
Effectiveness of Adapted Taekwondo, Multi-Component Training and Walking Exercise on Health Status in Independent Older Women: Study Protocol for a Randomized Controlled Trial (TKD & Aging Project)


 ,
, 
 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
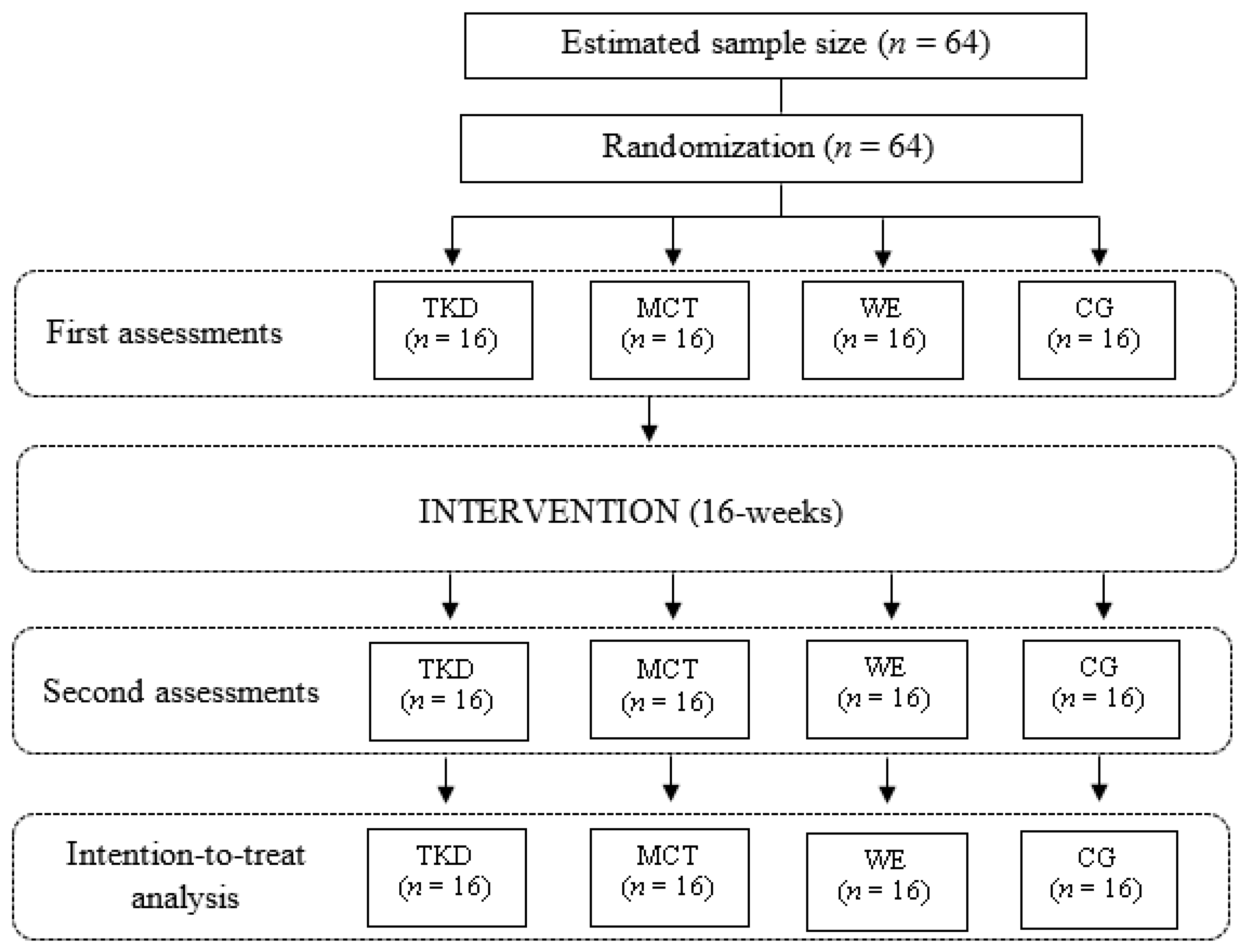
2.1. Study Design
2.2. Ethical Approval
2.3. Sample Size Calculation
2.4. Randomization and Blinding
2.5. Participants
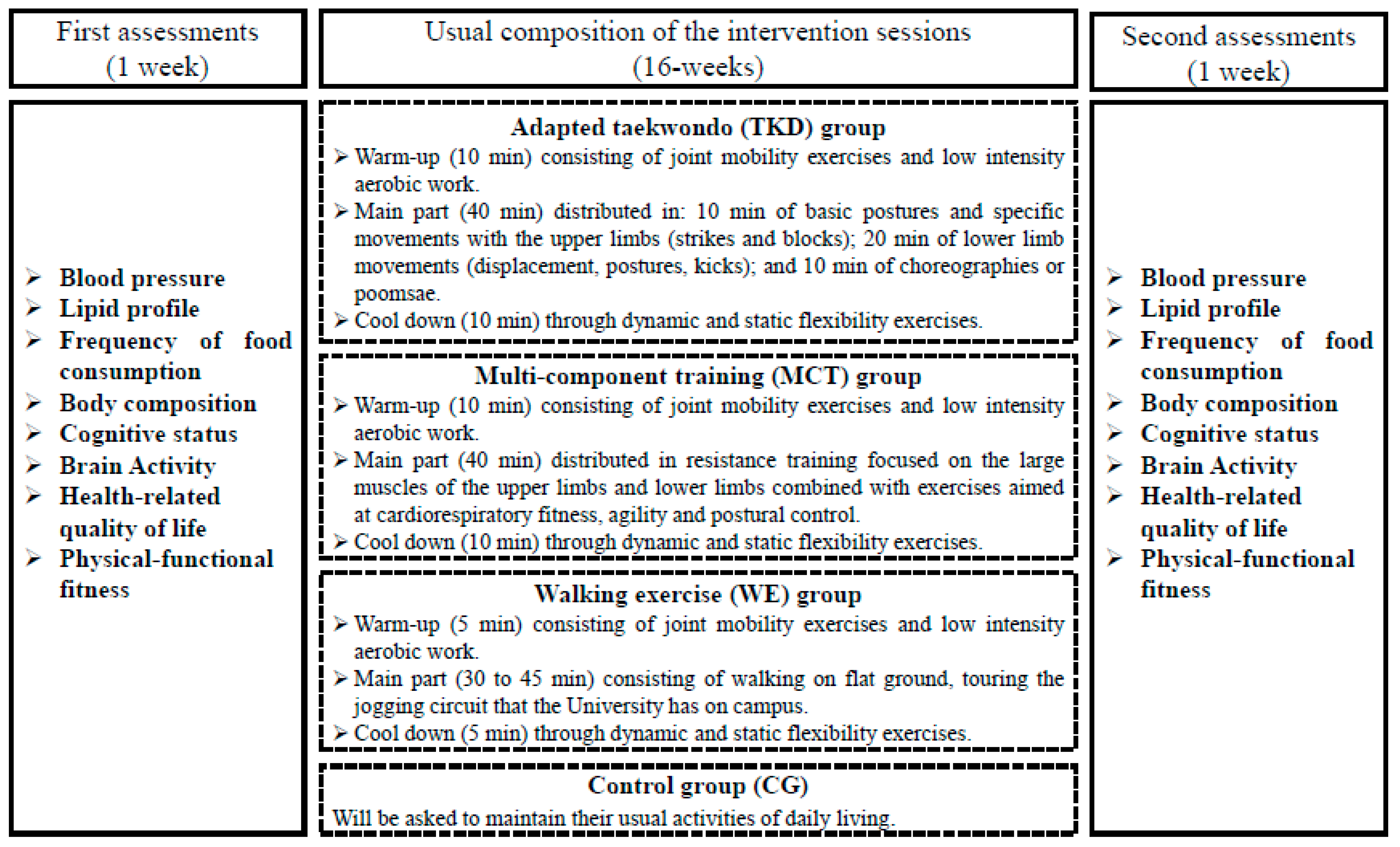
2.6. Intervention
2.6.1. Adapted Taekwondo (TKD) Program
2.6.2. Multi-Component Training (MCT) Program
2.6.3. Walking Exercise (WE) Program
2.6.4. Control Group (CG)
2.7. Outcomes and Procedures
2.7.1. Primary Outcomes
2.7.2. Secondary Outcomes
2.8. Statistical Analysis
2.8.1. Intention-to-Treat Analysis
2.8.2. Analysis by Protocol
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Claudino, J.G.; Afonso, J.; Sarvestan, J.; Lanza, M.B.; Pennone, J.; Filho, C.A.C.; Serrão, J.C.; Espregueira-Mendes, J.; Vasconcelos, A.L.V.; de Andrade, M.P. Strength training to prevent falls in older adults: A systematic review with meta-analysis of randomized controlled trials. J. Clin. Med. 2021, 10, 3184. [Google Scholar] [CrossRef]
- Neville, C.; Nguyen, H.; Ross, K.; Wingood, M.; Peterson, E.W.; Dewitt, J.E.; Moore, J.; King, M.J.; Atanelov, L.; White, J. Lower-limb factors associated with balance and falls in older adults: A systematic review and clinical synthesis. J. Am. Podiatr. Med. Assoc. 2020, 110, 1–42. