
Mechanisms of Cannabidiol (CBD) in Cancer Treatment: A Review





Abstract
:Simple Summary
Abstract
1. Introduction
2. General Characteristics of CBD in Cancer
3. Efficacy and Mechanism of CBD on Cancer
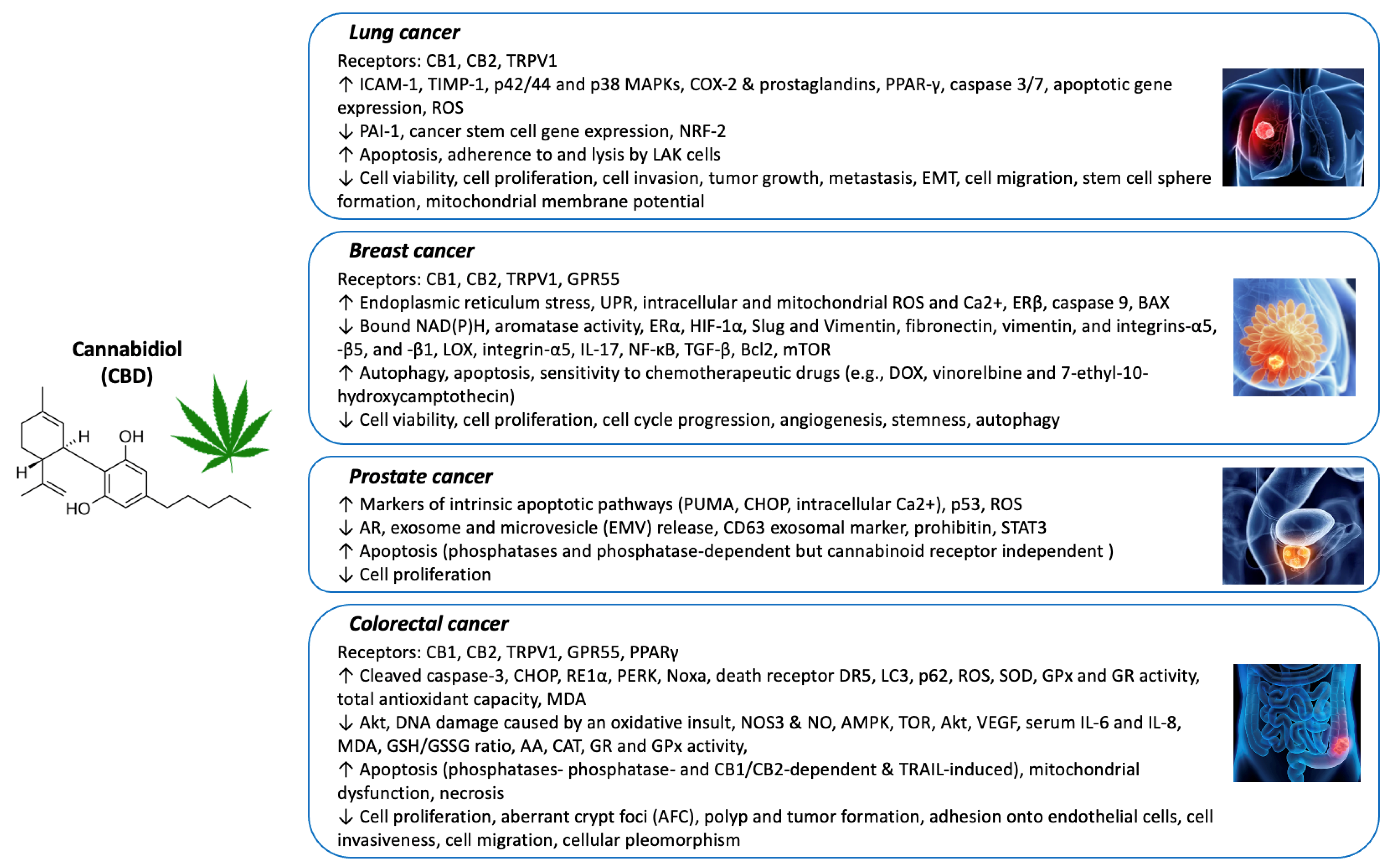
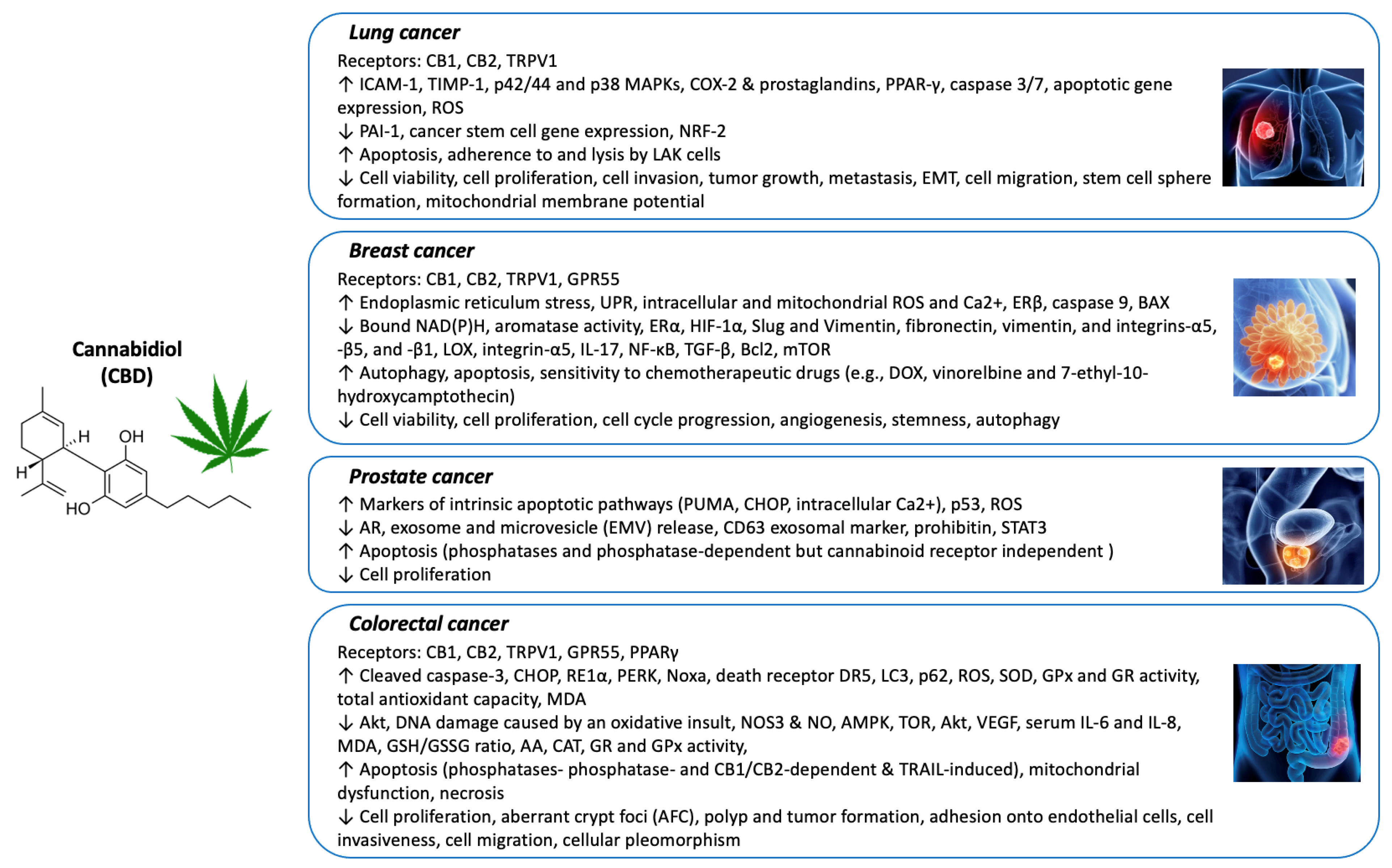
3.1. Lung Cancer
3.2. Breast Cancer
3.3. Prostate Cancer
3.4. Colorectal Cancer (CRC)
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| cannabidiol | (CBD) |
| ∆9-tetrahydrocannabinol | (THC) |
| cannabinoid receptor | (CB) |
| transient receptor potential | (TRP) |
| non-small cell lung cancer | (NSCLC) |
| Small cell lung cancer | (SCLC) |
| mitogen-activated protein kinase | (MAPK) |
| lymphokine-activated killer | (LAK) |
| cyclooxygenase-2 | (COX-2) |
| reactive oxygen species | (ROS) |
| epithelial-to-mesenchymal transition | (EMT) |
| epidermal growth factor | (EGF) |
| epidermal growth factor receptor | (EGFR) |
| vascular endothelial growth factor | (VEGF) |
| unfolded protein response | (UPR) |
| hypoxia-induced factor-1α | (HIF-1α) |
| doxorubicin | (DOX) |
| Src/von Hippel–Lindau tumor suppressor protein | (VHL) |
| extracellular vesicles encapsulated with CBD | (CBD EVs) |
| androgen receptor | (AR) |
| p53-up-regulated modulator of apoptosis | (PUMA) |
| C/EBP homologous protein | (CHOP) |
| exosome and microvesicle | (EMV) |
| colorectal cancer | (CRC) |
| G protein coupled receptor 55 | (GPR55) |
| inositol requiring enzyme-1α | (RE1α) |
| phosphorylated protein kinase RNA-like ER kinase | (PERK) |
| TNF-related apoptosis-inducing ligand | (TRAIL) |
| azoxymethane | (AOM) |
| aberrant crypt foci | (AFC) |
| superoxide dismutase | (SOD) |
| glutathione peroxidase | (GPx) |
| glutathione reductase | (GR) |
| mitochondrial permeability transition pore complex | (MPTP) |
| glutathione | (GSH) |
| oxidized glutathione | (GSSG) |
| ascorbic acid | (AA) |
| catalase | (CAT) |
| malondialdehyde | (MDA) |
| nitric oxide synthase 3 | (NOS3) |
| AMP-activated protein kinase | (AMPK) |
| nitric oxide | (NO) |
| randomized controlled trials | (RCT) |
References
- Zuk-Golaszewska, K.; Golaszewski, J. Cannabis sativa L.—Cultivation and quality of raw material. J. Elem. 2018, 23, 971–984. [Google Scholar] [CrossRef]
- Rehman, M.S.U.; Rashid, N.; Saif, A.; Mahmood, T.; Han, J.-I. Potential of bioenergy production from industrial hemp (Cannabis sativa): Pakistan perspective. Renew. Sustain. Energy Rev. 2013, 18, 154–164. [Google Scholar] [CrossRef]
- Śledziński, P.; Zeyland, J.; Słomski, R.; Nowak, A. The current state and future perspectives of cannabinoids in cancer biology. Cancer Med. 2018, 7, 765–775. [Google Scholar] [CrossRef] [PubMed]
- Grotenhermen, F.; Müller-Vahl, K. Medicinal Uses of Marijuana and Cannabinoids. Crit. Rev. Plant Sci. 2016, 35, 378–405. [Google Scholar] [CrossRef]
- Pertwee, R. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: Δ9-tetrahydrocannabinol, cannabidiol and Δ9-tetrahydrocannabivarin. Br. J. Pharmacol. 2008, 153, 199–215. [Google Scholar] [CrossRef] [Green Version]
- Pertwee, R.G. Pharmacological Actions of Cannabinoids. Cannabinoids 2005, 1–51. [Google Scholar] [CrossRef]
- Kogan, N.M.; Mechoulam, R. Cannabinoids in health and disease. Dialog. Clin. Neurosci. 2007, 9, 413–430. [Google Scholar] [CrossRef]
- Micale, V.; Di Marzo, V.; Sulcova, A.; Wotjak, C.T.; Drago, F. Endocannabinoid system and mood disorders: Priming a target for new therapies. Pharmacol. Ther. 2013, 138, 18–37. [Google Scholar] [CrossRef]
