Organizational culture refers to the values and beliefs that typify and prescribe norms of behavior in an organization. Although invisible and informal, it is an important force for managing organizations. A growth culture emphasizes innovation, creativity, openness and collaboration, while a conservative culture emphasizes authoritative leadership, guanxi and appearance [
1]. Different types of organizational culture have different effects on organizational performance. This effect can be positive, negative or without effect at all. Organizations must increasingly maintain a culture to gain a competitive advantage. Research found that innovative culture has a significant positive impact on knowledge transfer performance, but whether supportive culture has an impact on knowledge transfer performance has not been confirmed [
2,
3]. One study showed innovative culture and supportive culture has a positive impact on organizational innovation performance, while bureaucratic culture has no significant effect on organizational innovation performance [
4]. Several studies found the effects of various culture dimensions on performance [
5,
6,
7]. A study found that organization culture flexibility is positively correlated with organizational growth performance, while the stability of organizational culture is negatively correlated. The more the organizational culture focuses on the outside, the higher the organizational performance, and the more the organization focuses on the inside, the lower the performance [
8]. In China, more and more medical institutions are forming new consortiums, such as medical consortiums, medical communities, specialist alliances, internet hospitals, etc. Culture integration is a fact that cannot be ignored, and the new partnership needs to establish a more open and inclusive cultural atmosphere in order to promote better cooperation between institutions.
In recent years, organization culture, alongside structural reforms in order to improve healthcare performance, has been emphasized. Evidence from the research literature for a link between the culture of an organization and the quality and safety of the care that it provides is sparse. The link of organizational culture as related to hospital organization is weak from the research literature. Despite some evidence support establishing the links between culture and performance, however, much less is known regarding the mechanisms through which culture influences performance especially in healthcare organizations.
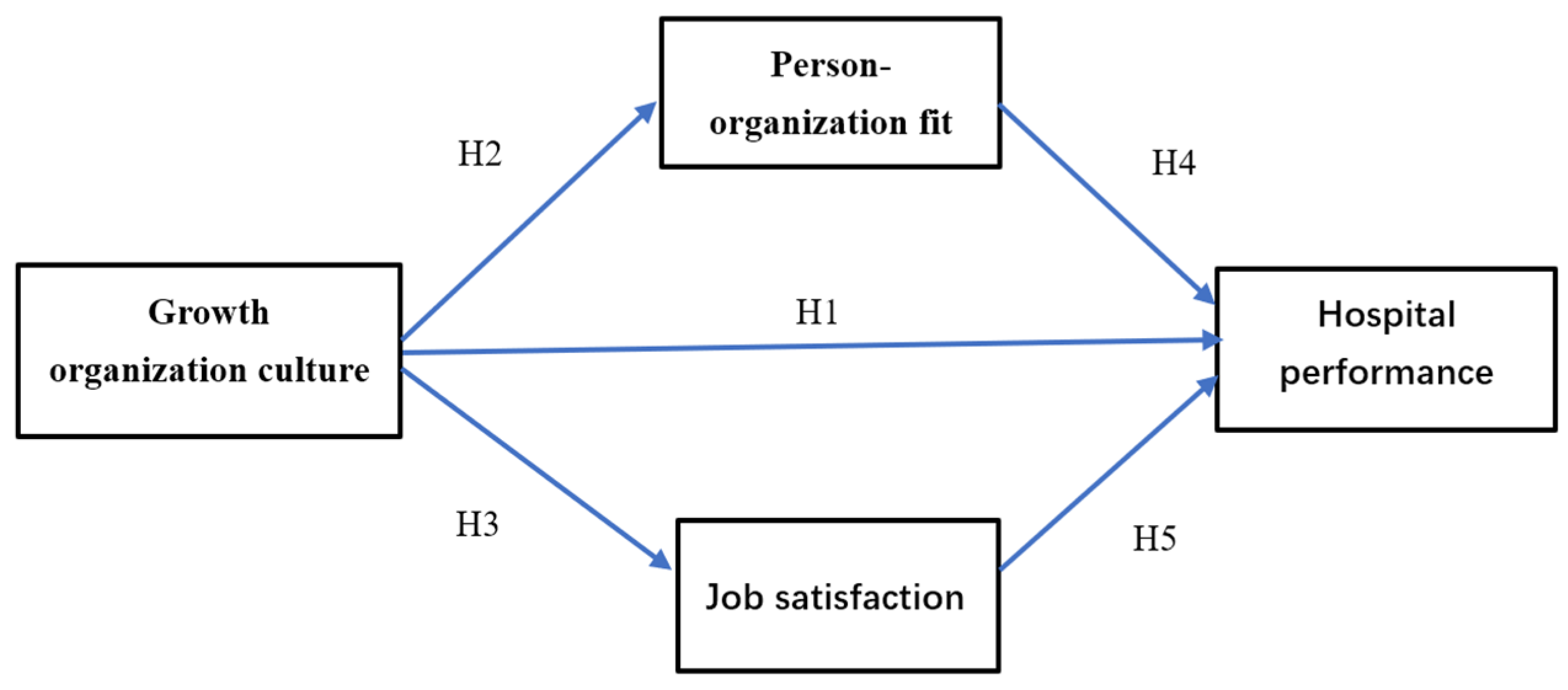
The purpose of our study, therefore, is to investigate and interpret the role of growth organizational culture (GOC), person–organization fit (POF), and job satisfaction (JS) in predicting hospital performance (HP) and when an organizational growth culture can effectively influence individual and organization value fit and increase job satisfaction. If physicians agree strongly about the direction and goals of hospitals, they continually renew efforts to achieve organizational goals. Therefore, our prediction is that the relationship between organizational growth culture and hospital performance can be partially explained through person–organization fit and job satisfaction.
