Antimicrobial Capacity and Surface Alterations Using Photodynamic Therapy and Light Activated Disinfection on Polymer-Infiltrated Ceramic Material Contaminated with Periodontal Bacteria

 ,
,
Abstract
:
1. Introduction
2. Results
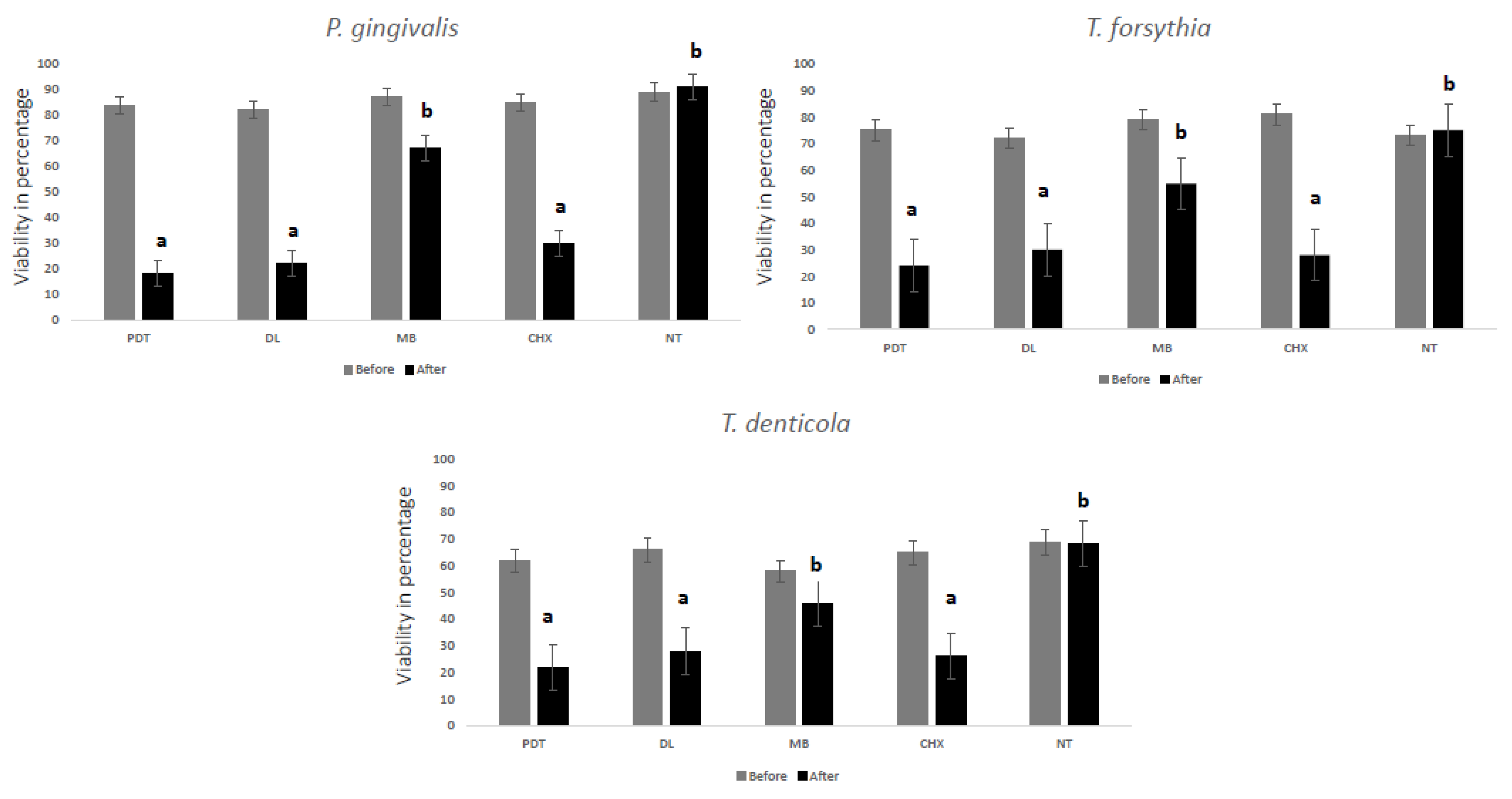
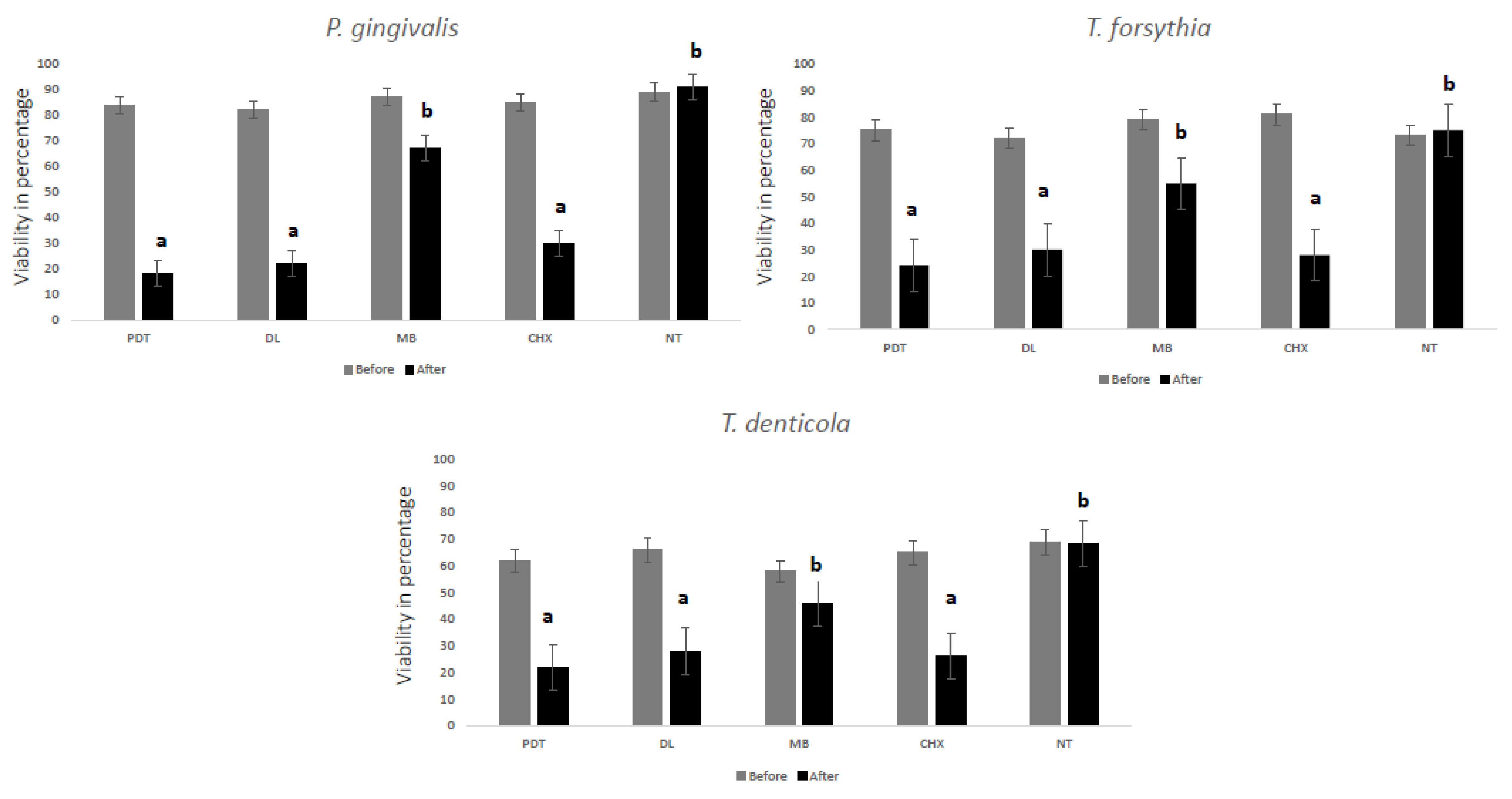
2.1. Antibacterial Testing
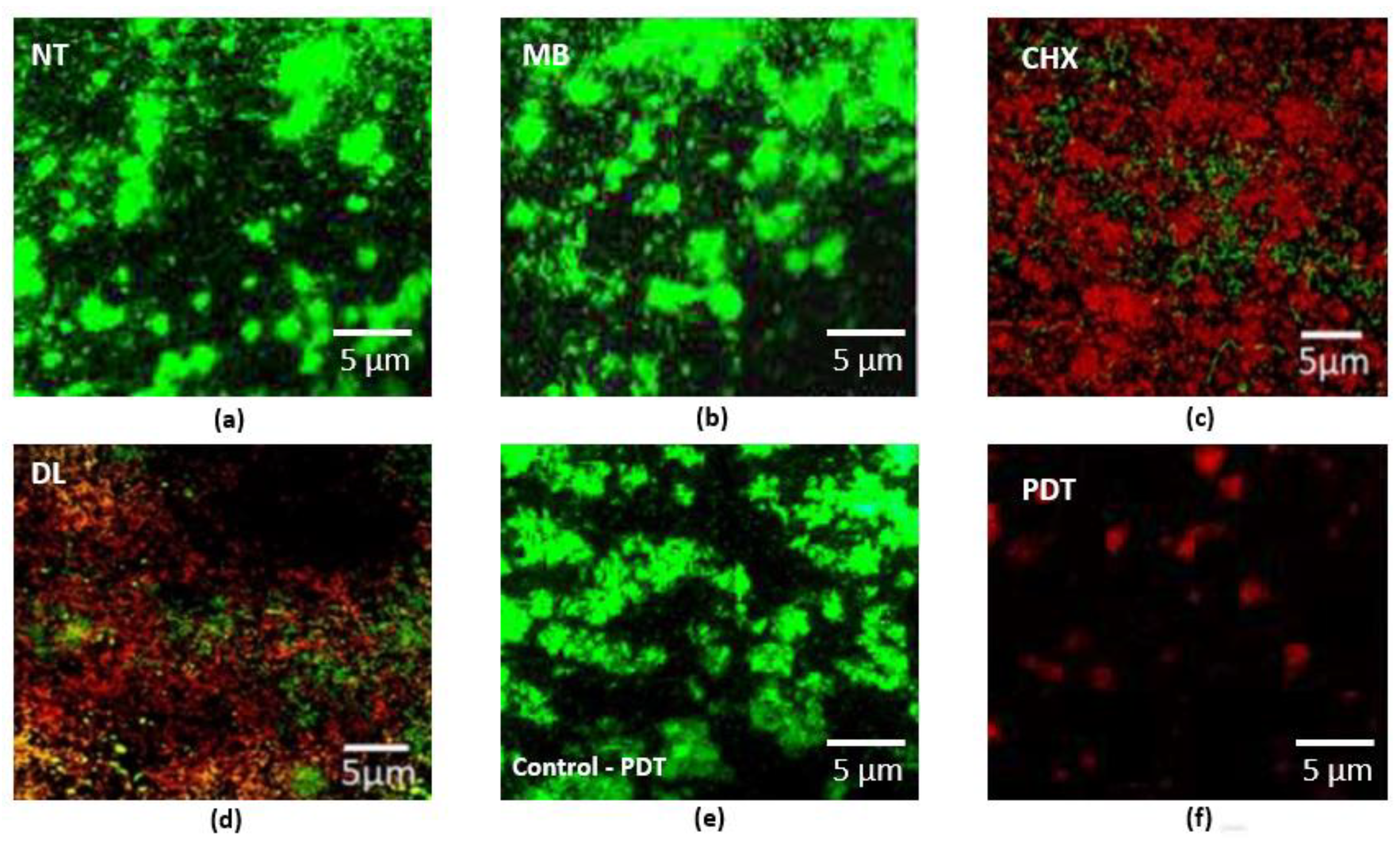
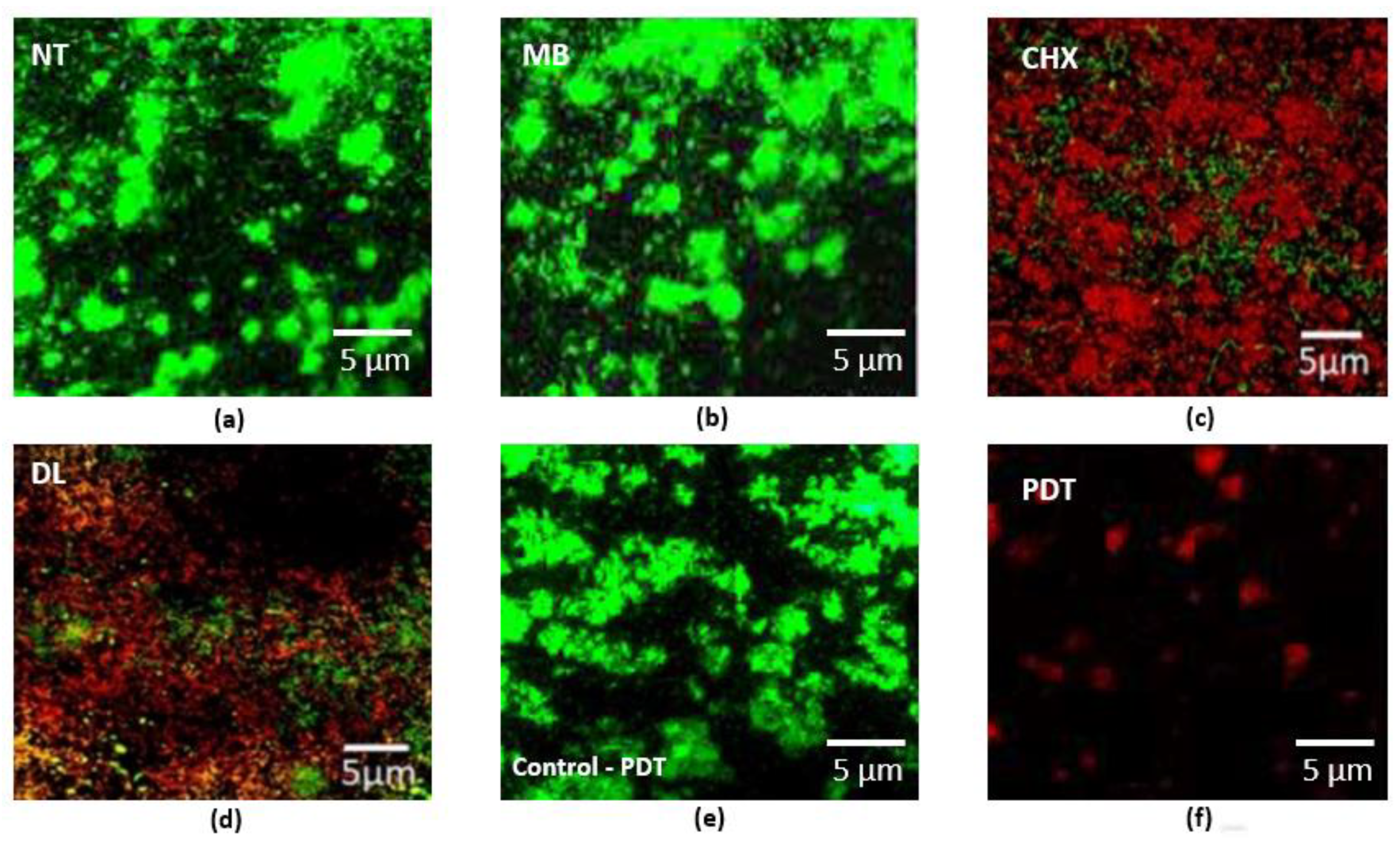
2.2. Live/Dead Assay
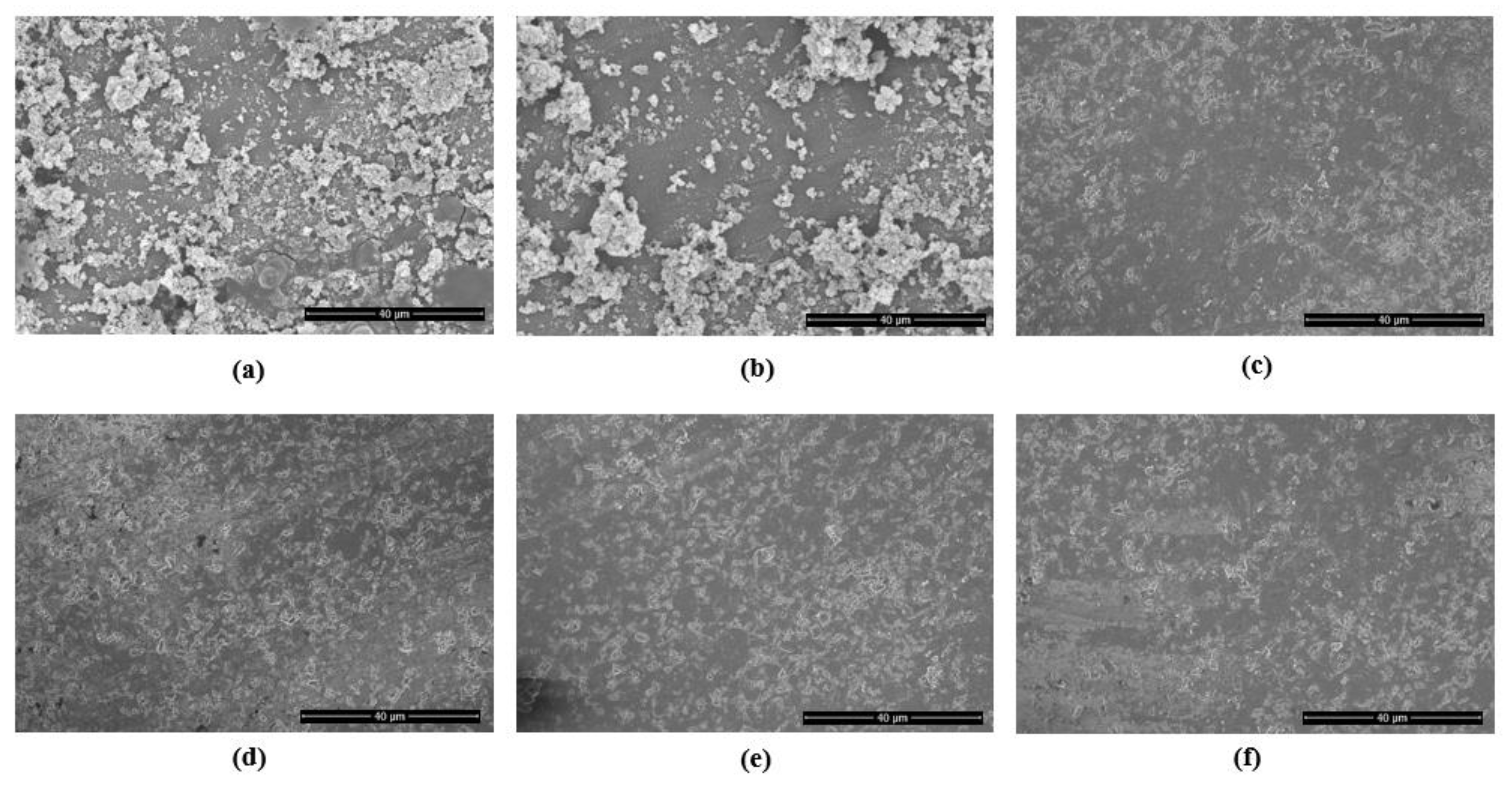
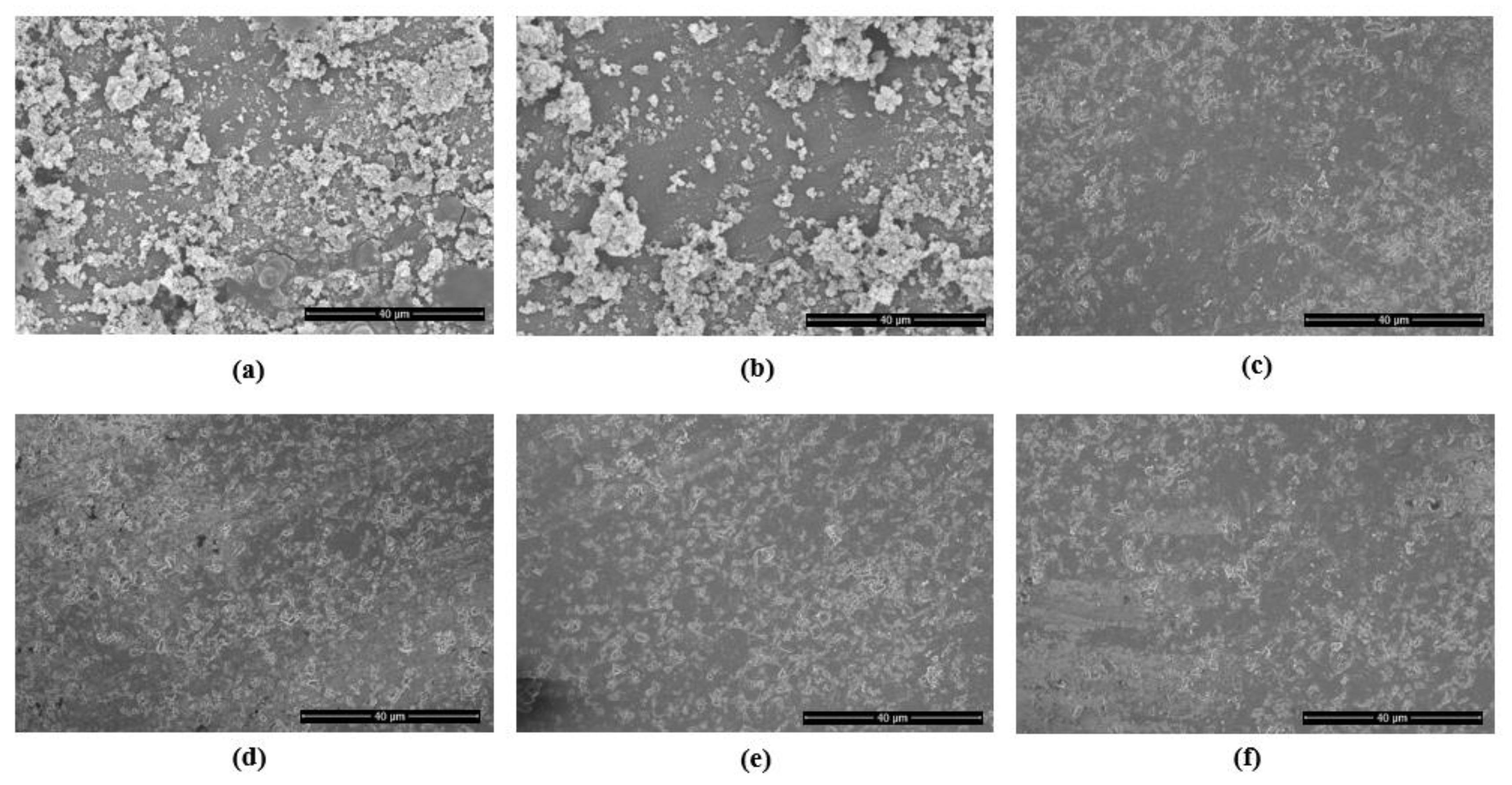
2.3. Surface Characterization
3. Discussion
4. Materials and Methods
4.1. Study Ethics and Samples
4.2. Microbial Contamination of the PICN Discs
4.3. Therapies
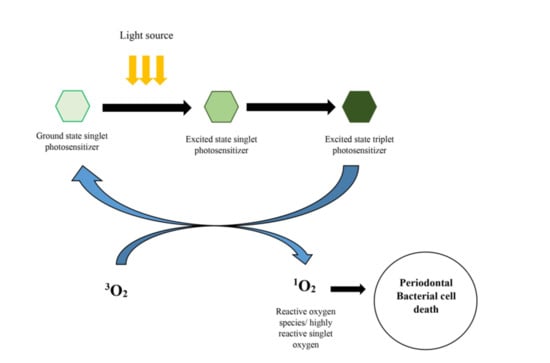
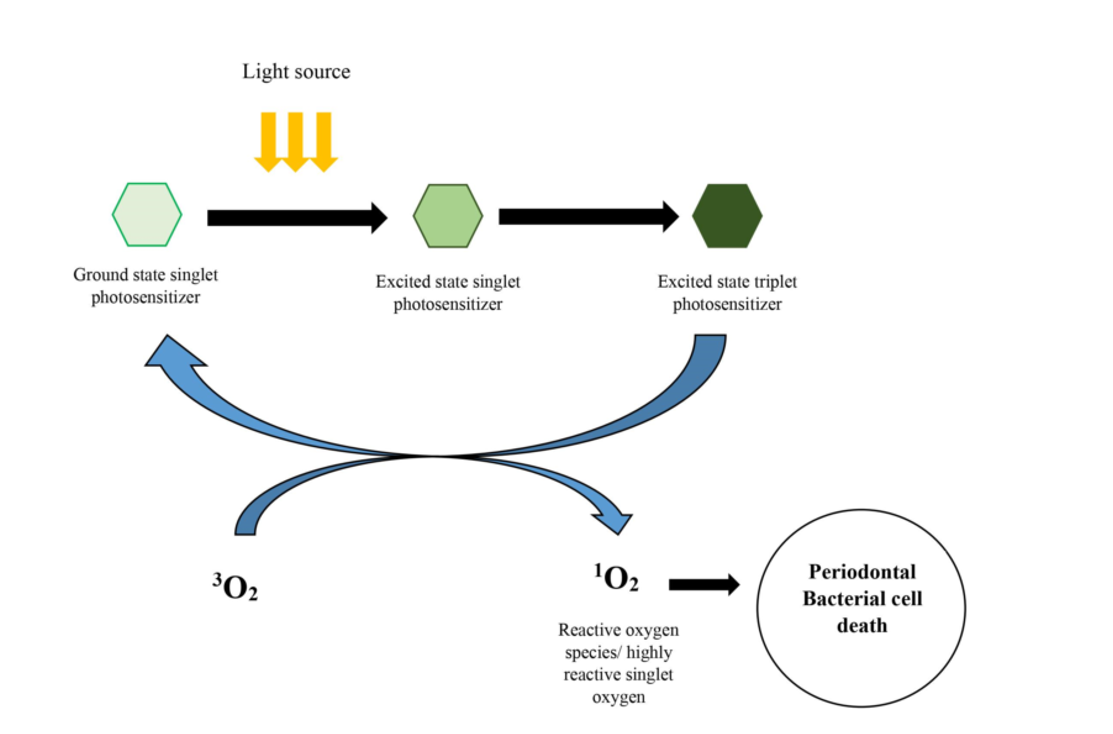
4.3.1. Photodynamic Therapy Group (PDT)
4.3.2. Diode Laser Group (DL)
4.3.3. Methylene Blue Group (MB)
4.3.4. Chlorhexidine Group (CHX)
4.3.5. No Treatment (NT)
4.4. Microbial Analysis
4.5. Confocal Laser Microscopy
4.6. Scanning Electron Microscopy
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Marcum, J.S. The effect of crown marginal depth upon gingival tissue. J. Prosthet. Dent. 1967, 17, 479–487. [Google Scholar] [CrossRef]
- Kancyper, S.G.; Koka, S. The influence of intracrevicular crown margins on gingival health: Preliminary findings. J. Prosthet. Dent. 2001, 85, 461–465. [Google Scholar] [CrossRef]
- Passariello, C.; Puttini, M.; Virga, A.; Gigola, P. Microbiological and host factors are involved in promoting the periodontal failure of metaloceramic crowns. Clin. Oral Investig. 2012, 16, 987–995. [Google Scholar] [PubMed]
