
Predicting Knee Joint Kinematics from Wearable Sensor Data in People with Knee Osteoarthritis and Clinical Considerations for Future Machine Learning Models

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection
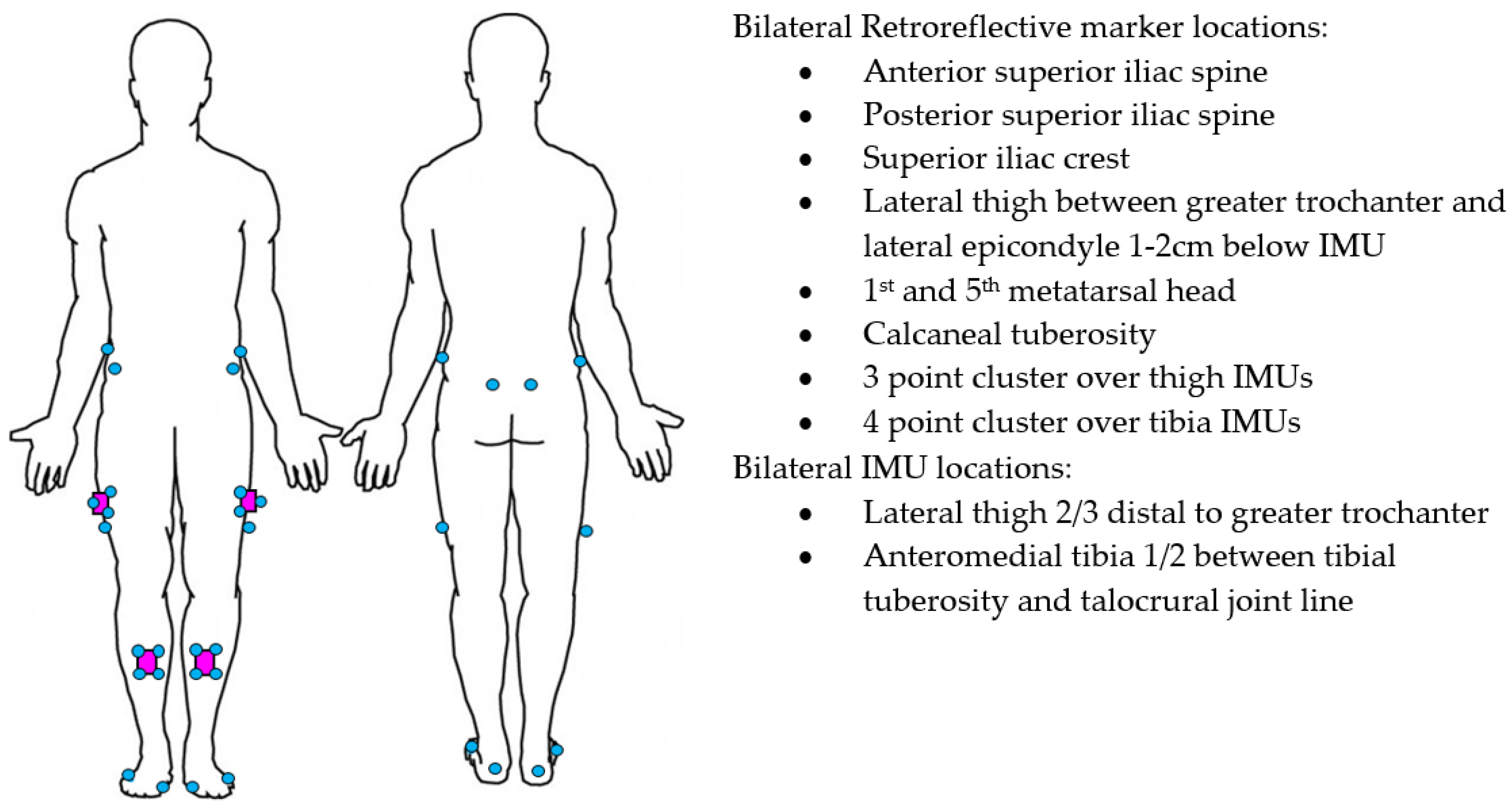
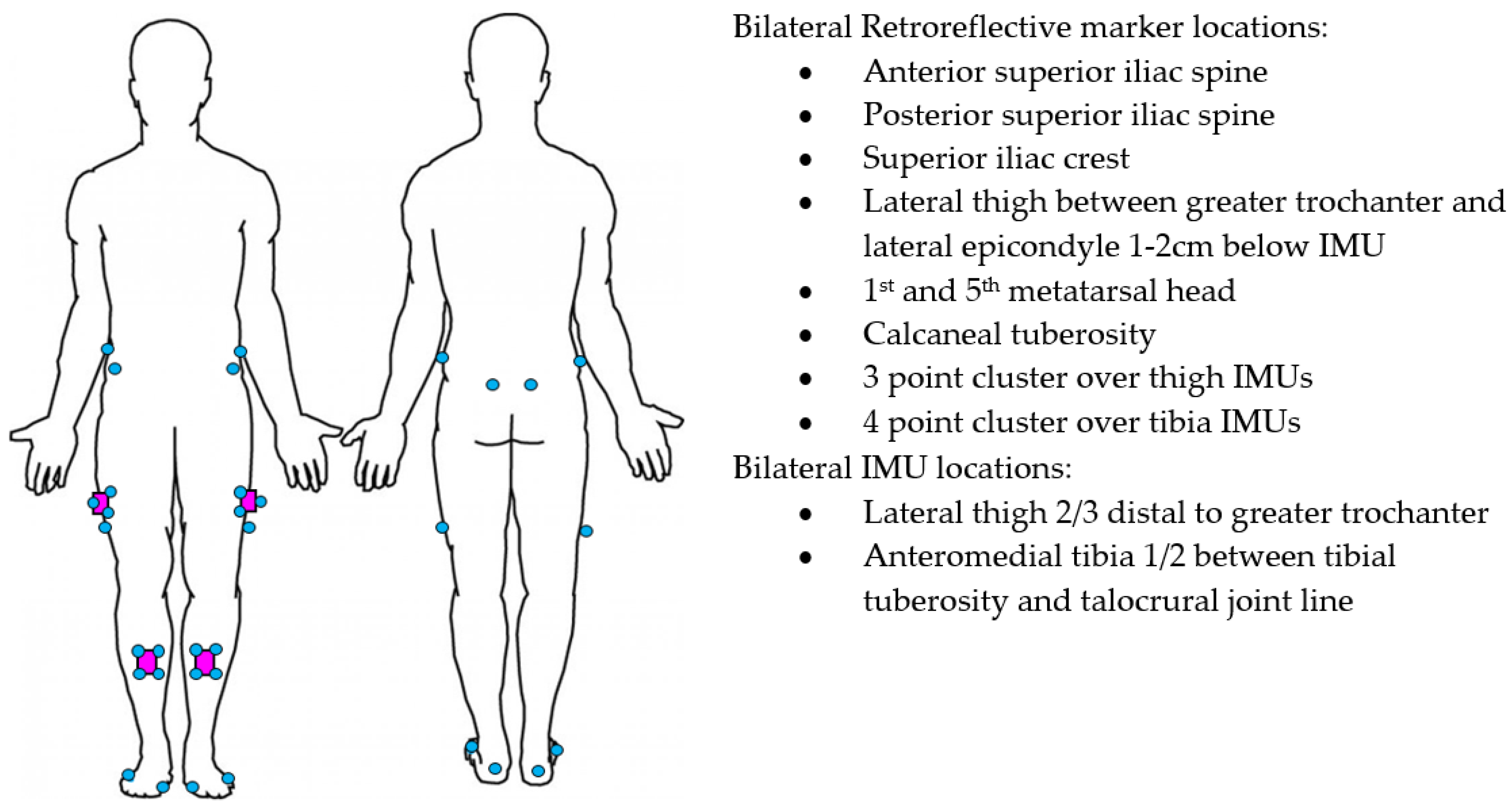
2.4. Instrumentation
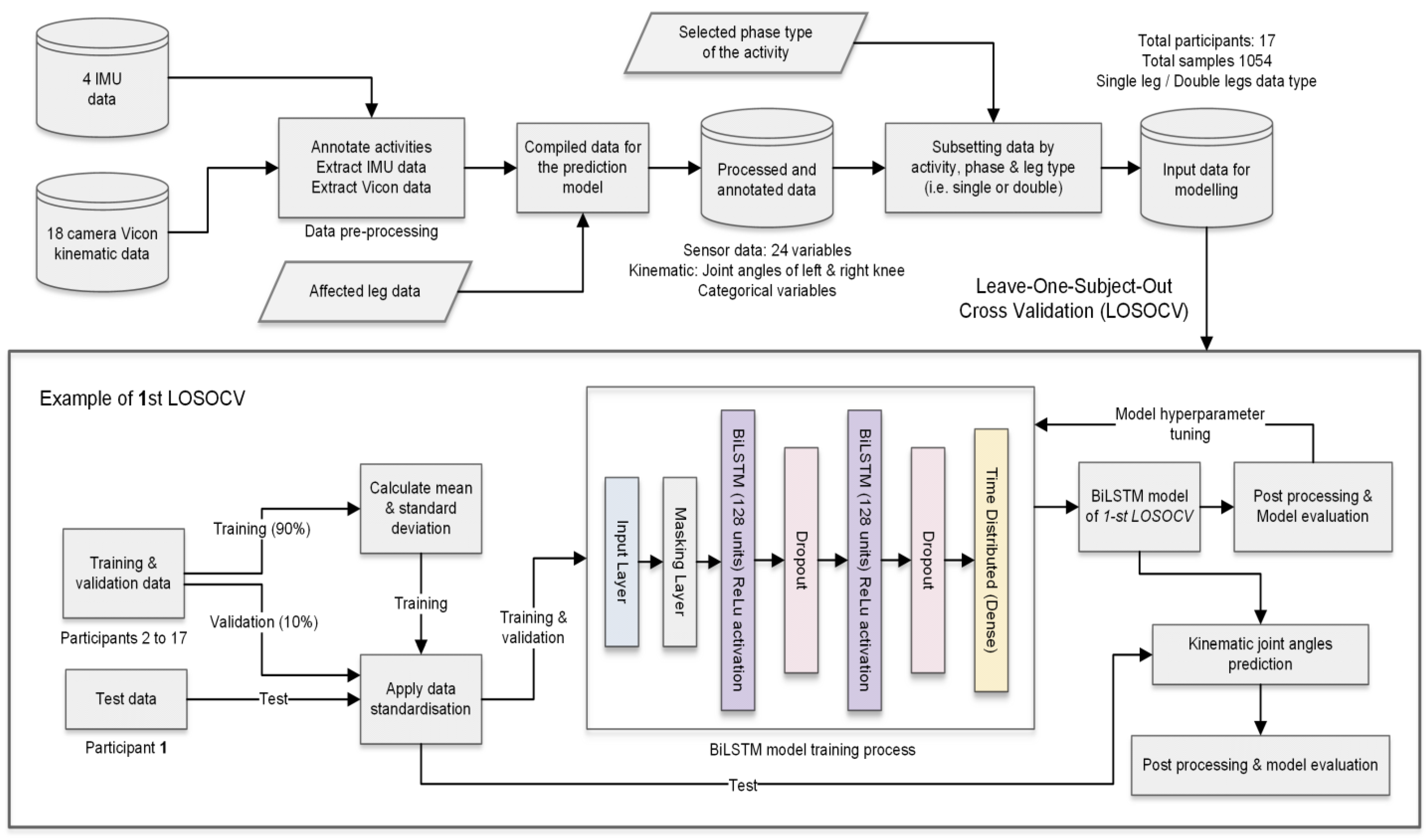
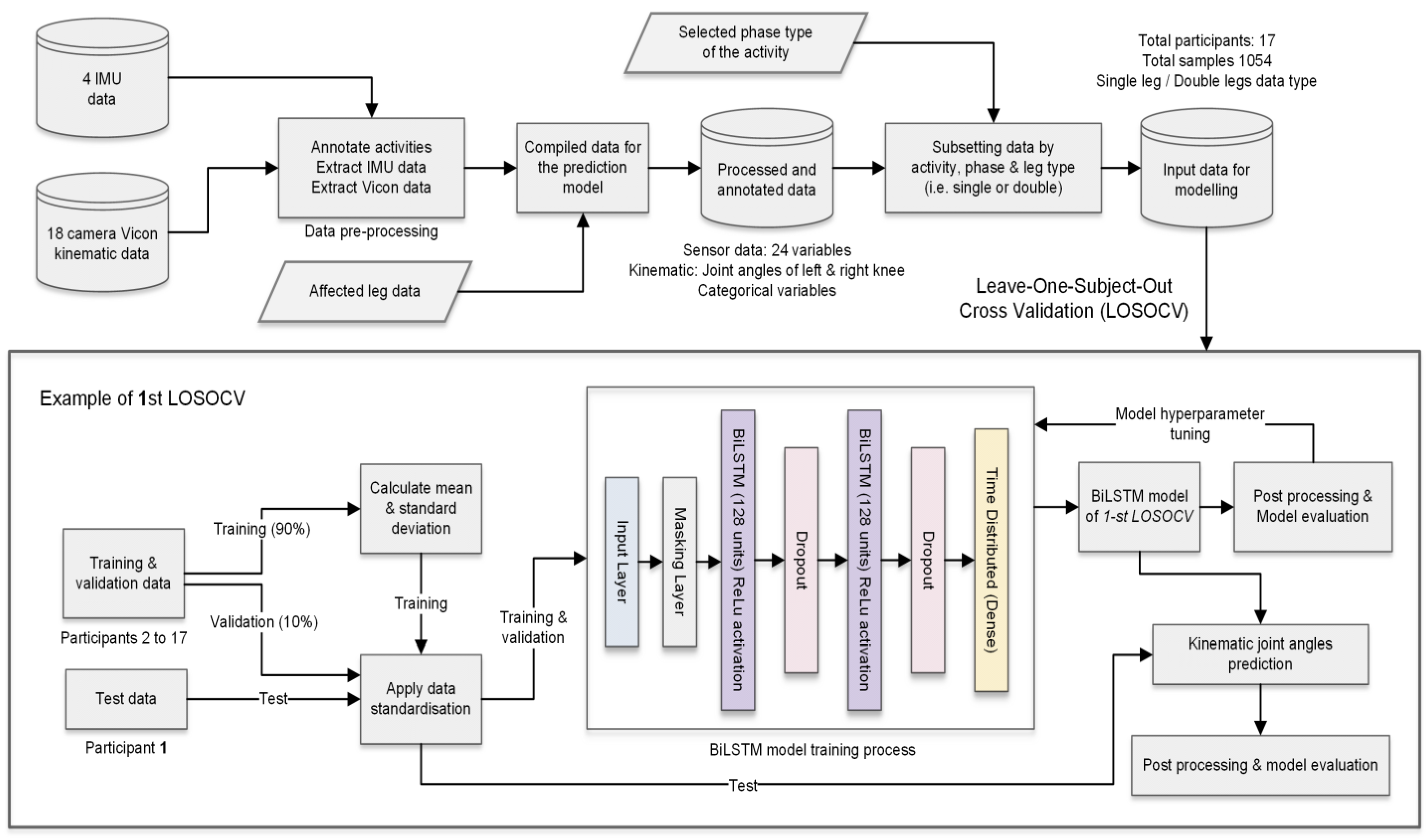
2.5. Data Preparation
2.6. Deep Learning Model Development
2.7. Model
2.8. Validation and Data Standardisation
3. Results
4. Discussion
4.1. Comparison to Previous Literature
4.2. Clinical Considerations for Kinematic Prediction Models
4.2.1. Variability of Movement in Clinical Populations
4.2.2. Selecting Clinically Important Activities and Biomechanical Parameters
4.2.3. Reducing the Burden for Clinicians
4.3. Considerations for Future Data Handling and Machine Learning Models
4.3.1. Developing Data Handling Pipelines
4.3.2. Single vs. Multiple Models
4.3.3. Augmented and Simulated Data
4.3.4. Deep Learning Architecture
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fukutani, N.; Iijima, H.; Aoyama, T.; Yamamoto, Y.; Hiraoka, M.; Miyanobu, K.; Jinnouchi, M.; Kaneda, E.; Tsuboyama, T.; Matsuda, S. Knee pain during activities of daily living and its relationship with physical activity in patients with early and severe knee osteoarthritis. Clin. Rheumatol. 2016, 35, 2307–2316. [Google Scholar] [CrossRef]
- Baliunas, A.J.; Hurwitz, D.E.; Ryals, A.B.; Karrar, A.; Case, J.P.; Block, J.A.; Andriacchi, T.P. Increased knee joint loads during walking are present in subjects with knee osteoarthritis. Osteoarthr. Cartil. 2002, 10, 573–579. [Google Scholar] [CrossRef] [Green Version]
- Bouchouras, G.; Patsika, G.; Hatzitaki, V.; Kellis, E. Kinematics and knee muscle activation during sit-to-stand movement in women with knee osteoarthritis. Clin. Biomech. 2015, 30, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Hinman, R.S.; Bennell, K.L.; Metcalf, B.R.; Crossley, K.M. Delayed onset of quadriceps activity and altered knee joint kinematics during stair stepping in individuals with knee osteoarthritis. Arch. Phys. Med. Rehabil. 2002, 83, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, I.; Hodgins, D.; Mor, A.; Elbaz, A.; Segal, G. Analysis of knee flexion characteristics and how they alter with the onset of knee osteoarthritis: A case control study. BMC Musculoskelet. Disord. 