
Nomogram Development and Feature Selection Strategy Comparison for Predicting Surgical Site Infection After Lower Extremity Fracture Surgery


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Data Collection and Review
2.4. Outcome Definition
2.5. Predictor Variables
2.6. Sample Size Considerations
2.7. Missing Data
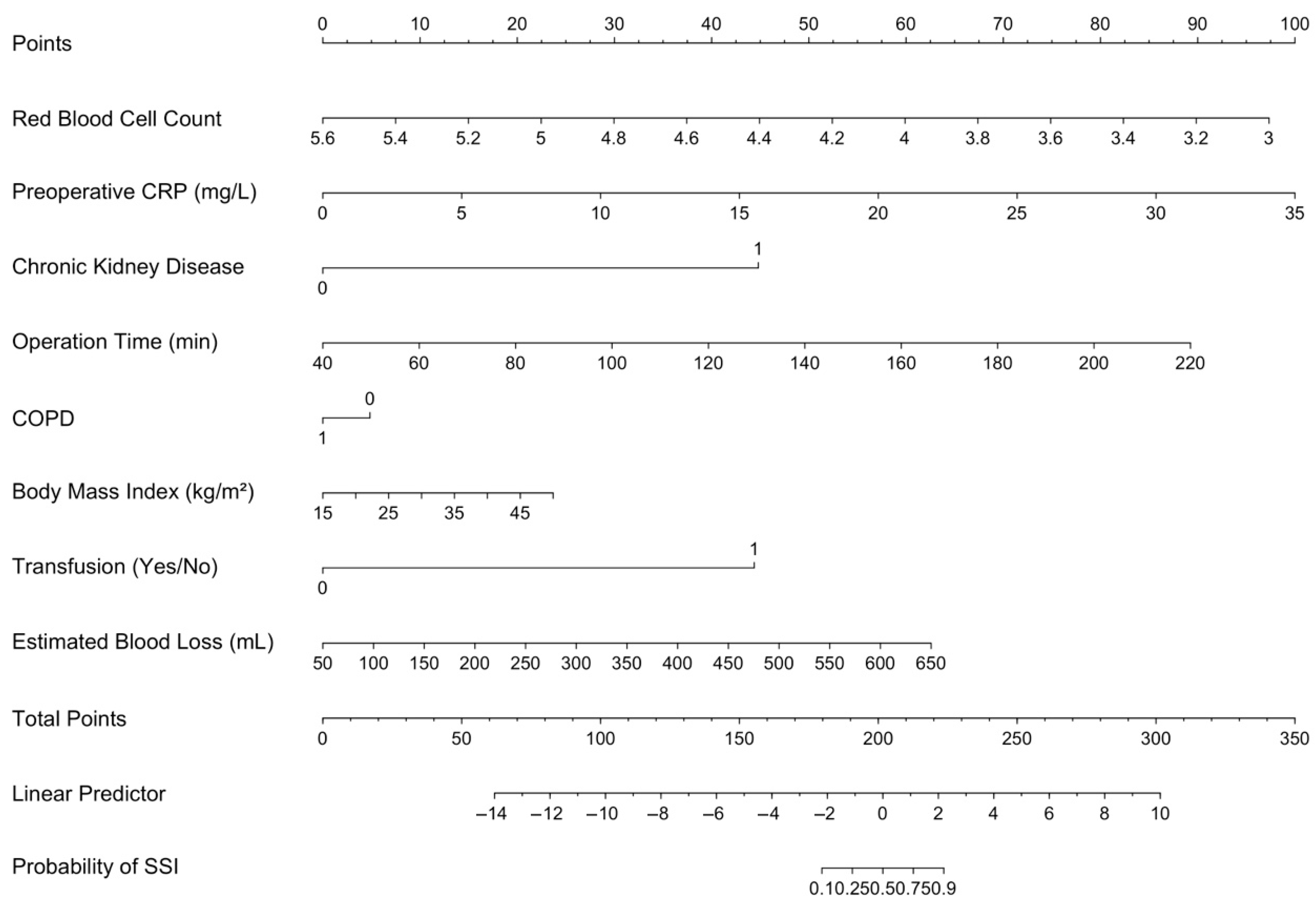
2.8. Nomogram Construction in Clinical Risk Prediction
2.9. Feature Selection Strategies in Prediction Model Development
2.10. Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SSI | Surgical Site Infection |
| AUROC | Area Under the Receiver Operating Characteristic Curve |
| CRP | C-Reactive Protein |
| BMI | Body Mass Index |
| ASA | American Society of Anesthesiologists |
| LASSO | Least Absolute Shrinkage and Selection Operator |
| RFE | Recursive Feature Elimination |
| AIC | Akaike Information Criterion |
| BIC | Bayesian Information Criterion |
| CDC | Centers for Disease Control and Prevention |
| LOWESS | Locally Weighted Scatterplot Smoothing |
| MAR | Missing at Random |
| MCAR | Missing Completely at Random |
| FMI | Fraction of Missing Information |
| EPP | Events-Per-Predictor |
| OR | Odds Ratio |
| CI | Confidence Interval |
References
- Zhang, J.; Bradshaw, F.; Hussain, I.; Karamatzanis, I.; Duchniewicz, M.; Krkovic, M. The Epidemiology of Lower Limb Fractures: A Major United Kingdom (UK) Trauma Centre Study. Cureus 2024, 16, e56581. [Google Scholar] [CrossRef] [PubMed]
- Beerekamp, M.S.H.; Keizer, R.J.O.d.M.; Schep, N.W.L.; Ubbink, D.T.; Panneman, M.J.M.; Goslings, J.C. Epidemiology of Extremity Fractures in the Netherlands. Injury 2017, 48, 1355–1362. [Google Scholar] [CrossRef]
- Wu, A.-M.; Bisignano, C.; James, S.L.; Abady, G.G.; Abedi, A.; Abu-Gharbieh, E.; Alhassan, R.K.; Alipour, V.; Arabloo, J.; Asaad, M.; et al. Global, Regional, and National Burden of Bone Fractures in 204 Countries and Territories, 1990–2019: A Systematic Analysis from the Global Burden of Disease Study 2019. Lancet Healthy Longev. 2021, 2, e580–e592. [Google Scholar] [CrossRef] [PubMed]
- Pigeolet, M.; Sana, H.; Askew, M.R.; Jaswal, S.; Ortega, P.F.; Bradley, S.R.; Shah, A.; Mita, C.; Corlew, D.S.; Saeed, A.; et al. Outcomes of External versus Internal Fixation for Traumatic Lower Limb Fractures in Low- and Middle-Income Countries: A Systematic Review and Meta-Analysis Protocol. Bone Jt. Open 2024, 5, 1020–1026. [Google Scholar] [CrossRef]
- Chokotho, L.; Wu, H.-H.; Shearer, D.; Lau, B.C.; Mkandawire, N.; Gjertsen, J.-E.; Hallan, G.; Young, S. Outcome at 1 Year in Patients with Femoral Shaft Fractures Treated with Intramedullary Nailing or Skeletal Traction in a Low-Income Country: A Prospective Observational Study of 187 Patients in Malawi. Acta Orthop. 2020, 91, 724–731. [Google Scholar] [CrossRef]
