Efficacy of Low-Dose Paroxetine for the Treatment of Hot Flushes in Surgical and Physiological Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Trials

 ,
,  , ,
, ,  ,
, 


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
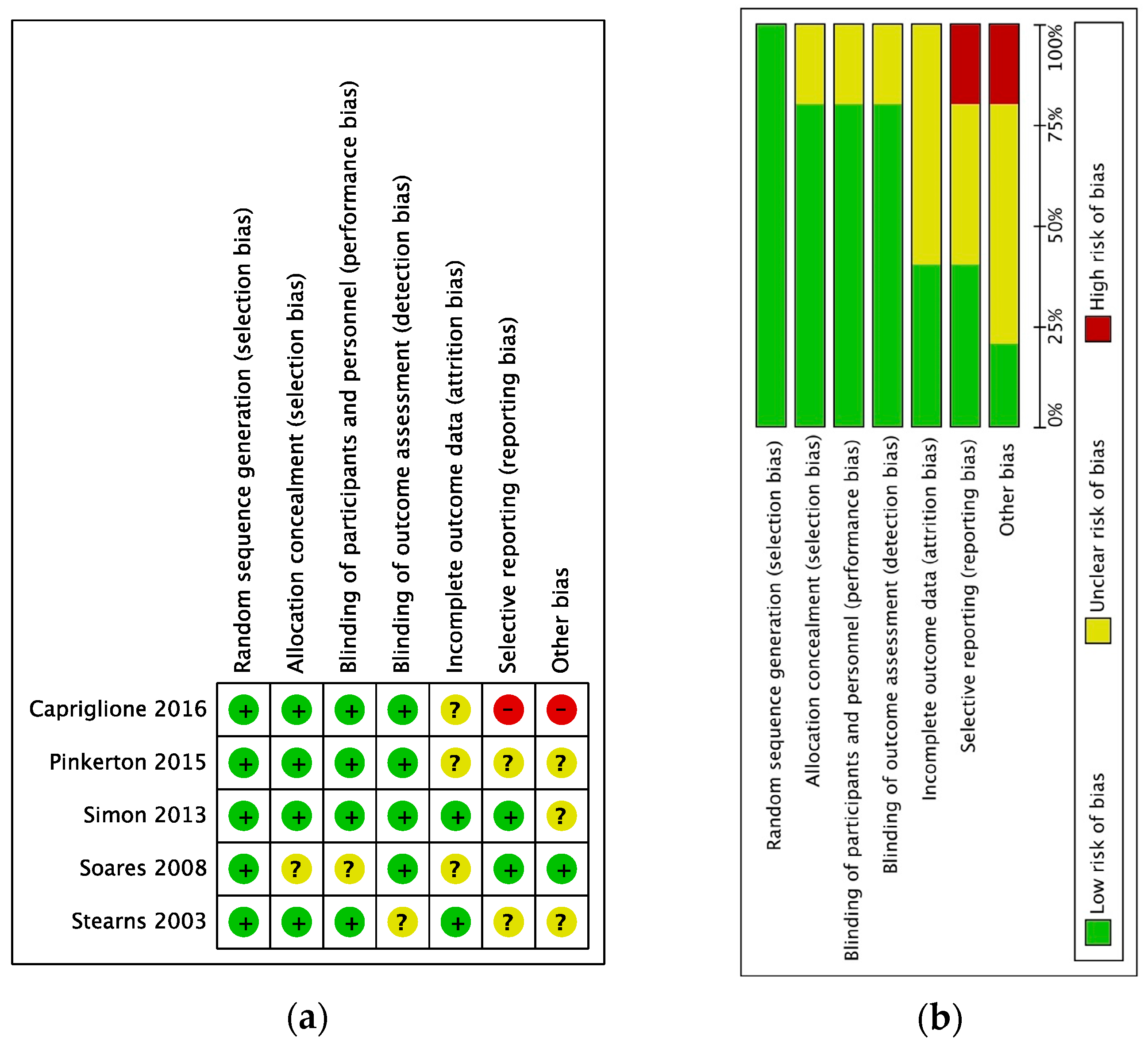
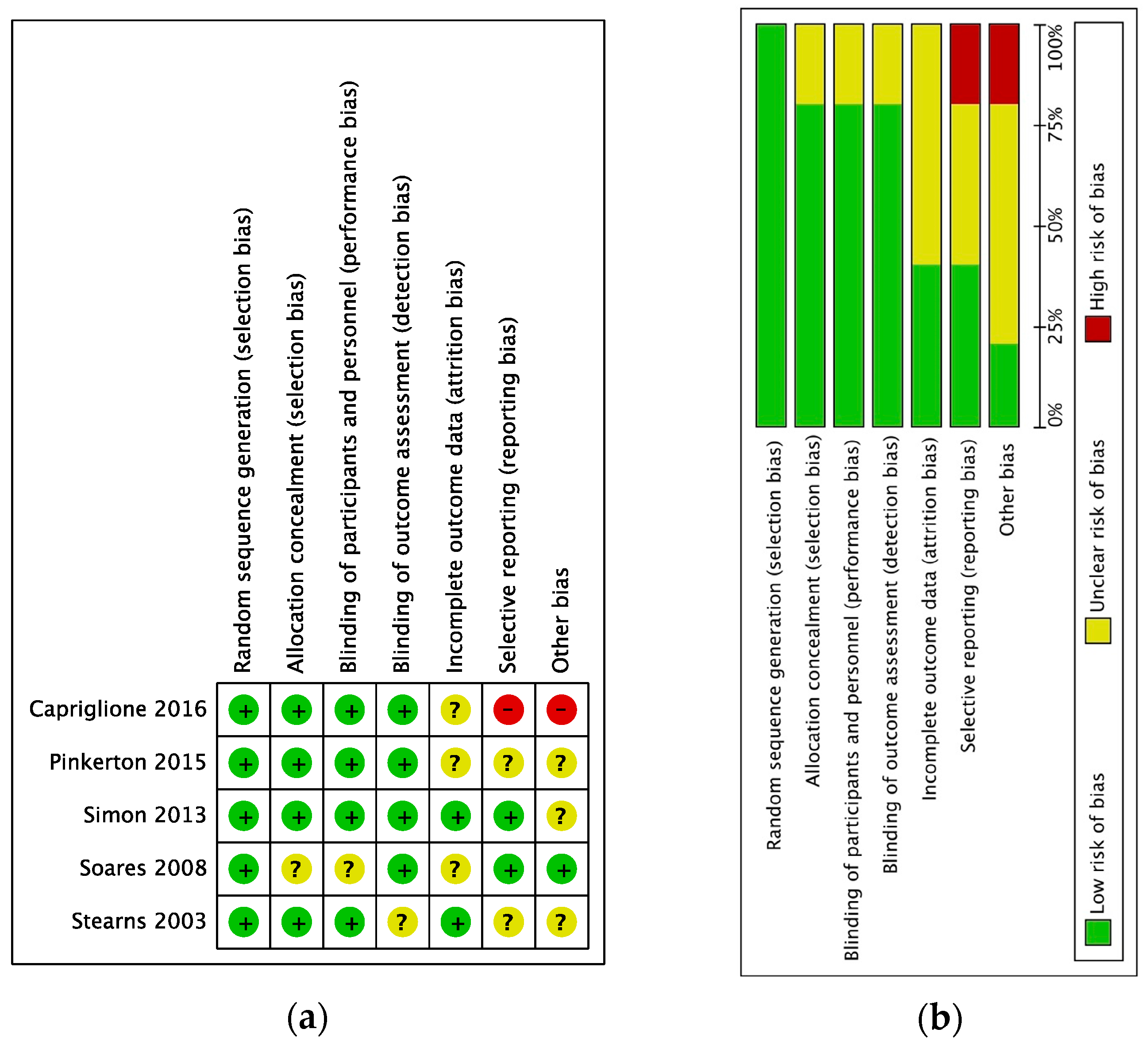
2.2. Study Selection and Risk of Bias
2.3. Outcomes
2.4. Data Analysis
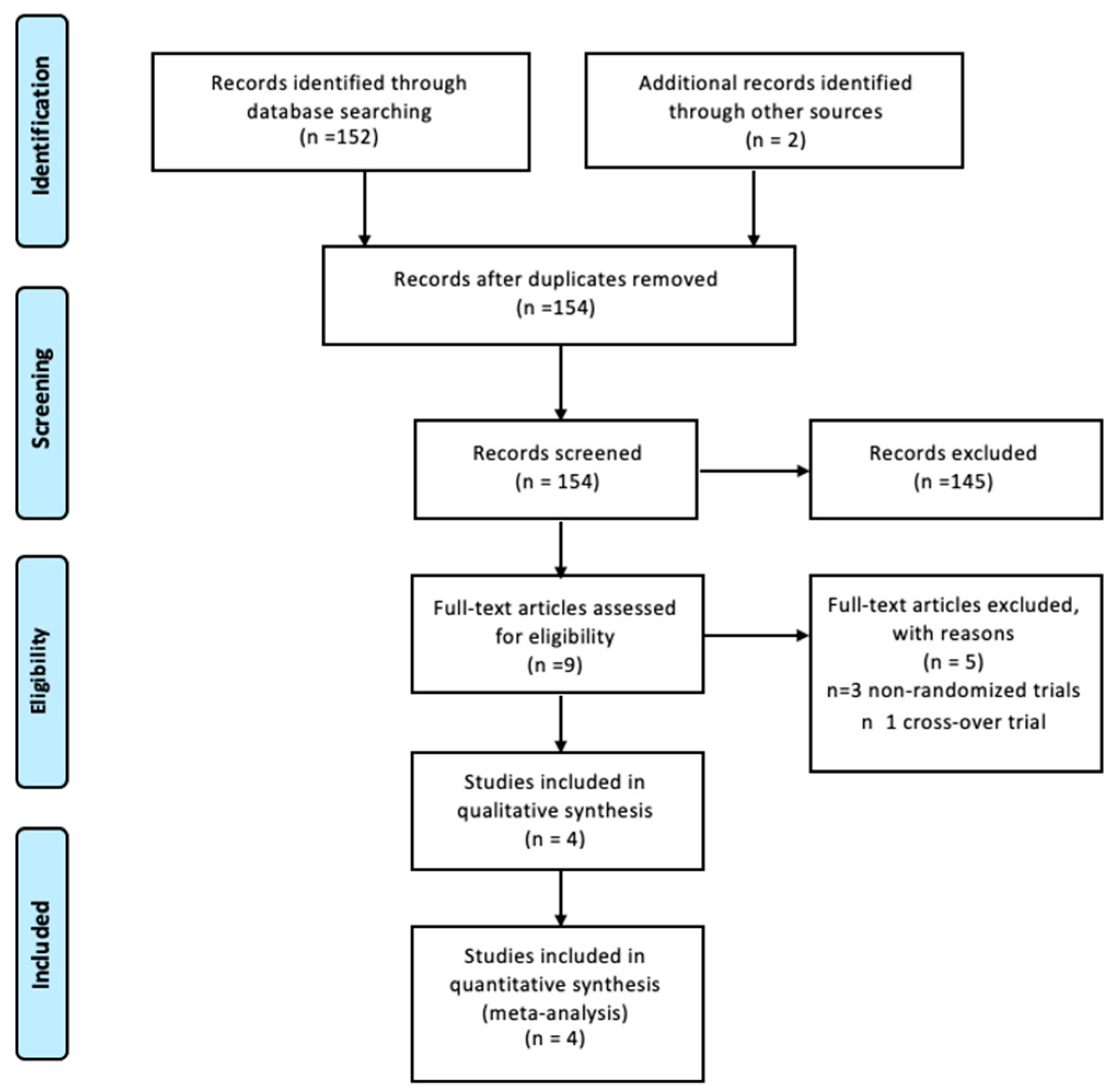
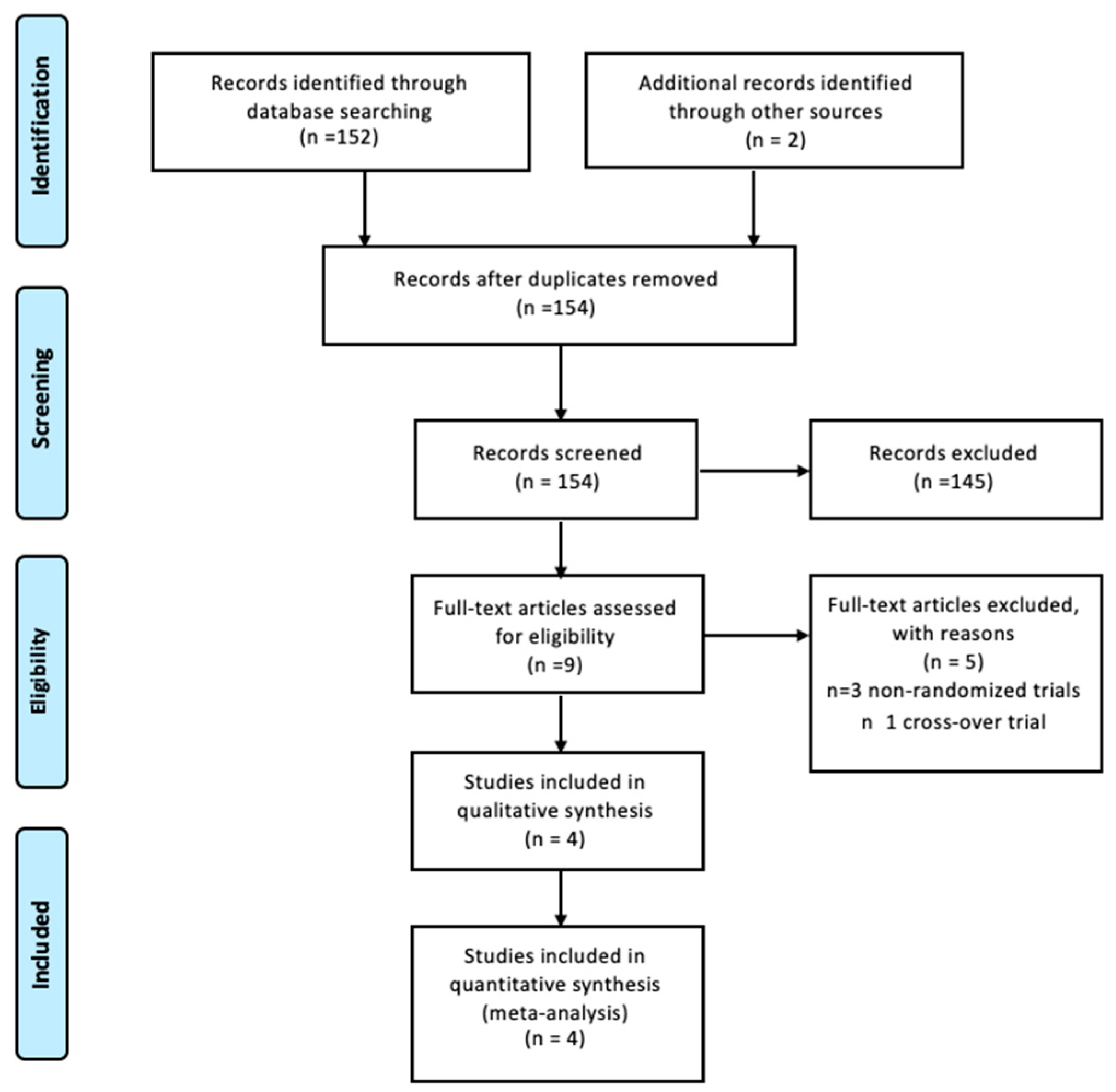
3. Results
3.1. Synthesis of Results
3.2. Heterogeneity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nelson, H.D. Menopause. Lancet 2008, 371, 760–770. [Google Scholar] [CrossRef]
- Santoro, N.; Epperson, C.N.; Mathews, S.B. Menopausal Symptoms and Their Management. Endocrinol. Metab. Clin. 2015, 44, 497–515. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Yim, G.; Park, H.Y. Vasomotor and physical menopausal symptoms are associated with sleep quality. PLoS ONE 2018, 13, e0192934. [Google Scholar] [CrossRef] [PubMed]
- Laganà, A.S.; Vitale, S.G.; Stojanovska, L.; Lambrinoudaki, I.; Apostolopoulos, V.; Chiofalo, B. Preliminary results of a single-arm pilot study to assess the safety and efficacy of visnadine, prenylflavonoids and bovine colostrum in postmenopausal sexually active women affected by vulvovaginal atrophy. Maturitas 2018, 109, 78–80. [Google Scholar] [CrossRef] [PubMed]
- Torella, M.; Del Deo, F.; Grimaldi, A.; Iervolino, S.A.; Pezzella, M.; Tammaro, C.; Gallo, P.; Rappa, C.; De Franciscis, P.; Colacurci, N. Efficacy of an orally administered combination of hyaluronic acid, chondroitin sulfate, curcumin and quercetin for the prevention of recurrent urinary tract infections in postmenopausal women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 207, 125–128. [Google Scholar] [CrossRef]
