Ionizing Radiation Measurement Solution in a Hospital Environment

Abstract
:
1. Introduction
2. Technological Background
2.1. Ionizing Radiation
- Alpha particles (α): They are usually generated in nuclear reactions or radioactive disintegration. Their capacity of penetration is low. They quickly lose their kinetic energy in the atmosphere, because they interact strongly with other molecules due to their great mass and electrical charge, generating a significant number of ions per centimeter of covered length. In general, they cannot pass through the thickness of multiple sheets of paper. However, if an alpha emitter enters the body it can be very harmful.
- Beta particles (β): They have greater penetration than alpha particles. They can be stopped by a few centimeters of wood or a thin sheet of metal. However, as with alpha particles, they can cause serious damage to the human body.
- Gamma particles (γ): Gamma radiation (γ) is a type of electromagnetic radiation [4]. Gamma rays can cause serious damage to the nucleus of cells, so they are used to sterilize medical equipment and food. Gamma rays easily pass through the skin and other organic substances; therefore, they could cause serious damage to internal human organs. X-rays are included under this category. They are also photons, but with a lower penetration capacity than gamma rays.
2.2. Recommended Criteria to Assign Dosimeters for Healthcare Workers
- The Spanish Health Protection regulation against Ionizing Radiation (Royal Decree 783/2001 (BOE 26/07/2001) defines exposed healthcare workers as those who, due to the circumstances in which their work is carried out, are habitually/occasionally subject to the risk of exposure to ionizing radiation that may involve doses higher than the limits recommended for members of the public. Exposed healthcare workers are further classified into two categories, A and B:
- Category A includes those who can receive an effective dose greater than 6 mSv (miliSievert) per official year, or a dose greater than 3/10 of the equivalent dose limit for eye lenses (45 mSv/year), skin and limbs (150 mSv/year). In Category A, exposed workers must use a personal dosimeter.
- Category B includes exposed workers who rarely receive effective doses in excess of 6 mSv per official year, or 3/10 of the equivalent dose limit for eye lenses, skin and limbs. These workers are not necessarily required to wear personal dosimeters. It is sufficient for them to be controlled by a dosimetry monitoring system that guarantees that the doses received are compatible with their level B classification.
- Non-exposed workers, such as members of the public health system, do not require any dosimetry control.
- Those who have to stay close to the radiation beam in interventional radiology and hemodynamics.
- Healthcare workers preparing and administering radioactive doses in nuclear medicine.
- Healthcare workers who are involved in the preparation of treatment and care of patients in radioactive metabolic therapy.
- Healthcare workers performing these functions in brachytherapy.
2.3. Dosimetry Classification
2.3.1. Personal Dosimetry
- Dosimetry of the whole organism: It is implemented by a lapel dosimeter, which must be placed in a position that is representative of the most exposed part of the body surface. In those cases where a lead apron is required, the dosimeter should be placed under the apron.
- Dosimetry of the upper extremities: It is implemented by wearing wrist or ring dosimeters. Recommended only in those cases where the doses to the hands can be notably higher than those of the whole organism, due to their proximity to the radiation beam.
- Abdomen dosimetry: It is implemented by lapel dosimeters. Only used on the abdomen of exposed pregnant workers. Where a lead apron is required, the dosimeter should be placed under the apron.
2.3.2. Non-Personal Dosimetry
- Area dosimetry: It is performed by means of lapel dosimeters. It is reserved for the estimation of doses in places or areas where workers are exposed under category A.
- Dosimetry of rotating workplaces: It is performed using lapel and/or wrist dosimeters. It is focused on estimating doses in those workplaces where an activity is occasionally performed, and category B workers could be exposed.
- Research dosimetry: It is carried out using lapel and/or wrist dosimeters. It is requested by a Radiation Protection Service to measure doses in all those situations not covered in the previous cases.
- Ionization chamber [13]. It is the most straightforward gas detector, considered as a plane-parallel capacitor, in which the region between planes is completely filled with a gas, preferably with air. The electric field in this region prevents the recombination of the ions with electrons, which involves electrons moving towards the positive electrode, while positively charged ions move to the negative electrode. The applied voltage sets the velocity at which electrons and ions move to the chamber electrodes. For instance, for a typical voltage value of about 100 V, ions move at speeds of 1 m/s. Under these conditions, ions take up to 0.01 s to get through a 1 cm thick chamber (note that electrons are more mobile than ions and they will move 1000 times faster). An inconvenience is that these temporal values are excessively long for the time dealt with in radiation detection (e.g., a Computer Tomography).
- Proportional counter [14]. It consists of a metal case filled with a noble gas such as argon or xenon, with a very fine thread crossing the center. The wire (anode) is set at a high potential difference in relation to the box, so that an electric field constantly passes through the gas. The process is the following: when an ionizing particle, such as an electron, goes through the gas, it releases electrons from its atoms (it ionizes the atoms), leaving behind a positively charged ion and a free electron. The free electrons generated in the gas are accelerated to the anode and their amount is proportional to the initial energy of the particle or X-ray. Unlike simple ionization chambers, the potential difference used in proportional counters is much greater, so the electrons accelerated towards the anode have enough energy to produce secondary but proportional ionizations (hence the name of the device), causing an electronic “cascade”. The electric current or voltage generated in the anode can then be measured and digitized and, as mentioned above, the voltage or charge is proportional to the energy of the particle or X-ray incident. To be able to observe individual pulses, we must increase the applied voltage (which means exceeding 1000 V, its main inconvenience). To this respect, the largest electric field is capable of accelerating electrons so that they can generate secondary ionizations. Accelerated secondary electrons produce new ionizations, eventually creating an avalanche or cascade of ionizations.
- Geiger-Müller counter [15]: If the electric field increases further, the Geiger-Müller region is reached. In this case, secondary avalanches are generated anywhere in the tube, caused by photons emitted by atoms stimulated in the original avalanche. These photons move relatively far from the original avalanche location and, in a short time, the entire tube is involved in the process. Counters based on this principle are known as Geiger-Müller meters. Since the entire tube is involved in each initial avalanche, there is no information on the energy of the original radiation (all incident radiation produces identical output pulses valued around 1 V). So, Geiger-Müller counters are employed as pulse counters. However, in these counters there is a serious problem. During their movement into the tube, ions can be accelerated, reaching the anode with enough energy to release electrons and starting the process again (due to the nature of the multiple avalanches). To overcome this inconvenience, a second type of gas, called quenching gas, is added. This gas is made up of complex organic molecules such as ethanol (while the primary gas is usually made up of simple molecules, such as argon). A typical mixture of gases will be: 90% argon and 10% ethanol. The molecular nature of this added gas prevents the appearance of continuous avalanches. Geiger-Müller sensors allow the obtaining of accurate radiation doses with a remarkably low cost, and its integration into any electronic system to manage the information and dispatch it to remote places is a straightforward process. These are the main reasons why the Geiger-Müller counter has been adopted as part of our proposal.
- Incident radiation interacts with the atoms and molecules of the material, stimulating them.
- Stimulated states are de-energized by emitting visible (or nearly visible) fluorescent light.
- The light reaches a photosensitive surface by pulling out photoelectrons.
- The electrons accelerate and multiply in number to form an electrical pulse.
2.4. Discussion
- Limited storage. There are devices that can store the radiation captured internally. However, due to the limited memory capacity of these devices, it is not possible to have a large amount of stored data.
- Scarce Flexibility. Most devices do not allow the collection of data in any other way than that established by the manufacturer. In the particular case of personal thermo-luminescent dosimeters, where the stored data can be accessed, radiation collection must be stopped and be replaced by another device while accessing the data.
