
Are Suggested Hiking Times Accurate? A Validation of Hiking Time Estimations for Preventive Measures in Mountains

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
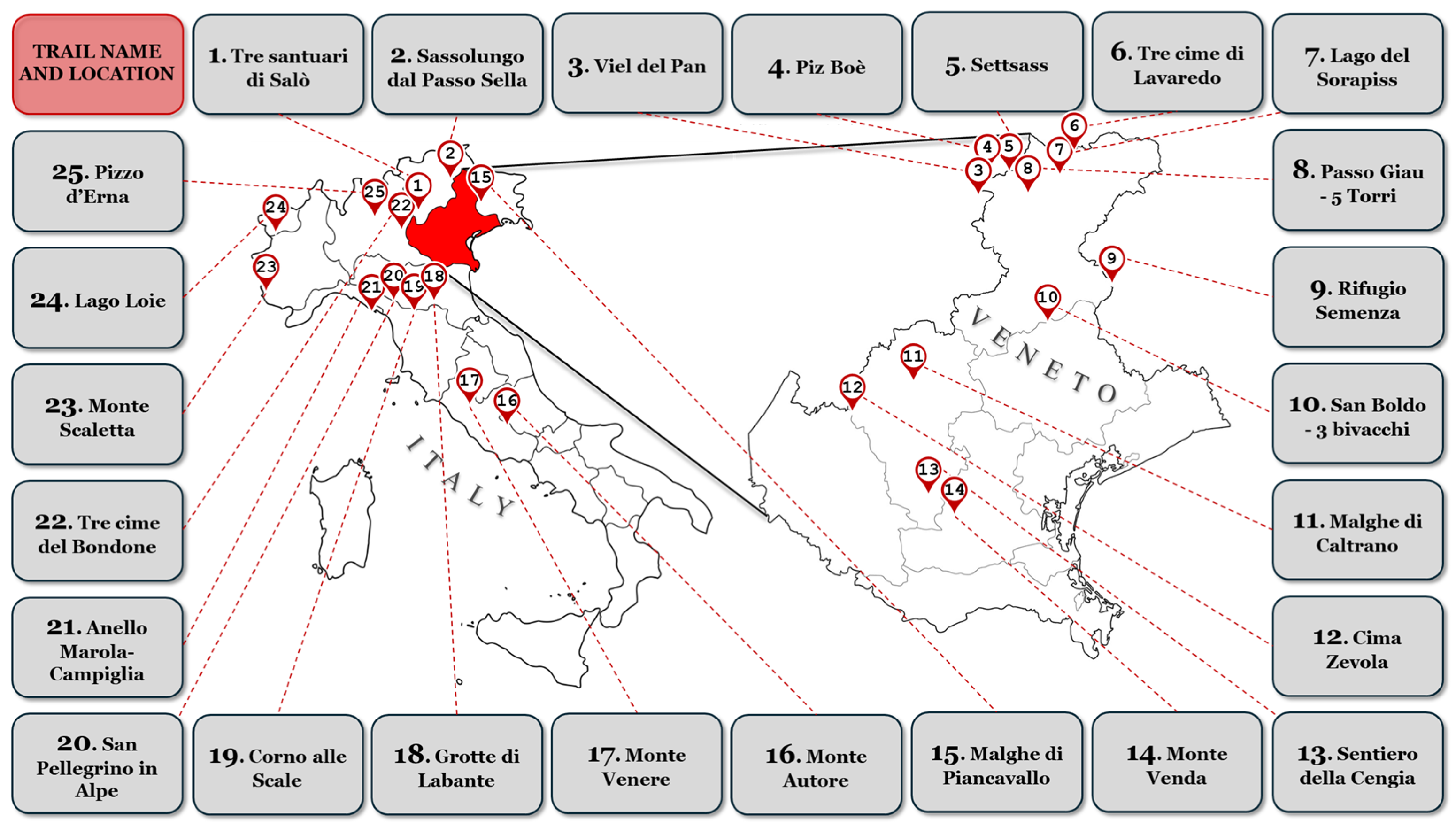
2.1. Trail Selection and Eligibility Criteria
- -
- Only the hiking activity was considered.
- -
- The tolerated variability in performing the respective hiking trail was ±1 km.
- -
- Trails with at least 20 uploaded users were selected.
- -
- Only circular trails with the same direction of travel were selected.
2.2. Hiking Time Estimation Methods
- -
- Komoot. Komoot is a web platform with different functionalities related to outdoor activities (route planner, navigation app, tour directory, and social network). It offers a generic time estimation in which the only customizable variable is the training level of the user. Not knowing the physical activity level of the selected users, intermediate training level (default setting) was considered for all users [29].
- -
- Outdooractive. Outdooractive is another well-known web platform with different functionalities for outdoor physical activities (route planner, navigation app, and tour directory). The “Route planner” function allows an estimation of the hiking time for a specific uploaded track. No details about the individual user are required [30].
- -
- Mountain signage. The hiking times of the different routes as provided by the mountain physical signposts of the Italian Alpine Club (CAI) have been identified through official online sources. The CAI suggests for an average trained hiker a positive elevation gain of 350 m and a negative elevation gain of 500 m in one hour of hiking. For flat sections, the pace considered is 3.5–4 km/h. Moreover, if the trail is at altitudes above 2800–3000 m, a positive elevation gain of 250 m and a negative elevation gain of 400 m in one hour of hiking are predicted. For estimated hiking times longer than four hours, adjustments are made to the next half-hour or hour [15].