2013, 14, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, J.-S.T.; Tikoft, E.T.; O’Sullivan, P.; Smith, A.; Campbell, A.; Caneiro, J.P.; Kent, P. The Relationship Between Changes in Movement and Activity Limitation or Pain in People with Knee Osteoarthritis: A Systematic Review. J. Orthop. Sports Phys. Ther. 2021, 51, 492–502. [Google Scholar] [CrossRef]
- Davis, H.C.; Luc-Harkey, B.A.; Seeley, M.K.; Troy Blackburn, J.; Pietrosimone, B. Sagittal plane walking biomechanics in individuals with knee osteoarthritis after quadriceps strengthening. Osteoarthr. Cartil. 2019, 27, 771–780. [Google Scholar] [CrossRef]
- Wang, J.; Siddicky, S.F.; Oliver, T.E.; Dohm, M.P.; Barnes, C.L.; Mannen, E.M. Biomechanical Changes Following Knee Arthroplasty During Sit-To-Stand Transfers: Systematic Review. J. Arthroplast. 2019, 34, 2494–2501. [Google Scholar] [CrossRef]
- Dobson, F.; Hinman, R.S.; Roos, E.M.; Abbott, J.H.; Stratford, P.; Davis, A.M.; Buchbinder, R.; Snyder-Mackler, L.; Henrotin, Y.; Thumboo, J.; et al. OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthr. Cartil. 2013, 21, 1042–1052. [Google Scholar] [CrossRef] [Green Version]
- Milanese, S.; Gordon, S.; Buettner, P.; Flavell, C.; Ruston, S.; Coe, D.; O’Sullivan, W.; McCormack, S. Reliability and concurrent validity of knee angle measurement: Smart phone app versus universal goniometer used by experienced and novice clinicians. Man. Ther. 2014, 19, 569–574. [Google Scholar] [CrossRef] [Green Version]
- Cudejko, T.; Button, K.; Willott, J.; Al-Amri, M. Applications of Wearable Technology in a Real-Life Setting in People with Knee Osteoarthritis: A Systematic Scoping Review. J. Clin. Med. 2021, 10, 5645. [Google Scholar] [CrossRef] [PubMed]
- Kobsar, D.; Masood, Z.; Khan, H.; Khalil, N.; Kiwan, M.Y.; Ridd, S.; Tobis, M. Wearable Inertial Sensors for Gait Analysis in Adults with Osteoarthritis—A Scoping Review. Sensors 2020, 20, 7143. [Google Scholar] [CrossRef]
- Small, S.R.; Bullock, G.S.; Khalid, S.; Barker, K.; Trivella, M.; Price, A.J. Current clinical utilisation of wearable motion sensors for the assessment of outcome following knee arthroplasty: A scoping review. BMJ Open 2019, 9, e033832. [Google Scholar] [CrossRef] [Green Version]