- High cost. Those alternatives that have some storage capacity and offer results in accurate, real time radiation doses (especially for area dosimeters) have a clear impact on the cost. Therefore, these solutions are addressed to public entities or big, private companies.
- Power supply. A large number of dosimeters described in this section are supplied by batteries. In the case of failing batteries, the received dose is not computed and a health risk could result.
- Manufacturer dependent. A priori, any modification of the device firmware to adapt it to new conditions of the application/environment is not possible.
3. Proposal
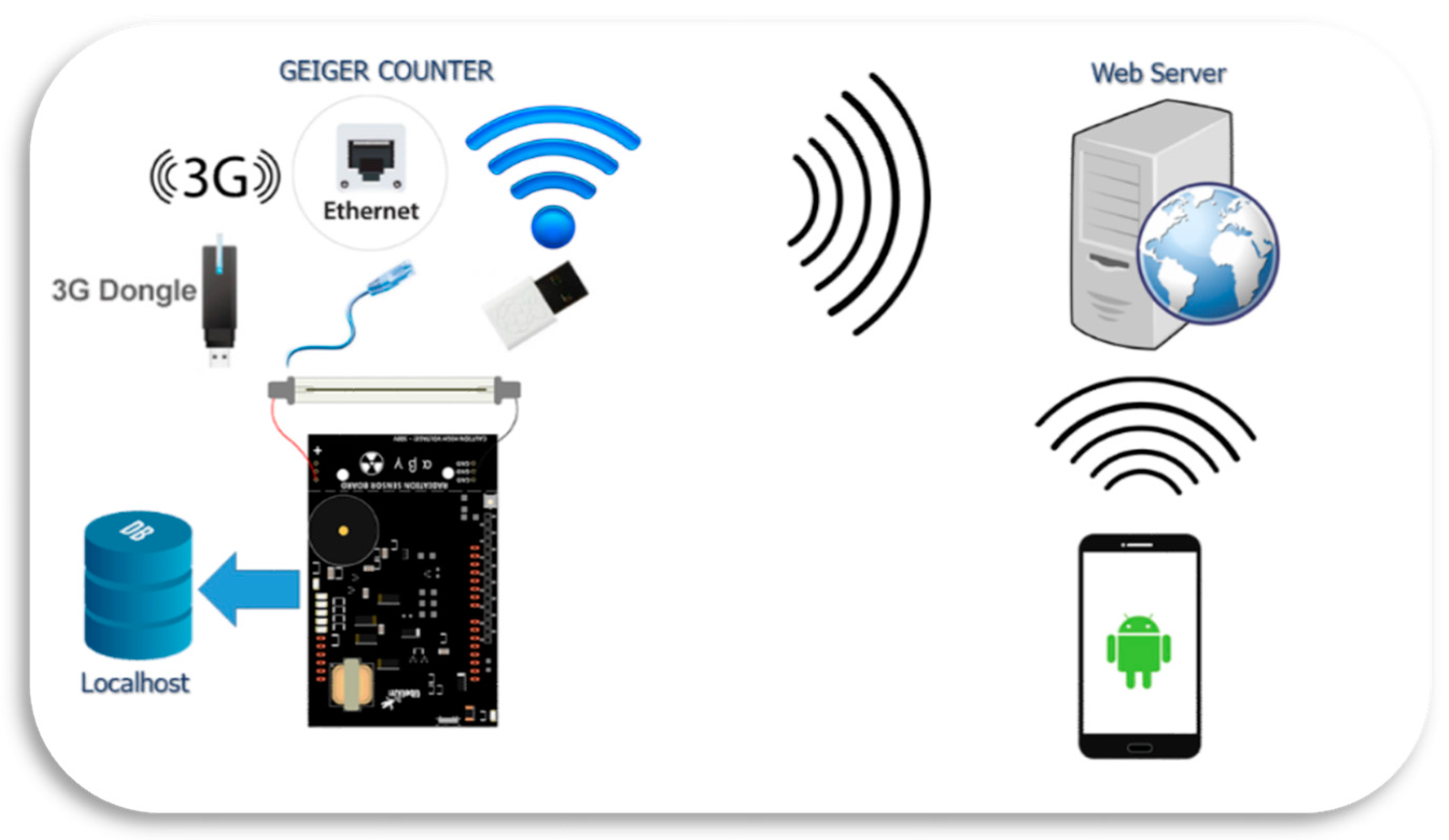
3.1. General Overview
3.2. Advantages of Our Proposal in Respect to Current α, β, γ Radiation Meters
- Low cost. In comparison to other systems, the features and functions offered by our system are more competitive in terms of cost.
- Double functionality. The device can be used for both personal (in specific places as, for instance, the CT room) and area dosimetry.
- Real time doses. This system is capable of displaying the dose values in real time either as a personal or area dosimeter.
- High storage capacity. In contrast to other current systems, our system has a large storage capacity, due to the database usage.
- Statistics. Several statistics are calculated immediately by the remote server, available for users at any time.
- Connection alternatives. The device is able to connect to remote databases through a set of interfaces (USB, Ethernet, WiFi and 3G).
- Data recovery. If the device loses the connection to the remote database, all radiation values are stored in the device until the connection is restored.
- Flexibility and modulation. The system is built using general-purpose and open-source technologies, which allows software/hardware modifications.
- Easy access. Users can check the data everywhere, due to the fact that the interface is a smartphone app that is connected to the remote database.
- Reliability. Different connection alternatives, replicated databases, and continuous energy supply contribute to a robust and reliable system.
- Verification. The device has been verified in CND, under standard calibration protocols.
- Easy handling and installation. Once the power is turned on, the device is automatically set to capture radiation, store it on the system and connect to the remote web service.
- Authentication. Security tasks will be implemented in a future work; however, the user must register to access dose values.
- Validation. This proposal has been validated at St. Lucia University Hospital in different environments, which will be further described in Section 5.