- Shaver, J.L.; Woods, N.F. Sleep and menopause: A narrative review. Menopause 2015, 22, 899–915. [Google Scholar] [CrossRef] [PubMed]
- Deecher, D.C.; Dorries, K. Understanding the pathophysiology of vasomotor symptoms (hot flushes and night sweats) that occur in perimenopause, menopause, and postmenopause life stages. Arch. Womens Ment. Health 2007, 10, 247–257. [Google Scholar] [CrossRef]
- Krause, M.S.; Nakajima, S.T. Hormonal and nonhormonal treatment of vasomotor symptoms. Obstet. Gynecol. Clin. 2015, 42, 163–179. [Google Scholar] [CrossRef]
- Chang, H.Y.; Jotwani, A.C.; Lai, Y.H.; Jensen, M.P.; Syrjala, K.L.; Fann, J.R.; Gralow, J. Hot flashes in breast cancer survivors: Frequency, severity and impact. Breast 2016, 27, 116–121. [Google Scholar] [CrossRef] [Green Version]
- De Franciscis, P.; Cobellis, L.; Fornaro, F.; Sepe, E.; Torella, M.; Colacurci, N. Low-dose hormone therapy in the perimenopause. Int. J. Gynaecol. Obstet. 2007, 98, 138–142. [Google Scholar] [CrossRef]
- Laganà, A.S.; La Rosa, V.L.; Rapisarda, A.M.C.; Valenti, G.; Sapia, F.; Chiofalo, B.; Rossetti, D.; Ban Frangež, H.; Vrtačnik Bokal, E.; Vitale, S.G. Anxiety and depression in patients with endometriosis: Impact and management challenges. Int. J. Womens Health 2017, 9, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Purgato, M.; Papola, D.; Gastaldon, C.; Trespidi, C.; Magni, L.R.; Rizzo, C.; Furukawa, T.A.; Watanabe, N.; Cipriani, A.; Barbui, C. Paroxetine versus other anti-depressive agents for depression. Cochrane Database Syst. Rev. 2014, 3, CD006531. [Google Scholar] [CrossRef] [PubMed]
