
Sinus Floor Elevation via an Osteotome Technique without Biomaterials


 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
- (a)
- Patients older than 18 years of age with good general health status
- (b)
- Absence of one or more teeth in locations where bone availability to the sinus floor was between 2–5 mm;
- (c)
- At least 4 months of healing had occurred between tooth extraction and implant assessment;
- (d)
- After implant placement the bone around the entire implant shoulder should be ≥1 mm;
- (e)
- No removable prostheses;
- (f)
- The patient had to sign an informed consent and accept to return for review appointments.
- (a)
- Patients with severe bruxism;
- (b)
- Smokers of more than 10 cigarettes/day;
- (c)
- Local, acute or chronic sinus pathology;
- (d)
- Presence of Underwood septa in the implant area.
2.1. Surgical Sequence and Prosthetic Rehabilitation
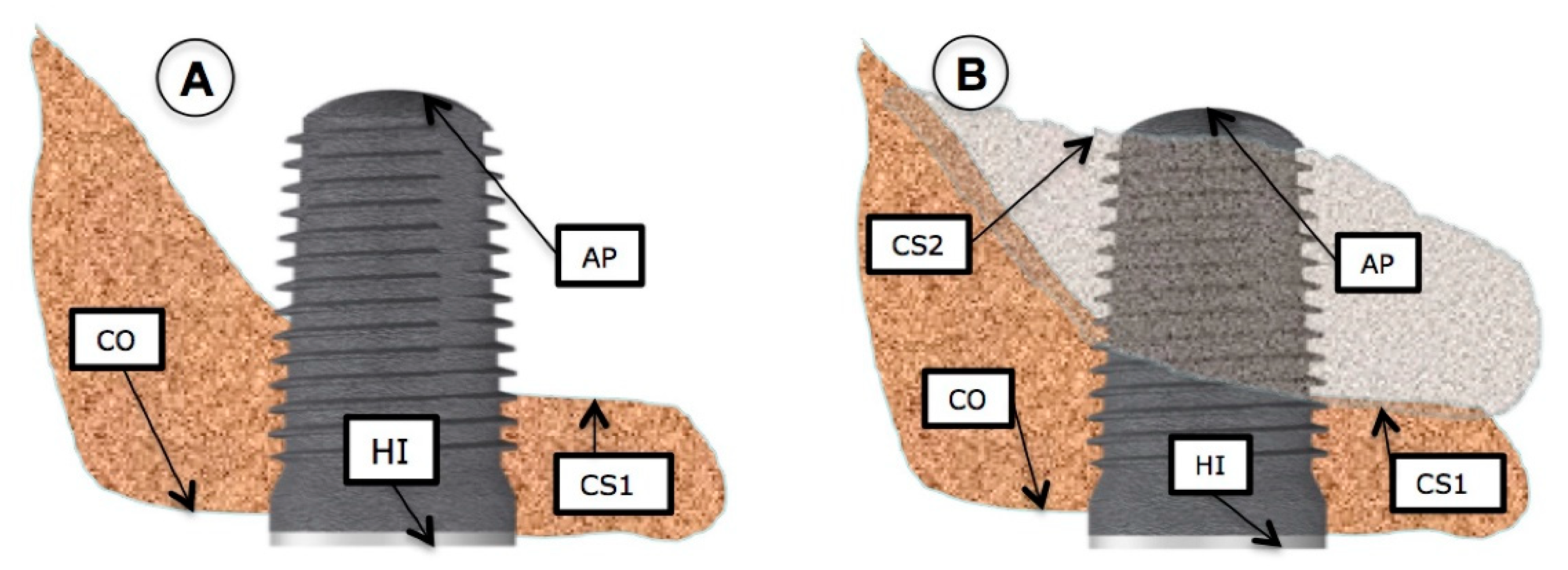
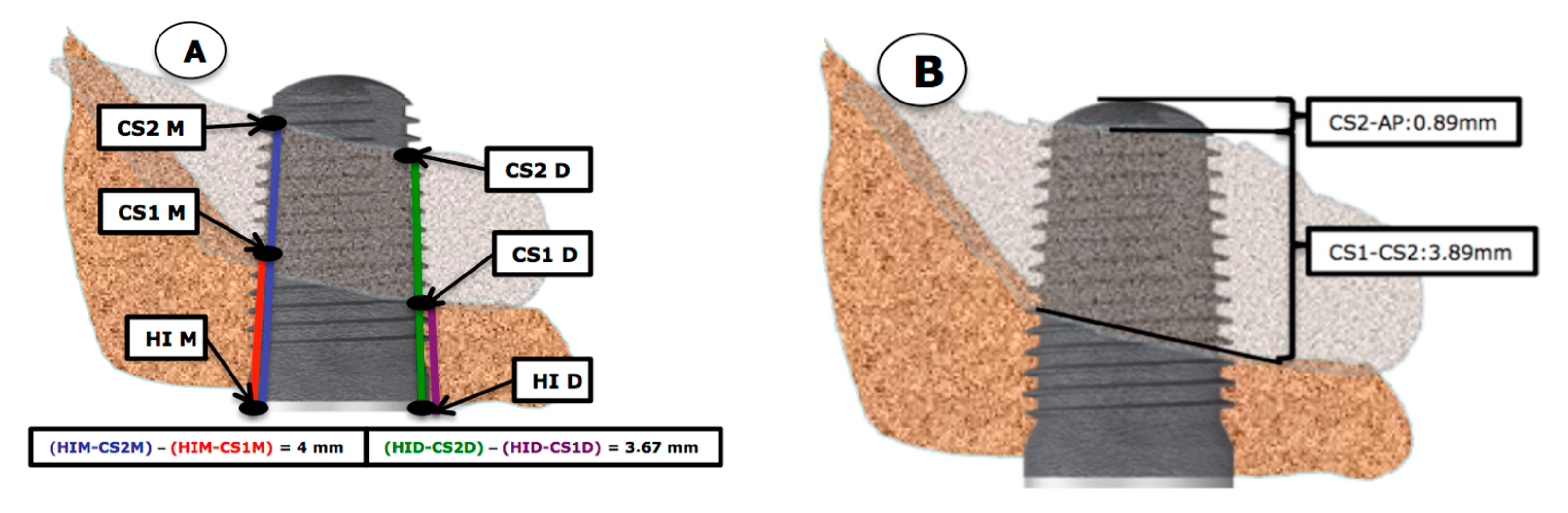
2.2. X-ray Measurements
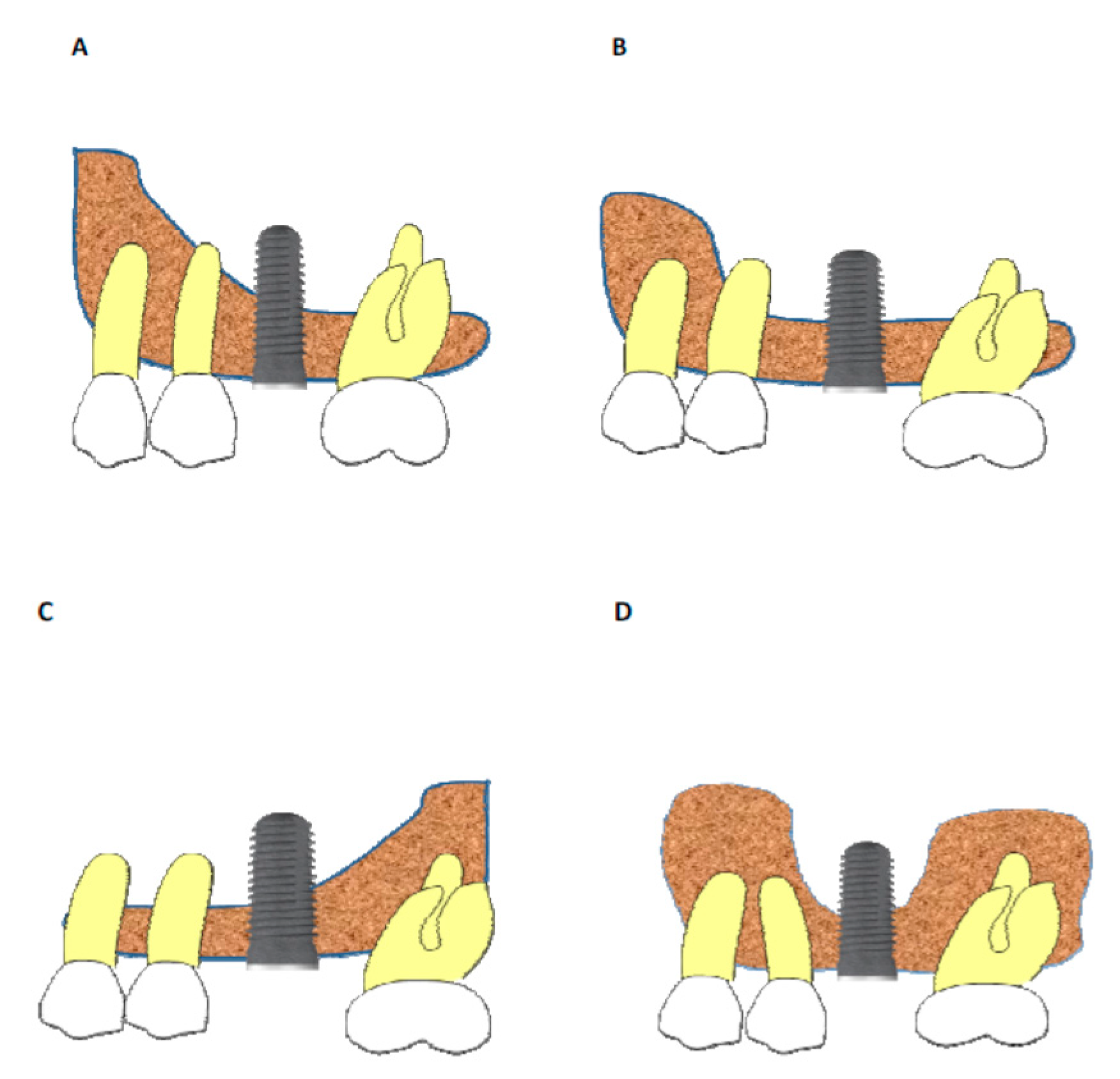
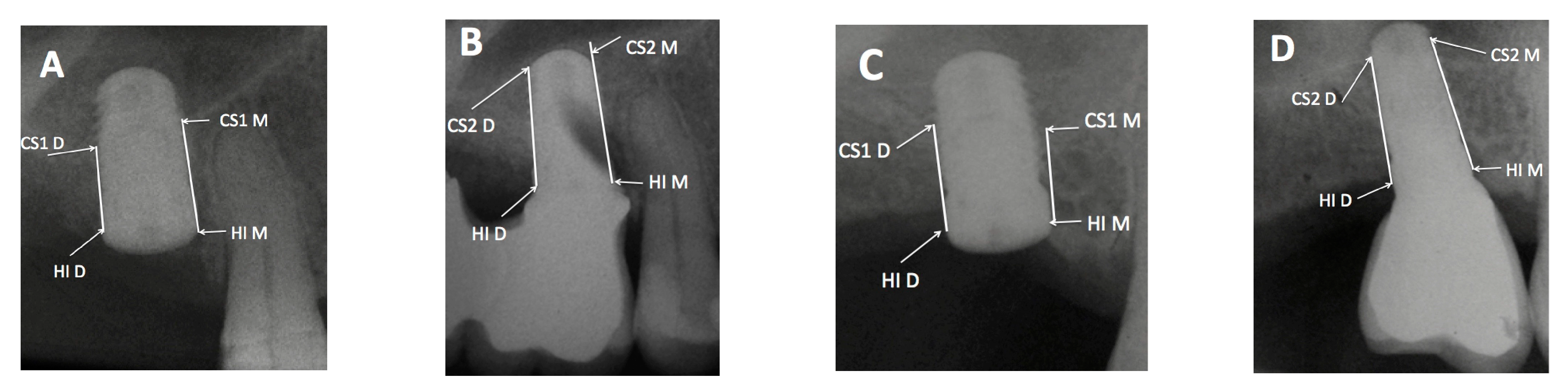
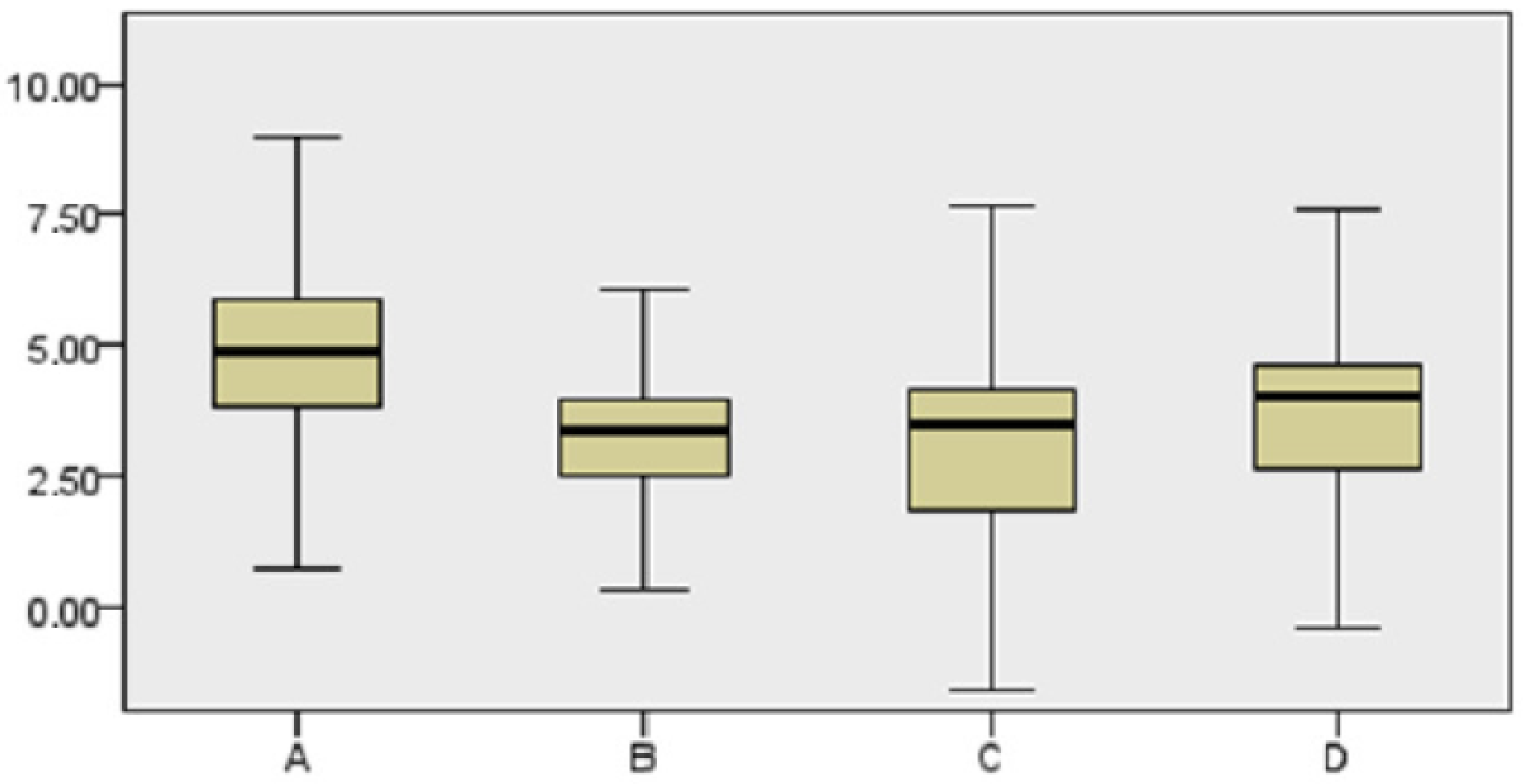
2.3. Relationship between the Maxillary Sinus Cavity and Implant Location
2.4. Statistical Analysis
3. Results
- -
- Sinus type A: implant is close to the mesial wall of the sinus (25% of cases);
- -
- Sinus type B: implant is located in a flat sinus floor at some distance from the osseous walls and/or partitions. This was the most common situation representing 37.5% of cases;
- -
- Sinus type C: implant is in contact with, or very close, to the distal sinus wall (12.5% of cases);
- -
- Sinus type D: implant is very close to a bony wall at the mesial and distal aspects of the maxillary sinus or in contact with an Underwood septum, delimiting the maxillary sinus into different compartments (25% of cases).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hirschfeld, L.; Wasserman, B. A Long-Term Survey of Tooth Loss in 600 Treated Periodontal Patients. J. Periodontol. 1978, 49, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; da Silva, J.C.C.; de Mendonça, A.F.; Lindhe, J. Ridge alterations following grafting of fresh extraction sockets in man. A randomized clinical trial. Clin. Oral Implants Res. 2015, 26, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Sukekava, F.; Wennström, J.L.; Lindhe, J. Tissue modeling following implant placement in fresh extraction sockets. Clin. Oral Implants Res. 2006, 17, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Tatum, H., Jr. Maxillary and sinus implant reconstructions. Dent. Clin. N. Am. 1986, 30, 207–229. [Google Scholar] [PubMed]