3.3. In Detail: Description HW/SW of the System
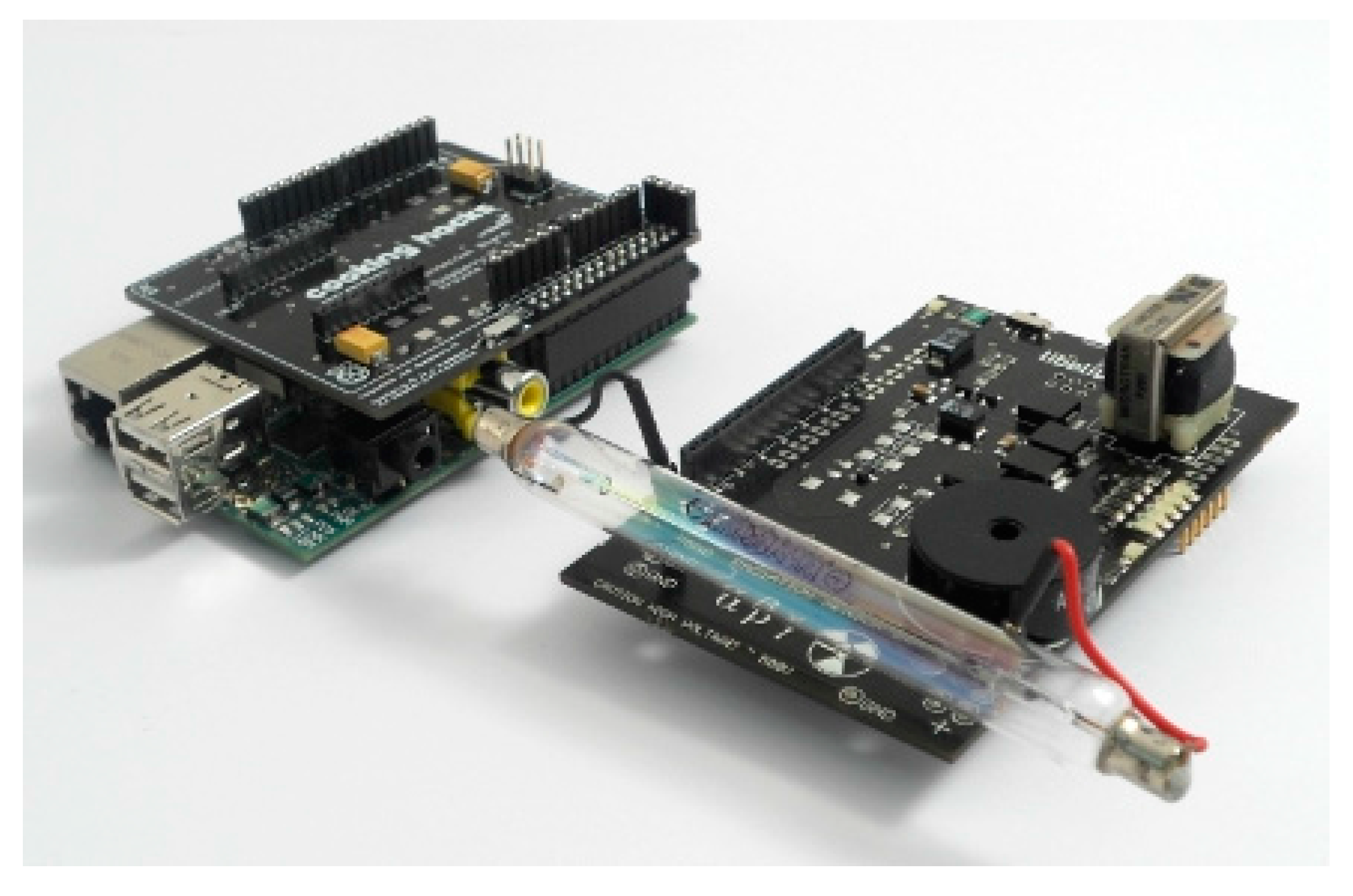
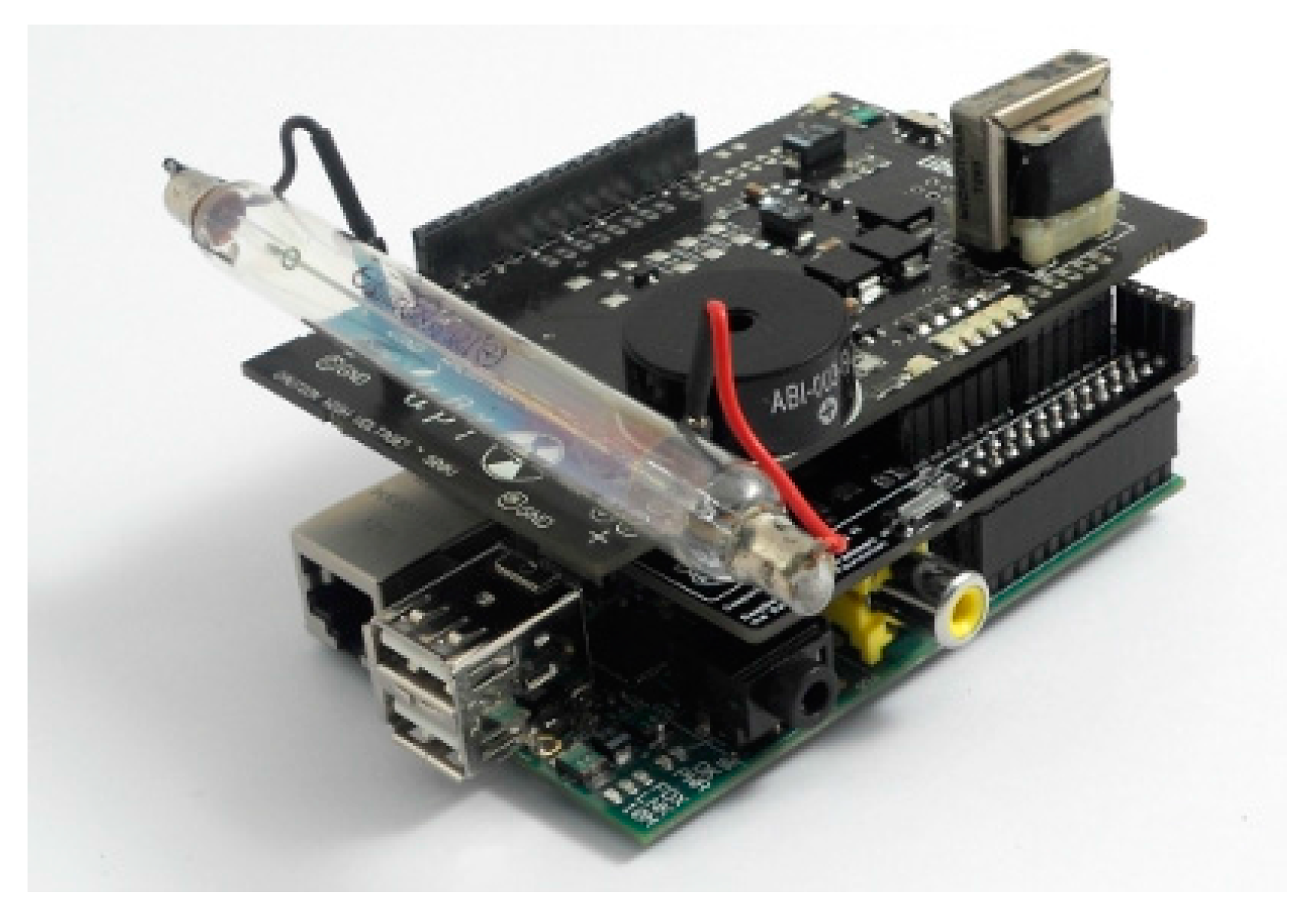
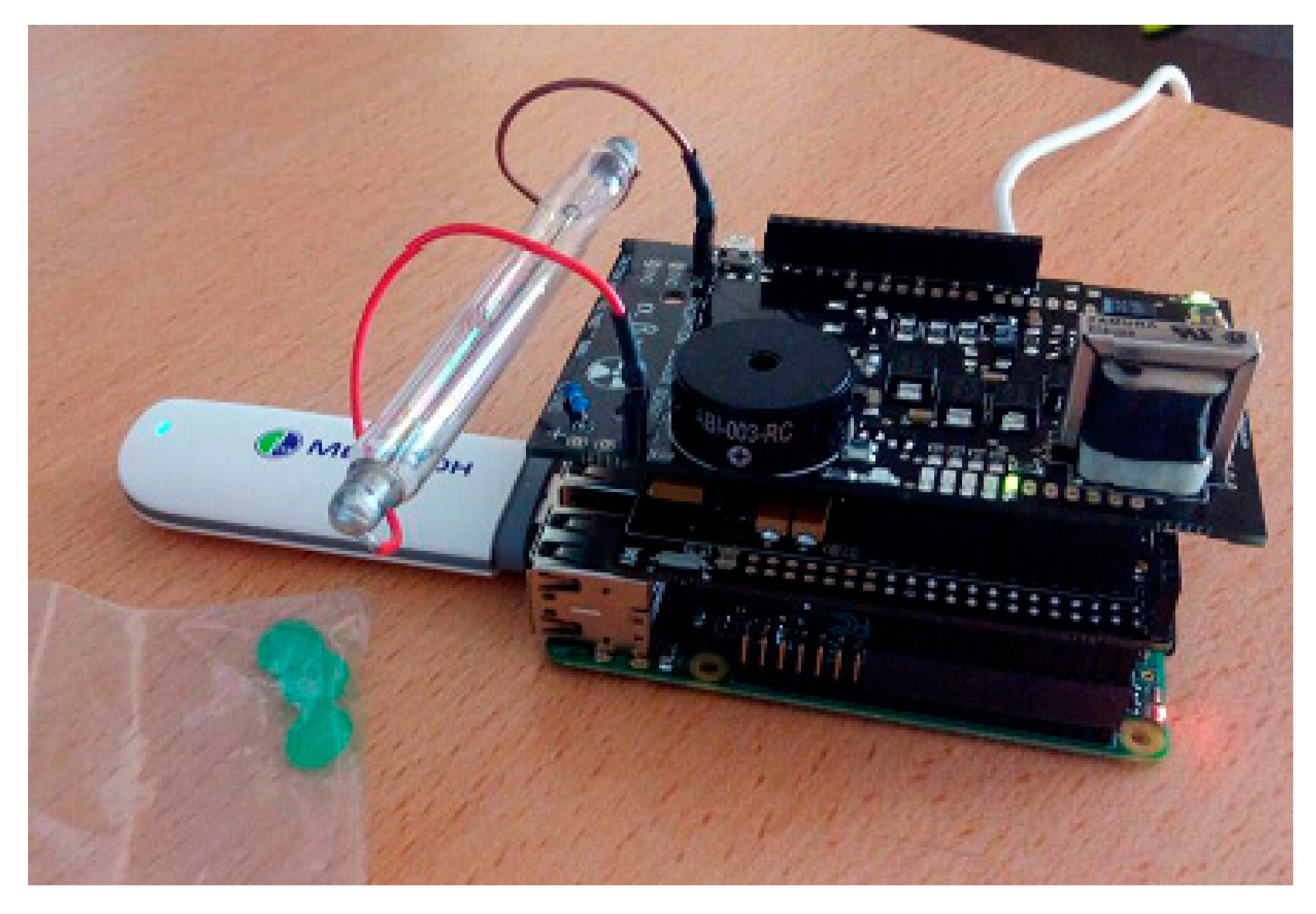
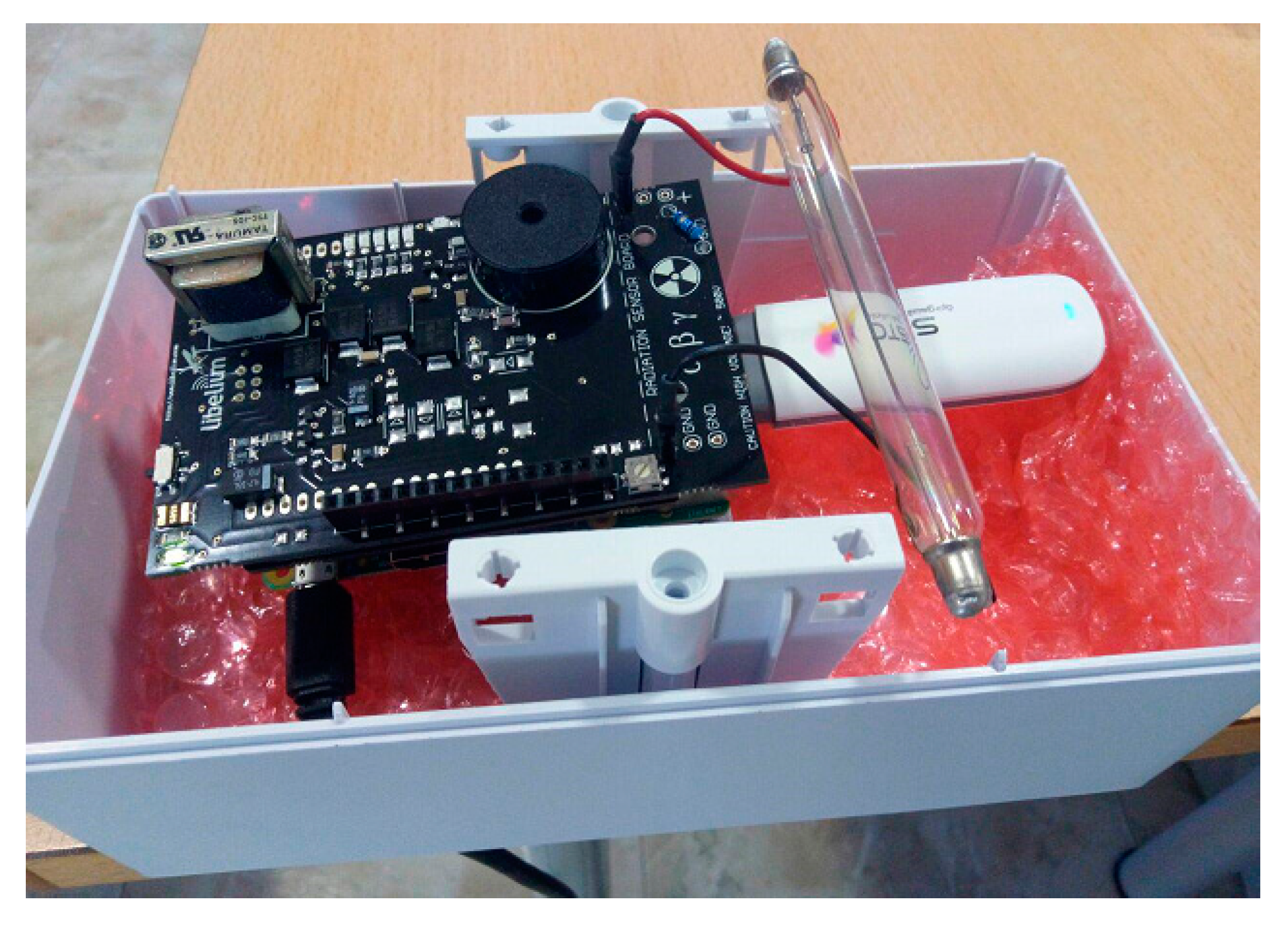
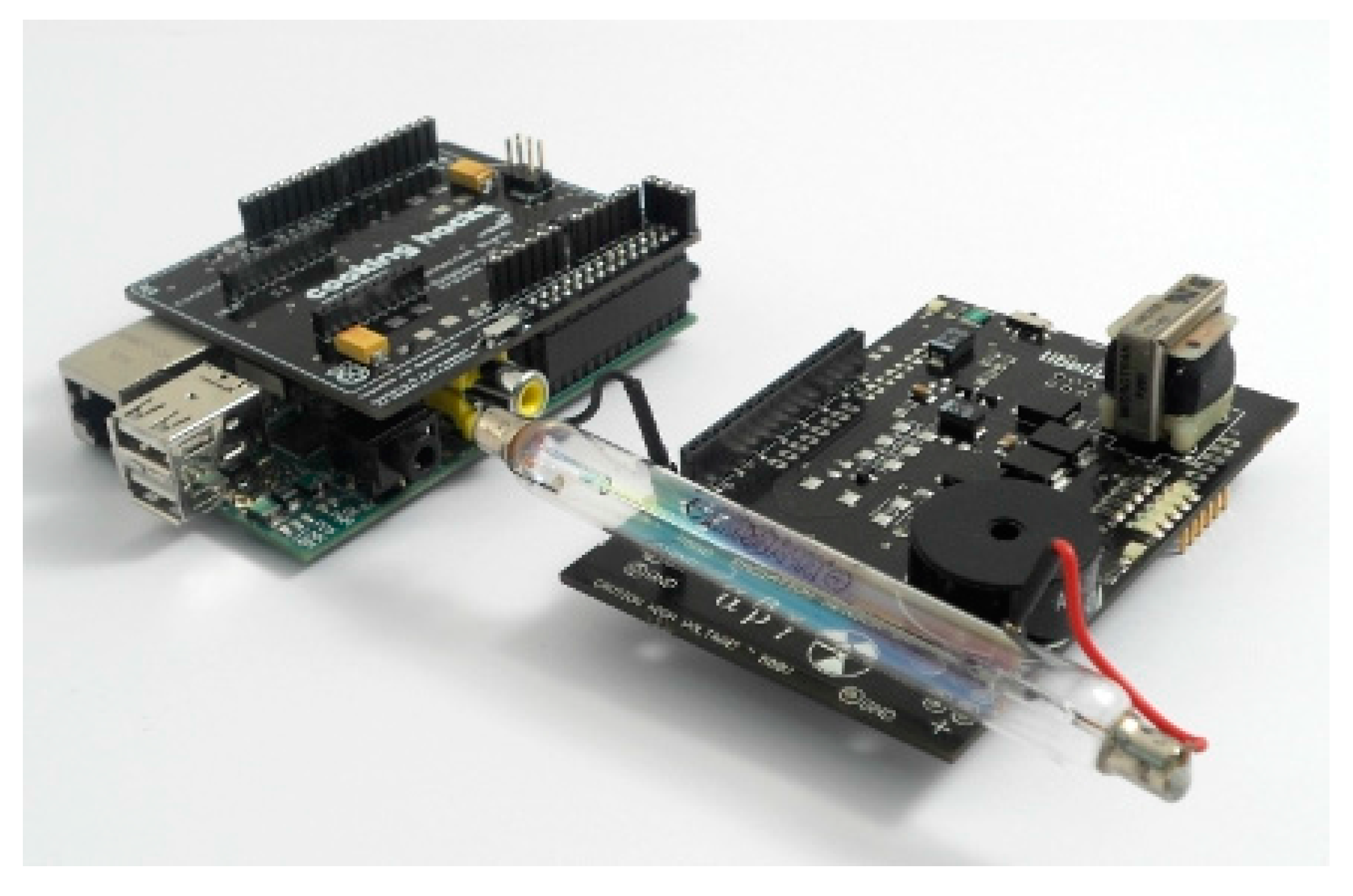
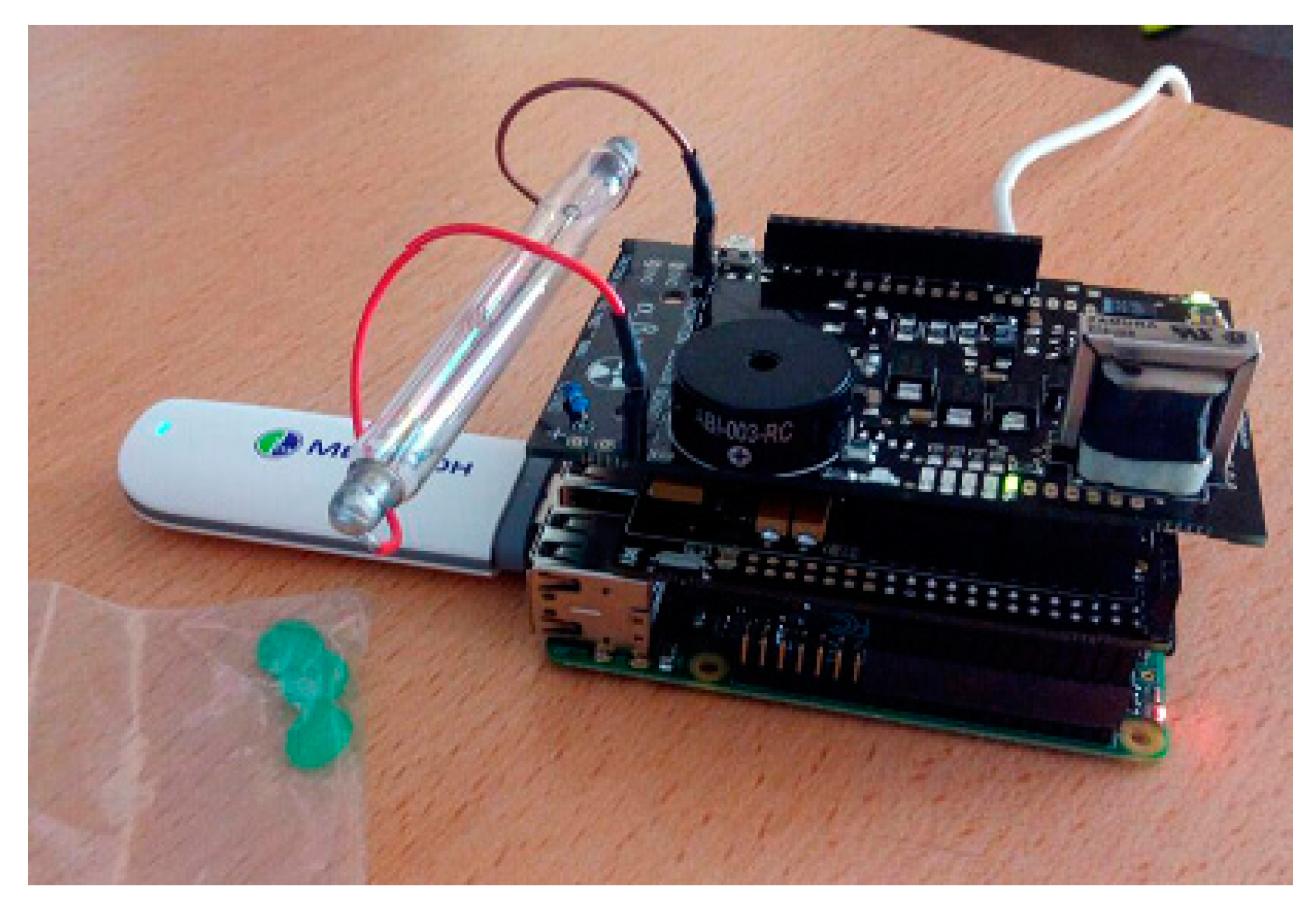
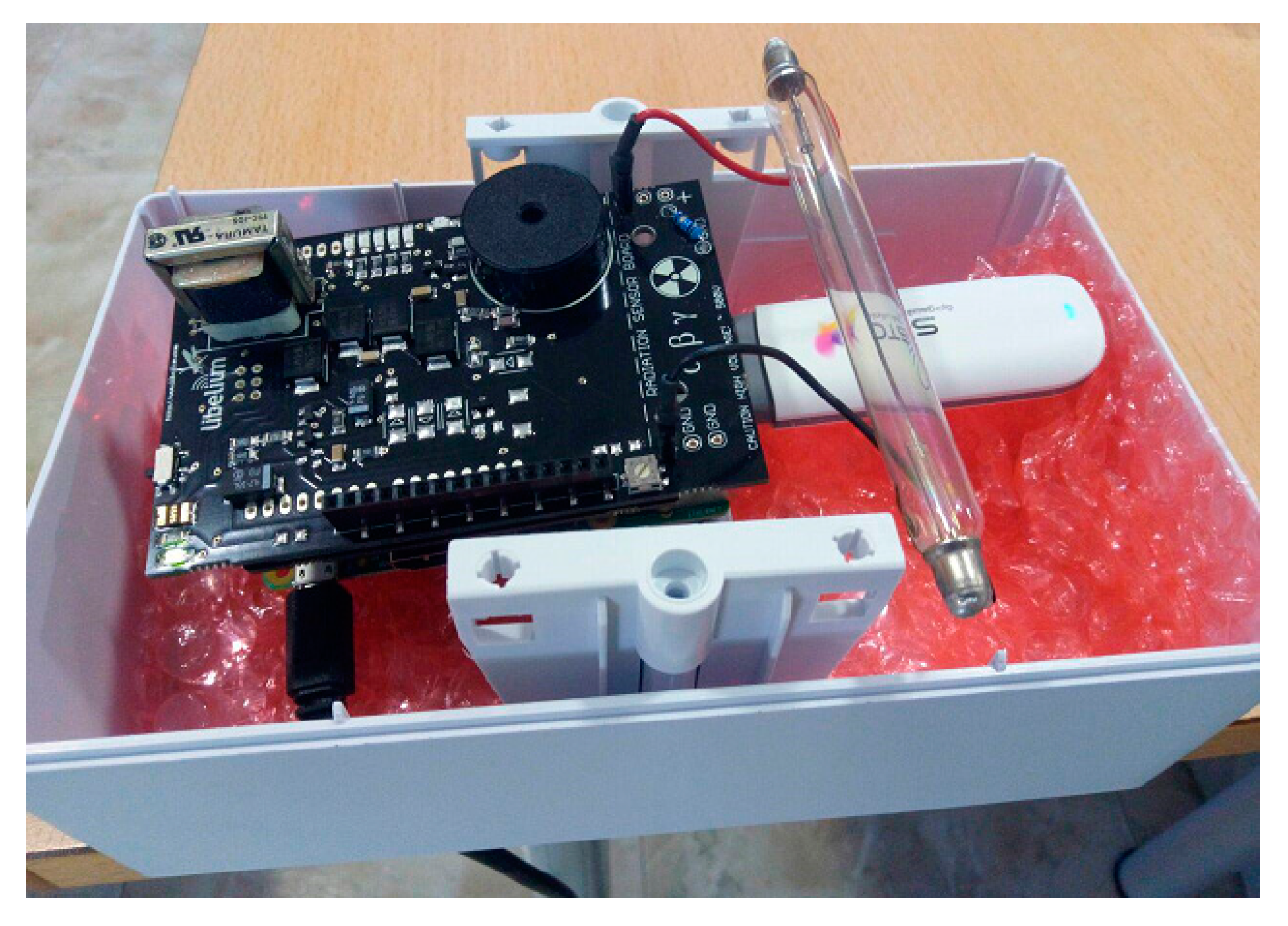
3.3.1. Hardware Description
- A Raspberry Pi.
- The radiation sensor board.
- The Bridge board that connects the Geiger counter to the Raspberry Pi, denoted as Arduino Shield Connection Bridge.