- -
- MOVE. MOVE is a scientifically developed digital algorithm, with an Italian national patent (deposit number: 102021000026513; approval 24.01.2024). It aims to estimate the expected hiking time needed to complete a hiking route, based on certain biological parameters of the user and physical characteristics of the trail, including altitude. More specifically, MOVE calculates maximal oxygen consumption (VO2 max) using the Whaley et al. equation, which considers factors such as sex, age, physical activity level, and body mass index (BMI). For the purposes of this study, a BMI of 22 kg/m2 was utilized as the standard for all subjects, thereby assuming a normal weight classification [31]. Additionally, cardiovascular risk is assessed using the ESC SCORE 2 chart, incorporating cholesterol levels, blood pressure, and smoking habits. Walking oxygen consumption is scaled progressively based on cardiovascular risk, ranging from 40% of VO2 max for very high-risk individuals to 69% of VO2 max for low-risk individuals [32]. For the prediction of the walking speed, the system employs the walking equation, which accounts for both uphill (positive grade) and downhill (negative grade) conditions [33].
2.3. Statistical Analyses
3. Results
4. Discussion
4.1. Incorrect Hiking Time Estimation as Potential Risk Factor
4.2. Why Different Hiking Time Estimates?
4.3. How This Tool Can Impact Prevention in the Mountain Environment
4.4. Limitations and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Romeo, R.; Russo, L.; UNWTO. Mountain Tourism—Towards a More Sustainable Path; FAO: Rome, Italy; The World Tourism Organization (UNWTO): Madrid, Spain, 2021; ISBN 978-92-5-135416-2. Available online: https://openknowledge.fao.org/server/api/core/bitstreams/f7257ef4-0b45-4c2b-b47f-80502c9e53f1/content (accessed on 10 November 2024).
- Van Veelen, M.J.; Voegele, A.; Rauch, S.; Kaufmann, M.; Brugger, H.; Strapazzon, G. COVID-19 Pandemic in Mountainous Areas: Impact, Mitigation Strategies, and New Technologies in Search and Rescue Operations. High Alt. Med. Biol. 2021, 22, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Mitten, D.; Overholt, J.R.; Haynes, F.I.; D’Amore, C.C.; Ady, J.C. Hiking: A Low-Cost, Accessible Intervention to Promote Health Benefits. Am. J. Lifestyle Med. 2018, 12, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Struthers, N.A.; Guluzade, N.A.; Zecevic, A.A.; Walton, D.M.; Gunz, A. Nature-Based Interventions for Physical Health Conditions: A Systematic Review and Meta-Analysis. Environ. Res. 2024, 258, 119421. [Google Scholar] [CrossRef] [PubMed]
- Neunhäuserer, D.; Sturm, J.; Baumgartlinger, M.M.; Niederseer, D.; Ledl-Kurkowski, E.; Steidle, E.; Plöderl, M.; Fartacek, C.; Kralovec, K.; Fartacek, R.; et al. Hiking in Suicidal Patients: Neutral Effects on Markers of Suicidality. Am. J. Med. 2013, 126, 927–930. [Google Scholar] [CrossRef] [PubMed]
- Sturm, J.; Plöderl, M.; Fartacek, C.; Kralovec, K.; Neunhäuserer, D.; Niederseer, D.; Hitzl, W.; Niebauer, J.; Schiepek, G.; Fartacek, R. Physical Exercise through Mountain Hiking in High-Risk Suicide Patients. A Randomized Crossover Trial. Acta Psychiatr. Scand. 2012, 126, 467–475. [Google Scholar] [CrossRef]
- Neumayr, G.; Fries, D.; Mittermayer, M.; Humpeler, E.; Klingler, A.; Schobersberger, W.; Spiesberger, R.; Pokan, R.; Schmid, P.; Berent, R. Effects of Hiking at Moderate and Low Altitude on Cardiovascular Parameters in Male Patients With Metabolic Syndrome: Austrian Moderate Altitude Study. Wilderness Environ. Med. 2014, 25, 329–334. [Google Scholar] [CrossRef]
- Schobersberger, W.; Schmid, P.; Lechleitner, M.; von Duvillard, S.P.; Hörtnagl, H.; Gunga, H.-C.; Klingler, A.; Fries, D.; Kirsch, K.; Spiesberger, R.; et al. Austrian Moderate Altitude Study 2000 (AMAS 2000). The Effects of Moderate Altitude (1,700 m) on Cardiovascular and Metabolic Variables in Patients with Metabolic Syndrome. Eur. J. Appl. Physiol. 2003, 88, 506–514. [Google Scholar] [CrossRef]
- Gatterer, H.; Raab, C.; Pramsohler, S.; Faulhaber, M.; Burtscher, M.; Netzer, N. Effect of Weekly Hiking on Cardiovascular Risk Factors in the Elderly. Z. Gerontol. Geriatr. 2015, 48, 150–153. [Google Scholar] [CrossRef]
- Jenkins, D.W.; Jenks, A. Hiking with Diabetes. J. Am. Podiatr. Med. Assoc. 2017, 107, 382–392. [Google Scholar] [CrossRef]
- Cornwell, W.K.; Baggish, A.L.; Bhatta, Y.K.D.; Brosnan, M.J.; Dehnert, C.; Sawalla Guseh, J.; Hammer, D.; Levine, B.D.; Parati, G.; Wolfel, E.E. Clinical Implications for Exercise at Altitude among Individuals with Cardiovascular Disease: A Scientific Statement from the American Heart Association. J. Am. Heart Assoc. 2021, 10, e023225. [Google Scholar] [CrossRef]
- Schobersberger, W.; Leichtfried, V.; Mueck-Weymann, M.; Humpeler, E. Austrian Moderate Altitude Studies (AMAS): Benefits of Exposure to Moderate Altitudes (1500–2500 M). Sleep Breath. 2010, 14, 201–207. [Google Scholar] [CrossRef]
- Milani, M.; Roveri, G.; Falla, M.; Dal Cappello, T.; Strapazzon, G. Occupational Accidents Among Search and Rescue Providers During Mountain Rescue Operations and Training Events. Ann. Emerg. Med. 2023, 81, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Direzione Nazionale Del CNSAS. Report Attività Di Soccorso 2023. Available online: https://news.cnsas.it/wp-content/uploads/2024/04/Report-attivita-di-soccorso-2023-Corpo-Nazionale-Soccorso-Alpino-e-Speleologico.pdf (accessed on 10 November 2024).