- Binnie, T.; Smith, A.; Kent, P.; Ng, L.; O’Sullivan, P.; Tan, J.-S.; Davey, P.C.; Campbell, A. Concurrent validation of inertial sensors for measurement of knee kinematics in individuals with knee osteoarthritis: A technical report. Health Technol. 2021. [Google Scholar] [CrossRef]
- Van der Straaten, R.; De Baets, L.; Jonkers, I.; Timmermans, A. Mobile assessment of the lower limb kinematics in healthy persons and in persons with degenerative knee disorders: A systematic review. Gait Posture 2018, 59, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Rast, F.M.; Labruyère, R. Systematic review on the application of wearable inertial sensors to quantify everyday life motor activity in people with mobility impairments. J. NeuroEng. Rehabil. 2020, 17, 148. [Google Scholar] [CrossRef] [PubMed]
- Schall, M.C.; Fethke, N.B.; Chen, H.; Oyama, S.; Douphrate, D.I. Accuracy and repeatability of an inertial measurement unit system for field-based occupational studies. Ergonomics 2016, 59, 591–602. [Google Scholar] [CrossRef]
- de Vries, W.H.K.; Veeger, H.E.J.; Baten, C.T.M.; van der Helm, F.C.T. Magnetic distortion in motion labs, implications for validating inertial magnetic sensors. Gait Posture 2009, 29, 535–541. [Google Scholar] [CrossRef]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity of inertial sensor based 3D joint kinematics of static and dynamic sport and physiotherapy specific movements. PLoS ONE 2019, 14, e0213064. [Google Scholar] [CrossRef] [Green Version]
- Argent, R.; Drummond, S.; Remus, A.; O’Reilly, M.; Caulfield, B. Evaluating the use of machine learning in the assessment of joint angle using a single inertial sensor. J. Rehabil. Assist. Technol. Eng. 2019, 6. [Google Scholar] [CrossRef] [Green Version]
- Findlow, A.; Goulermas, J.Y.; Nester, C.; Howard, D.; Kenney, L.P.J. Predicting lower limb joint kinematics using wearable motion sensors. Gait Posture 2008, 28, 120–126. [Google Scholar] [CrossRef]
- Hernandez, V.; Dadkhah, D.; Babakeshizadeh, V.; Kulić, D. Lower body kinematics estimation from wearable sensors for walking and running: A deep learning approach. Gait Posture 2021, 83, 185–193. [Google Scholar] [CrossRef]
- Mundt, M.; Koeppe, A.; David, S.; Witter, T.; Bamer, F.; Potthast, W.; Markert, B. Estimation of Gait Mechanics Based on Simulated and Measured IMU Data Using an Artificial Neural Network. Front. Bioeng. Biotechnol. 2020, 8, 41. [Google Scholar] [CrossRef]