- Muzyka, M.; Tagliafico, L.; Serafini, G.; Baiardini, I.; Braido, F.; Nencioni, A.; Monacelli, F. Neuropsychiatric Disorders and Frailty in Older Adults over the Spectrum of Cancer: A Narrative Review. Cancers 2022, 14, 258. [Google Scholar] [CrossRef]
- Izzo, A.A.; Camilleri, M. Cannabinoids in intestinal inflammation and cancer. Pharmacol. Res. 2009, 60, 117–125. [Google Scholar] [CrossRef]
- Pisanti, S.; Malfitano, A.M.; Ciaglia, E.; Lamberti, A.; Ranieri, R.; Cuomo, G.; Abate, M.; Faggiana, G.; Proto, M.C.; Fiore, D.; et al. Cannabidiol: State of the art and new challenges for therapeutic applications. Pharmacol. Ther. 2017, 175, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Kis, B.; Ifrim, F.C.; Buda, V.; Avram, S.; Pavel, I.Z.; Antal, D.; Paunescu, V.; Dehelean, C.A.; Ardelean, F.; Diaconeasa, Z.; et al. Cannabidiol—From Plant to Human Body: A Promising Bioactive Molecule with Multi-Target Effects in Cancer. Int. J. Mol. Sci. 2019, 20, 5905. [Google Scholar] [CrossRef] [Green Version]
- Siveen, K.S.; Nizamuddin, P.B.; Uddin, S.; Al-Thani, M.; Frenneaux, M.P.; Janahi, I.A.; Steinhoff, M.; Azizi, F. TRPV2: A Cancer Biomarker and Potential Therapeutic Target. Dis. Markers 2020, 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Chen, C.; Chiang, C.; Xiao, T.; Chen, Y.; Zhao, Y.; Zheng, D. The Impact of TRPV1 on Cancer Pathogenesis and Therapy: A Systematic Review. Int. J. Biol. Sci. 2021, 17, 2034–2049. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.R.; Lossignol, D.; Burnell-Nugent, M.; Fallon, M.T. An Open-Label Extension Study to Investigate the Long-Term Safety and Tolerability of THC/CBD Oromucosal Spray and Oromucosal THC Spray in Patients with Terminal Cancer-Related Pain Refractory to Strong Opioid Analgesics. J. Pain Symptom Manag. 2013, 46, 207–218. [Google Scholar] [CrossRef]
- Johnson, J.R.; Burnell-Nugent, M.; Lossignol, D.; Ganae-Motan, E.D.; Potts, R.; Fallon, M.T. Multicenter, double-blind, randomized, placebo-controlled, parallel-group study of the efficacy, safety, and tolerability of THC: CBD extract and THC extract in patients with intractable cancer-related pain. J. Pain Symptom Manag. 2010, 39, 167–179. [Google Scholar] [CrossRef]
- Turgeman, I.; Bar-Sela, G. Cannabis for cancer—Illusion or the tip of an iceberg: A review of the evidence for the use of Cannabis and synthetic cannabinoids in oncology. Expert Opin. Investig. Drugs 2018, 28, 285–296. [Google Scholar] [CrossRef]
- Curran, H.V.; Freeman, T.; Mokrysz, C.; Lewis, D.; Morgan, C.J.A.; Parsons, L.H. Keep off the grass? Cannabis, cognition and addiction. Nat. Rev. Neurosci. 2016, 17, 293–306. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Ligresti, A.; Moriello, A.S.; Starowicz, K.; Matias, I.; Pisanti, S.; De Petrocellis, L.; Laezza, C.; Portella, G.; Bifulco, M.; Di Marzo, V. Antitumor Activity of Plant Cannabinoids with Emphasis on the Effect of Cannabidiol on Human Breast Carcinoma. J. Pharmacol. Exp. Ther. 2006, 318, 1375–1387. [Google Scholar] [CrossRef] [Green Version]
- Massi, P.; Vaccani, A.; Ceruti, S.; Colombo, A.; Abbracchio, M.P.; Parolaro, D. Antitumor effects of cannabidiol, a nonpsychoactive cannabinoid, on human glioma cell lines. J. Pharmacol. Exp. Ther. 2004, 308, 838–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimison, P.; Mersiades, A.; Kirby, A.; Lintzeris, N.; Morton, R.; Haber, P.; Olver, I.; Walsh, A.; McGregor, I.; Cheung, Y. Oral THC: CBD cannabis extract for refractory chemotherapy-induced nausea and vomiting: A randomised, placebo-controlled, phase II crossover trial. Ann. Oncol. 2020, 31, 1553–1560. [Google Scholar] [CrossRef] [PubMed]
