Long-Term Relationship between Psychological Distress and Continuous Sedentary Behavior in Healthy Older Adults: A Three Panel Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Clinical Parameters and Measurement
2.4. Psychological Distress
2.5. Physical Activity
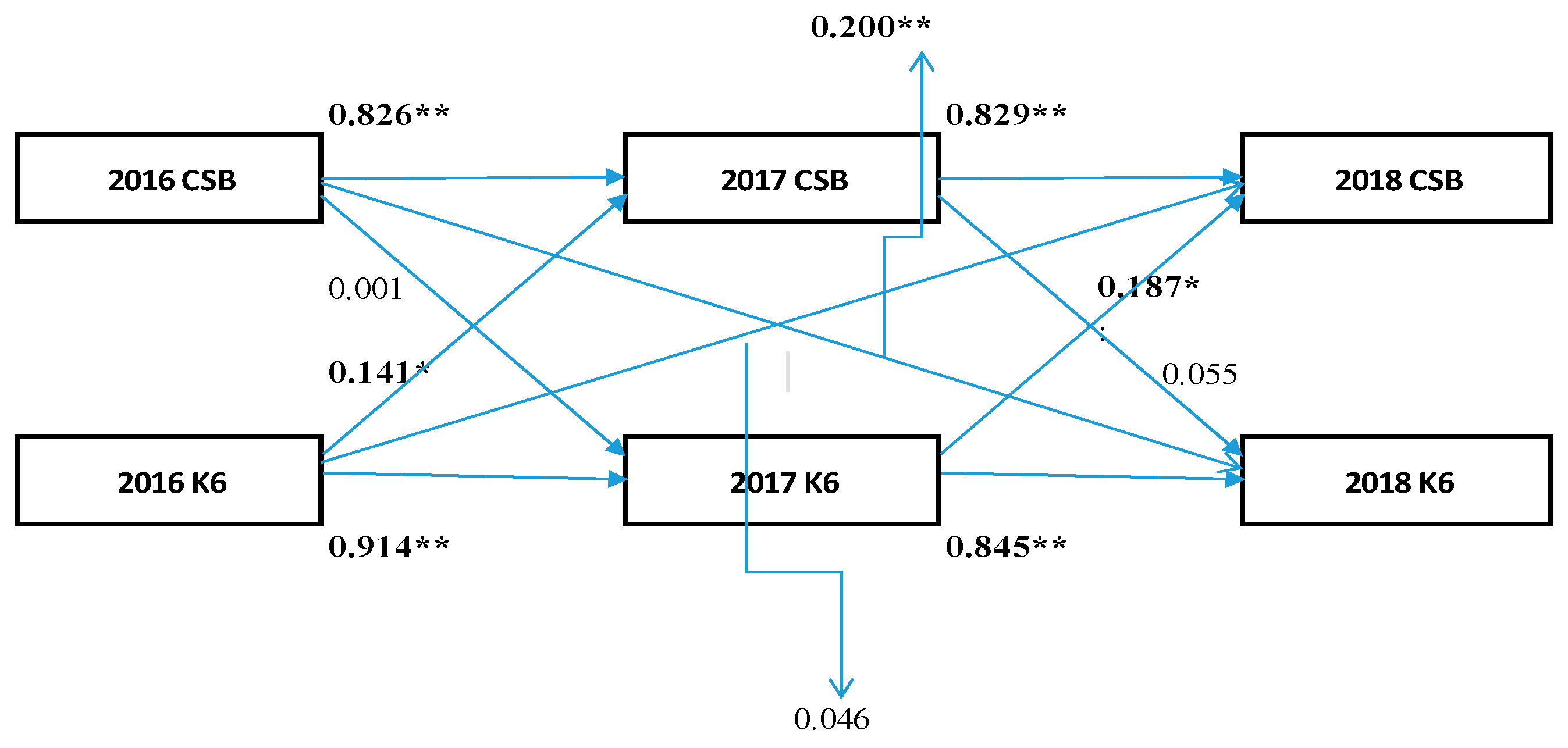
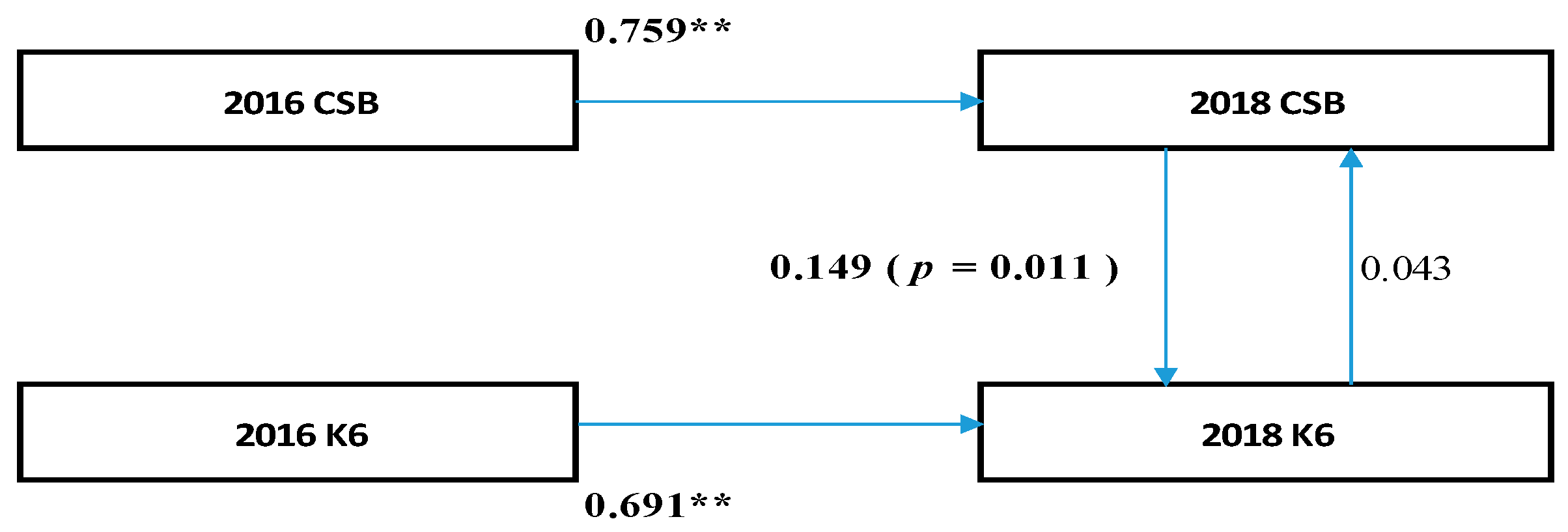
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Adrian, B.; Barbara, E.A.; James, F.S.; Maria, H.; Cora, L.C.; Fiona, C.B.; Michael, P.; Kamalesh, V.; Josephine, C.; Michael, S.B. The Descriptive Epidemiology of Sitting A 20-Country Comparison Using the International Physical Activity Questionnaire (IPAQ). Am. J. Prev. Med. 2011, 41, 228–235. [Google Scholar]
- Juliet, A.H.; Chastin, S.; Skelton, D. Prevalence of sedentary behavior in older adults: A systematic review. Int. J. Environ. Res. Public Health 2013, 10, 6645–6661. [Google Scholar]
- Healy, G.N.; Clark, B.K.; Winkler, E.A.; Gardiner, P.A.; Brown, W.J.; Matthews, C.E. Measurement of adult’ sedentary time in population-based studies. Am. J. Prev. Med. 2011, 41, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary behaviors and subsequent health outcomes: A systematic review of longitudinal studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Sedentary Behavior Research Network. Standardized use of the terms “sedentary” and “sedentary behaviors”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef]
- Buman, M.; Hekler, E.; Haskell, W.; Pruitt, L.; Conway, T.; Cain, K.; King, A. Objective Light-Intensity Physical Activity Associations with Rated Health in Older Adults. Am. J. Epidemiol. 2010, 172, 1155–1165. [Google Scholar] [CrossRef]
- Balboa-Castillo, T.; León-Muñoz, L.M.; Graciani, A.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Longitudinal association of physical activity and sedentary behavior during leisure time with health-related quality of life in community-dwelling older adults. Health Qual. Life Outcomes 2011, 9, 47. [Google Scholar] [CrossRef]
- De Rezende, L.F.; Rodrigues, L.M.; Rey-López, J.P.; Matsudo, V.K.; Luiz, O.C. Sedentary Behavior and Health Outcomes: An Overview of Systematic Reviews. PLoS ONE 2014, 9, e105620. [Google Scholar] [CrossRef]
- Cabinet Office, Government of Japan. 2018. Available online: http://www8.cao.go.jp/kourei/whitepaper/w-2018/zenbun/pdf/1s1s_01.pdf (accessed on 25 June 2019).