- Boyne, P.J.; James, R.A. Grafting of the maxillary sinus floor with autogenous marrow and bone. J. Oral Surg. 1980, 38, 613–616. [Google Scholar]
- Taschieri, S. Short dental implants as compared to maxillary sinus augmentation procedure for the rehabilitation of edentulous posterior maxilla: Three-year results of a randomized clinical study. Clin. Implants Dent. Relat. Res. 2018, 20, 9–12. [Google Scholar] [CrossRef]
- Yildrim, M.; Spiekermann, H.; Handt, S.; Edelhoff, D. Maxillary Sinus Augmentation with the Xenograft Bio-Oss and Autogenous Intraoral Bone for Qualitative Improvement of the Implant Site: A Histologic and Histomorphometric Clinical Study in Humans. Int. J. Oral Maxillofac. Implants 2001, 16, 23–33. [Google Scholar]
- Summers, R.B. A new concept in maxillary implant surgery: The osteotome technique. Compendium 1994, 15, 152–154. [Google Scholar]
- Summers, R.B. The osteotome technique: Part 3—Less invasive methods of elevating the sinus floor. Compendium 1994, 15, 698–700. [Google Scholar]
- Rosen, P.S.; Summers, R.; Mellado, J.R.; Salkin, L.M.; Shanaman, R.H.; Marks, M.H.; Fugazzotto, P.A. The bone-added osteotome sinus floor elevation technique: Multicenter retrospective report of consecutively treated patients. Int. J. Oral Maxillofac. Implants 1999, 14, 853–858. [Google Scholar] [PubMed]
- Andrés-García, R.; Vives, N.G.; Climent, F.H.; Palacín, A.F.; Santos, V.R.; Climent, M.H.; Bullón, P. In vitro evaluation of the influence of the cortical bone on the primary stability of two implant systems. Med. Oral Patol. Oral Cir. Bucal. 2009, 14, E93–E97. [Google Scholar] [PubMed]
- García-Vives, N.; Andrés-García, R.; Ríos-Santos, V.; Fernández-Palacín, A.; Bullón-Fernández, P.; Herrero-Climent, M.; Herrero-Climent, F. In vitro evaluation of the type of implant bed preparation with osteotomes in bone type IV and its influence on the stability of two implant systems. Med. Oral Patol. Oral Cir. Bucal. 2009, 14, e5–e460. [Google Scholar]