- Raspberry Pi [19]. It is a low-cost embedded board developed by the Raspberry Pi Foundation in the UK. Its size is approximately that of a credit card and encapsulates a Broadcom BCM2835 chip with an ARM processor up to 1 GHz speed. In our work, the Raspberry Pi B++ model has been selected for its low cost and ability to carry out all the functions of our system. Note that a MicroSD card including the operating system (Raspbian), is inserted in the back of the Raspberry, which will be explained later.
- −
- A/V connector power boards to operate (5 V).
- −
- USB ports used to connect the 3G dongle or wireless adapter. In addition, if the Raspberry needs to be programmed, they will be used to connect the mouse and keyboard.
- −
- A General Purpose Input/Output (GPIO) port consisting of 40 pins allows the Raspberry Pi to communicate with external elements. In particular, GPIO pins are managed and handled directly through code from the intermediate Bridge board.
- −
- An Ethernet port joins our system to the Internet.
- −
- An HDMI port connects the Raspberry to a monitor, for configuration tasks.
- Executing the code corresponding to the Geiger counter in order to display/visualize the dose values.
- Connecting to the Internet via Ethernet, WiFi adapter or 3G dongle through USB.
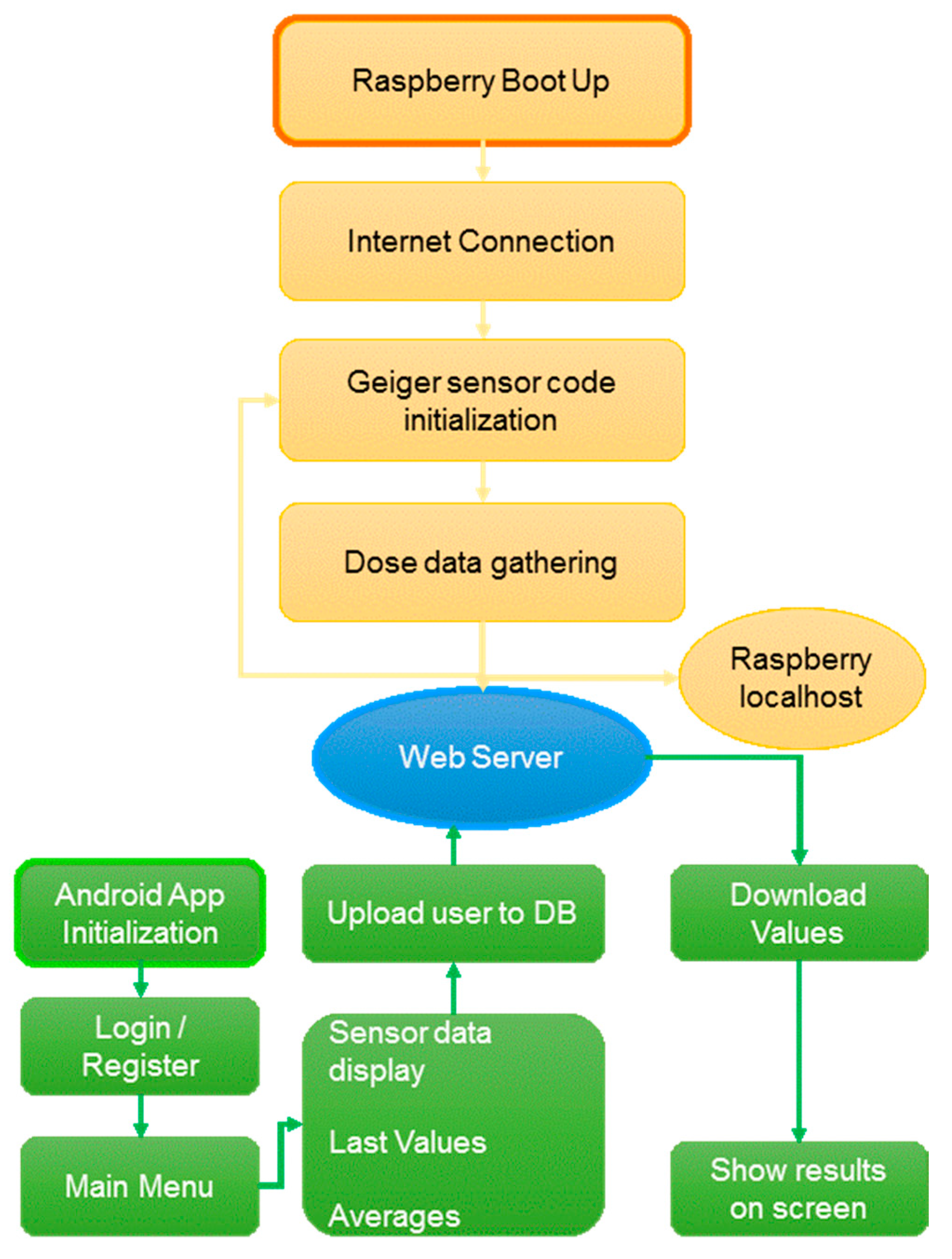
- Enabling the automatic execution of the Geiger counter code and automatic internet connection.