- Bourin, M.; Chue, P.; Guillon, Y. Paroxetine: A review. CNS Drug Rev. 2001, 7, 25–47. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, C.; Mattingly, L.; Crawford, S.A.; Wickersham, E.A.; Brockhaus, J.L.; McCarthy, L.H. Do SSRIs and SNRIs reduce the frequency and/or severity of hot flashes in menopausal women. J. Okla. State Med. Assoc. 2017, 110, 272–274. [Google Scholar] [PubMed]
- Simon, J.A.; Chandler, J.; Gottesdiener, K.; Lazarus, N.; He, W.; Rosenberg, E.; Wagner, J.A.; Denker, A.E. Diary of hot flashes reported upon occurrence: Results of a randomized double-blind study of raloxifene, placebo, and paroxetine. Menopause 2014, 21, 938–944. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Stearns, V.; Beebe, K.L.; Iyengar, M.; Dube, E. Paroxetine controlled release in the treatment of menopausal hot flashes: A randomized controlled trial. JAMA 2003, 289, 2827–2834. [Google Scholar] [CrossRef]
- Soares, C.N.; Joffe, H.; Viguera, A.C.; Petrillo, L.; Rydzewski, M.; Yehezkel, R.; Somley, B.; Cohen, L.S. Paroxetine versus placebo for women in midlife after hormone therapy discontinuation. Am. J. Med. 2008, 121, 159–162. [Google Scholar] [CrossRef]
- Simon, J.A.; Portman, D.J.; Kaunitz, A.M.; Mekonnen, H.; Kazempour, K.; Bhaskar, S.; Lippman, J. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: Two randomized controlled trials. Menopause 2013, 20, 1027–1035. [Google Scholar] [CrossRef]
- Portman, D.J.; Kaunitz, A.M.; Kazempour, K.; Mekonnen, H.; Bhaskar, S.; Lippman, J. Effects of low-dose paroxetine 7.5 mg on weight and sexual function during treatment of vasomotor symptoms associated with menopause. Menopause 2014, 21, 1082–1090. [Google Scholar] [CrossRef] [Green Version]