- Herrero-Climent, M.; Santos-García, R.; Jaramillo-Santos, R.; Romero-Ruiz, M.M.; Fernández-Palacín, A.; Lázaro, P.; Bullón, P.; Rios-Santos, J.V. Assessment of Osstell ISQ’s reliability for implant stability measurement: A cross-sectional clinical study. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e877–e882. [Google Scholar] [CrossRef] [PubMed]
- Winter, A.A.; Pollack, A.S.; Odrich, R.B. Placement of Implants in the Severely Atrophic Posterior Maxilla Using Localized Management of the Sinus Floor: A Preliminary Study. Int. J. Oral Maxillofac. Implants 2002, 17, 687–695. [Google Scholar]
- Gonzalez, S.; Mao-Chi, T.; Ahn, K.M.; Nowzari, H. Crestal Approach for Maxillary Sinus Augmentation in Patients With ≤4 Mm of Residual Alveolar Bone. Clin. Implant Dent. Relat. Res. 2014, 16, 827–835. [Google Scholar] [CrossRef]
- Nedir, R.; Nurdin, N.; Najm, A.S.; Hage, E.M.; Bischof, M. Short implants placed with or without grafting into atrophic sinuses: The 5-year results of a prospective randomized controlled study. Clin. Oral Implants Res. 2017, 28, 877–886. [Google Scholar] [CrossRef]
- Nedir, R.; Bischof, M.; Vazquez, L.; Nurdin, N.; Szmukler-Moncler, S.; Bernard, J.P. Osteotome Sinus Floor Elevation Technique Without Grafting Material: 3-year Results of a Prospective Pilot Study. Clin. Oral Implants Res. 2009, 20, 701–707. [Google Scholar] [CrossRef]
- Yang, J.; Xia, T.; Wang, H.; Cheng, Z.; Shi, B. Outcomes of Maxillary Sinus Floor Augmentation without Grafts in Atrophic Maxilla: A Systematic Review and Meta-Analysis Based on Randomised Controlled Trials. J. Oral Rehabil. 2019, 46, 282–290. [Google Scholar] [CrossRef]
- Lundgren, S.; Andersson, S.; Gualini, F.; Sennerby, L. Bone Reformation with Sinus Membrane Elevation: A New Surgical Technique for Maxillary Sinus Floor Augmentation. Clin. Implant Dent. Relat. Res. 2004, 6, 165–173. [Google Scholar] [CrossRef]
- Fugazzotto, P.A. Immediate Implant Placement Following a Modified Trephine/Osteotome Approach: Success Rates of 116 Implants to 4 Years in Function. Int. J. Oral Maxillofac. Implants 2002, 17, 113–120. [Google Scholar] [PubMed]
- Shalabi, M.M.; Manders, P.; Mulder, J.; Jansen, J.A.; Creugers, N.H. A meta-analysis of clinical studies to estimate the 4.5-year survival rate of implants placed with the osteotome technique. Int. J. Oral Maxillofac. Implants 2007, 22, 110–116. [Google Scholar] [PubMed]
