
Influence of Extra-Articular Augmentation on Clinical Outcomes and Survival in Patients Undergoing Anterior Cruciate Ligament Reconstruction: A Pseudorandomized Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
- −
- ACL group: Isolated intra-articular arthroscopic reconstruction of the ACL.
- −
- ACL+ALL group: The intra-articular reconstruction was augmented by an extra-articular reinforcement that stemmed from the lateral aspect of the femur, slightly proximal and posterior to the epicondyle, and attached distally to the tibia, 15 mm below the joint line and half way between the fibular head and Gerdy’s tubercle [14,54,55,56,57].
2.1. Anatomy and Biomechanics of ALL
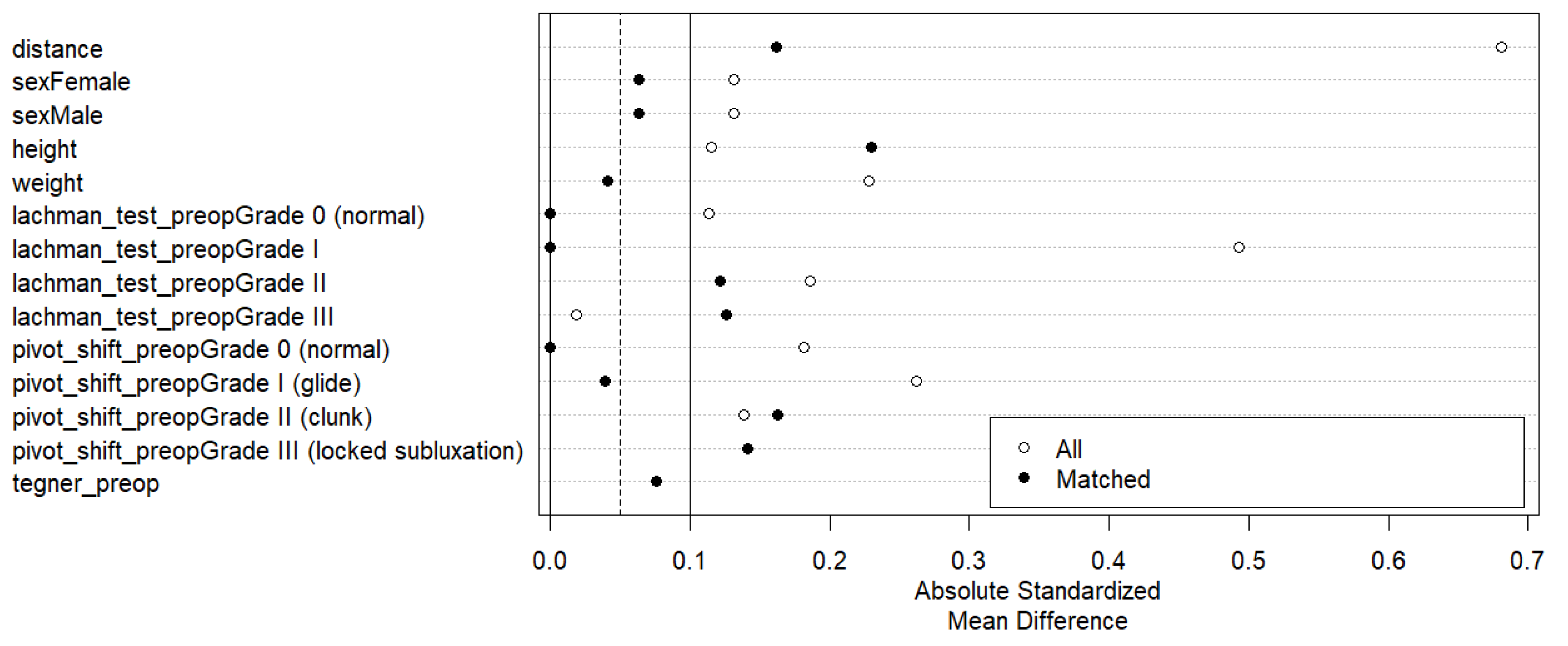
2.2. Statistical Analysis
3. Results
3.1. Anthropometry and Diagnosis
3.2. Preoperative Evaluation
3.3. Surgical Information
3.4. Evaluation During Follow-Up Period
3.5. Return to Sports Practice
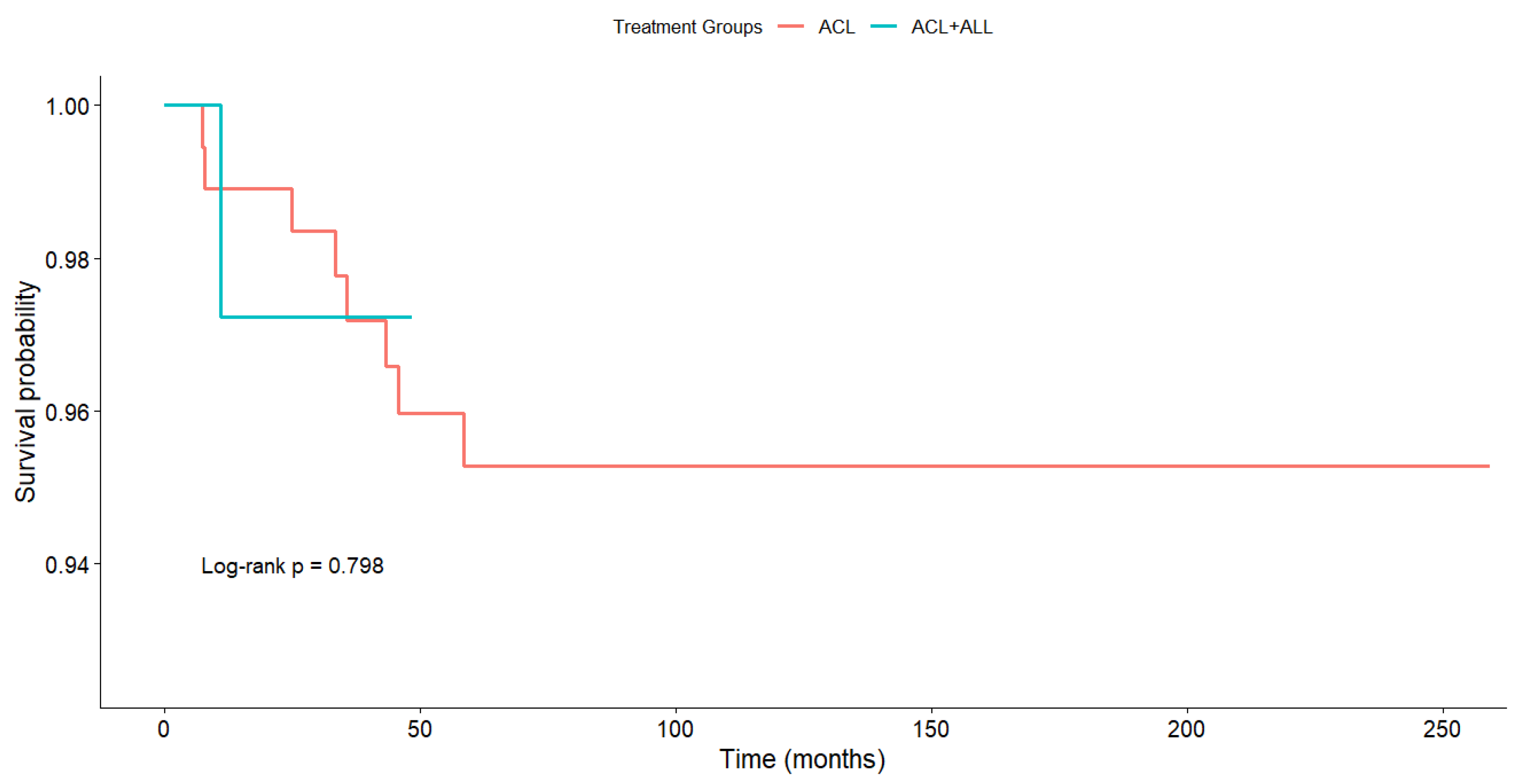
3.6. Survival
4. Discussion
4.1. Pivot Shift Test and Lachman Test
4.2. Return to Sports Practice
4.3. IKDC and Pain
4.4. YBT and Hop Tests
4.5. Survival
4.6. The Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACL | Anterior cruciate ligament |
| ALL | Anterolateral ligament |
| ACL+ALL | Anterior cruciate ligament repair combined with anterolateral ligament reconstruction |
| PCL | Posterior cruciate ligament |
| MCL | Medial collateral ligament |
| LCL | Lateral collateral ligament |
| YBT | Y-balance test |
| IKDC | International Knee Documentation Committee |
| PSM | Propensity score matching |
| VAS | Visual analog scale for pain |
References
- Bousquet, B.A.; O’Brien, L.; Singleton, S.; Beggs, M. Post-operative criterion based rehabilitation of acl repairs: A clinical commentary. Int. J. Sports Phys. Ther. 2018, 13, 293–305. [Google Scholar] [CrossRef]
- Kennedy, J.; Jackson, M.P.; O’Kelly, P.; Moran, R. Timing of Reconstruction of the Anterior Cruciate Ligament in Athletes and the Incidence of Secondary Pathology within the Knee. J. Bone Jt. Surg. Br. 2010, 92-B, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.C.; Ahn, J.H.; Lee, S.H.; Yoon, Y.C. Increasing Incidence of Medial Meniscal Tears in Nonoperatively Treated Anterior Cruciate Ligament Insufficiency Patients Documented by Serial Magnetic Resonance Imaging Studies. Am. J. Sports Med. 2009, 37, 1478–1483. [Google Scholar] [CrossRef] [PubMed]
- Sonnery-Cottet, B.; Saithna, A.; Blakeney, W.G.; Ouanezar, H.; Borade, A.; Daggett, M.; Thaunat, M.; Fayard, J.-M.; Delaloye, J.-R. Anterolateral Ligament Reconstruction Protects the Repaired Medial Meniscus: A Comparative Study of 383 Anterior Cruciate Ligament Reconstructions from the SANTI Study Group with a Minimum Follow-up of 2 Years. Am. J. Sports Med. 2018, 46, 1819–1826. [Google Scholar] [CrossRef]
- Shelbourne, K.D.; Gray, T. Results of Anterior Cruciate Ligament Reconstruction Based on Meniscus and Articular Cartilage Status at the Time of Surgery. Am. J. Sports Med. 2000, 28, 446–452. [Google Scholar] [CrossRef]
- Sommerlath, K.; Lysholm, J.; Gillquist, J. The Long-Term Course after Treatment of Acute Anterior Cruciate Ligament Ruptures. Am. J. Sports Med. 1991, 19, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, R.; Mansour, A.; Carey, J.; Spindler, K. Meniscus Status at Anterior Cruciate Ligament Reconstruction Associated with Radiographic Signs of Osteoarthritis at 5- to 10-Year Follow-Up—A Systematic Review. J. Knee Surg. 2009, 22, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Keays, S.L.; Newcombe, P.A.; Bullock-Saxton, J.E.; Bullock, M.I.; Keays, A.C. Factors Involved in the Development of Osteoarthritis after Anterior Cruciate Ligament Surgery. Am. J. Sports Med. 2010, 38, 455–463. [Google Scholar] [CrossRef]