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Gutiérrez-García, C.; Pérez-Gutiérrez, M.; Vargas-Vitoria, R.; López-Fuenzalida, A. Effects of physical activity governmental programs on health status in independent older adults: A systematic review. J. Aging Phys. Act. 2019, 27, 265–275. [Google Scholar] [CrossRef]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Alves, D.J.F.; Bartholomeu-Neto, J.; Júnior, E.R.; Zarricueta, B.S.R.; Nóbrega, O.T.; Córdova, C. Walking speed, risk factors, and cardiovascular events in older adults—Systematic review. J. Strength Cond. Res. 2017, 31, 3235–3244. [Google Scholar] [CrossRef]
- Sadjapong, U.; Yodkeeree, S.; Sungkarat, S.; Siviroj, P. Multicomponent exercise program reduces frailty and inflammatory biomarkers and improves physical performance in community-dwelling older adults: A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 3760. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Herrera-Valenzuela, T.; Ramirez-Campillo, R.; Aedo-Muñoz, E.; Martín, B.-S.; Ojeda-Aravena, A.; Branco, B.H.M. Effects of Olympic combat sports on older adults’ health status: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 7381. [Google Scholar] [CrossRef]
- Cho, S.-Y.; Roh, H.-T. Taekwondo enhances cognitive function as a result of increased neurotrophic growth factors in elderly women. Int. J. Environ. Res. Public Health 2019, 16, 962. [Google Scholar] [CrossRef]
- Hu, J.-P.; Guo, Y.-H.; Wang, F.; Zhao, X.-P.; Zhang, Q.-H.; Song, Q.-H. Exercise improves cognitive function in aging patients. Int. J. Clin. Exp. Med. 2014, 7, 3144. [Google Scholar]
- Izquierdo, M. Multicomponent physical exercise program: Vivifrail. Nutr. Hosp. 2019, 36, 50–56. [Google Scholar]