- Nedir, R.; Nurdin, R.; Khoury, P.; Perneger, P.; El Hage, P.; Bernard, J.P.; Bischof, M. Osteotome Sinus Floor Elevation with and Without Grafting Material in the Severely Atrophic Maxilla. A 1-year Prospective Randomized Controlled Study. Clin. Oral Implants Res. 2013, 24, 1257–1264. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Uzeda, M.G.; Sartoretto, S.C.; Calasans-Maia, M.D. Maxillary Sinus Floor Elevation With Simultaneous Implant Placement Without Grafting Materials: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 636–647. [Google Scholar] [CrossRef]
- Nedir, R.; Nurdin, N.; Huynh-Ba, G.; Bischof, M. Change in Crown-to-Implant Ratio of Implants Placed in Grafted and Nongrafted Posterior Maxillary Sites: A 5-year Prospective Randomized Study. Int. J. Oral Maxillofac. Implants 2019, 34, 1231–1236. [Google Scholar] [CrossRef]
- Tan, W.C.; Lang, N.P.; Zwahlen, M.; Pjetursson, B.E. A Systematic Review of the Success of Sinus Floor Elevation and Survival of Implants Inserted in Combination with Sinus Floor Elevation. Part II: Transalveolar Technique. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 241–254. [Google Scholar] [CrossRef]
- Abi Najm, S.; Nathalie, N.; El Hage, M.; Bischof, M.; Nedir, R. Osteotome Sinus Floor Elevation Without Grafting: A 10-Year Clinical and Cone-Beam Sinus Assessment. Implants Dent. 2018, 27, 439–444. [Google Scholar] [CrossRef]
- Misch, C.E.; Judy, K.W. Classification of partially edentulous arches for implant dentistry. Int. J. Oral Implantol. 1987, 4, 7–13. [Google Scholar]
- Cannizzaro, G.; Felice, P.; Minciarelli, A.F.; Leone, M.; Viola, P.; Esposito, M. Early implant loading in the atrophic posterior maxilla: 1-stage lateral versus crestal sinus lift and 8 mm hydroxyapatite-coated implants. A 5-year randomised controlled trial. Eur. J. Oral Implantol. 2013, 6, 13–25. [Google Scholar]
- Al-Moraissi, E.A.; Altairi, N.H.; Abotaleb, B.; Al-Iryani, G.; Halboub, E.; Alakhali, M.S. What is the Most Effective Rehabilitation Method for Posterior Maxillas with 4 to 8 mm of Residual Alveolar Bone Height Below the Maxillary Sinus With Implant-Supported Prostheses? A Frequentist Network Meta-Analysis. J. Oral Maxillofac. Surg. 2019, 77, 70.e1–70.e33. [Google Scholar] [CrossRef]