- Goldberg, P.V.; Higginbottom, F.L.; Wilson, T.G., Jr. Periodontal considerations in restorative and implant therapy. Periodontology 2000 2001, 25, 100–109. [Google Scholar] [PubMed]
- Gonzaga, C.C.; Yoshimura, H.N.; Cesar, P.F.; Miranda, W.G. Subcritical crack growth in porcelains, glass-ceramics, and glass-infiltrated alumina composite for dental restorations. J. Mater. Sci. Mater. Med. 2009, 20, 1017. [Google Scholar] [PubMed]
- Facenda, J.C.; Borba, M.; Corazza, P.H. A literature review on the new polymer-infiltrated ceramic-network material (PICN). J. Esthet. Restor. Dent. 2018, 30, 281–286. [Google Scholar] [CrossRef]
- Leung, B.T.; Tsoi, J.K.; Matinlinna, J.P.; Pow, E.H. Comparison of mechanical properties of three machinable ceramics with an experimental fluorophlogopite glass ceramic. J. Prosthet. Dent. 2015, 114, 440–446. [Google Scholar] [PubMed]
- Ercoli, C.; Caton, J.G. Dental prostheses and tooth-related factors. J. Periodontol. 2018, 89, S223–S236. [Google Scholar] [CrossRef]
- Nayak, A.; Bhat, K.; Shivanaikar, S.; Pushpa, P.; Kugaji, M.; Kumbar, V. Detection of red complex organisms in chronic periodontitis by multiplex polymerase chain reaction. J. Adv. Clin. Res. Insights 2018, 5, 139–144. [Google Scholar] [CrossRef]
- Akram, Z.; Shafqat, S.S.; Aati, S.; Kujan, O.; Fawzy, A. Clinical efficacy of probiotics in the treatment of gingivitis: A systematic review and meta-analysis. Aust. Dent. J. 2020, 65, 12–20. [Google Scholar] [CrossRef]
- Prietto, N.R.; Martins, T.M.; dos Santos Santinoni, C.; Pola, N.M.; Ervolino, E.; Bielemann, A.M.; Leite, F.R.M. Treatment of experimental periodontitis with chlorhexidine as adjuvant to scaling and root planing. Arch. Oral Biol. 2020, 110, 104600. [Google Scholar] [CrossRef]