This study expands the scope of previous study, exploring the relationship of growth organizational culture and hospital performance in hospital setting and discusses the moderating roles of job satisfaction and person–organization fit. We hypothesized that as growth organizational culture improved, hospital performance would improve.
Literature Review and Hypothesis Development
Hypothesis 1 (H1). Growth organization culture positively and significantly influences hospital performance.
Much evidence indicates that organizational culture can promote organizational performance [
9,
10]. Hospital safety culture has been studied most and can influence medical quality [
11]. Improved safety culture is associated with decreases in patient harm and hospital mortality across a hospital system [
12], but safety culture is more about the norms and constraints of medical staff behavior. In the changing hospital system reforms, a growth culture which is more open, inclusive and encourages innovation is needed. The direct impact of organizational culture on organizational performance has always been focus of researchers, but there are still many uncertainties in the relationship between organizational culture and organizational performance. However, when an organization wants to make changes, the organizational culture that has been formed may hinder organizational performance [
13]. In medical systems in China, hospitals have formed medical complexes in the form of urban hospital groups, specialty alliances and county medical communities. However, there are challenges in cultural integration.
The influence of organizational culture on organizational performance cannot be ignored in a multicultural workplace [
14]. In the context of the establishment of various medical union in China, the former medical institutions have their own organization cultures, and the combination of institutions makes hospitals become multicultural workplaces.
Hypothesis 2 (H2). Growth organization culture positively and significantly influences person–organization fit.
Growth culture provides employees with more growth and development opportunities, so that employees can be more grateful to the organization, more strongly identify with the values and goals of the organization, effectively mobilize their enthusiasm and initiative, motivate employees to develop their own potential and improve work involvement. Growth culture is perceived as a competitive advantage for every organization for better selection and integration if the workforce is culturally diverse. It brings numerous advantages on the personal level and creates a safe climate in which physicians are inspired, supported and motivated [
15]. Knowledge sharing culture can promote the relationship between the organization and the individual [
16].
A harmonious organizational culture helps to form a good organizational atmosphere in which people’s behaviors are consistent with the values of the organization as far as possible. People’s values, behavior habits, personality characteristics, organizational culture, values, norms and so on constitute a good organizational cultural environment.
Hypothesis 3 (H3). Growth organization culture positively and significantly influences job satisfaction.
Organizational culture imposes significant impacts on staff and patient outcomes. In the US, management interventions targeting organizational culture have been proved to result in reductions in medical errors in hospitals [
17]. A study conducted in Ethiopia showed that organizational culture is associated with staff satisfaction in primary hospitals [
18]. Similarly, a significant correlation between organizational culture and quality of work life in hospital nurses was found in Korea [
19].
Cameron and Quinn [
20] examined organizational culture from four perspectives: clan, adhocracy, market and hierarchy. This theory is often used to judge the characteristics of organizational culture and explore the relationship between organizational performance. According to Hofstede, organizational culture is a complex of values and practices, and values are the core [
21]. Hofstede’s theory is more appropriate at the level of national culture or society than organizations. Schein proposed three levels of organizational culture: artifacts, espoused beliefs and values and underlying assumptions [
22]. Schein’s theory is often applied to the external adaptation and internal integration of organizations. These classical organizational culture theories guide organizations to provide more efficient organizational climates. Job satisfaction is very sensitive to the variations in organizational culture [
18]. A perception of a highly people-oriented culture, for example, was found to be associated with lower workload, lower job strain, higher job satisfaction and lower intention to leave in hospital nurses in the US [
23]. Teamwork and a clan culture can help boost staff satisfaction in the healthcare setting [
18]. A study in Greece found the most important factor in doctors’ job satisfaction appears to be the nature of their job and the high levels of autonomy that they have [
24].