- Parker, B.; Petrou, S.; Masters, J.P.M.; Achana, F.; Costa, M.L. Economic Outcomes Associated with Deep Surgical Site Infection in Patients with an Open Fracture of the Lower Limb. Bone Jt. J. 2018, 100-B, 1506–1510. [Google Scholar] [CrossRef]
- Liu, H.; Wang, Y.; Xing, H.; Chang, Z.; Pan, J. Risk factors for deep surgical site infections following orthopedic trauma surgery: A meta-analysis and systematic review. J. Orthop. Surg. Res. 2024, 19, 811. [Google Scholar] [CrossRef]
- Bai, Y.; Zhang, X.; Tian, Y.; Tian, D.; Zhang, B. Incidence of Surgical-Site Infection Following Open Reduction and Internal Fixation of a Distal Femur Fracture: An Observational Case–Control Study. Medicine 2019, 98, e14547. [Google Scholar] [CrossRef]
- Willey, M.; Karam, M. Impact of Infection on Fracture Fixation. Orthop. Clin. N. Am. 2016, 47, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xie, X.; Zhang, J.; Shen, P.; Zhang, Y.; Chen, C.; Si, Y.; Zou, J. Novel Bedside Dynamic Nomograms to Predict the Probability of Postoperative Cognitive Dysfunction in Elderly Patients Undergoing Noncardiac Surgery: A Retrospective Study. CIA 2022, 17, 1331–1342. [Google Scholar] [CrossRef]
- Huang, X.; Guo, Y.; Fu, R.; Li, H. A Nomogram to Predict Postoperative Surgical Site Infection of Adult Patients Who Received Orthopaedic Surgery: A Retrospective Study. Sci. Rep. 2023, 13, 8129. [Google Scholar] [CrossRef]
- Campbell, M.P.; Mott, M.D.; Owen, J.R.; Reznicek, J.E.; Beck, C.A.; Muthukrishnan, G.; Golladay, G.J.; Kates, S.L. Low Albumin Level Is More Strongly Associated with Adverse Outcomes and Staphylococcus Aureus Infection than Hemoglobin A1C or Smoking Tobacco. J. Orthop. Res. 2022, 40, 2670–2677. [Google Scholar] [CrossRef]
- An, Y.; Cui, X.; Wang, H.; Sun, Y.; Zhu, B.; Feng, S.; Jiang, J. Nomogram for Predicting Surgical Site Infections in Elderly Patients after Open Lumbar Spine Surgery: A Retrospective Study. Int. Wound J. 2024, 21, e14734. [Google Scholar] [CrossRef]
- McNeish, D.M. Using Lasso for Predictor Selection and to Assuage Overfitting: A Method Long Overlooked in Behavioral Sciences. Multivar. Behav. Res. 2015, 50, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Moons, K.G.M.; Dhiman, P.; Riley, R.D.; Beam, A.L.; Van Calster, B.; Ghassemi, M.; Liu, X.; Reitsma, J.B.; van Smeden, M.; et al. TRIPOD+AI Statement: Updated Guidance for Reporting Clinical Prediction Models That Use Regression or Machine Learning Methods. BMJ 2024, 385, e078378. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; National Healthcare Safety Network (NHSN). Patient Safety Component Manual: Chapter 9—Surgical Site Infection (SSI) Event; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2024. [Google Scholar]