- De Petrocellis, L.; Ligresti, A.; Moriello, A.S.; Iappelli, M.; Verde, R.; Stott, C.G.; Cristino, L.; Orlando, P.; di Marzo, V. Non-THC cannabinoids inhibit prostate carcinoma growth in vitro and in vivo: Pro-apoptotic effects and underlying mechanisms. Br. J. Pharmacol. 2013, 168, 79–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Portenoy, R.K.; Ganae-Motan, E.D.; Allende, S.; Yanagihara, R.; Shaiova, L.; Weinstein, S.; McQuade, R.; Wright, S.; Fallon, M.T. Nabiximols for Opioid-Treated Cancer Patients With Poorly-Controlled Chronic Pain: A Randomized, Placebo-Controlled, Graded-Dose Trial. J. Pain 2012, 13, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramer, R.; Bublitz, K.; Freimuth, N.; Merkord, J.; Rohde, H.; Haustein, M.; Borchert, P.; Schmuhl, E.; Linnebacher, M.; Hinz, B. Cannabidiol inhibits lung cancer cell invasion and metastasis via intercellular adhesion molecule-1. FASEB J. 2011, 26, 1535–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramer, R.; Rohde, A.; Merkord, J.; Rohde, H.; Hinz, B. Decrease of Plasminogen Activator Inhibitor-1 May Contribute to the Anti-Invasive Action of Cannabidiol on Human Lung Cancer Cells. Pharm. Res. 2010, 27, 2162–2174. [Google Scholar] [CrossRef]
- Ramer, R.; Merkord, J.; Rohde, H.; Hinz, B. Cannabidiol inhibits cancer cell invasion via upregulation of tissue inhibitor of matrix metalloproteinases-1. Biochem. Pharmacol. 2010, 79, 955–966. [Google Scholar] [CrossRef] [Green Version]
- Ramer, R.; Heinemann, K.; Merkord, J.; Rohde, H.; Salamon, A.; Linnebacher, M.; Hinz, B. COX-2 and PPAR-γ Confer Cannabidiol-Induced Apoptosis of Human Lung Cancer Cells. Mol. Cancer Ther. 2012, 12, 69–82. [Google Scholar] [CrossRef] [Green Version]
- Haustein, M.; Ramer, R.; Linnebacher, M.; Manda, K.; Hinz, B. Cannabinoids increase lung cancer cell lysis by lymphokine-activated killer cells via upregulation of ICAM-1. Biochem. Pharmacol. 2014, 92, 312–325. [Google Scholar] [CrossRef]
- Milian, L.; Mata, M.; Alcacer, J.; Oliver, M.; Sancho-Tello, M.; De Llano, J.J.M.; Camps, C.; Galbis, J.; Carretero, J.; Carda, C. Cannabinoid receptor expression in non-small cell lung cancer. Effectiveness of tetrahydrocannabinol and cannabidiol inhibiting cell proliferation and epithelial-mesenchymal transition in vitro. PLoS ONE 2020, 15, e0228909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamad, H.; Olsen, B.B. Cannabidiol Induces Cell Death in Human Lung Cancer Cells and Cancer Stem Cells. Pharmaceuticals 2021, 14, 1169. [Google Scholar] [CrossRef] [PubMed]
- Misri, S.; Kaul, K.; Mishra, S.; Charan, M.; Verma, A.K.; Barr, M.P.; Ahirwar, D.K.; Ganju, R.K. Cannabidiol Inhibits Tumorigenesis in Cisplatin-Resistant Non-Small Cell Lung Cancer via TRPV2. Cancers 2022, 14, 1181. [Google Scholar] [CrossRef] [PubMed]
- de la Harpe, A.; Beukes, N.; Frost, C.L. CBD activation of TRPV1 induces oxidative signaling and subsequent ER stress in breast cancer cell lines. Biotechnol. Appl. Biochem. 2021, 69, 420–430. [Google Scholar] [CrossRef]
- Mould, R.R.; Botchway, S.W.; Parkinson, J.R.C.; Thomas, E.L.; Guy, G.W.; Bell, J.D.; Nunn, A.V.W. Cannabidiol Modulates Mitochondrial Redox and Dynamics in MCF7 Cancer Cells: A Study Using Fluorescence Lifetime Imaging Microscopy of NAD(P)H. Front. Mol. Biosci. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Amaral, C.; Trouille, F.M.; Almeida, C.; Correia-Da-Silva, G.; Teixeira, N. Unveiling the mechanism of action behind the anti-cancer properties of cannabinoids in ER+ breast cancer cells: Impact on aromatase and steroid receptors. J. Steroid Biochem. Mol. Biol. 2021, 210, 105876. [Google Scholar] [CrossRef] [PubMed]
