trout, herring, and eel | 0.71 | <0.01 | |
| Halibut, mackerel, brook trout, sole, and tuna | 0.56 | <0.01 | |
| Cod, flounder, plaice, pollock, and hake | 0.43 | <0.01 | |
| Herring, sardine, and tuna products | 0.54 | <0.01 | |
| Other fish products | 0.41 | <0.01 | |
| Vitamin D intake from fish and fish products (µg/day) | Intake from fish and fish products | 0.76 | <0.01 |
| Salmon, rainbow trout, herring, and eel | 0.71 | <0.01 | |
| Halibut, mackerel, brook trout, sole, and tuna | 0.56 | <0.01 | |
| Cod, flounder, plaice, pollock, and hake | 0.43 | <0.01 | |
| Herring, sardine, and tuna products | 0.54 | <0.01 | |
| Other fish products | 0.42 | <0.01 | |
| Body Mass Index (kg/m2) | 0.03 | 0.0093 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lachowicz, K.; Stachoń, M. Determinants of Dietary Vitamin D Intake in Population-Based Cohort Sample of Polish Female Adolescents. Int. J. Environ. Res. Public Health 2022, 19, 12184. https://doi.org/10.3390/ijerph191912184
Lachowicz K, Stachoń M. Determinants of Dietary Vitamin D Intake in Population-Based Cohort Sample of Polish Female Adolescents. International Journal of Environmental Research and Public Health. 2022; 19(19):12184. https://doi.org/10.3390/ijerph191912184
Chicago/Turabian StyleLachowicz, Katarzyna, and Małgorzata Stachoń. 2022. "Determinants of Dietary Vitamin D Intake in Population-Based Cohort Sample of Polish Female Adolescents" International Journal of Environmental Research and Public Health 19, no. 19: 12184. https://doi.org/10.3390/ijerph191912184
APA StyleLachowicz, K., & Stachoń, M. (2022). Determinants of Dietary Vitamin D Intake in Population-Based Cohort Sample of Polish Female Adolescents. International Journal of Environmental Research and Public Health, 19(19), 12184. https://doi.org/10.3390/ijerph191912184