- Wu, W.H.; Hackett, T.; Richmond, J.C. Effects of Meniscal and Articular Surface Status on Knee Stability, Function, and Symptoms after Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2002, 30, 845–850. [Google Scholar] [CrossRef]
- Ishibashi, Y.; Adachi, N.; Koga, H.; Kondo, E.; Kuroda, R.; Mae, T.; Uchio, Y. Japanese Orthopaedic Association (JOA) Clinical Practice Guidelines on the Management of Anterior Cruciate Ligament Injury—Secondary Publication. J. Orthop. Sci. 2020, 25, 6–45. [Google Scholar] [CrossRef]
- Longo, U.G.; Marino, M.; Arias, C.; Ruzzini, L.; Papalia, R.; Denaro, V. A Narrative Review of Anterior Cruciate Ligament Reconstruction in Skeletally Immature Patients. Minerva Orthop. 2024, 75, 163–170. [Google Scholar] [CrossRef]
- Passaretti, A.; Colò, G.; Bulgheroni, A.; Vulcano, E.; Surace, M.F. Gonarthrosis and ACL Lesion: An Intraoperative Analysis and Correlations in Patients Who Underwent Total Knee Arthroplasty. Minerva Orthop. 2024, 75, 331–336. [Google Scholar] [CrossRef]
- Dodds, A.L.; Gupte, C.M.; Neyret, P.; Williams, A.M.; Amis, A.A. Extra-Articular Techniques in Anterior Cruciate Ligament Reconstruction. J. Bone Jt. Surg. Br. 2011, 93, 1440–1448. [Google Scholar] [CrossRef]
- Zein, A.; Ali, M.; Ali, H.; Saleh Elsaid, A.N.; Mahmoud, A.Z.; Osman, M.K.; Mohamed Soliman, A.M. Combined Anatomic Reconstruction of the Anterior Cruciate and Anterolateral Ligaments Using Hamstring Graft Through a Single Femoral Tunnel and With a Single Femoral Fixation. Arthrosc. Tech. 2017, 6, e567–e577. [Google Scholar] [CrossRef] [PubMed]
- Chambat, P.; Guier, C.; Sonnery-Cottet, B.; Fayard, J.-M.; Thaunat, M. The Evolution of ACL Reconstruction over the Last Fifty Years. Int. Orthop. 2013, 37, 181–186. [Google Scholar] [CrossRef]
- Losee, R.E.; Johnson, T.R.; Southwick, W.O. Anterior Subluxation of the Lateral Tibial Plateau. A Diagnostic Test and Operative Repair. J. Bone Jt. Surg. Am. 1978, 60, 1015–1030. [Google Scholar] [CrossRef]
- Howe, J.G.; Johnson, R.J.; Kaplan, M.J.; Fleming, B.; Jarvinen, M. Anterior Cruciate Ligament Reconstruction Using Quadriceps Patellar Tendon Graft. Am. J. Sports Med. 1991, 19, 447–457. [Google Scholar] [CrossRef]
- Crawford, S.N.; Waterman, M.B.R.; Lubowitz, J.H. Long-Term Failure of Anterior Cruciate Ligament Reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1566–1571. [Google Scholar] [CrossRef]
- Bull, A.M.J.; Amis, A.A. The Pivot-Shift Phenomenon: A Clinical and Biomechanical Perspective. Knee 1998, 5, 141–158. [Google Scholar] [CrossRef]
- Norwood, L.A.; Andrews, J.R.; Meisterling, R.C.; Glancy, G.L. Acute Anterolateral Rotatory Instability of the Knee. J. Bone Jt. Surg. Am. 1979, 61, 704–709. [Google Scholar] [CrossRef]
- Fetto, J.F.; Marshall, J.L. Injury to the Anterior Cruciate Ligament Producing the Pivot-Shift Sign. J. Bone Jt. Surg. Am. 1979, 61, 710–714. [Google Scholar] [CrossRef]
- Dodds, A.L.; Halewood, C.; Gupte, C.M.; Williams, A.; Amis, A.A. The Anterolateral Ligament: Anatomy, Length Changes and Association with the Segond Fracture. Bone Jt. J. 2014, 96-B, 325–331. [Google Scholar] [CrossRef]
- Kittl, C.; Halewood, C.; Stephen, J.M.; Gupte, C.M.; Weiler, A.; Williams, A.; Amis, A.A. Length Change Patterns in the Lateral Extra-Articular Structures of the Knee and Related Reconstructions. Am. J. Sports Med. 2015, 43, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.H.; Patel, N.A.; Lin, C.C.; Lee, T.Q. The Anterolateral Ligament of the Knee Joint: A Review of the Anatomy, Biomechanics, and Anterolateral Ligament Surgery. Knee Surg. Relat. Res. 2019, 31, 12. [Google Scholar] [CrossRef]
- Ariel de Lima, D.; Helito, C.P.; Lacerda de Lima, L.; de Castro Silva, D.; Costa Cavalcante, M.L.; Dias Leite, J.A. Anatomy of the Anterolateral Ligament of the Knee: A Systematic Review. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 670–681. [Google Scholar] [CrossRef]