- Jo, M.J.; Kim, B.G.; Kim, W.Y.; Lee, D.-H.; Yun, H.K.; Jeong, S.; Park, S.H.; Kim, B.R.; Kim, J.L.; Kim, D.Y.; et al. Cannabidiol Suppresses Angiogenesis and Stemness of Breast Cancer Cells by Downregulation of Hypoxia-Inducible Factors-1α. Cancers 2021, 13, 5667. [Google Scholar] [CrossRef]
- Surapaneni, S.K.; Patel, N.; Sun, L.; Kommineni, N.; Kalvala, A.K.; Gebeyehu, A.; Arthur, P.; Duke, L.C.; Nimma, R.; Meckes, D.G. Anticancer and chemosensitization effects of cannabidiol in 2D and 3D cultures of TNBC: Involvement of GADD45α, integrin-α5,-β5,-β1, and autophagy. Drug Deliv. Transl. Res. 2022, 1–16. [Google Scholar] [CrossRef]
- Patel, N.; Kommineni, N.; Surapaneni, S.K.; Kalvala, A.; Yaun, X.; Gebeyehu, A.; Arthur, P.; Duke, L.C.; York, S.B.; Bagde, A.; et al. Cannabidiol loaded extracellular vesicles sensitize triple-negative breast cancer to doxorubicin in both in-vitro and in vivo models. Int. J. Pharm. 2021, 607, 120943. [Google Scholar] [CrossRef]
- Alsherbiny, M.A.; Bhuyan, D.J.; Low, M.N.; Chang, D.; Li, C.G. Synergistic Interactions of Cannabidiol with Chemotherapeutic Drugs in MCF7 Cells: Mode of Interaction and Proteomics Analysis of Mechanisms. Int. J. Mol. Sci. 2021, 22, 10103. [Google Scholar] [CrossRef]
- Sreevalsan, S.; Joseph, S.; Jutooru, I.; Chadalapaka, G.; Safe, S.H. Induction of apoptosis by cannabinoids in prostate and colon cancer cells is phosphatase dependent. Anticancer Res. 2011, 31, 3799–3807. [Google Scholar]
- Kosgodage, U.S.; Mould, R.; Henley, A.B.; Nunn, A.V.; Guy, G.W.; Thomas, E.; Inal, J.; Bell, J.D.; Lange, S. Cannabidiol (CBD) Is a Novel Inhibitor for Exosome and Microvesicle (EMV) Release in Cancer. Front. Pharmacol. 2018, 9, 889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aviello, G.; Romano, B.; Borrelli, F.; Capasso, R.; Gallo, L.; Piscitelli, F.; Di Marzo, V.; Izzo, A.A. Chemopreventive effect of the non-psychotropic phytocannabinoid cannabidiol on experimental colon cancer. Klin. Wochenschr. 2012, 90, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Romano, B.; Borrelli, F.; Pagano, E.; Cascio, M.G.; Pertwee, R.G.; Izzo, A.A. Inhibition of colon carcinogenesis by a standardized Cannabis sativa extract with high content of cannabidiol. Phytomedicine 2013, 21, 631–639. [Google Scholar] [CrossRef]
- Kargl, J.; Andersen, L.; Hasenöhrl, C.; Feuersinger, D.; Stančić, A.; Fauland, A.; Magnes, C.; El-Heliebi, A.; Lax, S.; Uranitsch, S. GPR55 promotes migration and adhesion of colon cancer cells indicating a role in metastasis. Br. J. Pharmacol. 2016, 173, 142–154. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.; Yun, H.K.; Jeong, Y.A.; Jo, M.J.; Kang, S.H.; Kim, J.L.; Kim, D.Y.; Park, S.H.; Kim, B.R.; Na, Y.J.; et al. Cannabidiol-induced apoptosis is mediated by activation of Noxa in human colorectal cancer cells. Cancer Lett. 2019, 447, 12–23. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.L.; Kim, B.R.; Kim, D.Y.; Jeong, Y.A.; Jeong, S.; Na, Y.J.; Park, S.H.; Yun, H.K.; Jo, M.J.; Kim, B.G.; et al. Cannabidiol Enhances the Therapeutic Effects of TRAIL by Upregulating DR5 in Colorectal Cancer. Cancers 2019, 11, 642. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.; Kim, B.G.; Kim, D.Y.; Kim, B.R.; Kim, J.L.; Park, S.H.; Na, Y.J.; Jo, M.J.; Yun, H.K.; Jeong, Y.A.; et al. Cannabidiol Overcomes Oxaliplatin Resistance by Enhancing NOS3- and SOD2-Induced Autophagy in Human Colorectal Cancer Cells. Cancers 2019, 11, 781. [Google Scholar] [CrossRef] [Green Version]
- Honarmand, M.; Namazi, F.; Mohammadi, A.; Nazifi, S. Can cannabidiol inhibit angiogenesis in colon cancer? Comp. Clin. Pathol. 2019, 28, 165–172. [Google Scholar] [CrossRef]
