
Factors Associated with Psychological Distress in French Medical Students during the COVID-19 Health Crisis: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Target Population
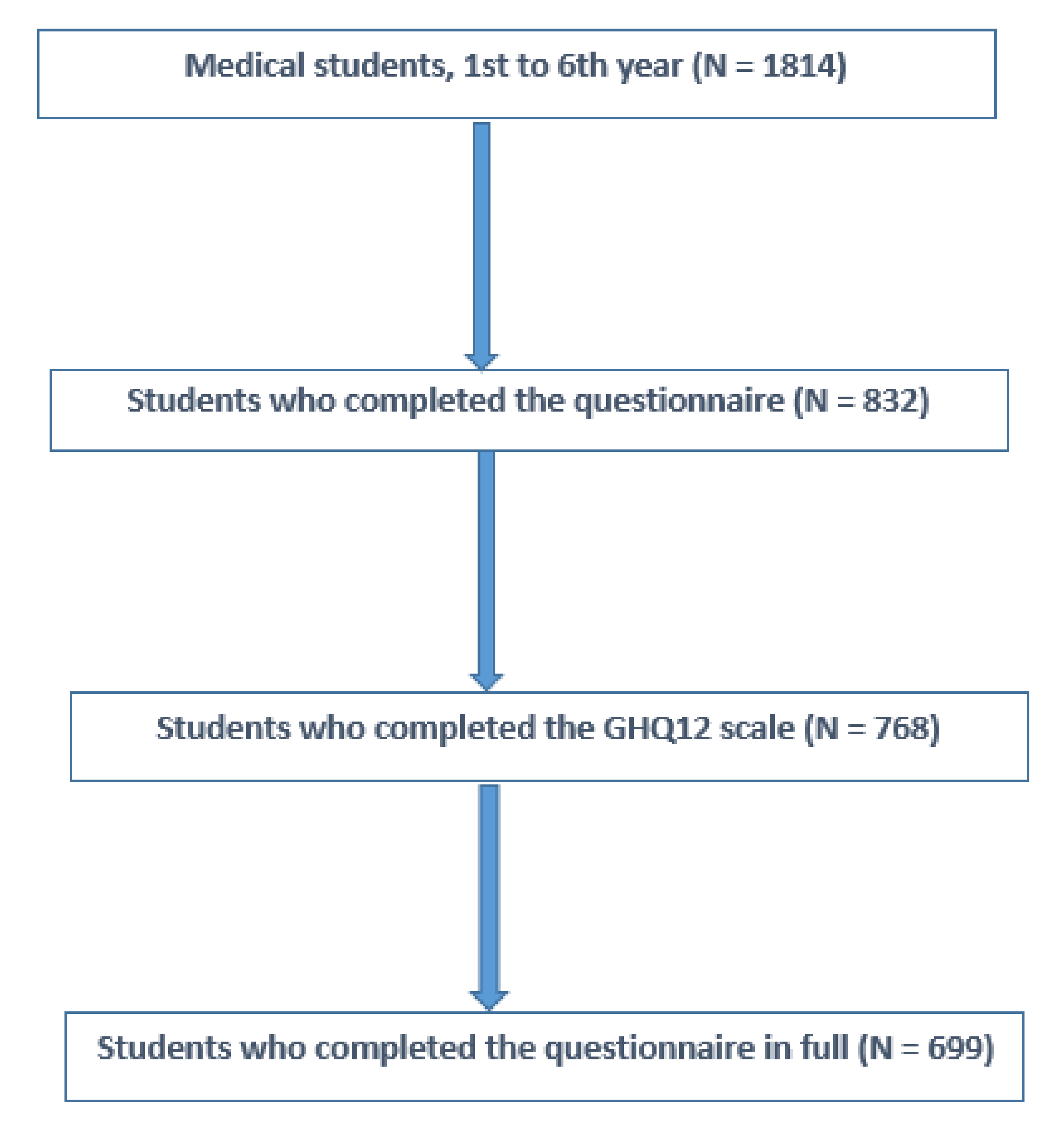
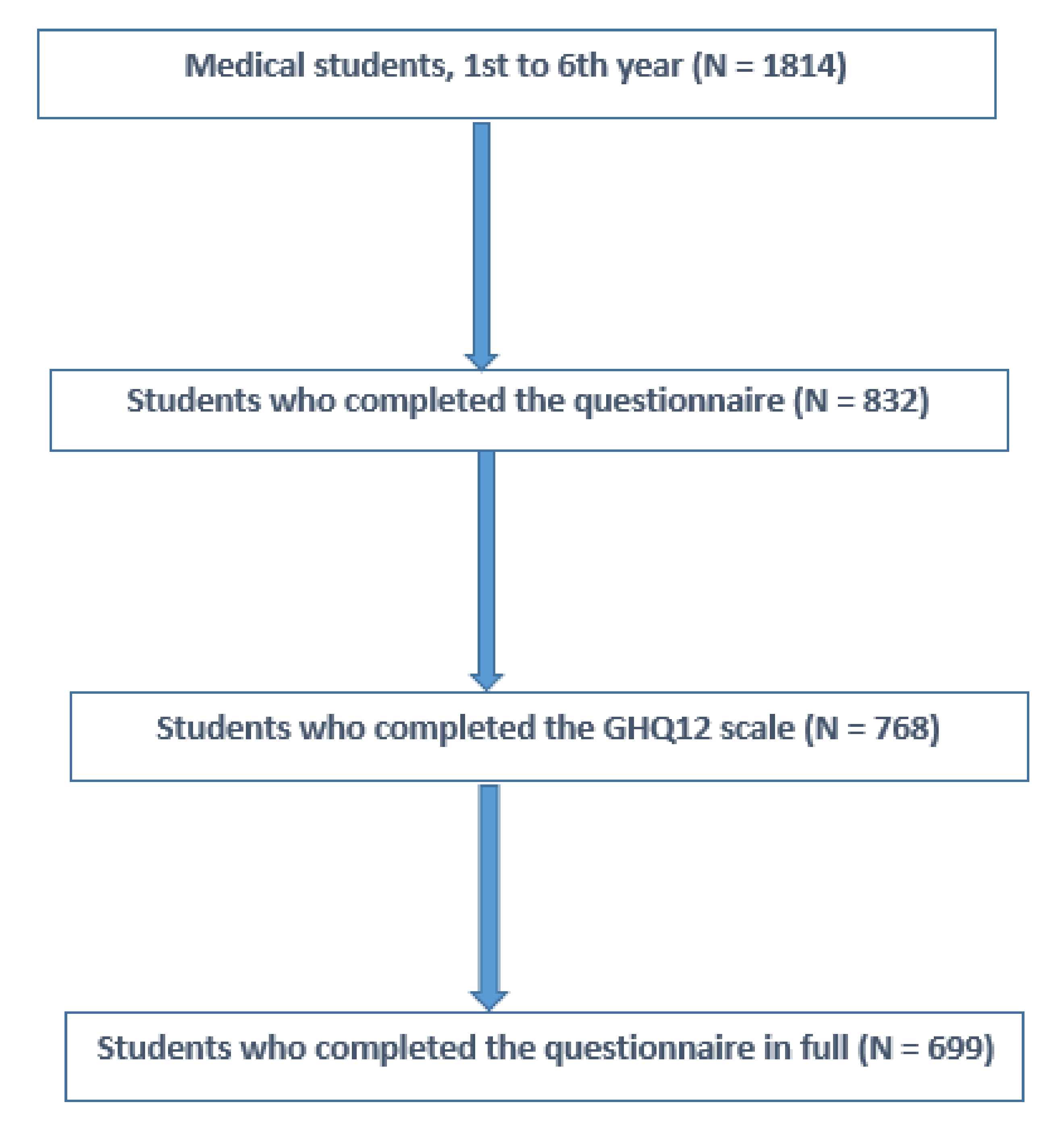
2.2. Study Sample
2.3. Measurements
2.4. Analysis
3. Results
3.1. Sociodemographic, Educational and Medical Characteristics
3.2. Prevalence of Psychological Distress
3.3. Relations between Psychological Distress and Educational and Medical Factors on Univariate Analysis
- Female gender, PR = 1.12 (1.02–1.23)
- Age, PR = 0.98 (0.96–0.99);
- 1st year of medical school (major), PR = 1.11 (1.01–1.21);
- Financial difficulties, PR = 1.11 (1.01–1.22);
- Psychological trauma during the health crisis COVID-19, PR = 1.21 (1.11–1.29);
- History of anxiety disorder, PR = 1.12 (1.03–1.22);
- History of depression, PR = 1.13 (1.03–1.24);
- Change in smoking, PR = 1.08 (0.99–1.19);
- Change in alcohol consumption, PR = 1.08 (1.01–1.16);
- Sense of mutual support and cooperation, PR = 0.80 (0.75–0.86);
- Impression of recognized work, PR = 0.75 (0.69–0.82);
- Hospital internship within the last three months, PR = 0.91 (0.84–0.98);
- Hospital internship on a COVID-19 ward within the last three months, PR = 0.90 (0.81–0.99);
- Experiencing difficulties with online learning, PR = 1.64 (1.39–1.94).