- Brayer, W.K.; Mellonig, J.T.; Dunlap, R.M.; Marinak, K.W.; Carson, R.E. Scaling and root planing effectiveness: The effect of root surface access and operator experience. J. Periodontol. 1989, 60, 67–72. [Google Scholar] [CrossRef]
- Raghavendra, M.; Koregol, A.; Bhola, S. Photodynamic therapy: A targeted therapy in periodontics. Aust. Dent. J. 2009, 54, S102–S109. [Google Scholar] [CrossRef] [PubMed]
- Knappe, V.; Frank, F.; Rohde, E. Principles of lasers and biophotonic effects. Photomed. Laser Surg. 2004, 22, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Kwiatkowski, S.; Knap, B.; Przystupski, D.; Saczko, J.; Kędzierska, E.; Knap-Czop, K.; Kotlińska, J.; Michel, O.; Kotowski, K.; Kulbacka, J. Photodynamic therapy–mechanisms, photosensitizers and combinations. Biomed. Pharmacother. 2018, 106, 1098–1107. [Google Scholar] [CrossRef]
- Akram, Z.; Hyder, T.; Al-Hamoudi, N.; Binshabaib, M.S.; Alharthi, S.S.; Hanif, A. Efficacy of photodynamic therapy versus antibiotics as an adjunct to scaling and root planing in the treatment of periodontitis: A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2017, 19, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Akram, Z.; Shafqat, S.S.; Niaz, M.O.; Raza, A.; Naseem, M. Clinical efficacy of photodynamic therapy and laser irradiation as an adjunct to open flap debridement in the treatment of chronic periodontitis: A systematic review and meta-analysis. Photodermatol. Photoimmunol. Photomed. 2020, 36, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Kellesarian, S.V.; Qayyum, F.; De Freitas, P.C.; Akram, Z.; Javed, F. Is antimicrobial photodynamic therapy a useful therapeutic protocol for oral decontamination? A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2017, 20, 55–61. [Google Scholar] [CrossRef]