- Cerretani, D.; Collodel, G.; Brizzi, A.; Fiaschi, A.I.; Menchiari, A.; Moretti, E.; Moltoni, L.; Micheli, L. Cytotoxic Effects of Cannabinoids on Human HT-29 Colorectal Adenocarcinoma Cells: Different Mechanisms of THC, CBD, and CB83. Int. J. Mol. Sci. 2020, 21, 5533. [Google Scholar] [CrossRef]
- Kotteas, E.A.; Boulas, P.; Gkiozos, I.; Tsagkouli, S.; Tsoukalas, G.; Syrigos, K.N. The intercellular cell adhesion molecule-1 (icam-1) in lung cancer: Implications for disease progression and prognosis. Anticancer Res. 2014, 34. [Google Scholar]
- Stingl, J.; Caldas, C. Molecular heterogeneity of breast carcinomas and the cancer stem cell hypothesis. Nat. Cancer 2007, 7, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Kärki, T.; Tojkander, S. TRPV Protein Family—From Mechanosensing to Cancer Invasion. Biomolecules 2021, 11, 1019. [Google Scholar] [CrossRef] [PubMed]
- Brentnall, M.; Rodriguez-Menocal, L.; De Guevara, R.L.; Cepero, E.; Boise, L.H. Caspase-9, caspase-3 and caspase-7 have distinct roles during intrinsic apoptosis. BMC Cell Biol. 2013, 14, 32. [Google Scholar] [CrossRef] [Green Version]
- Van Opdenbosch, N.; Lamkanfi, M. Caspases in cell death, inflammation, and disease. Immunity 2019, 50, 1352–1364. [Google Scholar] [CrossRef]
- Carneiro, B.A.; El-Deiry, W.S. Targeting apoptosis in cancer therapy. Nat. Rev. Clin. Oncol. 2020, 17, 395–417. [Google Scholar] [CrossRef]
- Tabernero, J. The Role of VEGF and EGFR Inhibition: Implications for Combining Anti–VEGF and Anti–EGFR Agents. Mol. Cancer Res. 2007, 5, 203–220. [Google Scholar] [CrossRef] [Green Version]
- Xiao, H.; Yang, C.S. Combination regimen with statins and NSAIDs: A promising strategy for cancer chemoprevention. Int. J. Cancer 2008, 123, 983–990. [Google Scholar] [CrossRef]
- DiMarco-Crook, C.; Xiao, H. Diet-Based Strategies for Cancer Chemoprevention: The Role of Combination Regimens Using Dietary Bioactive Components. Annu. Rev. Food Sci. Technol. 2015, 6, 505–526. [Google Scholar] [CrossRef]
- Foulkes, W.D.; Smith, I.E.; Reis-Filho, J.S. Triple-negative breast cancer. New Engl. J. Med. 2010, 363, 1938–1948. [Google Scholar] [CrossRef] [Green Version]
- Almeida, C.F.; Teixeira, N.; Correia-Da-Silva, G.; Amaral, C. Cannabinoids in Breast Cancer: Differential Susceptibility According to Subtype. Molecules 2021, 27, 156. [Google Scholar] [CrossRef] [PubMed]
- Lozano, C.; Córdova, C.; Marchant, I.; Zúñiga, R.; Ochova, P.; Ramírez-Barrantes, R.; González-Arriagada, W.A.; Rodríguez, B.; Olivero, P. Intracellular aggregated TRPV1 is associated with lower survival in breast cancer patients. Breast Cancer Targets Ther. 2018, 10, 161–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renu, K.; Abilash, V.G.; Tirupathi Pichiah, P.B.; Arunachalam, S. Molecular mechanism of doxorubicin-induced cardiomyopathy–An update. Eur. J. Pharmacol. 2018, 818, 241–253. [Google Scholar] [CrossRef]
- Avrutsky, M.I.; Troy, C.M. Caspase-9: A Multimodal Therapeutic Target with Diverse Cellular Expression in Human Disease. Front. Pharmacol. 2021, 12, 701301. [Google Scholar] [CrossRef]
- Formaggio, N.; Rubin, M.A.; Theurillat, J.-P. Loss and revival of androgen receptor signaling in advanced prostate cancer. Oncogene 2021, 40, 1205–1216. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Thomas, H.R.; Li, Z.; Yeo, N.C.; Scott, H.E.; Dang, N.; Hossain, M.I.; Andrabi, S.A.; Parant, J.M. Puma, noxa, p53, and p63 differentially mediate stress pathway induced apoptosis. Cell Death Dis. 2021, 12, 1–11. [Google Scholar] [CrossRef]