- Gupta, S.D.; Bobbert, M.F.; Kistemaker, D.A. The metabolic cost of walking in healthy young and older adults—A systematic review and meta analysis. Sci. Rep. 2019, 9, 9956. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Herrera-Valenzuela, T.; Guzmán-Muñoz, E.; Delgado-Floody, P.; Núñez-Espinosa, C.; Monsalves-Álvarez, M.; Andrade, D. Effects of Olympic combat sports on health-related quality of life in middle-aged and older people: A systematic review. Front. Psychol. 2021, 12, 797537. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Ramirez-Campillo, R.; Herrera-Valenzuela, T.; Branco, B.H.M.; Guzmán-Muñoz, E.; Mendez-Rebolledo, G.; Concha-Cisternas, Y.; Hernandez-Martínez, J. Effectiveness of Olympic combat sports on balance, fall risk or falls in older adults: A systematic review. Biology 2022, 11, 74. [Google Scholar] [CrossRef]
- Lee, S.H.; Scott, S.D.; Pekas, E.J.; Lee, S.; Lee, S.H.; Park, S.Y. Taekwondo training reduces blood catecholamine levels and arterial stiffness in postmenopausal women with stage-2 hypertension: Randomized clinical trial. Clin. Exp. Hypertens. 2019, 41, 675–681. [Google Scholar] [CrossRef]
- Baek, S.-H.; Hong, G.-R.; Min, D.-K.; Kim, E.-H.; Park, S.-K. Effects of functional fitness enhancement through taekwondo training on physical characteristics and risk factors of dementia in elderly women with depression. Int. J. Environ. Res. Public Health 2021, 18, 7961. [Google Scholar] [CrossRef]
- Cromwell, R.L.; Meyers, P.M.; Meyers, P.E.; Newton, R.A. Taekwondo: An effective exercise for improving balance and walking ability in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2007, 62, 641–646. [Google Scholar] [CrossRef]
- Ministerio del Deporte. Encuesta Nacional de Hábitos de Actividad Física y Deporte 2018 en Población de 18 Años y más; Ministerio del Deporte: Santiago, Chile, 2019.