- Bruschi, G.; Crespi, R.; Capparè, P.; Gherlone, E. Transcrestal sinus floor elevation: A retrospective study of 46 patients up to 16 years. Clin. Implant Dent. Relat. Res. 2012, 14, 759–767. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.X.; Shi, J.Y.; Zhuang, L.F.; Qian, S.J.; Mo, J.J.; Lai, H.C. Transalveolar sinus floor elevation using osteotomes without grafting in severely atrophic maxilla: A 5-year prospective study. Clin. Oral Implants Res. 2016, 27, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Nedir, R.; Nurdin, N.; Vazquez, L.; Abi Najm, S.; Bischof, M. Osteotome Sinus Floor Elevation without Grafting: A 10-Year Prospective Study. Clin. Implant Dent. Relat. Res. 2016, 18, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Verdugo, F.; Uribarri, A.; Laksmana, T.; D’addona, A. Long-term stable vertical bone regeneration after sinus floor elevation and simultaneous implant placement with and without grafting. Clin. Implant Dent. Relat. Res. 2017, 19, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Vazouras, K.; de Souza, A.B.; Gholami, H.; Papaspyridakos, P.; Pagni, S.; Weber, H.P. Effect of time in function on the predictability of short dental implants (≤6 mm): A meta-analysis. J. Oral Rehabil. 2020, 47, 403–415. [Google Scholar] [CrossRef]
- Bolle, C.; Felice, P.; Barausse, C.; Pistilli, V.; Trullenque-Eriksson, A.; Esposito, M. 4 mm long vs longer implants in augmented bone in posterior atrophic jaws: 1-year post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 31–47. [Google Scholar]
- Zhang, X.M.; Shi, J.Y.; Gu, Y.X.; Qiao, S.C.; Mo, J.J.; Lai, H.C. Clinical Investigation and Patient Satisfaction of Short Implants Versus Longer Implants with Osteotome Sinus Floor Elevation in Atrophic Posterior Maxillae: A Pilot Randomized Trial. Clin. Implant Dent. Relat. Res. 2017, 19, 161–166. [Google Scholar] [CrossRef]
- Hadzik, J.; Krawiec, M.; Paweł Kubasiewicz-Ross, P.; Prylińska-Czyżewska, A.; Gedrange, T.; Dominiak, M. Short Implants and Conventional Implants in The Residual Maxillary Alveolar Ridge: A 36-Month Follow-Up Observation. Med. Sci. Monit. 2018, 24, 5645–5652. [Google Scholar] [CrossRef]