- Wouda, F.J.; Giuberti, M.; Bellusci, G.; Maartens, E.; Reenalda, J.; van Beijnum, B.-J.F.; Veltink, P.H. Estimation of Vertical Ground Reaction Forces and Sagittal Knee Kinematics During Running Using Three Inertial Sensors. Front. Physiol. 2018, 9, 218. [Google Scholar] [CrossRef]
- Rapp, E.; Shin, S.; Thomsen, W.; Ferber, R.; Halilaj, E. Estimation of Kinematics from Inertial Measurement Units Using a Combined Deep Learning and Optimization Framework. J. Biomech. 2021, 116, 110229. [Google Scholar] [CrossRef]
- Renani, M.S.; Eustace, A.M.; Myers, C.A.; Clary, C.W. The Use of Synthetic IMU Signals in the Training of Deep Learning Models Significantly Improves the Accuracy of Joint Kinematic Predictions. Sensors 2021, 21, 5876. [Google Scholar] [CrossRef] [PubMed]
- Mundt, M.; Thomsen, W.; Witter, T.; Koeppe, A.; David, S.; Bamer, F.; Potthast, W.; Markert, B. Prediction of lower limb joint angles and moments during gait using artificial neural networks. Med. Biol. Eng. Comput. 2020, 58, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.-S.; Beheshti, B.K.; Binnie, T.; Davey, P.; Caneiro, J.P.; Kent, P.; Smith, A.; O’Sullivan, P.; Campbell, A. Human Activity Recognition for People with Knee Osteoarthritis—A Proof-of-Concept. Sensors 2021, 21, 3381. [Google Scholar] [CrossRef]
- Stetter, B.J.; Krafft, F.C.; Ringhof, S.; Stein, T.; Sell, S. A Machine Learning and Wearable Sensor Based Approach to Estimate External Knee Flexion and Adduction Moments During Various Locomotion Tasks. Front. Bioeng. Biotechnol. 2020, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- Stetter, B.J.; Ringhof, S.; Krafft, F.C.; Sell, S.; Stein, T. Estimation of Knee Joint Forces in Sport Movements Using Wearable Sensors and Machine Learning. Sensors 2019, 19, 3690. [Google Scholar] [CrossRef] [Green Version]
- National Clinical Guideline Centre (UK). Osteoarthritis: Care and Management in Adults. Available online: https://www.ncbi.nlm.nih.gov/books/NBK333067/ (accessed on 8 September 2021).
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [Green Version]
- Ehara, Y.; Fujimoto, H.; Miyazaki, S.; Tanaka, S.; Yamamoto, S. Comparison of the performance of 3D camera systems. Gait Posture 1995, 3, 166–169. [Google Scholar] [CrossRef]