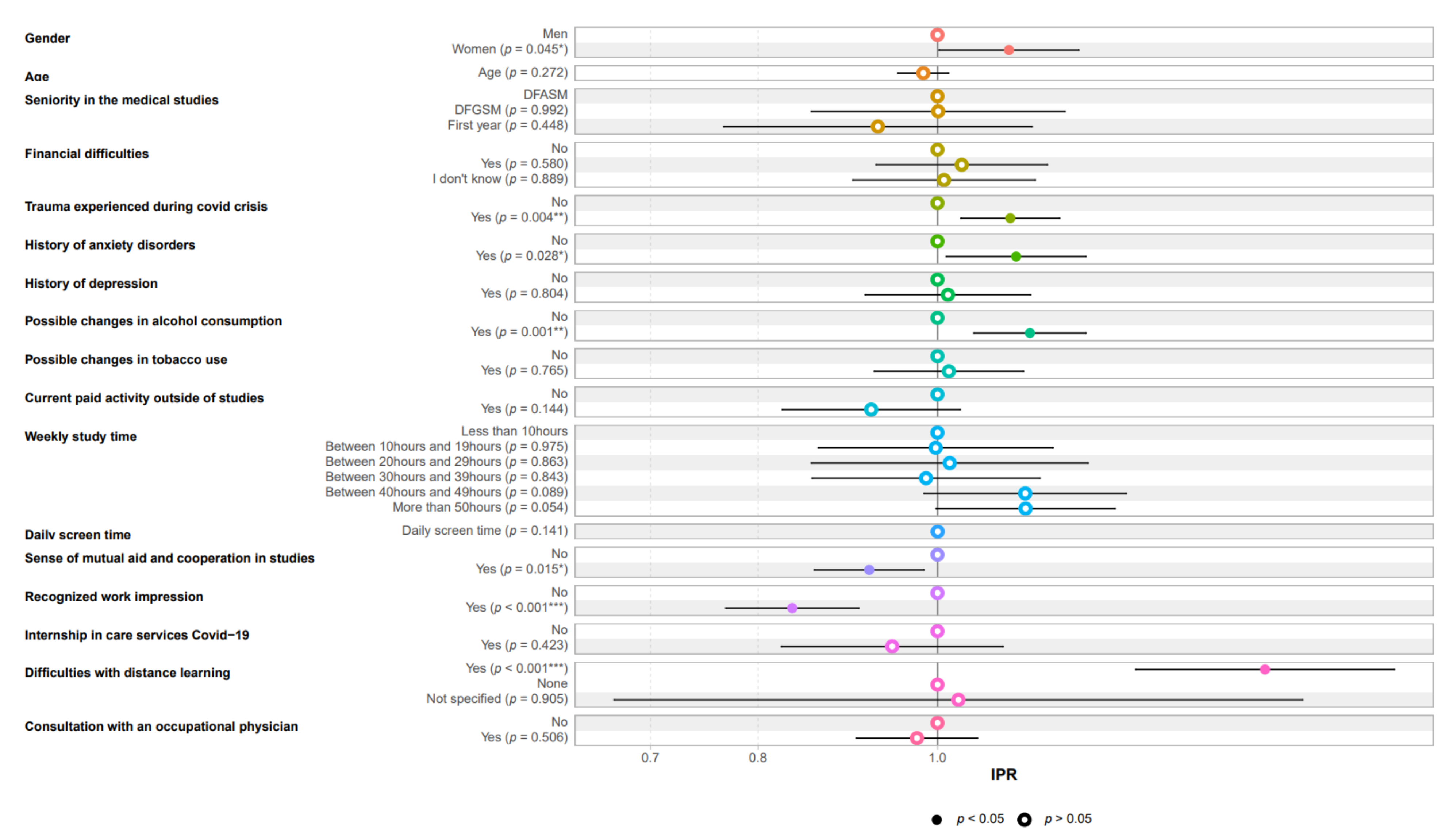
3.4. Relations between Psychological Distress and Educational and Medical Factors in Multivariate Analysis
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef] [Green Version]
- Mizumoto, K.; Chowell, G. Estimating Risk for Death from 2019 Novel Coronavirus Disease, China, January–February 2020. Emerg. Infect Dis. 2020, 26, 1251. [Google Scholar] [CrossRef]
- Puthran, R.; Zhang, M.W.B.; Tam, W.W.; Ho, R.C. Prevalence of depression amongst medical students: A meta-analysis. Med. Educ. Avr. 2016, 50, 456–468. [Google Scholar] [CrossRef]
- Adams, J. Straining to describe and tackle stress in medical students. Med. Educ. 2004, 38, 463–464. [Google Scholar] [CrossRef]
- Bayram, N.; Bilgel, N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 667–672. [Google Scholar] [CrossRef]
- Hill, M.R.; Goicochea, S.; Merlo, L.J. In their own words: Stressors facing medical students in the millennial generation. Med. Educ. Online 2018, 23, 1530558. [Google Scholar] [CrossRef] [Green Version]
- Rosenthal, J.M.; Okie, S. White Coat, Mood Indigo—Depression in Medical School. N. Engl. J. Med. 2005, 353, 1085–1088. [Google Scholar] [CrossRef] [Green Version]
- Sherina, M.S.; Rampal, L.; Kaneson, N. Psychological stress among undergraduate medical students. Med. J. Malays. 2004, 59, 207–211. [Google Scholar]
- Yusoff, M.S.B.; Rahim, A. Stress, Stressors and Coping Strategies: First Year Medical Students in Malaysian Public Universities; VDM Publishing: Saarbrücken, Germany, 2011. [Google Scholar]
- Dyrbye, L.N.; Thomas, M.R.; Shanafelt, T.D. Systematic Review of Depression, Anxiety, and Other Indicators of Psychological Distress Among, U.S. and Canadian Medical Students. Acad. Med. Avr. 2006, 81, 354–373. [Google Scholar] [CrossRef]
- Mousa, O.Y.; Dhamoon, M.S.; Lander, S.; Dhamoon, A.S. The MD Blues: Under-Recognized Depression and Anxiety in Medical Trainees. PLoS ONE 2016, 11, e0156554. [Google Scholar] [CrossRef] [Green Version]
- Yusoff, M.S.B.; Abdul Rahim, A.F.; Baba, A.A.; Ismail, S.B.; Mat Pa, M.N.; Esa, A.R. The impact of medical education on psychological health of students: A cohort study. Psychol. Health Med. 2013, 18, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Dutheil, F.; Aubert, C.; Pereira, B.; Dambrun, M.; Moustafa, F.; Mermillod, M.; Baker, J.S.; Trousselard, M.; Lesage, F.-X.; Navel, V. Suicide among physicians and health-care workers: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0226361. [Google Scholar] [CrossRef] [Green Version]
- Wong, J.G.W.S.; Cheung, E.P.T.; Cheung, V.; Cheung, C.; Chan, M.T.Y.; Chua, S.E.; McAlonan, G.; Tsang, K.W.; Ip, M.S.M. Psychological responses to the SARS outbreak in healthcare students in Hong Kong. Med. Teach. 2004, 26, 657–659. [Google Scholar] [CrossRef]
- Jaisoorya, T.S.; Janardhan Reddy, Y.C.; Nair, B.S.; Rani, A.; Menon, P.G.; Revamma, M.; Jeevan, C.R.; Radhakrishnan, K.S.; Jose, V.; Thennarasu, K. Prevalence and correlates of obsessive-compulsive disorder and subthreshold obsessive-compulsive disorder among college students in Kerala, India. Indian J. Psychiatry 2017, 59, 56–62. [Google Scholar] [CrossRef]
- Ishii, T.; Tachikawa, H.; Shiratori, Y.; Hori, T.; Aiba, M.; Kuga, K.; Arai, T. What kinds of factors affect the academic outcomes of university students with mental disorders? A retrospective study based on medical records. Asian J. Psychiatry 2018, 32, 67–72. [Google Scholar] [CrossRef]