- Pomajzl, R.; Maerz, T.; Shams, C.; Guettler, J.; Bicos, J. A Review of the Anterolateral Ligament of the Knee: Current Knowledge Regarding Its Incidence, Anatomy, Biomechanics, and Surgical Dissection. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 583–591. [Google Scholar] [CrossRef]
- Daggett, M.; Stephenson, C.; Dobson, J.; Whitaker, A.; Redler, A.; Monaco, E.; Wright, B.; Saithna, A.; Sonnery-Cottet, B. Anatomic and Histological Study of the Anterolateral Aspect of the Knee: A SANTI Group Investigation. Orthop. J. Sport. Med. 2018, 6, 232596711879997. [Google Scholar] [CrossRef]
- Parsons, E.M.; Gee, A.O.; Spiekerman, C.; Cavanagh, P.R. The Biomechanical Function of the Anterolateral Ligament of the Knee. Am. J. Sports Med. 2015, 43, 669–674. [Google Scholar] [CrossRef]
- Helito, C.P.; Demange, M.K.; Bonadio, M.B.; Tírico, L.E.P.; Gobbi, R.G.; Pécora, J.R.; Camanho, G.L. Anatomy and Histology of the Knee Anterolateral Ligament. Orthop. J. Sport. Med. 2013, 1, 232596711351354. [Google Scholar] [CrossRef]
- Vincent, J.-P.; Magnussen, R.A.; Gezmez, F.; Uguen, A.; Jacobi, M.; Weppe, F.; Al-Saati, M.F.; Lustig, S.; Demey, G.; Servien, E.; et al. The Anterolateral Ligament of the Human Knee: An Anatomic and Histologic Study. Knee Surg. Sport. Traumatol. Arthrosc. 2012, 20, 147–152. [Google Scholar] [CrossRef]
- Zein, A. Step-by-Step Arthroscopic Assessment of the Anterolateral Ligament of the Knee Using Anatomic Landmarks. Arthrosc. Tech. 2015, 4, e825–e831. [Google Scholar] [CrossRef] [PubMed]
- Helito, C.P.; Demange, M.K.; Bonadio, M.B.; Tirico, L.E.P.; Gobbi, R.G.; Pecora, J.R.; Camanho, G.L. Radiographic Landmarks for Locating the Femoral Origin and Tibial Insertion of the Knee Anterolateral Ligament. Am. J. Sports Med. 2014, 42, 2356–2362. [Google Scholar] [CrossRef] [PubMed]
- Claes, S.; Vereecke, E.; Maes, M.; Victor, J.; Verdonk, P.; Bellemans, J. Anatomy of the Anterolateral Ligament of the Knee. J. Anat. 2013, 223, 321–328. [Google Scholar] [CrossRef]
- Claes, S.; Bartholomeeusen, S.; Bellemans, J. High Prevalence of Anterolateral Ligament Abnormalities in Magnetic Resonance Images of Anterior Cruciate Ligament-Injured Knees. Acta Orthop. Belg. 2014, 80, 45–49. [Google Scholar] [PubMed]
- Sonnery-Cottet, B.; Daggett, M.; Fayard, J.-M.; Ferretti, A.; Helito, C.P.; Lind, M.; Monaco, E.; de Pádua, V.B.C.; Thaunat, M.; Wilson, A.; et al. Anterolateral Ligament Expert Group Consensus Paper on the Management of Internal Rotation and Instability of the Anterior Cruciate Ligament—Deficient Knee. J. Orthop. Traumatol. 2017, 18, 91–106. [Google Scholar] [CrossRef]
- Sonnery-Cottet, B.; Saithna, A.; Cavalier, M.; Kajetanek, C.; Temponi, E.F.; Daggett, M.; Helito, C.P.; Thaunat, M. Anterolateral Ligament Reconstruction Is Associated with Significantly Reduced ACL Graft Rupture Rates at a Minimum Follow-up of 2 Years: A Prospective Comparative Study of 502 Patients from the SANTI Study Group. Am. J. Sports Med. 2017, 45, 1547–1557. [Google Scholar] [CrossRef]
- Tramer, J.S.; Fidai, M.S.; Kadri, O.; Jildeh, T.R.; Hooda, Z.; Makhni, E.C.; Lock, T. Anterolateral Ligament Reconstruction Practice Patterns Across the United States. Orthop. J. Sport. Med. 2018, 6, 232596711881106. [Google Scholar] [CrossRef] [PubMed]
- Reider, B. ACL or ACL+. Am. J. Sports Med. 2020, 48, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Sonnery-Cottet, B.; Thaunat, M.; Freychet, B.; Pupim, B.H.B.; Murphy, C.G.; Claes, S. Outcome of a Combined Anterior Cruciate Ligament and Anterolateral Ligament Reconstruction Technique with a Minimum 2-Year Follow-Up. Am. J. Sports Med. 2015, 43, 1598–1605. [Google Scholar] [CrossRef] [PubMed]