- Capriglione, S.; Plotti, F.; Montera, R.; Luvero, D.; Lopez, S.; Scaletta, G.; Aloisi, A.; Serra, G.B.; Angioli, R. Role of paroxetine in the management of hot flashes in gynecological cancer survivors: Results of the first randomized single-center controlled trial. Gynecol. Oncol. 2016, 143, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Stearns, V.; Slack, R.; Greep, N.; Henry-Tilman, R.; Osborne, M.; Bunnell, C.; Ullmer, L.; Gallagher, A.; Cullen, J.; Gehan, E.; et al. Paroxetine is an effective treatment for hot flashes: Results from a prospective randomized clinical trial. J. Clin. Oncol. 2005, 23, 6919–6930. [Google Scholar] [CrossRef]
- Pinkerton, J.V.; Joffe, H.; Kazempour, K.; Mekonnen, H.; Bhaskar, S.; Lippman, J. Low-dose paroxetine (7.5 mg) improves sleep in women with vasomotor symptoms associated with menopause. Menopause 2015, 22, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weitzner, M.A.; Moncello, J.; Jacobsen, P.B.; Minton, S. A pilot trial of paroxetine for the treatment of hot flashes and associated symptoms in women with breast cancer. J. Pain Symptom Manag. 2002, 23, 337–345. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Intervention; John Wiley & Sons: New York, NY, USA, 2011. [Google Scholar]
- Mirkin, S.; Archer, D.F.; Pickar, J.H.; Komm, B.S. Recent advances help understand and improve the safety of menopausal therapies. Menopause 2015, 22, 351–360. [Google Scholar] [CrossRef]