- Point Épidémio Régional Spécial COVID 19 Auvergne Rhône Alpes 29 Octobre 2020. Sante Publique France, 2020. Available online: https://www.auvergne-rhone-alpes.ars.sante.fr/system/files/2020-10/20201029_PER_COVID19_ARA.VF__0.pdf (accessed on 3 December 2021).
- Lesage, F.-X.; Martens-Resende, S.; Deschamps, F.; Berjot, S. Validation of the General Health Questionnaire (GHQ-12] adapted to a work-related context. Open J. Prev. Med. 2011, 1, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, D. User’s Guide to the General Health Questionnaire. Windsor. 1988. Available online: https://ci.nii.ac.jp/naid/10016919943/ (accessed on 29 July 2021).
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO study of mental illness in general health care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- Yusoff, M.S.B. The validity of two malay versions of the general health questionnaire (ghq) in detecting distressed medical students. ASEAN J. Psychiatry. 2010, 11, 135–142. [Google Scholar]
- Goldberg, D. The Detection of Minor Psychiatric Illness by Questionnaire; Oxford University Press: Oxford, UK, 1972. [Google Scholar]
- Zou, G. A Modified Poisson Regression Approach to Prospective Studies with Binary Data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- Moffat, K.J.; McConnachie, A.; Ross, S.; Morrison, J.M. First year medical student stress and coping in a problem-based learning medical curriculum. Med. Educ. 2004, 38, 482–491. [Google Scholar] [CrossRef]
- Saraswathi, I.; Saikarthik, J.; Senthil Kumar, K.; Madhan Srinivasan, K.; Ardhanaari, M.; Gunapriya, R. Impact of COVID-19 outbreak on the mental health status of undergraduate medical students in a COVID-19 treating medical college: A prospective longitudinal study. PeerJ. 2020, 8, e10164. [Google Scholar] [CrossRef]
- Glowacz, F.; Schmits, E. Psychological distress during the COVID-19 lockdown: The young adults most at risk. Psychiatry Res. 2020, 293, 113486. [Google Scholar] [CrossRef]
- Seedat, S.; Scott, K.M.; Angermeyer, M.C.; Berglund, P.; Bromet, E.J.; Brugha, T.S.; Demyttenaere, K.; de Girolamo, G.; Haro, J.M.; Jin, R.; et al. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. AMA Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Waseem, M.; Aziz, N.; Arif, M.U.; Noor, A.; Mustafa, M.; Khalid, Z. Impact of post-traumatic stress of covid-19 on mental wellbeing of undergraduate medical students in pakistan. Pafmj. 2020, 70, S220–S224. [Google Scholar]
- Lasalvia, A.; Bonetto, C.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Amaddeo, F. Psychological impact of COVID-19 pandemic on healthcare workers in a highly burdened area of north-east Italy. Epidemiol. Psychiatry Sci. 2020, 30, e1. [Google Scholar] [CrossRef]
- Clay, J.M.; Parker, M.O. Alcohol use and misuse during the COVID-19 pandemic: A potential public health crisis? Lancet. Public. Health 2020, 5, e259. [Google Scholar] [CrossRef]
- O’Byrne, L.; Gavin, B.; McNicholas, F. Medical students and COVID-19: The need for pandemic preparedness. J. Med. Ethics 2020, 46, 623–626. Available online: https://covid19.elsevierpure.com/en/publications/medical-students-and-covid-19-the-need-for-pandemic-preparedness (accessed on 6 August 2021). [CrossRef]
- Bamber, M.D.; Kraenzle Schneider, J. Mindfulness-based meditation to decrease stress and anxiety in college students: A narrative synthesis of the research. Educ. Res. Rev. 2016, 18, 1–32. [Google Scholar] [CrossRef]