- Dunstan, D.W.; Howard, B.; Healy, G.N.; Owen, N. Too much sitting—A health hazard. Diabet. Res. Clin. Pract. 2012, 97, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Honda, T.; Chen, S.; Yonemoto, K.; Kishimoto, H.; Chen, T.; Narazaki, K.; Haeuchi, Y.; Kumagai, S. Sedentary bout durations and metabolic syndrome among working adults: A prospective cohort study. BMC Public Health 2016, 16, 888. [Google Scholar] [CrossRef]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Alkhajah, T.A.; Reeves, M.M.; Eakin, E.G.; Winkler, E.A.; Owen, N.; Healy, G.N. Sit-stand workstations: A pilot intervention to reduce office sitting time. Am. J. Prev. Med. 2012, 43, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Pronk, N.P.; Katz, A.S.; Lowry, M.; Payfer, J.R. Reducing occupational sitting time and improving worker health: The Take-a-Stand Project, 2011. Prev. Chron. Dis. 2012, 9, E154. [Google Scholar] [CrossRef]
- Meneguci, J.; Sasaki, J.E.; Santos, A.; Scatena, L.M.; Damião, R. Sitting Time and Quality of Life in Older Adults: A Population-Based Study. J. Phys. Act. Health 2015, 12, 1513–1519. [Google Scholar] [CrossRef] [PubMed]
- Ku, P.W.; Fox, K.R.; Liao, Y.; Sun, W.J.; Chen, L.J. Prospective associations of objectively assessed physical activity at different intensities with subjective well-being in older adults. Qual. Life Res. 2016, 25, 2909–2919. [Google Scholar] [CrossRef]
- Sardinha, L.B.; Santos, D.A.; Silva, A.M.; Baptista, F.; Owen, N. Breaking-up sedentary time is associated with physical function in older adults. J. Gerontol. A 2015, 1, 119–124. [Google Scholar] [CrossRef]
- Healy, G.N.; Matthews, C.E.; Dunstan, D.W.; Winkler, E.A.; Owen, N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003-06. Eur. Heart J. 2011, 32, 590–597. [Google Scholar] [CrossRef]
- Granger, C.W.J. Investigating causal relation by econometric models and cross-spectral methods. Ecomometrica 1969, 37, 424–438. [Google Scholar] [CrossRef]
- Owari, Y.; Miyatake, N.; Kataoka, H. Relationship between Psychological Distress, Social Participation and Physical Activities in Apparently Healthy Elderly People. Acta Med. Okayama 2018, 72, 31–37. [Google Scholar] [PubMed]
- Owari, Y.; Miyatake, N.; Suzuki, H. “Active Guide” Brochure Reduces Sedentary Behavior of Elderly People: A Randomized Controlled Trial. Acta Med. Okayama 2019, in press. [Google Scholar]
- Owari, Y.; Miyatake, N. Relationship between psychological distress and continuous sedentary behaviour in healthy older adults. Medicina 2019, 55, 324. [Google Scholar] [CrossRef] [PubMed]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Meth. (BJBRM) 2008, 6, 53–60. [Google Scholar]
- McArdle, J.J. Dynamic but Structural Equation Modeling of Repeated Measures Data. In The Handbook of Multivariate Experimental Psychology; Nesselroade, J.R., Cattell, R.B., Eds.; Plenum Press: New York, NY, USA, 1988; Volume 2, pp. 561–614. [Google Scholar]
- Finkel, S.E. Causal Analysis with Panel Data, Quantitative Applications in the Social Sciences; Sage: Thousand Oaks, CA, USA, 1995. [Google Scholar]