- Richards, J.G. The measurement of human motion: A comparison of commercially available systems. Hum. Mov. Sci. 1999, 18, 589–602. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Besier, T.F.; Sturnieks, D.L.; Alderson, J.A.; Lloyd, D.G. Repeatability of gait data using a functional hip joint centre and a mean helical knee axis. J. Biomech. 2003, 36, 1159–1168. [Google Scholar] [CrossRef]
- Mundt, M.; Koeppe, A.; Bamer, F.; David, S.; Markert, B. Artificial Neural Networks in Motion Analysis—Applications of Unsupervised and Heuristic Feature Selection Techniques. Sensors 2020, 20, 4581. [Google Scholar] [CrossRef]
- Mundt, M.; Johnson, W.R.; Potthast, W.; Markert, B.; Mian, A.; Alderson, J. A Comparison of Three Neural Network Approaches for Estimating Joint Angles and Moments from Inertial Measurement Units. Sensors 2021, 21, 4535. [Google Scholar] [CrossRef] [PubMed]
- Siami-Namini, S.; Tavakoli, N.; Namin, A.S. The Performance of LSTM and BiLSTM in Forecasting Time Series. In Proceedings of the 2019 IEEE International Conference on Big Data (Big Data), Los Angeles, CA, USA, 9–12 December 2019; pp. 3285–3292. [Google Scholar]
- Hendry, D.; Napier, K.; Hosking, R.; Chai, K.; Davey, P.; Hopper, L.; Wild, C.; O’Sullivan, P.; Straker, L.; Campbell, A. Development of a Machine Learning Model for the Estimation of Hip and Lumbar Angles in Ballet Dancers. Med. Probl. Perform. Artist. 2021, 36, 61–71. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Gholamiangonabadi, D.; Kiselov, N.; Grolinger, K. Deep Neural Networks for Human Activity Recognition with Wearable Sensors: Leave-One-Subject-Out Cross-Validation for Model Selection. IEEE Access 2020, 8, 133982–133994. [Google Scholar] [CrossRef]
- Ren, L.; Jones, R.K.; Howard, D. Whole body inverse dynamics over a complete gait cycle based only on measured kinematics. J. Biomech. 2008, 41, 2750–2759. [Google Scholar] [CrossRef] [PubMed]
- Corey, D.M.; Dunlap, W.P.; Burke, M.J. Averaging Correlations: Expected Values and Bias in Combined Pearson rs and Fisher’s z Transformations. J. Gen. Psychol. 1998, 125, 245–261. [Google Scholar] [CrossRef]
- Weygers, I.; Kok, M.; Konings, M.; Hallez, H.; De Vroey, H.; Claeys, K. Inertial Sensor-Based Lower Limb Joint Kinematics: A Methodological Systematic Review. Sensors 2020, 20, 673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Astephen, J.L.; Deluzio, K.J.; Caldwell, G.E.; Dunbar, M.J. Biomechanical changes at the hip, knee, and ankle joints during gait are associated with knee osteoarthritis severity. J. Orthop. Res. 2008, 26, 332–341. [Google Scholar] [CrossRef] [Green Version]