- Al-Balas, M.; Al-Balas, H.I.; Jaber, H.M.; Obeidat, K.; Al-Balas, H.; Aborajooh, E.A.; Al-Taher, R.; Al-Bala, B. Distance learning in clinical medical education amid COVID-19 pandemic in Jordan: Current situation, challenges, and perspectives. BMC Med. Educ. 2020, 341. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, Y.; Ochi, K.; Tokumasu, K.; Obika, M.; Hagiya, H.; Kataoka, H.; Otsuka, F. Impact of the COVID-19 Pandemic on the Psychological Distress of Medical Students in Japan: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e25232. [Google Scholar] [CrossRef]
- Długosz, P. The Relationship between Mental Health, Educational Burnout and Strategies for Coping with Stress among Students. A Cross-Sect. Study Polan. 2021, 18, 10827. [Google Scholar] [CrossRef]
- Arima, M.; Takamiya, Y.; Furuta, A.; Siriratsivawong, K.; Tsuchiya, S.; Izumi, M. Factors associated with the mental health status of medical students during the COVID-19 pandemic: A cross-sectional study in Japan. BMJ Open 2020, 10, e043728. [Google Scholar] [CrossRef]
- Alsubaie, M.M.; Stain, H.J.; Webster, L.A.D.; Wadman, R. The role of sources of social support on depression and quality of life for university students. Int. J. Adolesc. Youth 2019, 24, 484–496. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.C. Friends support as a mediator in the association between depressive symptoms and self-stigma among university students in South Korea. Int. J. Ment. Health 2020, 49, 247–253. [Google Scholar] [CrossRef]
- Saddik, B.; Hussein, A.; Sharif-Askari, F.S.; Kheder, W.; Temsah, M.-H.; Koutaich, R.A.; Haddad, E.S.; Al-Roub, N.M.; Marhoon, F.A.; Hamid, Q.; et al. Increased levels of anxiety among medical and non-medical university students during the COVID-19 pandemic in the United Arab Emirates. medRxiv 2020, arXiv:2020.05.10.2009693313. [Google Scholar]
- Ma, Z.; Zhao, J.; Li, Y.; Chen, D.; Wang, T.; Zhang, Z.; Chen, Z.; Yu, Q.; Jiang, J.; Fan, F.; et al. Mental health problems and correlates among 746 217 college students during the coronavirus disease 2019 outbreak in China. Epidemiol. Psychiaty Sci. 2020, 29, e181. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Pélissier, C.; Fontana, L.; For, T.E.; Vohito, M.; Sellier, B.; Perrier, C.; Fontana, L.; Fort, E.; Vohito, M.; Sellier, B.; et al. Impaired mental well-being and psychosocial risk: A cross-sectional study in female nursing home direct staff. BMJ Open 2015, 5, e007190. [Google Scholar] [CrossRef] [Green Version]
- Vegchel, N.; van de Jonge, J.; Bakker, A.B.; Schaufeli, W.B. Testing global and specific indicators of rewards in the Effort-Reward Imbalance Model: Does it make any difference? Eur. J. Work. Organ. Psychol. 2002, 11, 403–421. [Google Scholar] [CrossRef]
- Essadek, A.; Rabeyron, T. Mental health of French students during the Covid-19 pandemic. J. Affect. Disord. 2020, 277, 392–393. [Google Scholar] [CrossRef]
- Owens, M.R.; Brito-Silva, F.; Kirkland, T.; Moore, C.E.; Davis, K.E.; Patterson, M.A.; Miketinas, D.C.; Tucker, W.J. Prevalence and Social Determinants of Food Insecurity among College Students during the COVID-19 Pandemic. Nutrients 2020, 12, 2515. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Leung, C.W. Food Insecurity and COVID-19: Disparities in Early Effects for US Adults. Nutrients 2020, 12, 1648. [Google Scholar] [CrossRef]