- Hu, H.; Tian, M.; Ding, C.; Yu, S. The C/EBP Homologous Protein (CHOP) Transcription Factor Functions in Endoplasmic Reticulum Stress-Induced Apoptosis and Microbial Infection. Front. Immunol. 2019, 9, 3083. [Google Scholar] [CrossRef] [Green Version]
- Bakhshandeh, B.; Kamaleddin, A.; Aalishah, K. A Comprehensive Review on Exosomes and Microvesicles as Epigenetic Factors. Curr. Stem Cell Res. Ther. 2016, 12, 31–36. [Google Scholar] [CrossRef]
- Datta, S.R.; Dudek, H.; Tao, X.; Masters, S.; Fu, H.; Gotoh, Y.; Greenberg, M.E. Akt Phosphorylation of BAD Couples Survival Signals to the Cell-Intrinsic Death Machinery. Cell 1997, 91, 231–241. [Google Scholar] [CrossRef] [Green Version]
- Hayes, J.D.; Dinkova-Kostova, A.T.; Tew, K.D. Oxidative stress in cancer. Cancer Cell 2020, 38, 167–197. [Google Scholar] [CrossRef]
- Nikoletopoulou, V.; Markaki, M.; Palikaras, K.; Tavernarakis, N. Crosstalk between apoptosis, necrosis and autophagy. Biochim. Biophys. Acta (BBA)-Mol. Cell Res. 2013, 1833, 3448–3459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Wang, N.; Liu, P.; Xie, X. AMPK and Cancer. AMP-Act. Protein Kinase 2016, 203–226. [Google Scholar]
- Zou, D.; Li, Z.; Lv, F.; Yang, Y.; Yang, C.; Song, J.; Chen, Y.; Jin, Z.; Zhou, J.; Jiang, Y.; et al. Pan-Cancer Analysis of NOS3 Identifies Its Expression and Clinical Relevance in Gastric Cancer. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef]
- Burstein, S. Cannabidiol (CBD) and its analogs: A review of their effects on inflammation. Bioorganic Med. Chem. 2015, 23, 1377–1385. [Google Scholar] [CrossRef]
- Cohen, K.; Weinstein, A.M. Synthetic and Non-synthetic Cannabinoid Drugs and Their Adverse Effects-A Review from Public Health Prospective. Front. Public Health 2018, 6, 162. [Google Scholar] [CrossRef]
- Trecki, J.; Gerona, R.R.; Schwartz, M.D. Synthetic Cannabinoid–Related Illnesses and Deaths. New Engl. J. Med. 2015, 373, 103–107. [Google Scholar] [CrossRef]

{kind=link}
| Cancer Type | Model | Dosage/ Treatment | Effects | Reference |
|---|---|---|---|---|
| Lung Cancer | Non-small cell lung cancer (NSCLC) A549, H358, and H460 cell lines, and human-derived NSCLC cells | Up to 3 µM CBD | In NSCLC cell lines: ↓ Intercellular adhesion molecule-1 (ICAM-1)-dependent cell invasion; ↑ ICAM-1 and matrix metalloproteinases-1 (TIMP-1) via cannabinoid receptors, transient receptor potential vanilloid 1 (TRPV1), and p42/44 mitogen-activated protein kinase (MAPK) In primary NSCLC cells: ↓ ICAM-1-dependent cell invasion; ↑ ICAM-1 and TIMP-1 expression, CBD showed comparable anti-invasive efficacy to THC (3 µM) | [26] |
| Athymic nude mice xenografted with A549 | 5 mg/kg CBD by intraperitoneal injection | ↓ Tumor size and number of metastatic nodules; ↑ ICAM-1 and TIMP-1 expression | ||
| A549, H460, and H358 | Up to 1 µM CBD | ↓ Cell invasion, plasminogen activator inhibitor-1 (PAI-1) via CB1, CB2, and TRPV1 receptors | [27] | |
| Athymic nude mice xenografted with A549 | 5 mg/kg CBD by intraperitoneal injection | ↓ Tumor size, PAI-1 protein expression | ||
| A549 | 10 µM CBD | ↓ Cell invasion; ↑ TIMP-1, p42/44, and p38 MAPKs via CB1, CB2, and TRPV1 receptors | [28] | |
| A549-xenografted nude mice | 5 mg/kg CBD by intraperitoneal injection | ↓ Number of metastatic nodules | ||
| A549 and H460, and primary cells from a lung cancer patient | 3 µM CBD | ↓ Cell viability; ↑ apoptosis, cyclooxygenase-2 (COX-2) and PPAR-γ, COX-2-dependent prostaglandins, PPAR-γ–dependent apoptotic cell death | [29] | |
| A549-xenografted nude mice | 5 mg/kg CBD by intraperitoneal injection | ↓ Tumor size and CD31 (vascularization marker); ↑ COX-2 and PPAR-γ | ||