Organizational culture can reduce employee stress in the workplace, and HR practitioners should match the types of organizational culture and employee competency situationally to reduce employee stress. Organizations desiring professional competency for their employees should build a clan organizational culture. While organizations should encourage a market organizational culture for their employees who possess result-oriented competency [
25].
Hypothesis 4 (H4). Person–organization fit positively and significantly influences hospital performance.
Work performance of an employee is a reflection of actions for both personal and organizational purposes according to the person–organization value fit theory [
26]. A good person–organization value fit is beneficial in maintaining staff wellbeing, which helps the passion for the work of employees [
27,
28]. A study showed that person–organization fit is associated with organizational citizenship behaviors (OCB) and the organizational commitments of staffs [
29]. Its influence on organizational outcomes maybe much stronger than on work outcomes [
29,
30].
It is challenging to study the person–organization value fit of physicians, as physicians tend to serve as a consultant rather than an employee in the Chinese health context. Song and colleagues found that person–organization value fit is positively associated with medical workers’ engagement and negatively associated with turnover rate in public hospitals [
31]. A study also found that person–organization value fit is positively correlated with self-efficacy of nurses [
32]. We assume that the positive effects of person–organization value fit on physicians can improve hospital performance.
Hypothesis 5 (H5). Job satisfaction positively and significantly influences hospital performance.
Physicians’ job satisfaction refers to the general evaluation of their job [
33]. Job satisfaction of staff is a quite important factor that influences organizational performance and therefore should be of major concern to organizations. Researchers have proposed several theories to interpret the link between job satisfaction and organizational performance, including the motivation theory and the wellbeing and productivity theory [
34]. High job satisfaction means that physicians are happy at work and some evidence supports more job satisfaction resulting in better performance [
35,
36]. It is essential to know how staffs build organizational performance through their satisfaction and create competitive advantage in the workplace [
37].
How public hospitals can best cultivate organization performance is becoming a challenging factor and they are adopting positive strategies for it. In this study, promoting job satisfaction of physicians is suggested to be one effective strategy to improve public hospital performance.
Hypothesis 6 (H6). Person–organization value fit mediates the effect of growth organization culture on hospital performance.
The influence of organizational culture on organizational performance is actually restricted by environmental factors. Person–organization value fit is one of important environmental factors and usually affects individuals’ psychology and behavior outcomes. Growth organizational culture is beneficial to the links between organization and employers. A study found person–organization fit significantly moderates the effects of job satisfaction on turnover intentions among employees at higher education institutions [
38]. The mediating role of person–organization fit in the relationship between work environment and stress among social workers was verified [
39]. A systematic review showed there was a positive association between value fit and staff outcomes in health settings [
40]. Little literature has reported the cumulative effect of person–organization fit, job satisfaction and organization culture on hospital performance.
Combining matching theory and contingency management theory, this study believes that different organizational cultures have different effects on organizational performance, and the key is to match the internal and external environment of the organization. A culture well matched with the environment can mobilize the enthusiasm of employees, enhance the cohesion of employees and promote the improvement of organizational performance. However, a culture poorly matched with the environment will not be recognized by employees, will affect their organizational commitment and satisfaction and even hinder the improvement of organizational performance.
Hypothesis 7 (H7). Job satisfaction mediates the effect of growth organization culture on hospital performance.
Humans are the most precious resource in the organization, and the positivity of human resources in the organization directly determines the performance level of the organization. Therefore, the influence mechanism of organizational culture on organizational performance cannot be separated from the fundamental element of human resources. According to the viewpoint of modern psychology and behavior science, culture is an important factor affecting individual psychology and behavior, and the mechanism of the cultural field is realized through human beings. Therefore, it is a good choice to take employee psychology and behavior as the mediating variables. Different types of employee psychology and behavior can be selected according to different concerns.
A strong and balanced organization culture has a significant positive relationship with organizational performance, and this effect is mediated by employee attitudes [
41]. However, most hospitals operate physicians’ job satisfaction as solely the responsibility of the individual physician and neglect organizational factors. Strengthening organizational culture is one of nine organizational strategies to promote engagement [
42].




{kind=link}
{kind=link}