- Club Alpino Italiano. Sentieri Pianificazione Segnaletica e Manutenzione. Quaderno Di Escursionismo n.1. 4th Ed (2010). Available online: https://www.cai.it/wp-content/uploads/2024/04/8-1-Quaderno_1_2010.pdf (accessed on 10 November 2024).
- Club Alpino Svizzero. Scala CAS Delle Difficoltà Escursionistiche—Definizioni (2023). Available online: https://www.sac-cas.ch/fileadmin/Ausbildung_und_Wissen/Tourenplanung/Alpinmerkbl%C3%A4tter/20230811_Scala_escursionistica.pdf (accessed on 10 November 2024).
- Alpine Association of Slovenia. Available online: https://en.pzs.si/vsebina.php?pid=161 (accessed on 27 December 2024).
- Bergsport & Gesundheit Alpenverein. Available online: https://www.alpenverein.at/portal/berg-aktiv/bergsport-gesundheit/index.php (accessed on 27 December 2024).
- Test Di Autovalutazione | In Montagna a Passo Sicuro | UPI. Available online: https://www.trekking-sicuro.ch/it/autovalutazione (accessed on 27 December 2024).
- Gatterer, H.; Niedermeier, M.; Pocecco, E.; Frühauf, A.; Faulhaber, M.; Menz, V.; Burtscher, J.; Posch, M.; Ruedl, G.; Burtscher, M. Mortality in Different Mountain Sports Activities Primarily Practiced in the Summer Season—A Narrative Review. Int. J. Environ. Res. Public Health 2019, 16, 3920. [Google Scholar] [CrossRef] [PubMed]
- Luks, A.M.; Hackett, P.H. Medical Conditions and High-Altitude Travel. N. Engl. J. Med. 2022, 386, 364–373. [Google Scholar] [CrossRef]
- Parati, G.; Agostoni, P.; Basnyat, B.; Bilo, G.; Brugger, H.; Coca, A.; Festi, L.; Giardini, G.; Lironcurti, A.; Luks, A.M.; et al. Clinical Recommendations for High Altitude Exposure of Individuals with Pre-Existing Cardiovascular Conditions. Eur. Heart J. 2018, 39, 1546–1554. [Google Scholar] [CrossRef]
- Burtscher, M.; Niederseer, D. Sudden Cardiac Death during Mountain Sports Activities. Dtsch. Z. Sportmed. 2020, 71, 286–292. [Google Scholar] [CrossRef]
- Faulhaber, M.; Gatterer, H.; Burtscher, M. Preexisting Cardiovascular Diseases Among High-Altitude Mountaineers in the Alps: Table 1. J. Travel Med. 2011, 18, 355–357. [Google Scholar] [CrossRef]
- Burtscher, M. Exercise Capacity for Mountaineering: How Much Is Necessary? Res. Sport. Med. 2004, 12, 241–250. [Google Scholar] [CrossRef]
- Mieda, R.; Matsui, Y.; Tobe, M.; Kanamoto, M.; Suto, T.; Saito, S. Education Program for Prevention of Outdoor Accidents in Middle-High Aged Trekkers: Monitoring of Change in Blood Pressure and Heart Rate during Exercise. Prev. Med. Rep. 2021, 23, 101396. [Google Scholar] [CrossRef]
- Wikiloc | Trails of the World. Available online: https://www.wikiloc.com/ (accessed on 27 December 2024).
- Research Integrity Code of the University of Padua. 2019. Available online: https://www.unipd.it/en/sites/en.unipd.it/files/CodiceIntegrita%CC%80Ricerca_ENG.pdf (accessed on 27 December 2024).
- Komoot | Find, Plan and Share Your Adventures. Available online: https://www.komoot.com/ (accessed on 27 December 2024).
- Outdooractive Route Planner—Plan Your Next Adventure. Available online: https://www.outdooractive.com/en/routeplanner/ (accessed on 27 December 2024).