- Carpenter, J.; Gass, M.L.; Maki, P.M.; Newton, K.M.; Pinkerton, J.V.; Taylor, M.; Shifren, J.L. Nonhormonal management of menopause-associated vasomotor symptoms: 2015 position statement of The North American Menopause Society. Menopause 2015, 22, 1155–1172. [Google Scholar]
- Laganà, A.S.; Condemi, I.; Retto, G.; Muscatello, M.R.; Bruno, A.; Zoccali, R.A.; Triolo, O.; Cedro, C. Analysis of psychopathological comorbidity behind the common symptoms and signs of endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 194, 30–33. [Google Scholar] [CrossRef]
- Vitale, S.G.; Laganà, A.S.; Muscatello, M.R.; La Rosa, V.L.; Currò, V.; Pandolfo, G.; Zoccali, R.A.; Bruno, A. Psychopharmacotherapy in Pregnancy and Breastfeeding. Obstet. GynecolSurv. 2016, 71, 721–733. [Google Scholar] [CrossRef]
- Rizzo, M.R.; Leo, S.; De Franciscis, P.; Colacurci, N.; Paolisso, G. Short-term effects of low-dose estrogen/drospirenone vs low-dose estrogen/dydrogesterone on glycemic fluctuations in postmenopausal women with metabolic syndrome. Age 2014, 36, 265–274. [Google Scholar] [CrossRef]
- Slaton, R.M.; Champion, M.N.; Palmore, K.B. A review of paroxetine for the treatment of vasomotor symptoms. J. Pharm. Pract. 2015, 28, 266–274. [Google Scholar] [CrossRef]
- Wei, D.; Chen, Y.; Wu, C.; Wu, Q.; Yao, L.; Wang, Q.; Wang, X.Q.; Yang, K.H. Effect and safety of paroxetine for vasomotor symptoms: Systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 1735–1743. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stearns 2003 [17] | Simon 2013 [19]; Pinkerton 2014 [23] | Capriglione 2016 [21] | |
|---|---|---|---|
| Location | USA | USA | Italy |
| Sample size n. (Treatment/Placebo) | 228 (111/117) | 1174 (585/589) | 80(42/38) |