- Akram, Z.; Raffat, M.A.; Shafqat, S.S.; Mirza, S.; Ikram, S. Clinical efficacy of photodynamic therapy as an adjunct to scaling and root planing in the treatment of chronic periodontitis among cigarette smokers: A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2019, 26, 334–341. [Google Scholar] [CrossRef]
- Sivaramakrishnan, G.; Sridharan, K. Photodynamic therapy for the treatment of peri-implant diseases: A network meta-analysis of randomized controlled trials. Photodiagnosis Photodyn. Ther. 2018, 21, 1–9. [Google Scholar] [CrossRef]
- Mathew, M.G.; Samuel, S.; Soni, A.J.; Roopa, K.B. Evaluation of adhesion of Streptococcus mutans, plaque accumulation on zirconia and stainless steel crowns, and surrounding gingival inflammation in primary molars: Randomized controlled trial. Clin. Oral Investig. 2020, 24, 1–6. [Google Scholar] [CrossRef]
- Karimi, M.R.; Hasani, A.; Khosroshahian, S. Efficacy of antimicrobial photodynamic therapy as an adjunctive to mechanical debridement in the treatment of peri-implant diseases: A randomized controlled clinical trial. J. Lasers Med Sci. 2016, 7, 139. [Google Scholar] [CrossRef] [PubMed]
- Mizutani, K.; Aoki, A.; Coluzzi, D.; Yukna, R.; Wang, C.Y.; Pavlic, V.; Izumi, Y. Lasers in minimally invasive periodontal and peri-implant therapy. Periodontology 2000 2016, 71, 185–212. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; Mori, G.; Dibello, V.; Marrelli, M.; Mirgaldi, R.; De Vito, D.; Tatullo, M. Anti-plaque and antimicrobial efficiency of different oral rinses in a 3-day plaque accumulation model. J. Biol. Regul. Homeost. Agents 2016, 30, 1173–1178. [Google Scholar]