- Pray, R.; Riskin, S. The History and Faults of the Body Mass Index and Where to Look Next: A Literature Review. Cureus 2023, 15, e48230. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on Sports Cardiology and Exercise in Patients with Cardiovascular Disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, L.W.; Weyand, P.G. Walking Economy Is Predictably Determined by Speed, Grade, and Gravitational Load. J. Appl. Physiol. 2017, 123, 1288–1302. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, E.M.; Mair, J.L.; Aguiar, E.; Tudor-Locke, C.; Murphy, M.H. Outdoor Walking Speeds of Apparently Healthy Adults: A Systematic Review and Meta-Analysis. Sport. Med. 2021, 51, 125–141. [Google Scholar] [CrossRef]
- Coetzee, B.A.; Bloemhoff, H.J.; Coetzee, F.F.; Schall, R. Relationship between Hikers’ Self-Reported Physical Activity Responses and Ratings of Perceived Exertion. Afr. J. Phys. Act. Health Sci. 2021, 27, 424–438. [Google Scholar] [CrossRef]
- Statista Target Group: Hikers in Italy. 2023. Available online: https://www.statista.com/study/118843/target-audience-hikers-in-italy/ (accessed on 10 November 2024).
- Cogo, A.; Fiorenzano, G. Bronchial Asthma: Advice for Patients Traveling to High Altitude. High Alt. Med. Biol. 2009, 10, 117–121. [Google Scholar] [CrossRef]
- Doan, D.; Luks, A.M. Wilderness and Adventure Travel with Underlying Asthma. Wilderness Environ. Med. 2014, 25, 231–240. [Google Scholar] [CrossRef]
- Chu, W.Y.C.; Chong, Y.C.; Mok, W.Y. Hiking-Related Orthopaedic Injuries: Another Epidemic during the COVID-19 Pandemic. J. Orthop. Trauma Rehabil. 2021, 28, 1–4. [Google Scholar] [CrossRef]
- She, S.; Tian, Y.; Lu, L.; Eimontaite, I.; Xie, T.; Sun, Y. An Exploration of Hiking Risk Perception: Dimensions and Antecedent Factors. Int. J. Environ. Res. Public Health 2019, 16, 1986. [Google Scholar] [CrossRef]
- Ciesa, M.; Grigolato, S.; Cavalli, R. Retrospective Study on Search and Rescue Operations in Two Prealps Areas of Italy. Wilderness Environ. Med. 2015, 26, 150–158. [Google Scholar] [CrossRef]
- Linsell, J.D.; Pelham, E.C.; Hondula, D.M.; Wardenaar, F.C. Hiking Time Trial Performance in the Heat with Real-Time Observation of Heat Strain, Hydration Status and Fluid Intake Behavior. Int. J. Environ. Res. Public Health 2020, 17, 4086. [Google Scholar] [CrossRef]