- Zanardi, A.P.J.; da Silva, E.S.; Costa, R.R.; Passos-Monteiro, E.; dos Santos, I.O.; Kruel, L.F.M.; Peyré-Tartaruga, L.A. Gait parameters of Parkinson’s disease compared with healthy controls: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 752. [Google Scholar] [CrossRef]
- Renani, M.S.; Myers, C.A.; Zandie, R.; Mahoor, M.H.; Davidson, B.S.; Clary, C.W. Deep Learning in Gait Parameter Prediction for OA and TKA Patients Wearing IMU Sensors. Sensors 2020, 20, 5553. [Google Scholar] [CrossRef]
- Albert, M.; Toledo, S.; Shapiro, M.; Koerding, K. Using Mobile Phones for Activity Recognition in Parkinson’s Patients. Front. Neurol. 2012, 3, 158. [Google Scholar] [CrossRef] [Green Version]
- Lonini, L.; Gupta, A.; Kording, K.; Jayaraman, A. Activity recognition in patients with lower limb impairments: Do we need training data from each patient? In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3265–3268. [Google Scholar]
- Chehab, E.F.; Favre, J.; Erhart-Hledik, J.C.; Andriacchi, T.P. Baseline knee adduction and flexion moments during walking are both associated with 5 year cartilage changes in patients with medial knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 1833–1839. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, T.; Wada, M.; Kawahara, H.; Sato, M.; Baba, H.; Shimada, S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann. Rheum. Dis. 2002, 61, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Hendry, D.; Chai, K.; Campbell, A.; Hopper, L.; O’Sullivan, P.; Straker, L. Development of a Human Activity Recognition System for Ballet Tasks. Sports Med. Open 2020, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Joo, H.; Lee, J.; Chee, Y. Automatic Classification of Squat Posture Using Inertial Sensors: Deep Learning Approach. Sensors 2020, 20, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadillioglu, C.; Stetter, B.J.; Ringhof, S.; Krafft, F.C.; Sell, S.; Stein, T. Automated gait event detection for a variety of locomotion tasks using a novel gyroscope-based algorithm. Gait Posture 2020, 81, 102–108. [Google Scholar] [CrossRef]