- Leblebicioglu, B.; Ersanli, S.; Karabuda, C.; Tosun, T.; Gokdeniz, H. Radiographic evaluation of dental implants placed using an osteotome technique. J. Periodontol. 2005, 76, 385–390. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Tan, W.C.; Zwahlen, M.; Lang, N.P. A Systematic Review of the Success of Sinus Floor Elevation and Survival of Implants Inserted in Combination with Sinus Floor Elevation. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 216–240. [Google Scholar] [CrossRef]
- Antonaya–Mira, R.; Barona-Dorado, C.; Martínez-Rodriguez, N.; Cáceres-Madroño, E.; Martínez-González, J.M. Meta-analysis of the increase in height in maxillary sinus elevations with osteotome. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e146–e152. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pérez-Martínez, S.; Martorell-Calatayud, L.; Peñarrocha-Oltra, D.; García-Mira, B.; Peñarrocha-Diago, M. Indirect sinus lift without bone graft material: Systematic review and meta-analysys. J. Clin. Exp. Dent. 2015, 7, e316–e319. [Google Scholar] [CrossRef] [PubMed]
- Mi-Si, S.; Long-Fei, Z.; Ying-Xin, G.; Jia-Ji, M.; Shi-Chong, Q.; Hong-Chang, L. Osteotome Sinus Floor Elevation with or without Grafting: A 3-year Randomized Controlled Clinical Trial. J. Clin. Periodontol. 2013, 40, 396–403. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Rees, J.; Karasoulos, D.; Felice, P.; Alissa, R.; Worthington, H.; Coulthard, P. Effectiveness of sinus lift procedures for dental implant rehabilitation: A Cochrane systematic review. J. Oral Implantol. 2010, 3, 7–26. [Google Scholar]
- Kirmeier, R.; Payer, M.; Wehrschuetz, M.; Jakse, N.; Platzer, S.; Lorenzoni, M. Evaluation of three-dimensional changes after sinus floor augmentation with different grafting materials. Clin. Oral Implants Res. 2008, 19, 366–372. [Google Scholar] [CrossRef]
- Hatano, N.; Shimizu, Y.; Ooya, K. A Clinical Long-Term Radiographic Evaluation of Graft Height Changes After Maxillary Sinus Floor Augmentation with a 2:1 Autogenous Bone/Xenograft Mixture and Simultaneous Placement of Dental Implants. Clin. Oral Implants Res. 2004, 15, 339–345. [Google Scholar] [CrossRef]
- Si, M.S.; Jia-Ji, M.; Long-Fei, Z.; Ying-Xin, G.; Shi-Chong, Q.; Hong-Chang, L. Osteotome Sinus Floor Elevation with and without Grafting: An Animal Study in Labrador Dogs. Clin. Oral Implants Res. 2015, 26, 197–203. [Google Scholar] [CrossRef]