- Clancy, W.G.; Nelson, D.A.; Reider, B.; Narechania, R.G. Anterior Cruciate Ligament Reconstruction Using One-Third of the Patellar Ligament, Augmented by Extra-Articular Tendon Transfers. J. Bone Jt. Surg. Am. 1982, 64, 352–359. [Google Scholar] [CrossRef]
- Dejour, H.; Dejour, D.; Aït Si Selmi, T. Laxité Chronique Du Genou Traité Par Une Greffe de Tendon Rotulien Libre et Une Plastie Extra Articulaire Antérolatérale. 10 Ans de Recul. 148 Cas. Rev. Chir. Orthop. Réparatrice Appar. Locomot. 1999, 85, 777–789. [Google Scholar]
- Marcacci, M.; Zaffagnini, S.; Iacono, F.; Neri, M.P.; Loreti, I.; Petitto, A. Arthroscopic Intra- and Extra-Articular Anterior Cruciate Ligament Reconstruction with Gracilis and Semitendinosus Tendons. Knee Surg. Sport. Traumatol. Arthrosc. 1998, 6, 68–75. [Google Scholar] [CrossRef]
- Vadalà, A.P.; Iorio, R.; De Carli, A.; Bonifazi, A.; Iorio, C.; Gatti, A.; Rossi, C.; Ferretti, A. An Extra-Articular Procedure Improves the Clinical Outcome in Anterior Cruciate Ligament Reconstruction with Hamstrings in Female Athletes. Int. Orthop. 2013, 37, 187–192. [Google Scholar] [CrossRef]
- Monaco, E.; Maestri, B.; Conteduca, F.; Mazza, D.; Iorio, C.; Ferretti, A. Extra-Articular ACL Reconstruction and Pivot Shift. Am. J. Sports Med. 2014, 42, 1669–1674. [Google Scholar] [CrossRef] [PubMed]
- Duthon, V.B.; Magnussen, R.A.; Servien, E.; Neyret, P. ACL Reconstruction and Extra-Articular Tenodesis. Clin. Sports Med. 2013, 32, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Colombet, P.D. Navigated Intra-Articular ACL Reconstruction with Additional Extra-Articular Tenodesis Using the Same Hamstring Graft. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 384–389. [Google Scholar] [CrossRef]
- Song, G.; Hong, L.; Zhang, H.; Zhang, J.; Li, Y.; Feng, H. Clinical Outcomes of Combined Lateral Extra-Articular Tenodesis and Intra-Articular Anterior Cruciate Ligament Reconstruction in Addressing High-Grade Pivot-Shift Phenomenon. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 898–905. [Google Scholar] [CrossRef]
- O’Brien, S.J.; Warren, R.F.; Pavlov, H.; Panariello, R.; Wickiewicz, T.L. Reconstruction of the Chronically Insufficient Anterior Cruciate Ligament with the Central Third of the Patellar Ligament. J. Bone Jt. Surg. Am. 1991, 73, 278–286. [Google Scholar] [CrossRef]
- Roth, J.H.; Kennedy, J.C.; Lockstadt, H.; McCallum, C.L.; Cunning, L.A. Intra-Articular Reconstruction of the Anterior Cruciate Ligament with and without Extra-Articular Supplementation by Transfer of the Biceps Femoris Tendon. J. Bone Jt. Surg. Am. 1987, 69, 275–278. [Google Scholar] [CrossRef]
- Pernin, J.; Verdonk, P.; Si Selmi, T.A.; Massin, P.; Neyret, P. Long-Term Follow-Up of 24.5 Years After Intra-Articular Anterior Cruciate Ligament Reconstruction with Lateral Extra-Articular Augmentation. Am. J. Sports Med. 2010, 38, 1094–1102. [Google Scholar] [CrossRef]
- Ferretti, A.; Monaco, E.; Ponzo, A.; Basiglini, L.; Iorio, R.; Caperna, L.; Conteduca, F. Combined Intra-Articular and Extra-Articular Reconstruction in Anterior Cruciate Ligament–Deficient Knee: 25 Years Later. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 2039–2047. [Google Scholar] [CrossRef]
- Thiese, M.S. Observational and Interventional Study Design Types; an Overview. Biochem. Medica 2014, 24, 199–210. [Google Scholar] [CrossRef]
- López Capdevilla, L.; Santamaría Fumas, A.; Sales Pérez, J.M.; Domínguez Sevilla, A.; del Corral Cuervo, J.; Varela-Quintana, C.; Rabanal Rubio, M.; Roza Miguel, P. Amputation versus Circular External Fixation in the Treatment of Diabetic Foot with Osteomyelitis: A Cost and Quality-of-Life Analysis. Ther. Adv. Endocrinol. Metab. 2024, 15, 20420188241271795. [Google Scholar] [CrossRef] [PubMed]
- Maestro, A.; Maestro Fernández, A.; Pipa Muñiz, I.; Rodríguez García, N.; Maestro, A. Two-Stage Anterior Cruciate Ligament Reconstruction Revision Surgery for Severe Bone Defects with Anterolateral Ligament Reconstruction Technique. Arthrosc. Tech. 2020, 9, e327–e337. [Google Scholar] [CrossRef]