- Akram, Z.; Abduljabbar, T.; Sauro, S.; Daood, U. Effect of photodynamic therapy and laser alone as adjunct to scaling and root planing on gingival crevicular fluid inflammatory proteins in periodontal disease: A systematic review. Photodiagnosis Photodyn. Ther. 2016, 16, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Hokari, T.; Morozumi, T.; Komatsu, Y.; Shimizu, T.; Yoshino, T.; Tanaka, M.; Tanaka, Y.; Nohno, K.; Kubota, T.; Yoshie, H. Effects of antimicrobial photodynamic therapy and local administration of minocycline on clinical, microbiological, and inflammatory markers of periodontal pockets: A pilot study. Int. J. Dent. 2018, 2018, 1748584. [Google Scholar] [CrossRef]
- Cho, K.; Lee, S.Y.; Chang, B.-S.; Um, H.-S.; Lee, J.-K. The effect of photodynamic therapy on Aggregatibacter actinomycetemcomitans attached to surface-modified titanium. J. Periodontal Implant Sci. 2015, 45, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Prates, R.A.; Yamada Jr, A.M.; Suzuki, L.C.; Hashimoto, M.C.E.; Cai, S.; Gouw-Soares, S.; Gomes, L.; Ribeiro, M.S. Bactericidal effect of malachite green and red laser on Actinobacillus actinomycetemcomitans. J. Photochem. Photobiol. B Biol. 2007, 86, 70–76. [Google Scholar] [CrossRef]
- Azizi, B.; Budimir, A.; Bago, I.; Mehmeti, B.; Jakovljević, S.; Kelmendi, J.; Stanko, A.P.; Gabrić, D. Antimicrobial efficacy of photodynamic therapy and light-activated disinfection on contaminated zirconia implants: An in vitro study. Photodiagnosis Photodyn. Ther. 2018, 21, 328–333. [Google Scholar] [CrossRef]