- Sung-Han, S.; Byung-Ho, C.; Jingxu, L.; Seung-Mi, J.; Xuan, F. Effects of Sinus Membrane Elevation on Bone Formation Around Implants Placed in the Maxillary Sinus Cavity: An Experimental Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 684–687. [Google Scholar] [CrossRef]
- Schwarz, F.; Herten, M.; Bieling, K.; Becker, J. Crestal Bone Changes at Nonsubmerged Implants (Camlog) With Different Machined Collar Lengths: A Histomorphometric Pilot Study in Dogs. Int. J. Oral Maxillofac. Implants 2008, 23, 335–342. [Google Scholar]
- Gabbert, O.; Koob, A.; Schmitter, M.; Rammelsberg, P. Implants Placed in Combination with an Internal Sinus Lift without Graft Material: An Analysis of Short-Term Failure. J. Clin. Periodontol. 2009, 36, 177–183. [Google Scholar] [CrossRef]
- Reiser, G.M.; Rabinovitz, Z.; Bruno, J.; Damoulis, P.D.; Griffin, T.J. Evaluation of maxillary sinus membrane response following elevation with the crestal osteotome technique in human cadavers. Int. J. Oral Maxillofac. Implants 2001, 16, 833–840. [Google Scholar] [PubMed]
- Engelke, W.; Deckwer, I. Endoscopically controlled sinus floor augmentation. A preliminary report. Clin. Oral Implants Res. 1997, 8, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Jae-Hyung, J.; Byung-Ho, C.; Seung-Mi, J.; Jingxu, L.; Seoung-Ho, L.; Hyeon-Jung, L. A retrospective study of the effects on sinus complications of exposing dental implants to the maxillary sinus cavity. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 103, 623–625. [Google Scholar] [CrossRef]
- Millán, A.M.; Álvarez, R.B.; Montori, M.P.; González, M.G.; García-Martín, D.S.; Ríos-Carrasco, B.; Monticelli, F.; Ríos-Santos, J.V.; Fernández-Palacín, A. Assessment of the Simultaneous Use of Biomaterials in Transalveolar Sinus Floor Elevation: Prospective Randomized Clinical Trial in Humans. Int. J. Environ. Res. Public Health 2020, 17, 1888. [Google Scholar] [CrossRef]
- Tabrizi, R.; Amid, R.; Taha, O.B.; Khorshidi, H.; Langner, N.J. Effects of exposing dental implant to the maxillary sinus cavity. J. Craniofac. Surg. 2012, 23, 767–769. [Google Scholar] [CrossRef]
- Taschieri, S.; Corbella, S.; Saita, M.; Tsesis, I.; Del Fabbro, M. Osteotome-Mediated Sinus Lift without Grafting Material: A Review of Literature and a Technique Proposal. Int. J. Dent. 2012, 2012, 849093. [Google Scholar] [CrossRef]
- Kovacs, M.; Fejérdy, P.; Dobó, N.C. Metal artefact on head and neck cone-beam CT images. Fogorv. Szle. 2008, 101, 171–178. [Google Scholar]