| NSCLC A549 and H460 cell lines and human derived metastatic lung cancer cells | 3 µM CBD | ↑ Adherence to and lysis by lymphokine-activated killer (LAK) cells, ICAM-1 expression | [30] | |
| NSCLC cell lines A549, H460, H1792 | Tetrahydrocannabinol (THC) 30 µm, cannabidiol (CBD) 30 µm, and combination THC:CBD 10 µm each | All treatments: ↓ cancer cell proliferation, epithelial-to-mesenchymal transition (EMT), epidermal growth factor (EGF)-induced cell migration THC:CBD combination: ↓ epidermal growth factor receptor (EGFR) gene | [31] | |
| A549 and H1299 NSCLC cell lines and H69 small cell lung cancer (SCLC) cell line | Up to 48 µM CBD; 10 µM CBD for treatment of stem cell spheres | ↓ Cell viability, stem cell sphere formation, expression of cancer stem cell genes (SOX2, POU5F1, CD44, or PROM1), mitochondrial membrane potential; ↑ cell death, caspase 3/7 protein, expression of apoptotic genes (TP53, CDKN1A, BAD, BCL2, BAX, or BAK1), levels of reactive oxygen species (ROS) | [32] | |
| Cisplatin-resistant (CR) NSCLC cell lines H460 and A549 | Up to 90 µM CBD | ↓ Cell viability, nuclear factor erythroid 2-related factor 2 (NRF-2) expression; ↑ apoptosis, ROS, sphere formation and protein expression of Snail, Nanog, and Vimentin | [33] | |
| NSG mice injected with H460-CR cells | 10 mg/kg CBD by intraperitoneal injection | ↓ Tumor progression and metastasis | ||
| Breast Cancer | MCF7 (estrogen receptor-positive) and MDA-MB-231 (triple-negative) | 20 µM CBD | ↓ Cell viability of both MCF7 and MDA-MB- 231; ↑ Endoplasmic reticulum stress, unfolded protein response (UPR) activation, intracellular ROS and Ca2+ accumulation via the activated TRPV1 receptor in the MCF7 | [34] |
| MCF7 | Up to 20 µM CBD | ↓ Bound NAD(P)H; ↑ mitochondrial concentrations of ROS and Ca2+ | [35] | |
| Estrogen receptor-positive (ER+) aromatase-overexpressing MCF-7aro | Up to 20 µM CBD | ↓ Cell viability, aromatase activity, ERα levels, cell cycle progression; ↑ autophagy, apoptosis, ERβ levels | [36] | |
| MCF7, MDA-MB-231, T47D, and SK-BR-3 | Up to 7 µM CBD | ↓ Cell viability, angiogenesis, stemness, hypoxia-induced factor-1α (HIF-1α) expression through Src/von Hippel–Lindau tumor suppressor protein (VHL) signaling, Slug and Vimentin (EMT-related proteins) | [37] | |
| MDA-MB-231 and MDA-MB-468 (triple-negative) | Up to 5 µM CBD in 2D cultures and up to 50 µM in 3D cultures | ↓ Cell viability (CBD had greater IC50 values in 3D than 2D), fibronectin, vimentin, and integrins-α5, -β5, and -β1, autophagy | [38] | |
| MDA-MB-468 | Up to 5 µM CBD in combination with doxorubicin (DOX) | ↑ DOX sensitivity in cancer cells, caspase 9; ↓ LOX and integrin-α5 | ||
| MDA-MB-231 cells and female nude mice injected with MDA-MB-468 cells | CBD-loaded extracellular vesicles (5 mg/kg) | ↑ DOX sensitivity in cancer cells and xenograft tumors, caspase 9, and BAX; ↓ interleukin-17 (IL-17), NF-κB, TGF-β, Bcl2 and mTOR | [39] | |
| MCF7 | 38.42–64.6 µM CBD in combination with DOX, docetaxel, paclitaxel, vinorelbine, and 7-ethyl-10-hydroxycamptothecin | Enhanced effects were observed with the combination of CBD and all chemotherapeutic drugs, while the strongest synergism was found between CBD and vinorelbine and 7-ethyl-10-hydroxycamptothecin; ↑ apoptosis | [40] | |
| Prostate Cancer | Androgen receptor (AR)-positive prostate cancer cell line LNCaP | Up to 15 µM CBD | ↓ Cell proliferation; ↑ phosphatases and phosphatase-dependent apoptosis, but cannabinoid receptor independent | [41] |