- Ministerio de Salud. Encuesta Nacional de Salud 2016–2017: Primeros Resultados; Departamento de Epidemiología: Santiago, Chile, 2017.
- Valdés-Badilla, P.; Godoy-Cumillaf, A.; Ortega-Spuler, J.; Herrera-Valenzuela, T.; Durán-Agüero, S.; Zapata-Bastias, J.; Vargas-Vitoria, R.; Guzmán-Muñoz, E.; López-Fuenzalida, A. Asociación entre índices antropométricos de salud y condición física en mujeres mayores físicamente activas. Salud Pública de México 2017, 59, 682–690. [Google Scholar] [CrossRef][Green Version]
- Turner, L.; Shamseer, L.; Altman, D.G.; Weeks, L.; Peters, J.; Kober, T.; Dias, S.; Schulz, K.F.; Plint, A.C.; Moher, D. Consolidated standards of reporting trials (CONSORT) and the completeness of reporting of randomised controlled trials (RCTs) published in medical journals. Cochrane Database Syst. Rev. 2012, 11, MR000030. [Google Scholar] [CrossRef]
- Valdés-Badilla, P.; Guzmán-Muñoz, E.; Ramírez-Campillo, R.; Godoy-Cumillaf, A.; Concha-Cisternas, Y.; Ortega-Spuler, J.; Herrera-Valenzuela, T.; Durán-Agüero, S.; Vargas-Vitoria, R.; Magnani-Branco, B. Changes in anthropometric parameters and physical fitness in older adults after participating in a 16-weeks physical activity program. Rev. de la Fac. de Med. de la Univ. Nac. de Colomb. 2020, 68, 375–382. [Google Scholar] [CrossRef]
- Researcher Randomizer. Available online: https://www.randomizer.org/ (accessed on 13 May 2022).
- Ministerio de Salud. Manual de Aplicación del Examen de Medicina Preventiva del Adulto Mayor; Ministerio de Salud: Santiago, Chile, 2013.
- Aguilar, D.M.; Valdés-Badilla, P.; Herrera-Valenzuela, T.; Guzmán-Muñoz, E.; Magnani Branco, B.; Méndez-Rebolledo, G.; López-Fuenzalida, A. ¿ Bandas elásticas o equipos de gimnasio para el entrenamiento de adultos mayores? Retos Nuevas Tend. en Educ. Fís. Deporte y Recrea. 2020, 37, 370–378. [Google Scholar]
- Colado, J.C.; Pedrosa, F.M.; Juesas, A.; Gargallo, P.; Carrasco, J.J.; Flandez, J.; Chupel, M.U.; Teixeira, A.M.; Naclerio, F. Concurrent validation of the OMNI-resistance exercise scale of perceived exertion with elastic bands in the elderly. Exp. Gerontol. 2018, 103, 11–16. [Google Scholar] [CrossRef]
- Valdés Badilla, P.; Godoy Cumillaf, A.; Ortega Spuler, J.; Díaz Aravena, D.; Castro Garrido, N.; Sandoval Muñoz, L.; Herrera Valenzuela, T.; López Fuenzalida, A.; Vargas Vitoria, R.; Durán Agüero, S. Relación entre índices antropométricos de salud con el consumo de alimentos en adultos mayores físicamente activos. Nutr. Hosp. 2017, 34, 1073–1079. [Google Scholar] [CrossRef]
- Marfell-Jones, M.J.; Stewart, A.; de Ridder, J. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Wellington, New Zealand, 2012. [Google Scholar]
- Derio, C.D.; Bonnet, S.G.; Ponce, M.T.; Yanez, A.A.; Chonchol, A.S.; Pellegrino, M.B. Memoria, fluidez y orientación: Prueba de cribado de deterioro cognitivo en 5 minutos. Neurología 2013, 28, 400–407. [Google Scholar] [CrossRef]