- Maser, B.; Danilewitz, M.; Guérin, E.; Findlay, L.; Frank, E. Medical Student Psychological Distress and Mental Illness Relative to the General Population: A Canadian Cross-Sectional Survey. Acad. Med. 2019, 94, 1781–1791. [Google Scholar] [CrossRef]
- Essangri, H.; Sabir, M.; Benkabbou, A.; Majbar, M.A.; Amrani, L.; Ghannam, A.; Lekehal, B.; Mohsine, R.; Souadka, A. Predictive Factors for Impaired Mental Health among Medical Students during the Early Stage of the COVID-19 Pandemic in Morocco. Am. J. Trop. Med. Hyg. 2020, 104, 95–102. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Psychological Distress | |||||||
|---|---|---|---|---|---|---|---|
| Total | Yes (N = 625, 75.1%) | No (N = 207, 24.9%) | |||||
| N | % | N | % | N | % | ||
| Gender | Women | 609 | 73.2 | 470 | 77.2 | 139 | 22.8 |
| Men | 223 | 26.8 | 155 | 69.5 | 68 | 30.5 | |
| Age | 18 years | 248 | 29.8 | 197 | 79.4 | 51 | 20.6 |
| 19–20 years | 339 | 40.7 | 248 | 73.2 | 91 | 26.8 | |
| 21 years and over | 244 | 29.4 | 180 | 73.8 | 64 | 26.2 | |
| Family situation | Single | 623 | 75.0 | 466 | 25.2 | 157 | 74.8 |
| In a couple | 203 | 24.4 | 155 | 76.3 | 48 | 23.7 | |
| Widowed, Separated, Divorced | 5 | 0.6 | 4 | 80.0 | 1 | 20.0 | |
| Living alone | Yes | 32 | 3.8 | 22 | 68.8 | 10 | 31.2 |
| No | 799 | 96.1 | 196 | 24.5 | 603 | 85.5 | |
| Financial difficulties | Low | 684 | 84.3 | 519 | 75.9 | 165 | 24.1 |
| High | 78 | 9.6 | 66 | 84.6 | 12 | 15.4 | |
| Don’t know | 49 | 6.0 | 40 | 81.6 | 9 | 18.4 | |
| Perceived health status | Poor to mediocre | 99 | 13.3 | 97 | 98.0 | 2 | 2.0 |
| Moderate | 368 | 49.6 | 322 | 87.5 | 46 | 12.5 | |
| High, very high | 275 | 37.1 | 183 | 33.4 | 92 | 66.5 | |
| Perceived stress level | Low to moderate | 368 | 49.6 | 251 | 68.2 | 117 | 31.8 |
| High | 374 | 50.4 | 351 | 93.9 | 23 | 6.1 | |
| Trauma experienced during the COVID-19 crisis | No | 510 | 68.7 | 388 | 76.1 | 122 | 29.9 |
| Yes | 232 | 31.3 | 214 | 92.2 | 18 | 7.8 | |
| History of anxiety disorders | No | 650 | 87.6 | 519 | 79.8 | 131 | 20.1 |
| Yes | 92 | 12.4 | 83 | 90.2 | 9 | 9.8 | |
| History of depression | No | 688 | 92.7 | 553 | 80.4 | 135 | 19.6 |
| Yes | 54 | 7.3 | 49 | 90.7 | 5 | 903 | |
| Presence of suicidal ideation | No | 631 | 85.2 | 494 | 78.3 | 137 | 21.7 |
| Yes | 109 | 14.7 | 106 | 97.3 | 3 | 2.7 | |
| History of suicide attempts | No | 684 | 95.9 | 549 | 80.3 | 135 | 19.7 |
| Yes | 29 | 4.1 | 28 | 96.5 | 1 | 3.5 | |
| Average sleep duration | <6 h | 189 | 25.6 | 172 | 91.0 | 17 | 9.0 |
| 7–8 h | 494 | 67.0 | 389 | 78.8 | 105 | 21.2 | |
| ≥9 h | 54 | 7.3 | 37 | 68.5 | 17 | 31.5 | |
| Practice of a sport activity | Never | 219 | 29.7 | 189 | 86.3 | 30 | 13.7 |
| Rarely | 180 | 24.4 | 158 | 87.8 | 22 | 12.2 | |
| Once a week | 139 | 18.8 | 103 | 74.1 | 36 | 25.9 | |
| Several times a week | 164 | 22.2 | 124 | 75.6 | 40 | 24.4 | |
| Every day | 35 | 4.7 | 24 | 68.6 | 11 | 31.4 | |
| Frequency of alcohol consumption | Never | 324 | 44.0 | 267 | 82.4 | 57 | 17.6 |
| Less than once a month | 186 | 25.2 | 154 | 82.8 | 32 | 17.2 | |
| Between once a month and once a week | 196 | 26.6 | 156 | 79.6 | 40 | 20.4 | |
| Several times a week | 31 | 4.2 | 21 | 67.7 | 10 | 32.3 | |
| Possible changes in alcohol consumption | No, I never drink alcohol | 298 | 40.4 | 245 | 82.2 | 53 | 17.8 |