- Chan, C.C.Y.; Shum, H.P.; Wu, P.; Leung, N.Y.W.; Chang, L.L.; Yan, W.W. Patients with Heat-Related Illness Admitted to an Intensive Care Unit in Hong Kong: A Single-Centre Retrospective Study (2009–2020). Hong Kong J. Emerg. Med. 2023, 30, 247–252. [Google Scholar] [CrossRef]
- Fulco, C.S.; Rock, P.B. Maximal and Submaximal Exercise Performance at Altitude. Aviat. Space Environ. Med. 1998, 69, 793–801. [Google Scholar] [PubMed]
- Mangold, M.; Schwietering, A.; Zink, J.; Steinbauer, M.J.; Heurich, M. The Digitalization of Outdoor Recreation: Global Perspectives on the Opportunities and Challenges for Protected Area Management. J. Environ. Manage. 2024, 352, 120108. [Google Scholar] [CrossRef] [PubMed]
- Fattorini, L.; Pittiglio, G.; Bruno, F.; Rodio, A. Workload Comparison between Hiking and Indor Physical Activity. J Strength Cond. Res. 2012, 26, 2883–2889. [Google Scholar] [CrossRef] [PubMed]
- Sturdy, J.T.; Rizeq, H.N.; Silder, A.; Sessoms, P.H.; Silverman, A.K. Concentric and Eccentric Hip Musculotendon Work Depends on Backpack Loads and Walking Slopes. J. Biomech. 2024, 163, 111942. [Google Scholar] [CrossRef]
- Singh, G.K. High Altitude Dermatology. Indian J. Dermatol. 2017, 62, 59. [Google Scholar] [CrossRef]
- Hawke, A.L.; Jensen, R.L. Are Trekking Poles Helping or Hindering Your Hiking Experience? A Review. Wilderness Environ. Med. 2020, 31, 482–488. [Google Scholar] [CrossRef]
- Howatson, G.; Hough, P.; Pattison, J.; Hill, J.A.; Blagrove, R.; Glaister, M.; Thompson, K.G. Trekking Poles Reduce Exercise-Induced Muscle Injury during Mountain Walking. Med. Sci. Sports Exerc. 2011, 43, 140–145. [Google Scholar] [CrossRef]
- Yue, M.D.T.; Spivey, D.W.; Gingold, D.B.; Sward, D.G. The Effect of Wilderness and Medical Training on Injury and Altitude Preparedness among Backcountry Hikers in Rocky Mountain National Park. World J. Emerg. Med. 2018, 9, 172–177. [Google Scholar] [CrossRef]
- Procter, E.; Brugger, H.; Burtscher, M. Accidental Hypothermia in Recreational Activities in the Mountains: A Narrative Review. Scand. J. Med. Sci. Sports 2018, 28, 2464–2472. [Google Scholar] [CrossRef]
- Ebi, K.L.; Capon, A.; Berry, P.; Broderick, C.; de Dear, R.; Havenith, G.; Honda, Y.; Kovats, R.S.; Ma, W.; Malik, A.; et al. Hot Weather and Heat Extremes: Health Risks. Lancet 2021, 398, 698–708. [Google Scholar] [CrossRef]
- Golan, Y.; Onn, A.; Villa, Y.; Avidor, Y.; Kivity, S.; Berger, S.A.; Shapira, I.; Levo, Y.; Giladi, M. Asthma in Adventure Travelers. Arch. Intern. Med. 2002, 162, 2421. [Google Scholar] [CrossRef] [PubMed]