- Al-Radha, A.S.D.; Dymock, D.; Younes, C.; O’Sullivan, D. Surface properties of titanium and zirconia dental implant materials and their effect on bacterial adhesion. J. Dent. 2012, 40, 146–153. [Google Scholar] [CrossRef]
- Bottino, M.; Pereira, S.; Amaral, M.; Milhan, N.; Pereira, C.; Camargo, S.; Carvalho, A.; Melo, R. Streptococcus mutans Biofilm Formation and Cell Viability on Polymer-infiltrated Ceramic and Yttria-stabilized Polycrystalline Zirconium Dioxide Ceramic. Oper. Dent. 2019, 44, E271–E278. [Google Scholar] [PubMed]
- Scarano, A.; Piattelli, M.; Caputi, S.; Favero, G.A.; Piattelli, A. Bacterial adhesion on commercially pure titanium and zirconium oxide disks: An in vivo human study. J. Periodontol. 2004, 75, 292–296. [Google Scholar] [PubMed]
- Sayar, F.; Chiniforush, N.; Bahador, A.; Etemadi, A.; Akhondi, N.; Azimi, C. Efficacy of antimicrobial photodynamic therapy for elimination of Aggregatibacter actinomycetemcomitans biofilm on Laser-Lok titanium discs. Photodiagnosis Photodyn. Ther. 2019, 27, 462–466. [Google Scholar]
- Marrelli, M.; Maletta, C.; Inchingolo, F.; Alfano, M.; Tatullo, M. Three-point bending tests of zirconia core/veneer ceramics for dental restorations. Int. J. Dent. 2013, 2013, 831976. [Google Scholar] [PubMed]
- Dantas, L.C.D.M.; Silva-Neto, J.P.D.; Dantas, T.S.; Naves, L.Z.; das Neves, F.D.; da Mota, A.S. Bacterial adhesion and surface roughness for different clinical techniques for acrylic polymethyl methacrylate. Int. J. Dent. 2016, 2016, 8685796. [Google Scholar]