- Basso, D.; Saracini, C. Differential involvement of left and right frontoparietal areas in visuospatial planning: An rTMS study. Neuropsychologia 2020, 136, 107260. [Google Scholar] [CrossRef]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A. El cuestionario de salud SF-36 español: Una década de experiencia y nuevos desarrollos. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef]
- Rikli, R.; Jones, J. Senior Fitness Test Manual; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Mancilla, E.; Ramos, S.; Morales, P. Fuerza de prensión manual según edad, género y condición funcional en adultos mayores Chilenos entre 60 y 91 años. Rev. Méd. de Chile 2016, 144, 598–603. [Google Scholar] [CrossRef]
- Duarte, M.; Freitas, S. Revision of posturography based on force plate for balance evaluation. Braz. J. Phys. Ther. 2010, 14, 183–192. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Kinnunen, J.-V.; Piitulainen, H.; Piirainen, J.M. Neuromuscular adaptations to short-term high-intensity interval training in female ice-hockey players. J. Strength Cond. Res. 2019, 33, 479–485. [Google Scholar] [CrossRef]
- Bouchard, C.; Blair, S.N.; Church, T.S.; Earnest, C.P.; Hagberg, J.M.; Häkkinen, K.; Jenkins, N.T.; Karavirta, L.; Kraus, W.E.; Leon, A.S. Adverse metabolic response to regular exercise: Is it a rare or common occurrence? PLoS ONE 2012, 7, e37887. [Google Scholar] [CrossRef]
- Bromley, S.J.; Drew, M.K.; Talpey, S.; McIntosh, A.S.; Finch, C.F. A systematic review of prospective epidemiological research into injury and illness in Olympic combat sport. Br. J. Sports Med. 2018, 52, 8–16. [Google Scholar] [CrossRef]
- Youm, C.-H.; Lee, J.-S.; Seo, K.-E. Effects of Taekwondo and walking exercises on the double-leg balance control of elderly females. Korean J. Sport Biomech. 2011, 21, 123–129. [Google Scholar] [CrossRef]
- Chen, J. The Effects of Taekwondo-Based Exercise vs. Standard Balance Exercises on Fall Risk in Older Adults. Doctoral dissertation, Azusa Pacific University, Azusa, CA, USA, 2018.
- Ouergui, I.; Messaoudi, H.; Chtourou, H.; Wagner, M.O.; Bouassida, A.; Bouhlel, E.; Franchini, E.; Engel, F.A. Repeated sprint training vs. repeated high-intensity technique training in adolescent taekwondo athletes—A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 4506. [Google Scholar] [CrossRef]
- Ojeda-Aravena, A.; Herrera-Valenzuela, T.; Valdés-Badilla, P.; Cancino-López, J.; Zapata-Bastias, J.; García-García, J.M. Inter-Individual variability of a high-intensity interval training with specific techniques vs. repeated sprints program in sport-related fitness of taekwondo athletes. Front. Physiol. 2021, 12, 766153. [Google Scholar] [CrossRef]
- Ojeda-Aravena, A.; Herrera-Valenzuela, T.; Valdés-Badilla, P.; Cancino-López, J.; Zapata-Bastias, J.; García-García, J.M. Effects of 4 weeks of a technique-specific protocol with high-intensity intervals on general and specific physical fitness in taekwondo athletes: An inter-individual analysis. Int. J. Environ. Res. Public Health 2021, 18, 3643. [Google Scholar] [CrossRef]