- Vonzun, L.; Rüegg, L.; Zepf, J.; Moehrlen, U.; Meuli, M.; Ochsenbein-Kölble, N. Are Cervical Length and Fibronectin Predictors of Preterm Birth after Fetal Spina Bifida Repair? A Single Center Cohort Study. J. Clin. Med. 2023, 12, 123. [Google Scholar] [CrossRef]
- Ma, R.; He, J.; Xu, B.; Zhao, C.; Zhang, Y.; Li, X.; Sun, S.; Zhang, Q. Nomogram Prediction of Surgical Site Infection of HIV-Infected Patients Following Orthopedic Surgery: A Retrospective Study. BMC Infect. Dis. 2020, 20, 896. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, W.; Zhang, Y.; Zhang, S.; Jin, G.; Li, X. Establishment and Validation of a Nomogram Model for Postoperative Surgical Site Infection after Transforaminal Lumbar Interbody Fusion: A Retrospective Observational Study. Surgery 2023, 174, 1220–1226. [Google Scholar] [CrossRef]
- Chen, L.; Liu, C.; Ye, Z.; Huang, S.; Liang, T.; Li, H.; Chen, J.; Chen, W.; Guo, H.; Chen, T.; et al. Predicting Surgical Site Infection Risk after Spinal Tuberculosis Surgery: Development and Validation of a Nomogram. Surg. Infect. 2022, 23, 564–575. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, W.; Hu, Q.; Liu, L.; Xie, Z.; Xu, Y.; Jing, G.; Wang, Y. A Nomogram for Accurately Predicting the Surgical Site Infection Following Transforaminal Lumbar Interbody Fusion in Type 2 Diabetes Patients, Based on Glycemic Variability. Int. Wound J. 2023, 20, 981–994. [Google Scholar] [CrossRef]
- Cheng, Y.; Chen, Y.; Hou, X.; Yu, J.; Wen, H.; Dai, J.; Zheng, Y. Development of a Nomogram for Predicting Surgical Site Infection in Patients with Resected Lung Neoplasm Undergoing Minimally Invasive Surgery. Surg. Infect. 2022, 23, 754–762. [Google Scholar] [CrossRef]
- Luo, J.-Z.; Lin, J.-Z.; Chen, Q.-F.; Yang, C.-J.; Zhou, C.-S. Construction and Validation of a Nomogram Predictive Model for Assessing the Risk of Surgical Site Infections Following Posterior Lumbar Fusion Surgery. Sci. Rep. 2025, 15, 1023. [Google Scholar] [CrossRef] [PubMed]
- Staartjes, V.E.; Kernbach, J.M.; Stumpo, V.; van Niftrik, C.H.B.; Serra, C.; Regli, L. Foundations of Feature Selection in Clinical Prediction Modeling. In Machine Learning in Clinical Neuroscience; Staartjes, V.E., Regli, L., Serra, C., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 51–57. [Google Scholar]
- Xv, Y.; Lv, F.; Guo, H.; Liu, Z.; Luo, D.; Liu, J.; Gou, X.; He, W.; Xiao, M.; Zheng, Y. A CT-Based Radiomics Nomogram Integrated With Clinic-Radiological Features for Preoperatively Predicting WHO/ISUP Grade of Clear Cell Renal Cell Carcinoma. Front. Oncol. 2021, 11, 712554. [Google Scholar] [CrossRef] [PubMed]