- Daood, U.; Banday, N.; Akram, Z.; Tsoi, J.K.; Neelakantan, P.; Omar, H.; Abduljabbar, T.; Vohra, F.; Al-Hamoudi, N.; Fawzy, A.S. Mechanical and spectroscopic analysis of retrieved/failed dental implants. Coatings 2017, 7, 201. [Google Scholar] [CrossRef]
- Alasqah, M.N. Antimicrobial efficacy of photodynamic therapy on dental implant surfaces: A systematic review of in vitro studies. Photodiagnosis Photodyn. Ther. 2019, 25, 349–353. [Google Scholar]
- Spagnuolo, G.; Codispoti, B.; Marrelli, M.; Rengo, C.; Rengo, S.; Tatullo, M. Commitment of oral-derived stem cells in dental and maxillofacial applications. Dent. J. 2018, 6, 72. [Google Scholar]
- Ballini, A.; Cantore, S.; Scacco, S.; Coletti, D.; Tatullo, M. Mesenchymal stem cells as promoters, enhancers, and playmakers of the translational regenerative medicine 2018. Stem Cells Int. 2018, 2018, 927401. [Google Scholar]
- Marrazzo, P.; Paduano, F.; Palmieri, F.; Marrelli, M.; Tatullo, M. Highly efficient in vitro reparative behaviour of dental pulp stem cells cultured with standardised platelet lysate supplementation. Stem Cells Int. 2016, 2016, 7230987. [Google Scholar]
- Marotti, J.; Tortamano, P.; Cai, S.; Ribeiro, M.S.; Franco, J.E.M.; de Campos, T.T. Decontamination of dental implant surfaces by means of photodynamic therapy. Lasers Med. Sci. 2013, 28, 303–309. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | P. gingivalis | T. forsythia | T. denticola | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | p-Value | Mean | SD | p-Value | Mean | SD | p-Value | Mean | SD | p-Value | |
| PDT | 0.6 a | 1.1 | <0.001 * | 0.5 a | 0.7 | <0.001 * | 0.5 a | 0.8 | <0.001 * | 0.7 a | 0.9 | <0.001 * |
| DL | 0.8 a | 1.2 | 0.8 a | 0.9 | 0.6 a | 0.7 | 0.9 a | 1.0 | ||||