- Boutsiadis, A.; Brossard, P.; Panisset, J.-C.; Graveleau, N.; Barth, J. Minimally Invasive Combined Anterior and Anterolateral Stabilization of the Knee Using Hamstring Tendons and Adjustable-Loop Suspensory Fixation Device: Surgical Technique. Arthrosc. Tech. 2017, 6, e419–e425. [Google Scholar] [CrossRef] [PubMed]
- Saithna, A.; Thaunat, M.; Delaloye, J.R.; Ouanezar, H.; Fayard, J.M.; Sonnery-Cottet, B. Combined ACL and Anterolateral Ligament Reconstruction. JBJS Essent. Surg. Tech. 2018, 8, e2. [Google Scholar] [CrossRef]
- Helito, C.P.; Bonadio, M.B.; Gobbi, R.G.; da Mota e Albuquerque, R.F.; Pécora, J.R.; Camanho, G.L.; Demange, M.K. Combined Intra- and Extra-Articular Reconstruction of the Anterior Cruciate Ligament: The Reconstruction of the Knee Anterolateral Ligament. Arthrosc. Tech. 2015, 4, e239–e244. [Google Scholar] [CrossRef]
- Gurtler, R.A.; Stine, R.; Torg, J.S. Lachman Test Evaluated. Quantification of a Clinical Observation. Clin. Orthop. Relat. Res. 1987, 216, 141–150. [Google Scholar] [CrossRef]
- Galway, R.D.; Beaupre, A.; McIntosh, D.L. Pivot Shift: A Clinical Sign of Symptomatic Anterior Cruciate Insufficiency. Bone Jt. Surg. Br. 1972, 54B, 763–764. [Google Scholar]
- Tegner, Y.; Lysholm, J. Rating Systems in the Evaluation of Knee Ligament Injuries. Clin. Orthop. Relat. Res. 1985, 198, 43–49. [Google Scholar] [CrossRef]
- Hayes, M.; Patterson, D. Experimental Development of the Graphic Rating Method. Psychol. Bull. 1921, 18, 98–99. [Google Scholar]
- Gustavsson, A.; Neeter, C.; Thomeé, P.; Grävare Silbernagel, K.; Augustsson, J.; Thomeé, R.; Karlsson, J. A Test Battery for Evaluating Hop Performance in Patients with an ACL Injury and Patients Who Have Undergone ACL Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 778–788. [Google Scholar] [CrossRef] [PubMed]
- Hertel, J.; Braham, R.A.; Hale, S.A.; Olmsted-Kramer, L.C. Simplifying the Star Excursion Balance Test: Analyses of Subjects with and Without Chronic Ankle Instability. J. Orthop. Sports Phys. Ther. 2006, 36, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Stiffler, M.R.; Sanfilippo, J.L.; Brooks, M.A.; Heiderscheit, B.C. Star Excursion Balance Test Performance Varies by Sport in Healthy Division I Collegiate Athletes. J. Orthop. Sports Phys. Ther. 2015, 45, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Hertel, J. Sensorimotor Deficits with Ankle Sprains and Chronic Ankle Instability. Clin. Sports Med. 2008, 27, 353–370. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Hertel, J.; Plisky, P. Using the Star Excursion Balance Test to Assess Dynamic Postural-Control Deficits and Outcomes in Lower Extremity Injury: A Literature and Systematic Review. J. Athl. Train. 2012, 47, 339–357. [Google Scholar] [CrossRef]
- Irrgang, J.J.; Anderson, A.F.; Boland, A.L.; Harner, C.D.; Kurosaka, M.; Neyret, P.; Richmond, J.C.; Shelborne, K.D. Development and Validation of the International Knee Documentation Committee Subjective Knee Form. Am. J. Sports Med. 2001, 29, 600–613. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.-Y.; Luo, J.-C.; Su, Y.; Zhang, Y.-J.; Tu, G.-W.; Luo, Z. Propensity Score Matching with R: Conventional Methods and New Features. Ann. Transl. Med. 2021, 9, 812. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.W.; Maldonado, D.R.; Kowalski, B.L.; Miecznikowski, K.B.; Kyin, C.; Gornbein, J.A.; Domb, B.G. Best Practice Guidelines for Propensity Score Methods in Medical Research: Consideration on Theory, Implementation, and Reporting. A Review. Arthrosc. J. Arthrosc. Relat. Surg. 2022, 38, 632–642. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. 2020. Available online: https://ropensci.org/blog/2021/11/16/h (accessed on 1 April 2019).