- Burtscher, M. Risk and Protective Factors for Sudden Cardiac Death During Leisure Activities in the Mountains: An Update. Heart Lung Circ. 2017, 26, 757–762. [Google Scholar] [CrossRef] [PubMed]
- Jan Van Veelen, M.; Roveri, G.; Voegele, A.; Dal Cappello, T.; Masè, M.; Falla, M.; Regli, I.B.; Mejia-Aguilar, A.; Mayrgündter, S.; Strapazzon, G. Drones Reduce the Treatment-Free Interval in Search and Rescue Operations with Telemedical Support-A Randomized Controlled Trial. Am. J. Emerg. Med. 2023, 66, 40–44. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Trail | Gender (Men; %) | Length (km) | Average Elevation Gain (m) | Technical Difficulty (Easy/Moderate/Difficult) | Most Popular Month | Average Max Altitude (m) | Average Min Altitude (m) | Average Coordinates | Hiking Time (h:min) |
|---|---|---|---|---|---|---|---|---|---|
| Trail #1 | 12 (60%) | 9.92 ± 0.65 | 511 ± 43 | 4/15/1 | March | 534 ± 20 | 130 ± 35 | 1770 ± 578 | 2:39 ± 39 |
| Trail #2 | 15 (75%) | 11.49 ± 0.39 | 791 ± 107 | 5/14/1 | August | 2673 ± 19 | 2059 ± 19 | 2008 ± 81 | 3:29 ± 37 |
| Trail #3 | 8 (40%) | 13.82 ± 0.87 | 570 ± 70 | 1/18/1 | August | 2492 ± 36 | 2094 ± 24 | 2368 ± 252 | 3:36 ± 44 |
| Trail #4 | 12 (60%) | 9.95 ± 0.52 | 1003 ± 105 | 2/16/2 | August | 3127 ± 23 | 2235 ± 18 | 1728 ± 159 | 3:23 ± 61 |
| Trail #5 | 16 (80%) | 11.36 ± 0.39 | 555 ± 45 | 1/16/3 | August | 2320 ± 15 | 2062 ± 13 | 2022 ± 68 | 3:31 ± 21 |
| Trail #6 | 17 (85%) | 10.49 ± 0.37 | 438 ± 31 | 2/17/1 | July | 2468 ± 26 | 2188 ± 28 | 1921 ± 264 | 3:03 ± 24 |
| Trail #7 | 13 (60%) | 13.70 ± 0.49 | 859 ± 144 | 0/19/1 | August | 2298 ± 14 | 1731 ± 13 | 2363 ± 554 | 3:58 ± 58 |
| Trail #8 | 14 (60%) | 11.38 ± 0.30 | 702 ± 67 | 0/20/0 | August | 2569 ± 21 | 2124 ± 18 | 2014 ± 93 | 3:43 ± 42 |
| Trail #9 | 15 (60%) | 11.04 ± 0.38 | 850 ± 51 | 2/16/2 | October | 2025 ± 35 | 1209 ± 21 | 1921 ± 107 | 3:20 ± 38 |
| Trail #10 | 13 (60%) | 10.92 ± 0.83 | 628 ± 70 | 5/15/0 | March | 1274 ± 44 | 699 ± 21 | 1833 ± 202 | 2:47 ± 38 |
| Trail #11 | 11 (60%) | 13.12 ± 1.25 | 284 ± 43 | 2/15/3 | August | 1418 ± 32 | 1253 ± 26 | 2068 ± 328 | 3:12 ± 67 |
| Trail #12 | 14 (60%) | 10.25 ± 1.19 | 751 ± 109 | 1/19/0 | July | 1921 ± 62 | 1232 ± 48 | 1777 ± 233 | 3:02 ± 37 |
| Trail #13 | 17 (60%) | 10.25 ± 0.47 | 497 ± 20 | 4/16/0 | November | 425 ± 24 | 49 ± 15 | 1793 ± 110 | 2:23 ± 24 |