- Hamada, M.; Tanimu, J.J.; Hassan, M.; Kakudi, H.A.; Robert, P. Evaluation of Recursive Feature Elimination and LASSO Regularization-Based Optimized Feature Selection Approaches for Cervical Cancer Prediction. In Proceedings of the 2021 IEEE 14th International Symposium on Embedded Multicore/Many-core Systems-on-Chip (MCSoC), Singapore, 20–23 December 2021; pp. 333–339. [Google Scholar]
- Lenert, M.C.; Walsh, C.G. Balancing Performance and Interpretability: Selecting Features with Bootstrapped Ridge Regression. AMIA Annu. Symp. Proc. 2018, 2018, 1377–1386. [Google Scholar]
- Passos, S.C.; Castro, S.M.d.J.; Stahlschmidt, A.; Neto, P.C.d.S.; Pereira, P.J.I.; Leal, P.d.C.; Lopes, M.B.; Falcão, L.F.d.R.; de Azevedo, V.L.F.; Lineburger, E.B.; et al. Development and Validation of the Ex-Care BR Model: A Multicentre Initiative for Identifying Brazilian Surgical Patients at Risk of 30-Day in-Hospital Mortality. Br. J. Anaesth. 2024, 133, 125–134. [Google Scholar] [CrossRef]
- Bugarin, A.; Shah, A.A.; Devana, S.; Lee, C.; SooHoo, N.F. Development of a Machine Learning Algorithm for Prediction of Complications after Ankle Arthrodesis. Foot Ankle Orthop. 2022, 7, 2473011421S00122. [Google Scholar] [CrossRef]
- Tsvetkov, N.; Mallaev, M.; Gahl, B.; Hojski, A.; Tamm, M.; Steiner, L.A.; Lardinois, D. Validation of the American College of Surgeons Surgical Risk Calculator for Thoracic Surgery. J. Thorac. Dis. 2024, 16, 5698. [Google Scholar] [CrossRef]
- Shah, A.A.; Devana, S.; Lee, C.; Bugarin, A.; Upfill-Brown, A.; Lord, E.L.; Park, D.Y.; SooHoo, N. P30. Development of a Machine Learning Algorithm for Prediction of Complications and Readmission after Lumbar Spinal Fusion. Spine J. 2021, 21, S154–S155. [Google Scholar] [CrossRef]
- Murray, I.; Lim, K.; Howells, R.; Jones, R.; Sharma, A.; Jones, S. The Utility of a Personalised Risk Calculator in Gynae-Oncology Surgery. Clin. Oncol. Res. 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- Davis, F.M.; Sutzko, D.C.; Grey, S.F.; Mansour, M.A.; Jain, K.M.; Nypaver, T.J.; Gaborek, G.; Henke, P.K. Predictors of Surgical Site Infection after Open Lower Extremity Revascularization. J. Vasc. Surg. 2017, 65, 1769–1778.e3. [Google Scholar] [CrossRef]
- Gutierrez-Naranjo, J.M.; Moreira, A.; Valero-Moreno, E.; Bullock, T.S.; Ogden, L.A.; Zelle, B.A. A Machine Learning Model to Predict Surgical Site Infection after Surgery of Lower Extremity Fractures. Int. Orthop. (SICOT) 2024, 48, 1887–1896. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Shibahashi, K.; Aoki, M.; Kudo, D.; Kushimoto, S. Risk Factors for Surgical Site Infection Following Orthopaedic Surgery for Fracture by Trauma: A Nested Case–Control Study. J. Hosp. Infect. 2024, 145, 52–58. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variable | SSI− (n = 562) | SSI+ (n = 76) | p | Mean Difference (95% CI) |
|---|---|---|---|---|
| Age (years) | 48.1 ± 18.7 | 52.8 ± 18.7 | 0.045 | 4.64 (0.12 to 9.17) |