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef]
- Meuffels, D.E.; Poldervaart, M.T.; Diercks, R.L.; Fievez, A.W.F.M.; Patt, T.W.; Van Der Hart, C.P.; Hammacher, E.R.; Van Der Meer, F.; Goedhart, E.A.; Lenssen, A.F.; et al. Guideline on Anterior Cruciate Ligament Injury. Acta Orthop. 2012, 83, 379–386. [Google Scholar] [CrossRef]
- Carey, J.L.; Shea, K.G. AAOS Clinical Practice Guideline. J. Am. Acad. Orthop. Surg. 2015, 23, e6–e8. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.S.; Steadman, J.R.; Briggs, K.K.; Sterett, W.I.; Hawkins, R.J. Relationships between Objective Assessment of Ligament Stability and Subjective Assessment of Symptoms and Function after Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2004, 32, 629–634. [Google Scholar] [CrossRef]
- Kubo, S.; Muratsu, H.; Yoshiya, S.; Mizuno, K.; Kurosaka, M. Reliability and Usefulness of a New In Vivo Measurement System of the Pivot Shift. Clin. Orthop. Relat. Res. 2007, 454, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Acquitter, Y.; Hulet, C.; Locker, B.; Delbarre, J.-C.; Jambou, S.; Vielpeau, C. Patellar Tendon-Bone Autograft Reconstruction of the Anterior Cruciate Ligament for Advanced-Stage Chronic Anterior Laxity: Is an Extra-Articular Plasty Necessary? A Prospective Randomized Study of 100 Patients with Five Year Follow-Up. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2003, 89, 413–422. [Google Scholar]
- Draganich, L.F.; Reider, B.; Ling, M.; Samuelson, M. An in Vitro Study of an Intraarticular and Extraarticular Reconstruction in the Anterior Cruciate Ligament Deficient Knee. Am. J. Sports Med. 1990, 18, 262–266. [Google Scholar] [CrossRef]
- Engebretsen, L.; Lew, W.D.; Lewis, J.L.; Hunter, R.E. The Effect of an Iliotibial Tenodesis on Intraarticular Graft Forces and Knee Joint Motion. Am. J. Sports Med. 1990, 18, 169–176. [Google Scholar] [CrossRef]
- Colombet, P. Knee Laxity Control in Revision Anterior Cruciate Ligament Reconstruction Versus Anterior Cruciate Ligament Reconstruction and Lateral Tenodesis. Am. J. Sports Med. 2011, 39, 1248–1254. [Google Scholar] [CrossRef]
- Giraud, B.; Besse, J.-L.; Cladière, F.; Ecochard, R.; Moyen, B.; Lerat, J.-L. Influence d’une Ligamentoplastie Extra-Articulaire Latérale Sur Les Résultats de La Reconstruction Du Ligament Croisé Antérieur Avec Le Ligament Patellaire Avec 7 Ans de Recul. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2006, 92, 788–797. [Google Scholar] [CrossRef] [PubMed]
- Hewison, C.E.; Tran, M.N.; Kaniki, N.; Remtulla, A.; Bryant, D.; Getgood, A.M. Lateral Extra-Articular Tenodesis Reduces Rotational Laxity When Combined with Anterior Cruciate Ligament Reconstruction: A Systematic Review of the Literature. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 2022–2034. [Google Scholar] [CrossRef] [PubMed]
- Rosenstiel, N.; Praz, C.; Ouanezar, H.; Saithna, A.; Fournier, Y.; Hager, J.-P.; Thaunat, M.; Sonnery-Cottet, B. Combined Anterior Cruciate and Anterolateral Ligament Reconstruction in the Professional Athlete: Clinical Outcomes from the Scientific Anterior Cruciate Ligament Network International Study Group in a Series of 70 Patients with a Minimum Follow-Up of 2 Y. Arthrosc. J. Arthrosc. Relat. Surg. 2019, 35, 885–892. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fifty-Five per Cent Return to Competitive Sport Following Anterior Cruciate Ligament Reconstruction Surgery: An Updated Systematic Review and Meta-Analysis Including Aspects of Physical Functioning and Contextual Factors. Br. J. Sports Med. 2014, 48, 1543–1552. [Google Scholar] [CrossRef] [PubMed]
- Hurley, E.T.; Manjunath, A.K.; Strauss, E.J.; Jazrawi, L.M.; Alaia, M.J. Return to Play After Anterior Cruciate Ligament Reconstruction with Extra-Articular Augmentation: A Systematic Review. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 381–387. [Google Scholar] [CrossRef]
- Laboudie, P.; Douiri, A.; Bouguennec, N.; Biset, A.; Graveleau, N. Combined ACL and ALL Reconstruction Reduces the Rate of Reoperation for Graft Failure or Secondary Meniscal Lesions in Young Athletes. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 3488–3498. [Google Scholar] [CrossRef] [PubMed]
- Sonnery-Cottet, B.; Haidar, I.; Rayes, J.; Fradin, T.; Ngbilo, C.; Vieira, T.D.; Freychet, B.; Ouanezar, H.; Saithna, A. Long-Term Graft Rupture Rates After Combined ACL and Anterolateral Ligament Reconstruction Versus Isolated ACL Reconstruction: A Matched-Pair Analysis from the SANTI Study Group. Am. J. Sports Med. 2021, 49, 2889–2897. [Google Scholar] [CrossRef] [PubMed]
- Coquard, M.; Carrozzo, A.; Saithna, A.; Vigne, G.; Le Guen, M.; Fournier, Y.; Hager, J.-P.; Vieira, T.D.; Sonnery-Cottet, B. Anterolateral Ligament Reconstruction Does Not Delay Functional Recovery, Rehabilitation, and Return to Sport After Anterior Cruciate Ligament Reconstruction: A Matched-Pair Analysis from the SANTI (Scientific ACL Network International) Study Group. Arthrosc. Sports Med. Rehabil. 2022, 4, e9–e16. [Google Scholar] [CrossRef] [PubMed]