| No, I kept the same alcohol consumption | 188 | 25.5 | 141 | 75.0 | 47 | 25.0 | |
| Yes, I have cut down on my drinking a bit | 215 | 29.2 | 181 | 84.2 | 34 | 15.8 | |
| Yes, I have increased my alcohol consumption a bit | 36 | 4.9 | 31 | 86.1 | 5 | 13.9 | |
| Smoking | No | 654 | 88.8 | 525 | 80.3 | 129 | 17.7 |
| Yes | 83 | 11.2 | 73 | 87.9 | 10 | 12.1 | |
| Possible changes in smoking | No, I never smoke | 638 | 86.6 | 513 | 80.4 | 125 | 19.6 |
| No, I kept the same smoking level | 19 | 2.6 | 4 | 78.9 | 15 | 21.1 | |
| Yes, I have cut down on smoking a bit | 21 | 2.8 | 5 | 23.8 | 16 | 76.2 | |
| Yes, I have increased smoking a bit | 59 | 8.0 | 54 | 91.5 | 5 | 8.5 | |
| Cannabis use | No | 698 | 94.7 | 563 | 80.7 | 135 | 19.3 |
| Yes | 39 | 5.3 | 35 | 89.7 | 4 | 10.3 | |
| Possible changes in cannabis use | Never | 696 | 94.4 | 562 | 80.7 | 134 | 19.3 |
| No change | 25 | 3.4 | 22 | 88.0 | 3 | 12.0 | |
| Decrease | 8 | 1.1 | 7 | 12.5 | 1 | 87.5 | |
| Increase | 8 | 1.1 | 7 | 12.5 | 1 | 87.5 | |
| Date of last consultation with a general practitioner | <12 months | 165 | 22.4 | 125 | 75.8 | 40 | 24.2 |
| ≥12 months | 211 | 28.6 | 166 | 78.7 | 45 | 21.3 | |
| Never consulted a general practitioner | 362 | 49.0 | 307 | 84.8 | 55 | 15.2 | |
| Psychological Distress | |||||||
|---|---|---|---|---|---|---|---|
| Total | Yes (N = 625, 75.1%) | No (N = 207, 24.9%) | |||||
| N | % | N | % | N | % | ||
| Seniority in medical studies | 1st year | 492 | 59.4 | 379 | 77.0 | 113 | 23.0 |
| 2nd and 3rd year | 128 | 15.4 | 94 | 73.4 | 34 | 26.6 | |
| 4th, 5th, and 6th year | 209 | 25.2 | 152 | 72.7 | 57 | 27.3 | |
| Weekly study time (hours) | <10 h | 79 | 10.8 | 64 | 19.0 | 15 | 81.0 |
| 10–19 h | 72 | 9.9 | 56 | 77.8 | 16 | 22.2 | |
| 20–29 h | 63 | 8.6 | 47 | 74.6 | 16 | 25.4 | |
| 30–39 h | 100 | 13.7 | 74 | 74.0 | 26 | 26.0 | |
| 40–49 h | 88 | 12.1 | 77 | 87.5 | 11 | 12.5 | |
| >50 h | 326 | 44.8 | 272 | 83.4 | 54 | 16.6 | |
| Sense of mutual support and cooperation | Yes | 382 | 52.5 | 277 | 72.5 | 105 | 27.5 |
| No | 346 | 47.5 | 313 | 90.5 | 33 | 9.5 | |
| Impression of recognized work | Yes | 286 | 60.7 | 192 | 67.1 | 94 | 32.9 |
| No | 442 | 39.3 | 398 | 90.0 | 44 | 10.0 | |
| Perceived level of stress related to studies | Low to moderate | 171 | 23.5 | 88 | 51.5 | 83 | 48.5 |
| High | 558 | 76.5 | 503 | 90.1 | 55 | 9.9 | |
| Face-to-face courses in the last 3 months | No | 541 | 74.3 | 443 | 81.9 | 98 | 18.1 |
| Yes, 1 day a week on average | 139 | 19.1 | 110 | 79.1 | 29 | 20.9 | |
| Yes, 2 days a week on average | 32 | 4.4 | 27 | 84.4 | 5 | 15.6 | |
| Yes, 3 days per week on average | 16 | 2.2 | 10 | 62.5 | 6 | 37.5 | |
| Hospital internship in the last 3 months | No | 439 | 60.3 | 369 | 84.0 | 70 | 16.0 |
| Yes | 289 | 39.7 | 221 | 76.5 | 68 | 23.5 | |
| Internship in COVID-19 care units | No | 567 | 77.9 | 469 | 82.7 | 98 | 17.3 |
| Yes | 161 | 22.1 | 121 | 75.2 | 40 | 24.8 | |
| Difficulties in following distance learning courses due to: | |||||||
| Time management, personal life, or occupational life | No | 76 | 12.7 | 184 | 84.4 | 34 | 15.6 |
| Yes | 524 | 87.3 | 399 | 88.7 | 43 | 11.3 | |
| Workload | No | 228 | 38.0 | 180 | 78.9 | 48 | 21.1 |
| Yes | 372 | 62.0 | 343 | 92.2 | 29 | 7.8 | |
| Lack of communication with the teaching staff | No | 341 | 56.8 | 291 | 85.34 | 50 | 14.66 |
| Yes | 259 | 43.2 | 232 | 89.6 | 27 | 10.4 | |