| Sex (Male) | 348 (61.9%) | 54 (71.1%) | 0.155 | |
| BMI (kg/m2) | 26.9 ± 9.5 | 30.1 ± 10.6 | 0.015 | 3.18 (0.64 to 5.71) |
| Diabetes mellitus | 65 (11.6%) | 19 (25.0%) | 0.002 | |
| Hypertension | 183 (32.6%) | 34 (44.7%) | 0.048 | |
| Malignancy | 16 (2.8%) | 6 (7.9%) | 0.054 | |
| Smoking | 117 (20.8%) | 15 (19.7%) | 0.946 | |
| CKD | 20 (3.6%) | 5 (6.6%) | 0.338 | |
| COPD | 53 (9.4%) | 10 (13.2%) | 0.414 | |
| ASA Score = 3–4 | 18 (3.2%) | 5 (6.6%) | 0.174 | |
| Emergency surgery | 172 (30.6%) | 30 (39.5%) | 0.153 | |
| Open fracture present | 78 (13.9%) | 26 (34.2%) | <0.001 | |
| Tourniquet use | 386 (68.7%) | 33 (43.4%) | <0.001 | |
| Time to surgery (hours) | 17.4 ± 7.3 | 22.3 ± 9.2 | <0.001 | 4.87 (2.69 to 7.05) |
| OR time (minutes) | 111.7 ± 26.8 | 126.0 ± 27.0 | <0.001 | 14.29 (7.73 to 20.84) |
| Minimally invasive technique | 133 (23.7%) | 7 (9.2%) | 0.007 | |
| Fixation: external fixator | 135 (24.0%) | 32 (42.1%) | 0.005 | |
| Flap coverage performed | 3 (0.5%) | 18 (23.7%) | <0.001 | |
| Bone grafting performed | 0 (0.0%) | 10 (13.2%) | <0.001 | |
| Drain inserted | 223 (39.7%) | 43 (56.6%) | 0.007 | |
| Reoperation | 2 (0.4%) | 9 (11.8%) | <0.001 | |
| Blood transfusion | 18 (3.2%) | 20 (26.3%) | <0.001 | |
| Estimated blood loss (mL) | 235.0 ± 112.6 | 302.2 ± 126.9 | <0.001 | 67.15 (36.75 to 97.56) |
| Length of hospital stay (days) | 4.4 ± 2.1 | 8.9 ± 4.8 | <0.001 | 4.53 (3.42 to 5.64) |
| Variable | SSI− (n = 562) | SSI+ (n = 76) | p | Mean Difference (95% CI) |
|---|---|---|---|---|
| Hemoglobin (g/dL) | 130.7 ± 14.1 | 129.7 ± 14.6 | 0.571 | |
| RBC count (×106/μL) | 4.4 ± 0.4 | 4.3 ± 0.4 | 0.009 | –0.14 (–0.24 to –0.04) |
| WBC count (×109/L) | 10.0 ± 1.7 | 10.5 ± 1.7 | 0.011 | 0.55 (0.13 to 0.98) |
| Neutrophil count (×109/L) | 6.2 ± 1.2 | 6.9 ± 1.2 | <0.001 | 0.74 (0.44 to 1.03) |
| Lymphocyte count (×109/L) | 1.5 ± 0.3 | 1.3 ± 0.3 | <0.001 | –0.24 (–0.31 to –0.17) |
| Platelet count (×103/μL) | 239.0 ± 44.5 | 240.7 ± 50.2 | 0.780 | |
| Prothrombin time (s) | 11.0 ± 0.6 | 11.0 ± 0.6 | 0.476 | |
| APTT (s) | 25.9 ± 1.8 | 26.1 ± 2.0 | 0.473 | |
| Albumin (g/dL) | 40.6 ± 1.8 | 39.8 ± 1.5 | <0.001 | –0.79 (–1.17 to –0.41) |
| Glucose (mg/dL) | 125.6 ± 23.2 | 151.6 ± 28.7 | <0.001 | 26.03 (19.22 to 32.85) |
| D-Dimer (mg/L) | 6.9 ± 4.2 | 15.1 ± 9.1 | <0.001 | 8.13 (6.03 to 10.22) |
| Preoperative CRP (mg/L) | 10.1 ± 6.0 | 17.7 ± 6.5 | <0.001 | 7.62 (6.06 to 9.19) |
| Postoperative CRP (mg/L) | 74.5 ± 32.1 | 115.1 ± 33.7 | <0.001 | 40.68 (32.55 to 48.81) |
| Feature Selection Method | Variables Selected by FS (n) | Variables in Final Model (n) | AUROC (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | Hosmer–Lemeshow p | Nagelkerke R2 |
|---|---|---|---|---|---|---|---|