| Treatment administered | Paroxetine 12.5 mg/day for 6 weeks | Paroxetine 7.5 mg/day for 12 weeks | Paroxetine 7.5 mg/day for 16 weeks |
| Inclusion criteria | Physiologic postmenopausal women with hot flushes and sleep disturbances | Physiologic or surgical postmenopausal women with hot flushes and sleep disturbances | Surgical postmenopausal women with hot flushes and sleep disturbances |
| Mean Age (SD): Treatment Placebo | 56.3 | 54.6 (5.73) | 53.5 (5.71) |
| 56.3 | 54.5 (6.01) | 53.6 (5.01) | |
| Mean BMI (SD): Treatment Placebo | Not available | 28.62 (5.73) | 26.7 (4.62) |
| 29.03 (5.51) | 27.5 (4.71) | ||
| Follow-up | 6 weeks | 12 weeks | 16 weeks |
| Outcomes | Hot flushes reduction; sleep disturbance | Hot flushes reduction; sleep disturbance | Hot flushes reduction; sleep disturbance |
| + | Stearns 2003 [17] | Simon 2013 [19] | Pinkerton 2014 [23] | Capriglione 2016 [21] | I2 | Mean Difference (MD) and 95% CI | |
|---|---|---|---|---|---|---|---|
| Hot flushes reduction (mean weekly reduction) | Paroxetine | −23.1 ± 5.3 | −43.5 ± 12.1 | Not available | −46.5 ± 3.2 | 93% | −7.97 [−10.51, −5.42] |
| Placebo | −12.6 ± 5.4 | −37.3 ± 12.1 | −39.3 ± 3.1 | ||||
| Sleep interference reduction (mean nighttime awakenings reduction) | Paroxetine | Not applicable | Not available | −1.98 ± 1.21 | −1.39 ± 0.32 | 0% | −0.40 [−1.38, 0.58] |
| Placebo | −1.56 ± 1.21 | −1.01 ± 0.31 | |||||
| Population | Outcome | Included Studies | Total | I2 | MD (95% CI) |
|---|---|---|---|---|---|
| Physiological postmenopausal | Hot flushes reduction | Simon 2013, Stearns 2003 | 615/701 (87.7%) vs. 641/720 (89.0%) | 65% | −7.89 [−11.23, −4.81] |