- Getgood, A.; Hewison, C.; Bryant, D.; Litchfield, R.; Heard, M.; Buchko, G.; Hiemstra, L.A.; Willits, K.R.; Firth, A.; MacDonald, P. No Difference in Functional Outcomes When Lateral Extra-Articular Tenodesis Is Added to Anterior Cruciate Ligament Reconstruction in Young Active Patients: The Stability Study. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 1690–1701. [Google Scholar] [CrossRef]
- Helito, C.P.; Camargo, D.B.; Sobrado, M.F.; Bonadio, M.B.; Giglio, P.N.; Pécora, J.R.; Camanho, G.L.; Demange, M.K. Combined Reconstruction of the Anterolateral Ligament in Chronic ACL Injuries Leads to Better Clinical Outcomes than Isolated ACL Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3652–3659. [Google Scholar] [CrossRef]
- Plisky, P.J.; Rauh, M.J.; Kaminski, T.W.; Underwood, F.B. Star Excursion Balance Test as a Predictor of Lower Extremity Injury in High School Basketball Players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef]
- Butler, R.J.; Lehr, M.E.; Fink, M.L.; Kiesel, K.B.; Plisky, P.J. Dynamic Balance Performance and Noncontact Lower Extremity Injury in College Football Players. Sports Health A Multidiscip. Approach 2013, 5, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, E.M.; Greenberg, E.T.; Ganley, T.J.; Lawrence, J.T.R. Strength and Functional Performance Recovery After Anterior Cruciate Ligament Reconstruction in Preadolescent Athletes. Sports Health A Multidiscip. Approach 2014, 6, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Lockie, R.G.; Callaghan, S.J.; Berry, S.P.; Cooke, E.R.A.; Jordan, C.A.; Luczo, T.M.; Jeffriess, M.D. Relationship Between Unilateral Jumping Ability and Asymmetry on Multidirectional Speed in Team-Sport Athletes. J. Strength Cond. Res. 2014, 28, 3557–3566. [Google Scholar] [CrossRef] [PubMed]
- Sannicandro, I.; Cofano, G.; Rosa, R.A.; Piccinno, A. Balance Training Exercises Decrease Lower-Limb Strength Asymmetry in Young Tennis Players. J. Sports Sci. Med. 2014, 13, 397–402. [Google Scholar] [PubMed]
- Gribble, P.A.; Hertel, J. Considerations for Normalizing Measures of the Star Excursion Balance Test. Meas. Phys. Educ. Exerc. Sci. 2003, 7, 89–100. [Google Scholar] [CrossRef]
- Magnussen, R.A.; Reinke, E.K.; Huston, L.J.; Hewett, T.E.; Spindler, K.P.; Andrish, J.T.; Jones, M.H.; Parker, R.D.; McCarty, E.C.; Marx, R.G.; et al. Effect of High-Grade Preoperative Knee Laxity on Anterior Cruciate Ligament Reconstruction Outcomes. Am. J. Sports Med. 2016, 44, 3077–3082. [Google Scholar] [CrossRef]
- Hopper, G.P.; Pioger, C.; Philippe, C.; El Helou, A.; Campos, J.P.; Gousopoulos, L.; Carrozzo, A.; Vieira, T.D.; Sonnery-Cottet, B. Risk Factors for Anterior Cruciate Ligament Graft Failure in Professional Athletes: An Analysis of 342 Patients with a Mean Follow-up of 100 Months from the SANTI Study Group. Am. J. Sports Med. 2022, 50, 3218–3227. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Feller, J.A. Exploring the High Reinjury Rate in Younger Patients Undergoing Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2016, 44, 2827–2832. [Google Scholar] [CrossRef] [PubMed]
- Kamath, G.V.; Murphy, T.; Creighton, R.A.; Viradia, N.; Taft, T.N.; Spang, J.T. Anterior Cruciate Ligament Injury, Return to Play, and Reinjury in the Elite Collegiate Athlete. Am. J. Sports Med. 2014, 42, 1638–1643. [Google Scholar] [CrossRef]
- Carey, T.; Sanders, G.; Viswanathan, M. Framework for Considering Study Designs for Future Research Needs [Internet]. Agency for Healthcare Research and Quality (US). Available online: https://www.ncbi.nlm.nih.gov/books/NBK95280/ (accessed on 20 September 2024).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) | Mean | SD | p-Value |
|---|---|---|---|---|
| Sex (M/F) | ||||
| ACL | 58 (78%)/16 (22%) | - | - | 0.748 |
| ACL+ALL | 28 (76%)/9 (24%) | - | - | |
| Laterality (R/L) | ||||
| ACL | 33 (45%)/40 (55%) | - | - | 0.542 |
| ACL+ALL | 19 (51%)/18 (49%) | - | - | |
| Age | ||||
| ACL | - | 30.9 | 11.9 | 0.781 |
| ACL+ALL | - | 30.2 | 15.1 | |
| Height | ||||
| ACL | - | 171.2 | 8.4 | 0.927 |
| ACL+ALL | - | 173.4 | 9.6 | |
| Weight | ||||
| ACL | - | 73.2 | 10.8 | 0.714 |
| ACL+ALL | - | 72.3 | 12.1 |
| Variable | N (%) | Mean | SD | p-Value |
|---|---|---|---|---|
| Injured limb—Flexion (°) | ||||
| ACL | - | 108.6 | 14.1 | 0.169 |
| ACL+ALL | - | 113.5 | 19.1 | |
| Injured limb—Extension (°) | ||||
| ACL | - | −3.6 | 3.1 | 0.747 |
| ACL+ALL | - | −3.8 | 4.3 | |
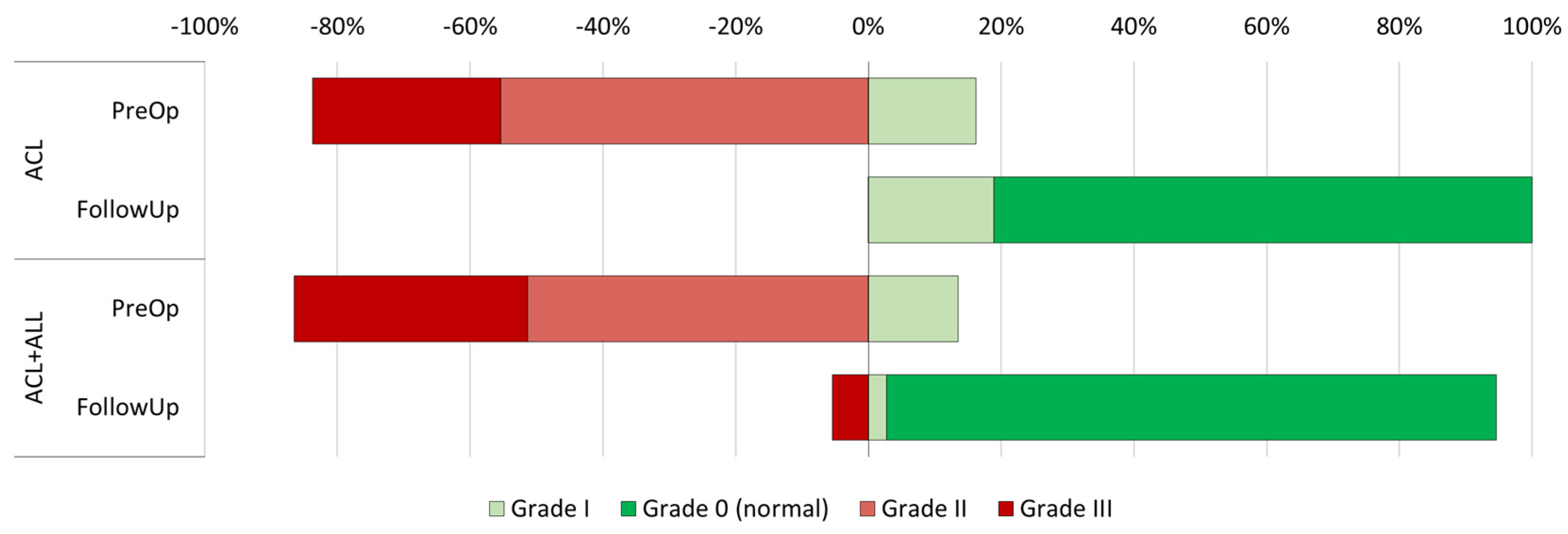
| Lachman test—PreOp | ||||
| ACL | 0.350 | |||
| Normal | 0 (0%) | - | - | |
| Grade I | 3 (4%) | - | - | |
| Grade II | 61 (82%) | - | - | |
| Grade III | 10 (14%) | - | - | |