| AR-positive (LNCaP and 22RV1) and AR-negative (DU-145 and PC-3) cells | 1–10 µM CBD | ↓ Cell viability and AR (in LNCaP and 22RV1 cells); ↑ apoptosis, markers of intrinsic apoptotic pathways (p53-up-regulated modulator of apoptosis (PUMA), C/EBP homologous protein (CHOP) and intracellular Ca2+) partly due to TRPM8 antagonism, p53 (in LNCaP cells), and ROS | [23] | |
| PC-3 | 1 and 5 µM CBD | ↓ Exosome and microvesicle (EMV) release, CD63 exosomal marker, prohibitin, and STAT3 | [42] | |
| Colorectal Cancer (CRC) | SW480 | Up to 15 µM CBD | ↓ Cell proliferation; ↑ phosphatases and phosphatase-, CB1/CB2-dependent apoptosis | [41] |
| Caco-2 and HCT116 | 10 µM CBD | ↓ Cell proliferation via CB1, TRPV1, and PPARγ receptors, Akt activation, and DNA damage caused by an oxidative insult | [43] | |
| CRC induced by azoxymethane (AOM) in male ICR mice | 1 and 5 mg/kg CBD by intraperitoneal injection | 1 mg/kg: ↓ AOM-induced aberrant crypt foci (AFC), polyp and tumor formation, and Akt activation; ↑ apoptoic protein cleaved caspase-3 5 mg/kg: ↓ AOM-induced polyp formation | ||
| DLD-1 and HCT116 | Up to 5 µM CBD | ↓ Cell proliferation via CB1 receptor | [44] | |
| HCT116 | 1 and 2.5 µM CBD | ↓ Adhesion of HCT116 cells onto endothelial cells, invasiveness, migration via G protein-coupled receptor 55 (GPR55) | [45] | |
| HCT116 and DLD-1 | 6 µM CBD | ↓ Cell viability; ↑ apoptosis by regulating pro- and anti-apoptotic proteins (CHOP, inositol requiring enzyme-1α (RE1α), phosphorylated protein kinase RNA-like ER kinase (PERK), etc.), in a Noxa-and-ROS-dependent manner | [46] | |
| BALB/c nude mice injected with HCT116 Luc+ cells (a luminescent cell line derived from HCT116) | 10 and 20 mg/kg CBD by intraperitoneal injection | 20 mg/kg ↓ tumor size; ↑ apoptosis and Noxa expression | ||
| HCT116, HT29, and DLD-1 | 4 µM CBD | ↓ Cell viability; ↑ apoptosis by regulating pro- and anti-apoptotic proteins (CHOP, PERK, death receptor DR5 expression by ER stress, etc.), TNF-related apoptosis-inducing ligand (TRAIL)-induced apoptosis | [47] | |
| Oxaliplatin-resistant DLD-1 and colo205 | 4 µM CBD | ↓ Cell proliferation, nitric oxide synthase 3 (NOS3), nitric oxide (NO), AMP-activated protein kinase (AMPK), TOR, and Akt; ↑ autophagic markers LC3 and p62, ROS via superoxide dismutase 2 (SOD2) causing mitochondrial dysfunction | [48] | |
| BALB/c mice injected with CT26 (mouse CRC cells) | 1 and 5 mg/kg CBD by intraperitoneal injection | ↓ Tumor size, cellular pleomorphism, vascular endothelial growth factor (VEGF), serum levels of IL-6 and IL-8 (5 mg/kg), and malondialdehyde (MDA); ↑ apoptosis, SOD (5 mg/kg), glutathione peroxidase (GPx) and glutathione reductase (GR) activity, and total antioxidant capacity | [49] | |
| HT-29 | 30 µM CBD | ↓ Cell viability, glutathione (GSH)-to-oxidized-glutathione (GSSG) ratio, ascorbic acid (AA), catalase (CAT), and GR and GPx activity; ↑ MDA and necrosis | [50] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heider, C.G.; Itenberg, S.A.; Rao, J.; Ma, H.; Wu, X. Mechanisms of Cannabidiol (CBD) in Cancer Treatment: A Review. Biology 2022, 11, 817. https://doi.org/10.3390/biology11060817
Heider CG, Itenberg SA, Rao J, Ma H, Wu X. Mechanisms of Cannabidiol (CBD) in Cancer Treatment: A Review. Biology. 2022; 11(6):817. https://doi.org/10.3390/biology11060817
Chicago/Turabian StyleHeider, Camren G., Sasha A. Itenberg, Jiajia Rao, Hang Ma, and Xian Wu. 2022. "Mechanisms of Cannabidiol (CBD) in Cancer Treatment: A Review" Biology 11, no. 6: 817. https://doi.org/10.3390/biology11060817
APA StyleHeider, C. G., Itenberg, S. A., Rao, J., Ma, H., & Wu, X. (2022). Mechanisms of Cannabidiol (CBD) in Cancer Treatment: A Review. Biology, 11(6), 817. https://doi.org/10.3390/biology11060817