- Aravena-Tapia, D.; Roman-Barrera, V.; Da Silva Santos, J.; Franchini, E.; Valdés-Badilla, P.; Orihuela, P.; Herrera-Valenzuela, T. High-intensity interval training improves specific performance in taekwondo athletes. Rev. de Artes Marciales Asiáticas 2020, 15, 4–13. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Program | Month | Weeks | Frequency (Weekly) | Total Time Per Session (min) | Exercise | Set | Rep | Rest | Intensity |
|---|---|---|---|---|---|---|---|---|---|
| TKD | 1 | 1–4 | 3 | 60 | UL | 3 | 8 | 2 min | 50–70% HRmax |
| LL | |||||||||
| Poomsae | --- | 6 | |||||||
| 2 | 5–8 | UL | 4 | 8 | |||||
| LL | |||||||||
| Poomsae | --- | 6 | |||||||
| 3 | 9–12 | UL | 4 | 12 | |||||
| LL | |||||||||
| Poomsae | --- | 6 | |||||||
| 4 | 13–16 | UL | 4 | 12 | 90 s | ||||
| LL | |||||||||
| Poomsae | --- | 6 | |||||||
| MCT | 1 | 1–4 | 60 | RT | 3 | 10 | 2 min | OMNI-RES (5–8 points) | |
| CF | 50–70% HRmax | ||||||||
| APC | |||||||||
| 2 | 5–8 | RT | 4 | 10 | OMNI-RES (5–8 points) | ||||
| CF | 50–70% HRmax | ||||||||
| APC | |||||||||
| 3 | 9–12 | RT | 4 | 12 | OMNI-RES (5–8 points) | ||||
| CF | 50–70% HRmax | ||||||||
| APC | |||||||||
| 4 | 13–16 | RT | 90 s | OMNI-RES (5–8 points) | |||||
| CF | 50–70% HRmax | ||||||||
| APC | |||||||||
| WE | 1 | 1–4 | 45 | --- | --- | --- | --- | 50–70% HRmax | |
| 2 | 5–8 | 50 | --- | --- | --- | ---- | |||
| 3 | 9–12 | 55 | --- | --- | --- | ---- | |||
| 4 | 13–16 | 60 | --- | --- | --- | ---- | |||
| Control group | 1–4 | 16 | Will be asked to maintain their usual activities of daily living. | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdés-Badilla, P.; Herrera-Valenzuela, T.; Guzmán-Muñoz, E.; Branco, B.H.M.; Zapata-Bastias, J.; Lucero, B.; Castillo-Retamal, F. Effectiveness of Adapted Taekwondo, Multi-Component Training and Walking Exercise on Health Status in Independent Older Women: Study Protocol for a Randomized Controlled Trial (TKD & Aging Project). Biology 2022, 11, 816. https://doi.org/10.3390/biology11060816
Valdés-Badilla P, Herrera-Valenzuela T, Guzmán-Muñoz E, Branco BHM, Zapata-Bastias J, Lucero B, Castillo-Retamal F. Effectiveness of Adapted Taekwondo, Multi-Component Training and Walking Exercise on Health Status in Independent Older Women: Study Protocol for a Randomized Controlled Trial (TKD & Aging Project). Biology. 2022; 11(6):816. https://doi.org/10.3390/biology11060816
Chicago/Turabian StyleValdés-Badilla, Pablo, Tomás Herrera-Valenzuela, Eduardo Guzmán-Muñoz, Braulio Henrique Magnani Branco, José Zapata-Bastias, Boris Lucero, and Franklin Castillo-Retamal. 2022. "Effectiveness of Adapted Taekwondo, Multi-Component Training and Walking Exercise on Health Status in Independent Older Women: Study Protocol for a Randomized Controlled Trial (TKD & Aging Project)" Biology 11, no. 6: 816. https://doi.org/10.3390/biology11060816
APA StyleValdés-Badilla, P., Herrera-Valenzuela, T., Guzmán-Muñoz, E., Branco, B. H. M., Zapata-Bastias, J., Lucero, B., & Castillo-Retamal, F. (2022). Effectiveness of Adapted Taekwondo, Multi-Component Training and Walking Exercise on Health Status in Independent Older Women: Study Protocol for a Randomized Controlled Trial (TKD & Aging Project). Biology, 11(6), 816. https://doi.org/10.3390/biology11060816