- Blumenthal, J.A.; Babyak, M.A.; Moore, K.A.; Craighead, W.E.; Herman, S.; Khatri, P.; Waugh, R.; Napolitano, M.A.; Forman, L.M.; Appelbaum, M.; et al. Effects of exercise training on older patients with major depression. Arch. Intern. Med. 1999, 159, 2349–2356. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, J.-A.H.; Brar, J.S.; Rush, E.B.; Jolley, C.J. Physical activity and depressive symptoms in older adults. Geriatr. Nurs. 2014, 35, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Strawbridge, W.J.; Deleger, S.; Roberts, R.E.; Kaplan, G.A. Physical activity reduce the risk of subsequent depression for older adults. Am. J. Epidemiol. 2002, 156, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Hamilton, D.G.; Theodore; Zderic, T.W. Exercise Physiology versus Inactivity Physiology: An Essential Concept for Understanding Lipoprotein Lipase Regulation. Exerc. Sport Sci. Rev. 2004, 32, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef]
- Hamer, M.; Coombs, N.; Stamatakis, E. Associations between objectively assessed and self-reported sedentary time with mental health in adults: An analysis of data from the Health Survey for England. BMJ Open 2014, 4, e004580. [Google Scholar] [CrossRef]
- Barnett, A.G.; van der Pols, J.C.; Dobson, A.J. Regression to the mean: What it is and how to deal with it. Int. J. Epidemiol. 2005, 34, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Dawn, I. Structural equations modeling: Fit indices, sample size and advanced topics. J. Consum. Psychol. 2010, 20, 90–98. [Google Scholar]



{kind=link}
{kind=link}
| 2016 | 2017 | 2018 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | Minimum | Maximum | Mean | ± | SD | Minimum | Maximum | Mean | ± | SD | Minimum | Maximum | |
| Number of subjects | 72 (men = 23) | ||||||||||||||
| Age (year) | 72.6 | ± | 5.4 | 65 | 85 | ||||||||||
| Height (cm) | 157.2 | ± | 9.1 | 138.3 | 178.4 | 157.1 | ± | 9.1 | 138.1 | 178.2 | 157.1 | ± | 9.0 | 138.0 | 178.2 |
| Body weight (kg) | 55.8 | ± | 10.0 | 40.3 | 83.1 | 56.0 | ± | 9.7 | 40.5 | 83.3 | 56.1 | ± | 10.1 | 40.2 | 83.6 |
| BMI (kg/m2) | 22.9 | ± | 2.4 | 13.9 | 29.1 | 23.1 | ± | 2.6 | 14.9 | 29.2 | 23.6 | ± | 2.6 | 15.1 | 29.2 |
| ≤1.5 Mets (%/day) | 55.1 | ± | 9.7 | 35.4 | 79.9 | 55.5 | ± | 10.9 | 20.9 | 75.4 | 55.7 | ± | 11.0 | 30.8 | 86.6 |
| CSB:Interrupted of sedentary behavior (%) | 14.7 | ± | 8.5 | 0.0 | 40.8 | 15.8 | ± | 9.5 | 0.0 | 45.4 | 15.1 | ± | 7.9 | 0.0 | 39.8 |
| K6 scores | 2.5 | ± | 3.1 | 0 | 14 | 2.7 | ± | 3.2 | 0 | 14 | 2.5 | ± | 2.3 | 0 | 11 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owari, Y.; Miyatake, N. Long-Term Relationship between Psychological Distress and Continuous Sedentary Behavior in Healthy Older Adults: A Three Panel Study. Medicina 2019, 55, 555. https://doi.org/10.3390/medicina55090555
Owari Y, Miyatake N. Long-Term Relationship between Psychological Distress and Continuous Sedentary Behavior in Healthy Older Adults: A Three Panel Study. Medicina. 2019; 55(9):555. https://doi.org/10.3390/medicina55090555
Chicago/Turabian StyleOwari, Yutaka, and Nobuyuki Miyatake. 2019. "Long-Term Relationship between Psychological Distress and Continuous Sedentary Behavior in Healthy Older Adults: A Three Panel Study" Medicina 55, no. 9: 555. https://doi.org/10.3390/medicina55090555
APA StyleOwari, Y., & Miyatake, N. (2019). Long-Term Relationship between Psychological Distress and Continuous Sedentary Behavior in Healthy Older Adults: A Three Panel Study. Medicina, 55(9), 555. https://doi.org/10.3390/medicina55090555