| Trail #14 | 13 (60%) | 8.38 ± 0.43 | 374 ± 52 | 1/14/5 | March, June, July | 594 ± 65 | 331 ± 60 | 1395 ± 157 | 1:55 ± 29 |
| Trail #15 | 19 (60%) | 8.81 ± 0.63 | 223 ± 15 | 0/13/7 | August | 1371 ± 15 | 1163 ± 11 | 1523 ± 163 | 2:09 ± 18 |
| Trail #16 | 16 (60%) | 9.09 ± 0.53 | 379 ± 32 | 9/11/0 | October, November | 1854 ± 24 | 1558 ± 28 | 1567 ± 106 | 2:33 ± 33 |
| Trail #17 | 13 (60%) | 5.38 ± 0.65 | 265 ± 18 | 4/16/0 | August, September, October | 848 ± 38 | 586 ± 37 | 907 ± 104 | 1:40 ± 58 |
| Trail #18 | 15 (60%) | 9.23 ± 0.56 | 383 ± 45 | 4/16/0 | June, September, November | 746 ± 29 | 449 ± 13 | 1613 ± 194 | 2:20 ± 31 |
| Trail #19 | 12 (60%) | 14.32 ± 1.04 | 899 ± 87 | 4/16/0 | July | 1940 ± 19 | 1295 ± 84 | 2418 ± 227 | 4:39 ± 84 |
| Trail #20 | 15 (60%) | 14.01 ± 0.77 | 433 ± 61 | 4/16/0 | August | 1674 ± 23 | 1382 ± 24 | 2354 ± 186 | 3:29 ± 36 |
| Trail #21 | 12 (60%) | 8.62 ± 0.64 | 689 ± 128 | 3/16/1 | March | 595 ± 89 | 101 ± 88 | 1509 ± 120 | 3:07 ± 71 |
| Trail #22 | 14 (60%) | 10.67 ± 0.57 | 788 ± 65 | 0/13/7 | June | 2235 ± 302 | 1620 ± 304 | 1791 ± 219 | 3:29 ± 63 |
| Trail #23 | 16 (60%) | 13.90 ± 1.31 | 1165 ± 103 | 1/15/4 | July | 2840 ± 40 | 1845 ± 73 | 2387 ± 261 | 4:11 ± 44 |
| Trail #24 | 14 (60%) | 12.09 ± 0.58 | 827 ± 35 | 3/17/0 | July | 2428 ± 214 | 1658 ± 218 | 2134 ± 154 | 3:37 ± 41 |
| Trail #25 | 16 (60%) | 10.24 ± 1.15 | 857 ± 83 | 1/18/1 | August | 1341 ± 50 | 558 ± 32 | 1722 ± 326 | 2:53 ± 65 |
| TOTAL | 352 (70%) | 10.90 ± 2.22 | 628 ± 255 | 63/397/40 | August (25%) | 1760 ± 793 | 1264 ± 709 | 1876 ± 476 | 3:07 ± 62 |
| Trail | Wikiloc (hh:mm) | Komoot (hh:mm) | ∆WK (min) | p | Outdoor Active (hh:mm) | ∆WO (min) | p | Mountain Signs (hh:mm) | ∆WS (min) | p | MOVE (hh:mm) | ∆WM (min) | p |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
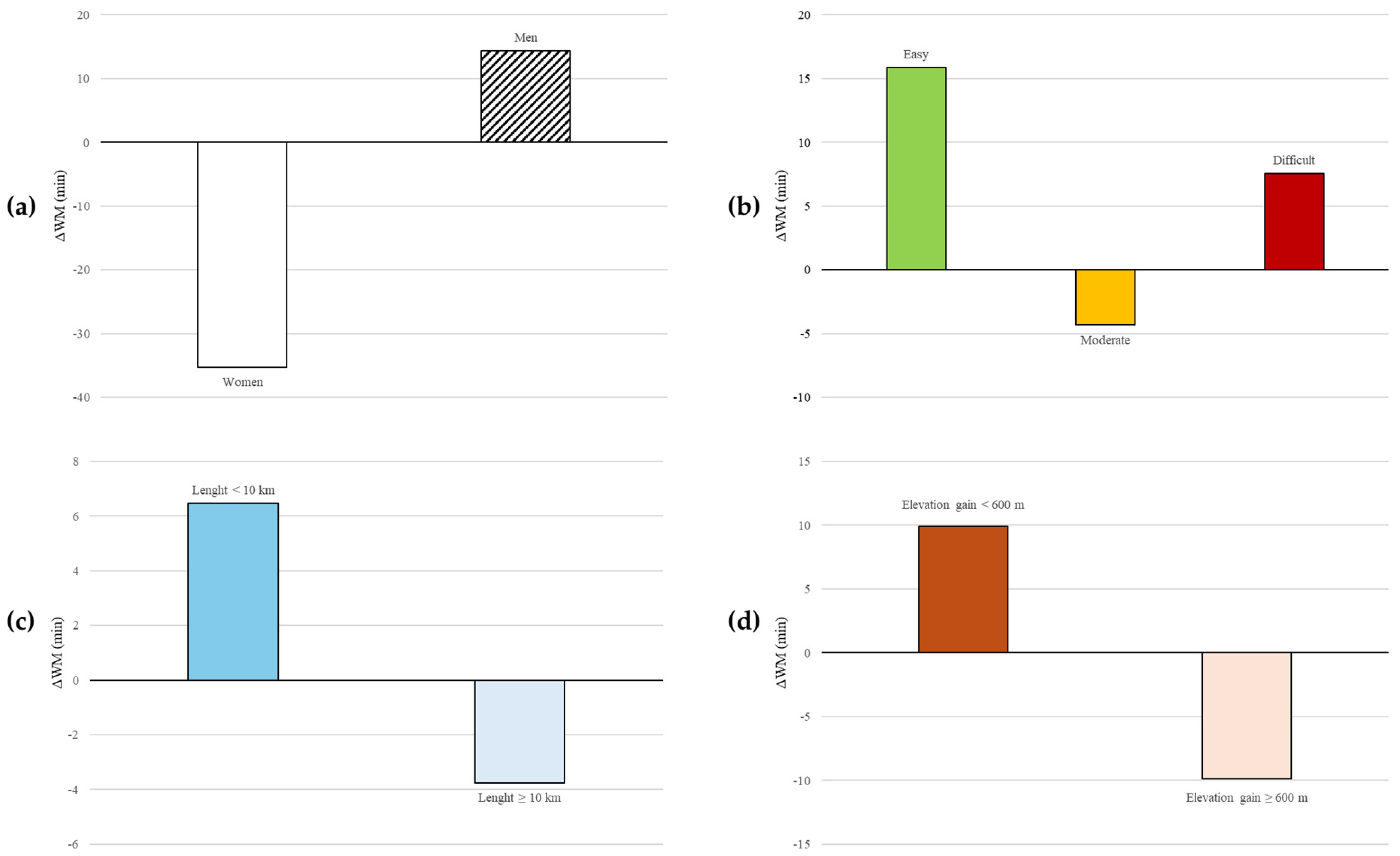
| Men (n = 352) | 3:11 ± 1:03 | 3:57 ± 1:06 | −45.92 ± 57.01 | 0.183 | 4:16 ± 1:07 | −65.09 ± 58.32 | 0.082 | 3:38 ± 1:03 | −26.65 ± 59.50 | 0.161 | 2:57 ± 1:05 | 14.37 ± 61.82 | <0.001 |
| Women (n = 141) | 2:55 ± 58 | 3:48 ± 1:05 | −53.48 ± 56.73 | 4:10 ± 59 | −75.08 ± 55.33 | 3:29 ± 1:00 | −34.99 ± 57.36 | 3:30 ± 1:14 | −35.24 ± 62.96 | ||||
| Easy (n = 63) | 2:58 ± 1:00 | 3:24 ± 59 | −25.67 ± 58.81 | <0.001 | 3:46 ± 1:04 | −47.86 ± 61.63 | 0.005 | 3:04 ± 55 | −5.47 ± 62.04 | 0.001 | 2:43 ± 1:00 | 15.86 ± 63.57 | 0.060 |
| Moderate (n = 396) | 3:04 ± 59 | 3:56 ± 1:05 | −51.63 ± 54.77 | 4:16 ± 1:05 | −71.95 ± 56.27 | 3:36 ± 1:02 | −32.64 ± 56.99 | 3:08 ± 1:09 | −4.31 ± 63.40 | ||||