| Surgical postmenopausal | Hot flushes reduction | Capriglione 2016, Simon 2013, | 110/766 (14.3%) vs. 100/760 (13.1%) | 55% | −7.63 [−10.15; −5.56] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riemma, G.; Schiattarella, A.; La Verde, M.; Zarobbi, G.; Garzon, S.; Cucinella, G.; Calagna, G.; Labriola, D.; De Franciscis, P. Efficacy of Low-Dose Paroxetine for the Treatment of Hot Flushes in Surgical and Physiological Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Trials. Medicina 2019, 55, 554. https://doi.org/10.3390/medicina55090554
Riemma G, Schiattarella A, La Verde M, Zarobbi G, Garzon S, Cucinella G, Calagna G, Labriola D, De Franciscis P. Efficacy of Low-Dose Paroxetine for the Treatment of Hot Flushes in Surgical and Physiological Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Trials. Medicina. 2019; 55(9):554. https://doi.org/10.3390/medicina55090554
Chicago/Turabian StyleRiemma, Gaetano, Antonio Schiattarella, Marco La Verde, Giuseppina Zarobbi, Simone Garzon, Gaspare Cucinella, Gloria Calagna, Domenico Labriola, and Pasquale De Franciscis. 2019. "Efficacy of Low-Dose Paroxetine for the Treatment of Hot Flushes in Surgical and Physiological Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Trials" Medicina 55, no. 9: 554. https://doi.org/10.3390/medicina55090554
APA StyleRiemma, G., Schiattarella, A., La Verde, M., Zarobbi, G., Garzon, S., Cucinella, G., Calagna, G., Labriola, D., & De Franciscis, P. (2019). Efficacy of Low-Dose Paroxetine for the Treatment of Hot Flushes in Surgical and Physiological Postmenopausal Women: Systematic Review and Meta-Analysis of Randomized Trials. Medicina, 55(9), 554. https://doi.org/10.3390/medicina55090554