| ACL+ALL | ||||
| Normal | 0 (0%) | - | - | |
| Grade I | 1 (3%) | - | - | |
| Grade II | 27 (73%) | - | - | |
| Grade III | 9 (24%) | - | - | |
| Pivot shift—PreOp | ||||
| ACL | 0.756 | |||
| Grade 0 (normal) | 0 (0%) | - | - | |
| Grade I (glide) | 12 (16%) | - | - | |
| Grade II (clunk) | 41 (55%) | - | - | |
| Grade III (locked subluxation) | 21 (28%) | - | - | |
| ACL+ALL | ||||
| Grade 0 (normal) | 0 (0%) | - | - | |
| Grade I (glide) | 5 (14%) | - | - | |
| Grade II (clunk) | 19 (51%) | - | - | |
| Grade III (locked subluxation) | 13 (35%) | - | - |
| Variable | N (%) | Mean | SD | p-Value |
|---|---|---|---|---|
| Meniscal repair | ||||
| ACL | 45 (61%) | - | - | 0.678 |
| ACL+ALL | 24 (65%) | - | - | |
| Chondral repair | ||||
| ACL | 3 (4%) | - | - | 0.219 |
| ACL+ALL | 4 (11%) | - | - | |
| IntraOp complications | ||||
| ACL | 4 (5%) | - | - | 0.299 |
| ACL+ALL | 0 (0%) | - | - |
| Variable | N (%) | Mean | SD | p-Value |
|---|---|---|---|---|
| Injured limb—Flexion (°) | ||||
| ACL | - | 133.2 | 7.7 | 0.037 * |
| ACL+ALL | - | 129.6 | 9.8 | |
| Injured limb—Extension (°) | ||||
| ACL | - | −0.1 | 0.8 | 0.191 |
| ACL+ALL | - | −0.7 | 2.4 | |
| Lachman test—Follow-Up | ||||
| ACL | 0.201 | |||
| Normal | 58 (78%) | - | - | |
| Grade I | 14 (19%) | - | - | |
| Grade II | 2 (2%) | - | - | |
| Grade III | 0 (0%) | - | - | |
| ACL+ALL | ||||
| Normal | 32 (86%) | - | - | |
| Grade I | 3 (8%) | - | - | |
| Grade II | 1 (3%) | - | - | |
| Grade III | 1 (3%) | - | - | |
| Pivot shift—Follow-Up | ||||
| ACL | 0.007 * | |||
| Grade 0 (normal) | 60 (81%) | - | - | |
| Grade I | 14 (19%) | - | - | |
| Grade II | 0 (0%) | - | - | |
| Grade III | 0 (0%) | - | - | |
| ACL+ALL | ||||
| Grade 0 (normal) | 34 (92%) | - | - | |
| Grade I | 1 (3%) | - | - | |
| Grade II | 0 (0%) | - | - | |
| Grade III | 2 (5%) | - | - | |
| IKDC Knee score—Follow-Up | ||||
| ACL | 0.169 | |||
| A—Normal | 70 (95%) | - | - | |
| B—Nearly normal | 4 (5%) | - | - | |
| C—Abnormal | 0 (0%) | - | - | |
| D—Severely abnormal | 0 (0%) | - | - | |
| ACL+ALL | ||||
| A—Normal | 35 (97%) | - | - | |
| B—Nearly normal | 0 (0%) | - | - | |
| C—Abnormal | 1 (3%) | - | - | |
| D—Severely abnormal | 0 (0%) | - | - | |
| IKDC Subjective Score—Follow-Up | ||||
| ACL | - | 82.4 | 5.8 | 0.095 |
| ACL+ALL | - | 83.0 | 9.1 | |
| Pain—VAS | ||||
| ACL | - | 0.70 | 1.3 | 0.928 |
| ACL+ALL | - | 0.68 | 1.2 | |
| Complications During Treatment | ||||
| ACL | 7 (9%) | - | - | 0.529 |
| ACL+ALL | 5 (14%) | - | - |
| Variable | Mean | SD | p-Value |
|---|---|---|---|
| LSI—Single hop test | |||
| ACL | 95.3 | 15.4 | 0.710 |
| ACL+ALL | 94.2 | 13.5 | |
| LSI—Triple hop test | |||
| ACL | 96.4 | 12.9 | 0.653 |
| ACL+ALL | 98.0 | 20.2 | |
| LSI—Crossover hop test | |||
| ACL | 94.6 | 15.0 | 0.682 |
| ACL+ALL | 95.8 | 13.9 | |
| LSI—6 meter timed hop test | |||
| ACL | 102.7 | 12.2 | 0.360 |
| ACL+ALL | 105.5 | 15.3 | |
| LSI—YBT composite score (normalized) | |||
| ACL | 100.0 | 12.6 | 0.488 |
| ACL+ALL | 98.4 | 10.2 |
| Return to Sports | ACL | ACL+ALL | p-Value |
|---|---|---|---|
| Same or better level | 83.8% | 81.1% | 0.723 |
| Worse level | 16.2% | 18.9% |
| Group | Same or Better Level | Worse Level | P-Value |
|---|---|---|---|
| Sex | |||
| Males | 84.1% | 15.9% | 0.539 |
| Females | 78.3% | 21.7% | |
| Meniscal damage | |||
| No | 84.1% | 15.9% | 0.674 |
| Yes | 81.0% | 19.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maestro, A.; Rodríguez, N.; Pipa, I.; Toyos, C.; Lanuza, L.; Machado, F.; Castaño, C.; Maestro, S. Influence of Extra-Articular Augmentation on Clinical Outcomes and Survival in Patients Undergoing Anterior Cruciate Ligament Reconstruction: A Pseudorandomized Study. Medicina 2025, 61, 116. https://doi.org/10.3390/medicina61010116
Maestro A, Rodríguez N, Pipa I, Toyos C, Lanuza L, Machado F, Castaño C, Maestro S. Influence of Extra-Articular Augmentation on Clinical Outcomes and Survival in Patients Undergoing Anterior Cruciate Ligament Reconstruction: A Pseudorandomized Study. Medicina. 2025; 61(1):116. https://doi.org/10.3390/medicina61010116
Chicago/Turabian StyleMaestro, Antonio, Nicolás Rodríguez, Iván Pipa, Carmen Toyos, Lucía Lanuza, Filipe Machado, César Castaño, and Santiago Maestro. 2025. "Influence of Extra-Articular Augmentation on Clinical Outcomes and Survival in Patients Undergoing Anterior Cruciate Ligament Reconstruction: A Pseudorandomized Study" Medicina 61, no. 1: 116. https://doi.org/10.3390/medicina61010116
APA StyleMaestro, A., Rodríguez, N., Pipa, I., Toyos, C., Lanuza, L., Machado, F., Castaño, C., & Maestro, S. (2025). Influence of Extra-Articular Augmentation on Clinical Outcomes and Survival in Patients Undergoing Anterior Cruciate Ligament Reconstruction: A Pseudorandomized Study. Medicina, 61(1), 116. https://doi.org/10.3390/medicina61010116