- Running a localhost, including its corresponding database, which allows us to have a backup database.
- Ensuring that collected doses are uploaded to the database on the remote web server every second.
- Raspberry Pi to Arduino Shield Connection Bridge [28]. Since the connection between the Geiger Sensor Board and Raspberry is not possible, an intermediate board or bridge is required. This board is called Raspberry Pi to Arduino Shield Connection Bridge, but for the sake of brevity, we will denote it a bridge board.
- Geiger Sensor Board [18]. This board is responsible for measuring radiation values using a Geiger-Müller tube. The radiation board is composed of two parts: the supply side and the signal side. The supply side is responsible for ensuring the high voltage required by the Geiger-Müller tube (400 V–800 V). The signal side adapts the output analog pulses from the GM tube to digital data understandable by the Raspberry Pi.
- 3G dongle. When connecting to the Internet via 3G, it is necessary to put a 3G dongle into the interface USB of the Raspberry Pi. Although there are several models compatible with Raspberry Pi, the selected dongle [29] together with a prepaid card have allowed the use of the device anywhere in the hospital environment. In addition, in the specific case of not having access to WiFi or Ethernet in the hospital under study, or when the system was verified at CND, the use of the 3G dongle has been essential to dispatch the captured radiation data to the remote web server.
- WiFi Adapter. This component is placed in a USB port, providing access to the Internet thanks to the WiFi hospital infrastructure. It should be noted that our device ensures an Internet connection (and therefore, the dose information for each user in the remote web server) by selecting of one these technologies: WiFi, 3G and Ethernet.
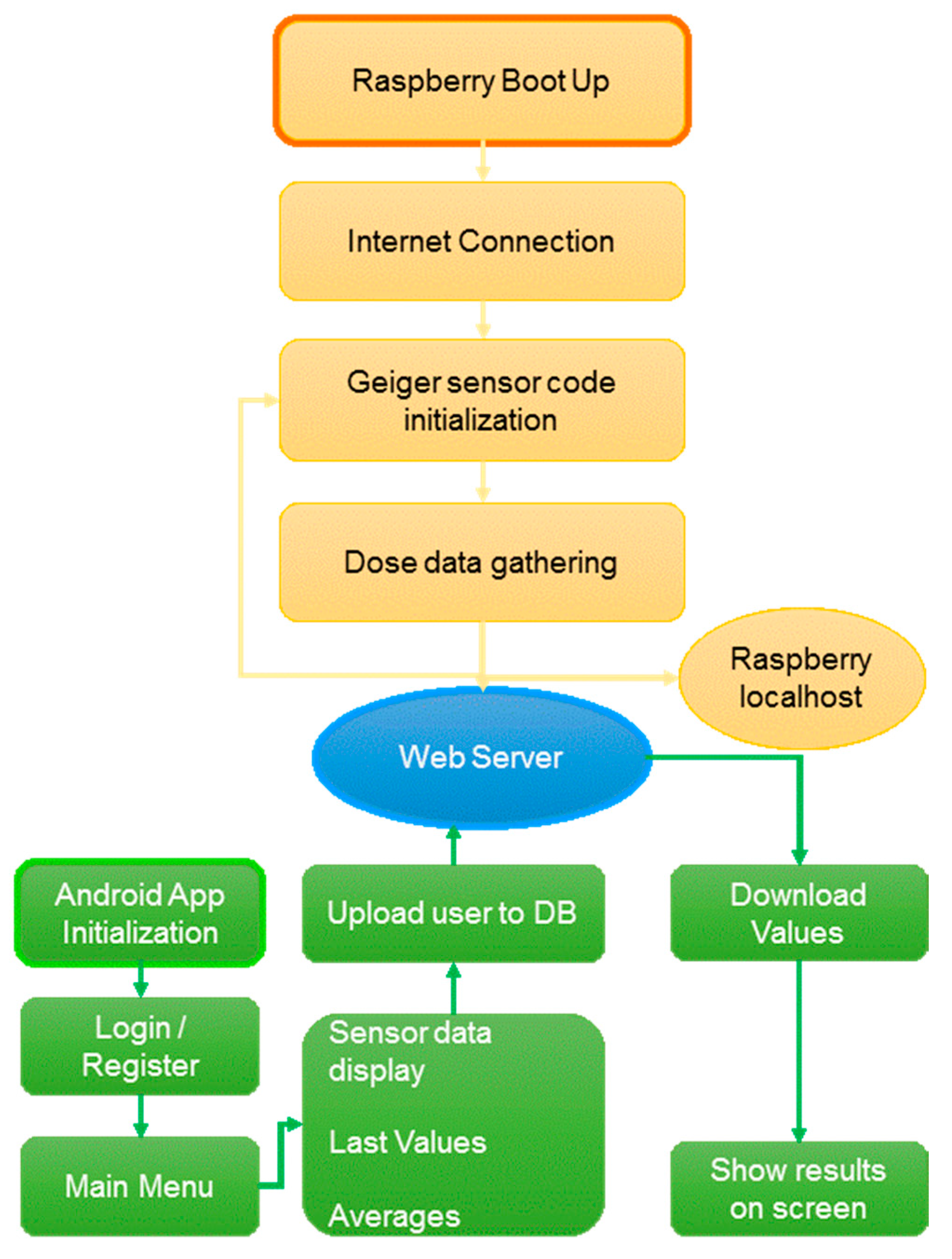
3.3.2. Software Description
- Operating System. The operating system (OS) for Raspberry Pi is denoted as Raspbian. In particular, Raspbian Jessie was the version installed, because it offers multiple functionality and documentation in terms of capturing data and communication issues.