| Bootstrap + LRM | 9 | 7 | 0.924 (0.876–0.973) | 0.862 (0.694–0.945) | 0.895 (0.838–0.933) | 0.367 | 0.708 |
| LASSO + Firth | 21 | 1 | 0.755 (0.657–0.852) | 0.724 (0.543–0.853) | 0.691 (0.616–0.757) | 0.0002 | 0.310 |
| Univariate + Firth (Shrinked) | 27 | 27 | 0.997 (0.989–1.000) | Not reportable | Not reportable | 0.118 | 1.00 (pre-shrink) |
| Stepwise + LRM | 18 | 12 | 0.882 (0.814–0.950) | 0.414 (0.255–0.593) | 0.963 (0.922–0.983) | <0.001 | 0.664 |
| Boruta + Ridge + LRM | 16 | 9 | 0.997 (0.992–1.000) | 0.931 (0.780–0.981) | 0.988 (0.956–0.997) | 1.000 | 0.934 |
| RFE + LRM | 13 | 13 | 0.954 (0.905–1.000) | 0.897 (0.736–0.964) | 0.975 (0.938–0.990) | Not available | 1.000 |
| Model | ΔAUROC | Brier Score | Calibration Slope | AIC | BIC |
|---|---|---|---|---|---|
| Bootstrap + LRM | 0.0571 | 0.0602 | 3.2659 | 114.62 | 151.54 |
| LASSO + Firth | 0.1810 | 0.0117 | 12.6590 | 239.42 | 310.97 |
| Univariate + Firth (Shrinked) | 0.0030 | 0.0207 | 0.5343 | 199.59 | 327.87 |
| Stepwise + LRM | 0.0887 | 0.0772 | 5.7881 | 128.21 | 165.13 |
| Boruta + Ridge + LRM | 0.0019 | 0.0191 | 8.1792 | 53.49 | 106.82 |
| RFE + LRM | 0.0460 | 0.0366 | 5.8358 | 28.00 | 85.44 |
| Variable | OR (95% CI) | p |
|---|---|---|
| RBC (×106/μL) | 0.13 (0.05–0.32) | <0.0001 |
| Preoperative CRP (mg/L) | 13.13 (5.18–33.30) | <0.0001 |
| Chronic Kidney Disease | 88.75 (5.51–1428.80) | 0.0016 |
| Operation Time (minutes) | 5.41 (2.66–10.98) | <0.0001 |
| COPD * | 0.62 (0.11–3.41) | 0.500 |
| Body Mass Index (kg/m2) | 3.06 (1.08–8.70) | 0.036 |
| Transfusion (Yes/No) | 85.07 (11.69–619.09) | <0.0001 |
| Estimated Blood Loss (mL) | 5.37 (2.45–11.77) | <0.0001 |
| Body Mass Index (kg/m2) | 3.06 (1.08–8.70) | 0.036 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baki, H.; Parmaksızoğlu, A.S. Nomogram Development and Feature Selection Strategy Comparison for Predicting Surgical Site Infection After Lower Extremity Fracture Surgery. Medicina 2025, 61, 1378. https://doi.org/10.3390/medicina61081378
Baki H, Parmaksızoğlu AS. Nomogram Development and Feature Selection Strategy Comparison for Predicting Surgical Site Infection After Lower Extremity Fracture Surgery. Medicina. 2025; 61(8):1378. https://doi.org/10.3390/medicina61081378
Chicago/Turabian StyleBaki, Humam, and Atilla Sancar Parmaksızoğlu. 2025. "Nomogram Development and Feature Selection Strategy Comparison for Predicting Surgical Site Infection After Lower Extremity Fracture Surgery" Medicina 61, no. 8: 1378. https://doi.org/10.3390/medicina61081378
APA StyleBaki, H., & Parmaksızoğlu, A. S. (2025). Nomogram Development and Feature Selection Strategy Comparison for Predicting Surgical Site Infection After Lower Extremity Fracture Surgery. Medicina, 61(8), 1378. https://doi.org/10.3390/medicina61081378