- Dorschky, E.; Nitschke, M.; Martindale, C.F.; van den Bogert, A.J.; Koelewijn, A.D.; Eskofier, B.M. CNN-Based Estimation of Sagittal Plane Walking and Running Biomechanics From Measured and Simulated Inertial Sensor Data. Front. Bioeng. Biotechnol. 2020, 8, 604. [Google Scholar] [CrossRef] [PubMed]
- Ascioglu, G.; Senol, Y. Design of a wearable wireless multi-sensor monitoring system and application for activity recognition using deep learning. IEEE Access 2020, 8, 169183–169195. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Phase of Activity | Samples (Participants) |
|---|---|
| Sit-to-stand | 61 (15) |
| Stand-to-sit | 61 (15) |
| Walk swing | 245 (17) |
| Walk stance | 244 (17) |
| Stair up swing | 130 (15) |
| Stair up stance | 87 (15) |
| Stair down swing | 83 (15) |
| Stair down stance | 44 (15) |
| Total | 955 (17) |
| All Participants (n = 17) | ||
|---|---|---|
| Characteristics | Mean | SD |
| Age (years) | 66.2 | 8.7 |
| Male (%) | 59% | |
| Weight (kg) | 80.3 | 15.9 |
| Height (cm) | 173 | 8.8 |
| BMI (kg/m2) | 26.6 | 15.9 |
| KOOS function | 68.4 | 12.6 |
| Single-Leg Prediction Model | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Walk | Stair Down | Stair Up | |||||||
| Outcome | Sit- to-stand | Stand- to-sit | Swing | Stance | Swing | Stance | Swing | Stance | |
| Time- Series | RMSE (°) (SD) | 8.24 | 9.30 | 9.70 | 7.04 | 11.78 | 8.22 | 10.41 | 8.99 |
| (3.02) | (2.99) | (3.86) | (2.60) | (6.04) | (2.80) | (5.11) | (3.70) | ||
| nRMSE (%) (SD) | 9.79 | 10.86 | 17.66 | 36.33 | 14.06 | 22.91 | 15.06 | 19.14 | |
| (3.71) | (3.78) | (9.05) | (14.39) | (7.90) | (9.99) | (8.70) | (10.00) | ||
| MAE (°) (SD) | 7.12 | 7.96 | 8.46 | 5.99 | 10.37 | 7.00 | 9.06 | 8.06 | |
| (2.87) | (2.60) | (3.45) | (2.34) | (5.44) | (2.55) | (4.54) | (3.64) | ||
| R | 0.99 | 0.99 | 0.98 | 0.85 | 0.99 | 0.96 | 0.98 | 0.98 | |
| Peak | RMSE (°) (SD) | 6.46 | 6.89 | 9.75 | 10.31 | 9.72 | 21.38 | 9.78 | 11.73 |
| (2.48) | (4.28) | (6.21) | (5.42) | (3.72) | (12.29) | (6.65) | (6.39) | ||
| Minimum | RMSE (°) (SD) | 6.92 | 7.71 | 7.35 | 6.21 | 8.07 | 6.07 | 10.33 | 8.04 |
| (4.57) | (5.77) | (3.72) | (2.99) | (5.73) | (4.69) | (5.00) | (5.76) | ||
| Double-Leg Prediction Model | |||||||||
| Walk | Stair Down | Stair Up | |||||||
| Outcome | Sit- to-stand | Stand- to-sit | Swing | Stance | Swing | Stance | Swing | Stance | |