- Fornell, J.; Lars-Åke, J.; Bolin, A.; Isaksson, S.; Sennerby, L. Flapless, CBCT-guided osteotome sinus floor elevation with simultaneous implant installation. I: Radiographic examination and surgical technique. A prospective 1-year follow-up. Clin. Oral Implants Res. 2012, 23, 28–34. [Google Scholar] [CrossRef]
- El Hage, M.; Balleri, P.; Veltri, M.; Nuti, N.; Ferrari, M. Implant Placement in Combination with Sinus Membrane Elevation without Biomaterials: A 1-Year Study on 15 Patients. Clin. Implants Dent. Relat. Res. 2012, 14, 682–689. [Google Scholar]
- Nurdin, N.; Najm, S.A.; Bischof, M.; Nedir, R. Osteotome Sinus Floor Elevation without Grafting: A 10-Year Study of Cone Beam Computerized Tomography vs Periapical Radiography. Int. J. Periodontics Restor. Dent. 2019, 39, e89–e97. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrés-García, R.; Ríos-Santos, J.V.; Herrero-Climent, M.; Bullón, P.; Fernández-Farhall, J.; Gómez-Menchero, A.; Fernández-Palacín, A.; Ríos-Carrasco, B. Sinus Floor Elevation via an Osteotome Technique without Biomaterials. Int. J. Environ. Res. Public Health 2021, 18, 1103. https://doi.org/10.3390/ijerph18031103
Andrés-García R, Ríos-Santos JV, Herrero-Climent M, Bullón P, Fernández-Farhall J, Gómez-Menchero A, Fernández-Palacín A, Ríos-Carrasco B. Sinus Floor Elevation via an Osteotome Technique without Biomaterials. International Journal of Environmental Research and Public Health. 2021; 18(3):1103. https://doi.org/10.3390/ijerph18031103
Chicago/Turabian StyleAndrés-García, Rodrigo, José Vicente Ríos-Santos, Mariano Herrero-Climent, Pedro Bullón, Javier Fernández-Farhall, Alberto Gómez-Menchero, Ana Fernández-Palacín, and Blanca Ríos-Carrasco. 2021. "Sinus Floor Elevation via an Osteotome Technique without Biomaterials" International Journal of Environmental Research and Public Health 18, no. 3: 1103. https://doi.org/10.3390/ijerph18031103
APA StyleAndrés-García, R., Ríos-Santos, J. V., Herrero-Climent, M., Bullón, P., Fernández-Farhall, J., Gómez-Menchero, A., Fernández-Palacín, A., & Ríos-Carrasco, B. (2021). Sinus Floor Elevation via an Osteotome Technique without Biomaterials. International Journal of Environmental Research and Public Health, 18(3), 1103. https://doi.org/10.3390/ijerph18031103