| Difficult (n = 40) | 3:43 ± 1:01 | 4:47 ± 1:05 | −64.73 ± 57.21 | 5:02 ± 55 | −79.45 ± 58.36 | 4:25 ± 56 | −42.70 ± 54.60 | 3:35 ± 1:13 | 7.58 ± 74.81 | ||||
| Length <10 km (n = 171) | 2:25 ± 52 | 2:54 ± 49 | −28.63 ± 52.92 | <0.001 | 3:19 ± 52 | −54.56 ± 55.07 | <0.001 | 2:49 ± 59 | −24.06 ± 60.91 | 0.131 | 2:18 ± 50 | 6.47 ± 54.14 | 0.229 |
| Length ≥10 km (n = 329) | 3:29 ± 55 | 4:28 ± 50 | −59.47 ± 56.51 | 4:46 ± 52 | −76.69 ± 58.46 | 4:01 ± 50 | −32.47 ± 57.70 | 3:33 ± 1:04 | −3.77 ± 70.81 | ||||
| Gain <600 m (n = 243) | 2:39 ± 50 | 3:07 ± 45 | −27.63 ± 40.22 | <0.001 | 3:28 ± 48 | −48.37 ± 48.73 | <0.001 | 2:49 ± 42 | −9.74 ± 46.38 | <0.001 | 2:29 ± 46 | 9.89 ± 45.61 | <0.001 |
| Gain ≥600 m (n = 257) | 3:33 ± 1:00 | 4:42 ± 49 | −69.05 ± 63.26 | 5:02 ± 45 | −88.76 ± 59.73 | 4:22 ± 44 | −48.27 ± 63.24 | 3:43 ± 1:08 | −9.88 ± 79.12 | ||||
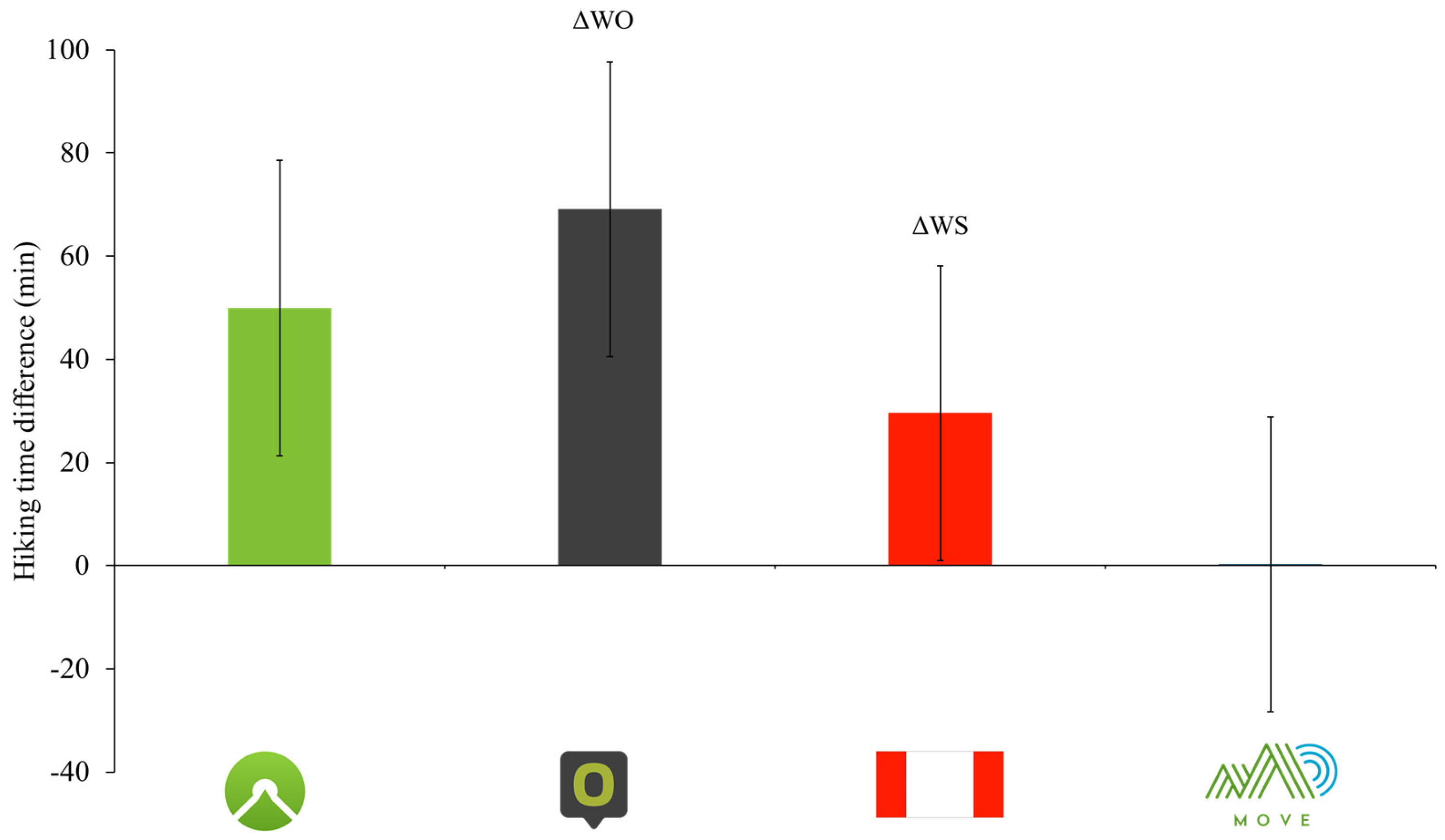
| Whole sample (n = 500) | 3:07 ± 1:02 | 3:56 ± 1:07 | −48.92 ± 57.16 | <0.001 | 4:16 ± 1:06 | −69.13 ± 58.23 | <0.001 | 3:37 ± 1:03 | −29.59 ± 59.90 | <0.001 | 3:07 ± 1:09 | −0.27 ± 65.72 | 0.278 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vecchiato, M.; Borasio, N.; Scettri, E.; Franzoi, V.; Duregon, F.; Savino, S.; Ermolao, A.; Neunhaeuserer, D. Are Suggested Hiking Times Accurate? A Validation of Hiking Time Estimations for Preventive Measures in Mountains. Medicina 2025, 61, 115. https://doi.org/10.3390/medicina61010115
Vecchiato M, Borasio N, Scettri E, Franzoi V, Duregon F, Savino S, Ermolao A, Neunhaeuserer D. Are Suggested Hiking Times Accurate? A Validation of Hiking Time Estimations for Preventive Measures in Mountains. Medicina. 2025; 61(1):115. https://doi.org/10.3390/medicina61010115
Chicago/Turabian StyleVecchiato, Marco, Nicola Borasio, Emiliano Scettri, Vanessa Franzoi, Federica Duregon, Sandro Savino, Andrea Ermolao, and Daniel Neunhaeuserer. 2025. "Are Suggested Hiking Times Accurate? A Validation of Hiking Time Estimations for Preventive Measures in Mountains" Medicina 61, no. 1: 115. https://doi.org/10.3390/medicina61010115
APA StyleVecchiato, M., Borasio, N., Scettri, E., Franzoi, V., Duregon, F., Savino, S., Ermolao, A., & Neunhaeuserer, D. (2025). Are Suggested Hiking Times Accurate? A Validation of Hiking Time Estimations for Preventive Measures in Mountains. Medicina, 61(1), 115. https://doi.org/10.3390/medicina61010115