| Time- Series | RMSE (°) (SD) | 7.27 | 8.10 | 9.81 | 8.19 | 12.85 | 10.19 | 10.17 | 9.61 |
| (1.72) | (2.29) | (3.98) | (2.69) | (5.63) | (3.19) | (4.63) | (3.59) | ||
| nRMSE (%)(SD) | 8.68 | 9.45 | 17.78 | 43.33 | 15.70 | 32.93 | 15.14 | 19.90 | |
| (2.58) | (2.89) | (8.68) | (16.55) | (7.45) | (23.18) | (8.29) | (8.50) | ||
| MAE (°) (SD) | 6.03 | 6.72 | 8.47 | 6.92 | 11.09 | 8.47 | 8.81 | 8.36 | |
| (1.69) | (2.11) | (3.52) | (2.39) | (5.07) | (3.02) | (4.25) | (3.40) | ||
| R | 0.99 | 0.99 | 0.97 | 0.74 | 0.98 | 0.92 | 0.98 | 0.96 | |
| Peak | RMSE (°) (SD) | 5.09 | 6.44 | 9.23 | 10.29 | 10.73 | 24.33 | 10.01 | 13.28 |
| (2.97) | (4.23) | (5.65) | (6.51) | (5.39) | (10.70) | (8.22) | (8.18) | ||
| Minimum | RMSE (°) (SD) | 6.49 | 6.15 | 8.76 | 6.60 | 11.21 | 8.99 | 10.36 | 7.79 |
| (4.55) | (4.13) | (4.31) | (2.37) | (8.60) | (3.79) | (5.02) | (5.36) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, J.-S.; Tippaya, S.; Binnie, T.; Davey, P.; Napier, K.; Caneiro, J.P.; Kent, P.; Smith, A.; O’Sullivan, P.; Campbell, A. Predicting Knee Joint Kinematics from Wearable Sensor Data in People with Knee Osteoarthritis and Clinical Considerations for Future Machine Learning Models. Sensors 2022, 22, 446. https://doi.org/10.3390/s22020446
Tan J-S, Tippaya S, Binnie T, Davey P, Napier K, Caneiro JP, Kent P, Smith A, O’Sullivan P, Campbell A. Predicting Knee Joint Kinematics from Wearable Sensor Data in People with Knee Osteoarthritis and Clinical Considerations for Future Machine Learning Models. Sensors. 2022; 22(2):446. https://doi.org/10.3390/s22020446
Chicago/Turabian StyleTan, Jay-Shian, Sawitchaya Tippaya, Tara Binnie, Paul Davey, Kathryn Napier, J. P. Caneiro, Peter Kent, Anne Smith, Peter O’Sullivan, and Amity Campbell. 2022. "Predicting Knee Joint Kinematics from Wearable Sensor Data in People with Knee Osteoarthritis and Clinical Considerations for Future Machine Learning Models" Sensors 22, no. 2: 446. https://doi.org/10.3390/s22020446
APA StyleTan, J.-S., Tippaya, S., Binnie, T., Davey, P., Napier, K., Caneiro, J. P., Kent, P., Smith, A., O’Sullivan, P., & Campbell, A. (2022). Predicting Knee Joint Kinematics from Wearable Sensor Data in People with Knee Osteoarthritis and Clinical Considerations for Future Machine Learning Models. Sensors, 22(2), 446. https://doi.org/10.3390/s22020446