| Work location | No | 378 | 63.0 | 326 | 86.2 | 52 | 13.8 |
| Yes | 222 | 37.0 | 197 | 88.7 | 25 | 11.3 | |
| Lack of communication with other students | No | 481 | 80.2 | 414 | 86.0 | 67 | 14.0 |
| Yes | 119 | 19.8 | 109 | 91.6 | 10 | 8.4 | |
| Equipment | No | 524 | 87.3 | 455 | 86.8 | 69 | 13.2 |
| Yes | 76 | 12.7 | 68 | 89.5 | 8 | 10.5 | |
| Paid work outside the framework of studies | No | 570 | 78.3 | 466 | 81.8 | 104 | 18.2 |
| Yes | 158 | 11.7 | 124 | 78.5 | 34 | 21.5 | |
| Psychological Distress | |||
|---|---|---|---|
| Variables | PR [CI] | Adjusted PR [CI] | |
| Gender | Women (ref: Men) | 1.12 [1.02–1.23] * | 1.09 [1.00–1.19] * |
| Age | 0.98 [0.96–0.99] * | 0.98 [0.95–1.01] | |
| Seniority in the medical studies | 1st year medicine main stream (ref: 4th, 5th, and 6th year) | 1.11 [1.01–1.21] * | 0.92 [0.77–1.12] |
| Financial difficulties | Yes (ref: NO) | 1.11 [1.01–1.22] * | 1.03 [0.93–1.15] |
| Trauma experienced during the COVID-19 crisis | Yes (ref: NO) | 1.21 [1.11–1.29] **** | 1.10 [1.03–1.16] ** |
| History of anxiety disorder | Yes (ref: NO) | 1.12 [1.03–1.22] ** | 1.11 [1.01–1.20] * |
| History of depression | Yes (ref: NO) | 1.13 [1.03–1.24] * | 1.01 [0.91–1.12] |
| Possible change in alcohol consumption | Yes (ref: NO) | 1.08 [1.01–1.16] * | 1.12 [1.05–1.20] ** |
| Possible change in smoking | Yes (ref: NO) | 1.08 [0.99–1.19] | 1.01 [0.92–1.11] |
| Paid work outside the framework of studies | Yes (ref: NO) | 0.90 [0.81–1.00] | 0.92 [0.82–1.03] |
| Sense of mutual support and cooperation | Yes (ref: NO) | 0.80 [0.75–0.86] **** | 0.92 [0.86–0.98] * |
| Impression of recognized work | Yes (ref: NO) | 0.75 [0.69–0.82] **** | 0.84 [0.77–0.91] *** |
| Hospital internship in the last 3 months | Yes (ref: NO) | 0.91 [0.84–0.98] * | / |
| Internship in COVID-19 care units | Yes (ref: NO) | 0.90 [0.81–0.99] * | 0.94 [0.82–1.08] |
| Difficulties in following distance learning courses | Yes (ref: NO) | 1.64 [1.39–1.94] **** | 1.50 [1.28–1.77] *** |
| Consultation with a general practitioner | Yes (ref: NO) | 0.91 [0.85–0.98] * | 0.97 [0.90–1.05] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelissier, C.; Viale, M.; Berthelot, P.; Poizat, B.; Massoubre, C.; Tiffet, T.; Fontana, L. Factors Associated with Psychological Distress in French Medical Students during the COVID-19 Health Crisis: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12951. https://doi.org/10.3390/ijerph182412951
Pelissier C, Viale M, Berthelot P, Poizat B, Massoubre C, Tiffet T, Fontana L. Factors Associated with Psychological Distress in French Medical Students during the COVID-19 Health Crisis: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(24):12951. https://doi.org/10.3390/ijerph182412951
Chicago/Turabian StylePelissier, Carole, Manon Viale, Philippe Berthelot, Brigitte Poizat, Catherine Massoubre, Theophile Tiffet, and Luc Fontana. 2021. "Factors Associated with Psychological Distress in French Medical Students during the COVID-19 Health Crisis: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 24: 12951. https://doi.org/10.3390/ijerph182412951
APA StylePelissier, C., Viale, M., Berthelot, P., Poizat, B., Massoubre, C., Tiffet, T., & Fontana, L. (2021). Factors Associated with Psychological Distress in French Medical Students during the COVID-19 Health Crisis: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(24), 12951. https://doi.org/10.3390/ijerph182412951