| MB | 5.7 b | 1.0 | 5.6 b | 1.3 | 5.4 b | 1.1 | 6.8 b | 1.3 | ||||
| CHX | 1.0 a | 1.1 | 0.9 a | 1.0 | 0.8 a | 0.9 | 1.3 a | 1.4 | ||||
| NT | 6.5 b | 1.3 | 6.2 b | 0.9 | 6.1 b | 1.3 | 7.1 b | 0.9 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eldwakhly, E.; Saadaldin, S.; Aldegheishem, A.; Salah Mostafa, M.; Soliman, M. Antimicrobial Capacity and Surface Alterations Using Photodynamic Therapy and Light Activated Disinfection on Polymer-Infiltrated Ceramic Material Contaminated with Periodontal Bacteria. Pharmaceuticals 2020, 13, 350. https://doi.org/10.3390/ph13110350
Eldwakhly E, Saadaldin S, Aldegheishem A, Salah Mostafa M, Soliman M. Antimicrobial Capacity and Surface Alterations Using Photodynamic Therapy and Light Activated Disinfection on Polymer-Infiltrated Ceramic Material Contaminated with Periodontal Bacteria. Pharmaceuticals. 2020; 13(11):350. https://doi.org/10.3390/ph13110350
Chicago/Turabian StyleEldwakhly, Elzahraa, Selma Saadaldin, Alhanoof Aldegheishem, Marwa Salah Mostafa, and Mai Soliman. 2020. "Antimicrobial Capacity and Surface Alterations Using Photodynamic Therapy and Light Activated Disinfection on Polymer-Infiltrated Ceramic Material Contaminated with Periodontal Bacteria" Pharmaceuticals 13, no. 11: 350. https://doi.org/10.3390/ph13110350
APA StyleEldwakhly, E., Saadaldin, S., Aldegheishem, A., Salah Mostafa, M., & Soliman, M. (2020). Antimicrobial Capacity and Surface Alterations Using Photodynamic Therapy and Light Activated Disinfection on Polymer-Infiltrated Ceramic Material Contaminated with Periodontal Bacteria. Pharmaceuticals, 13(11), 350. https://doi.org/10.3390/ph13110350