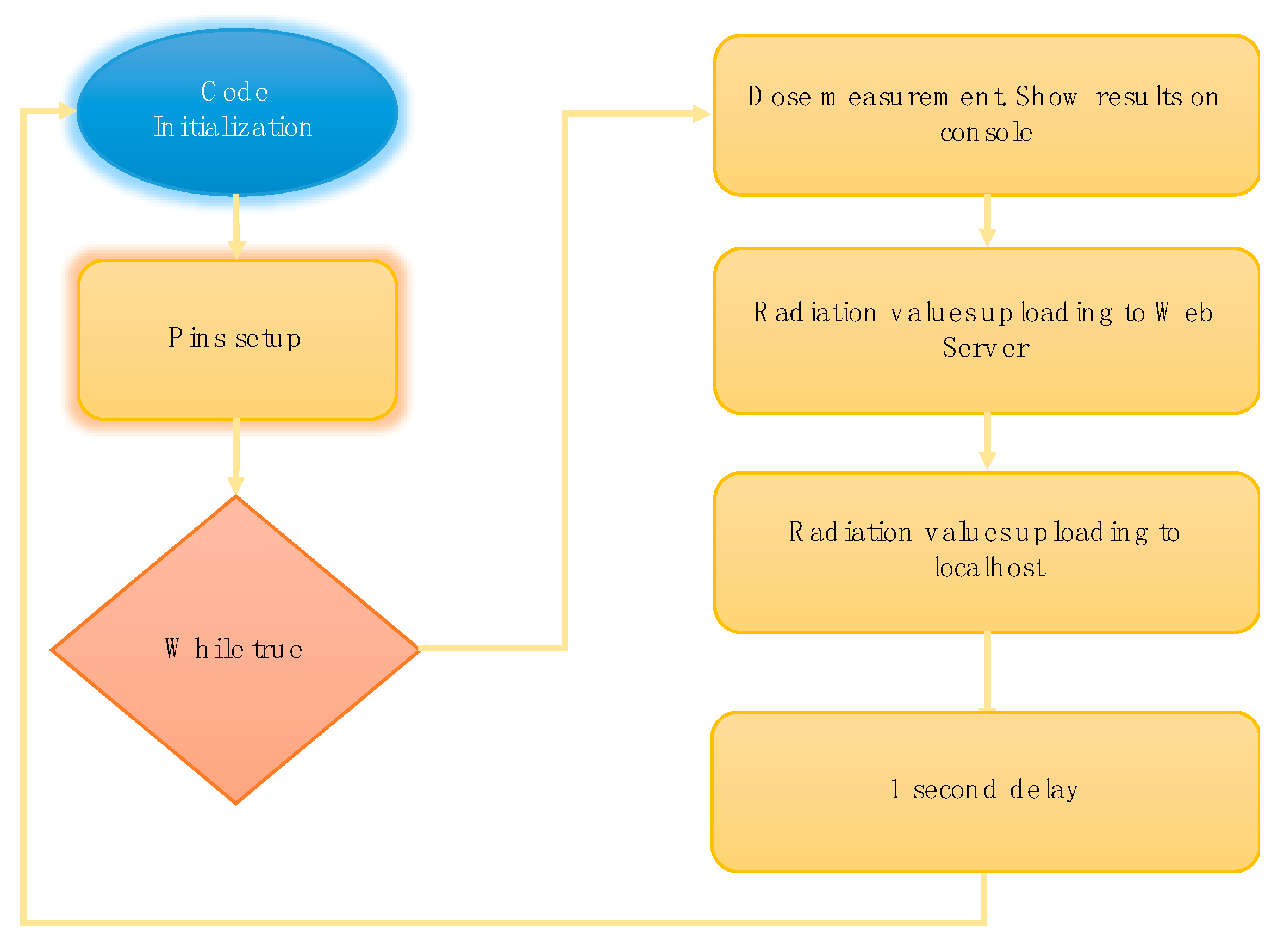
- Geiger sensor code. This code, implemented in C language, quantifies the counts per minute and equivalent radiation measured by the GM detector on the board. Raspberry Pi executes the programmed code obtaining the dose data from the Geiger detector through its GPIO pins. Since the sensor uses the same connections as Arduino, it is necessary to include the arduPi library codes provided by the manufacturer.
- 3.
- Servers. A server is required to store the dose data collected by the device. The one selected for both the remote web server and the localhost is Apache [30], which is a free-service and open-source HTTP server with the same features as other high-cost competitors. The Apache web server is responsible for storing the GM-captured radiation data and managing them in an Android application. In this case, the Android application accesses this server, both to log in or register a new user, and to display the radiation measurements/statistics. The remote web server requires Internet access, so, it must have a domain and therefore, a public IP address. In a certain way, both the device and the Android application connect to the server through this public IP. Under this premise, note that a web server allows us to access data anywhere. Using the Android application or a PC, we check the radiation values at any time and place, even if the detector fails or turns off. This also allows us to control the login and registration of users, avoiding, for instance, that two different users employ the same user name. The Apache localhost is configured as a backup service, lacks an Internet connection, and data are recovered via USB.
- 4.
- Database. They are responsible for storing both radiation data from the GM detector and information from user registers. PhpMyAdmin [31] has been selected as the tool to generate database, both in the local server and the remote web server. PhpMyAdmin written in PHP ensures the database management and handles the MySQL facilitates. For instance, the user can create/delete databases, generate/delete/modify tables, delete/edit/add fields, execute any SQL statement, handle keys in fields, manage privileges, and export data in various formats.
- 5.
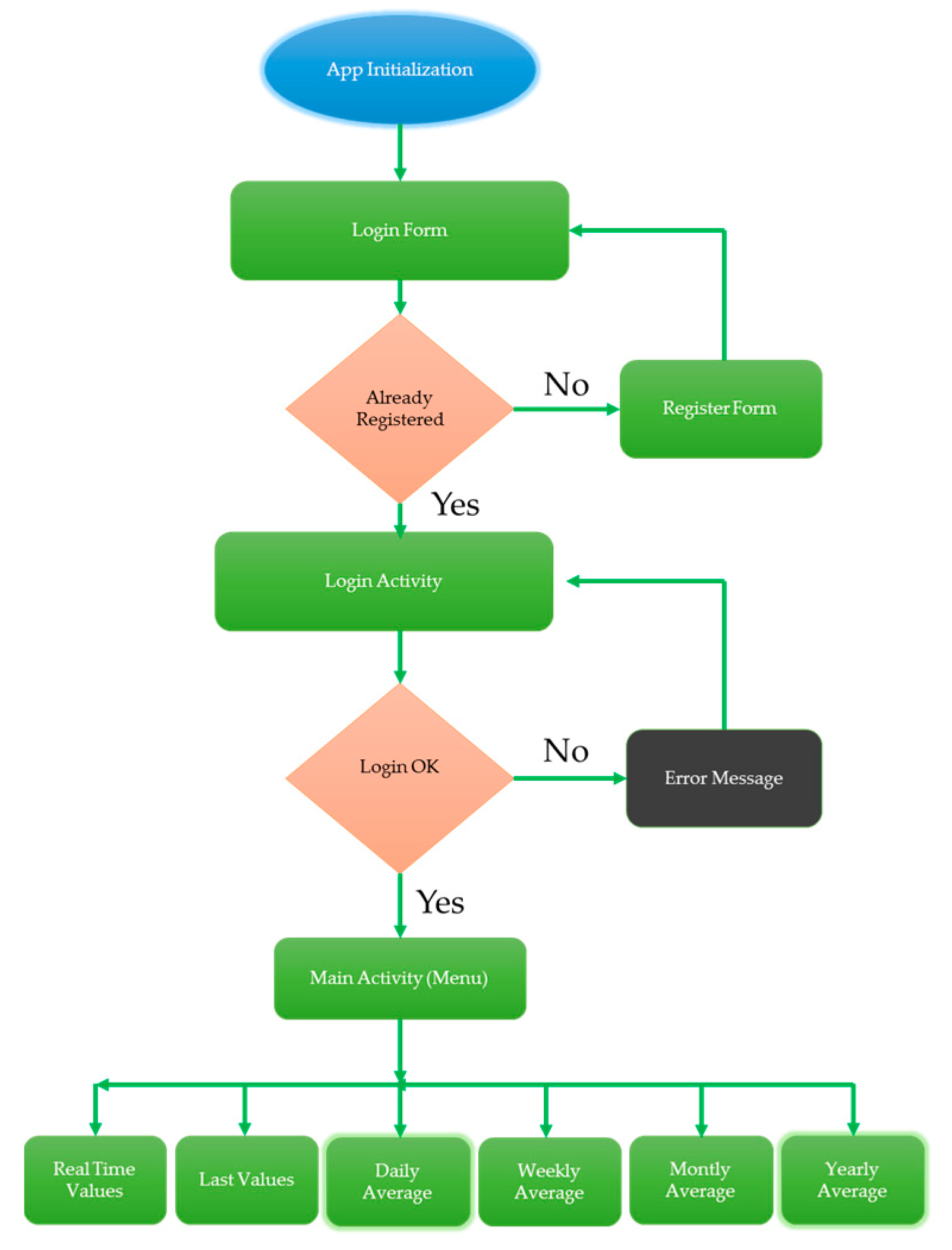
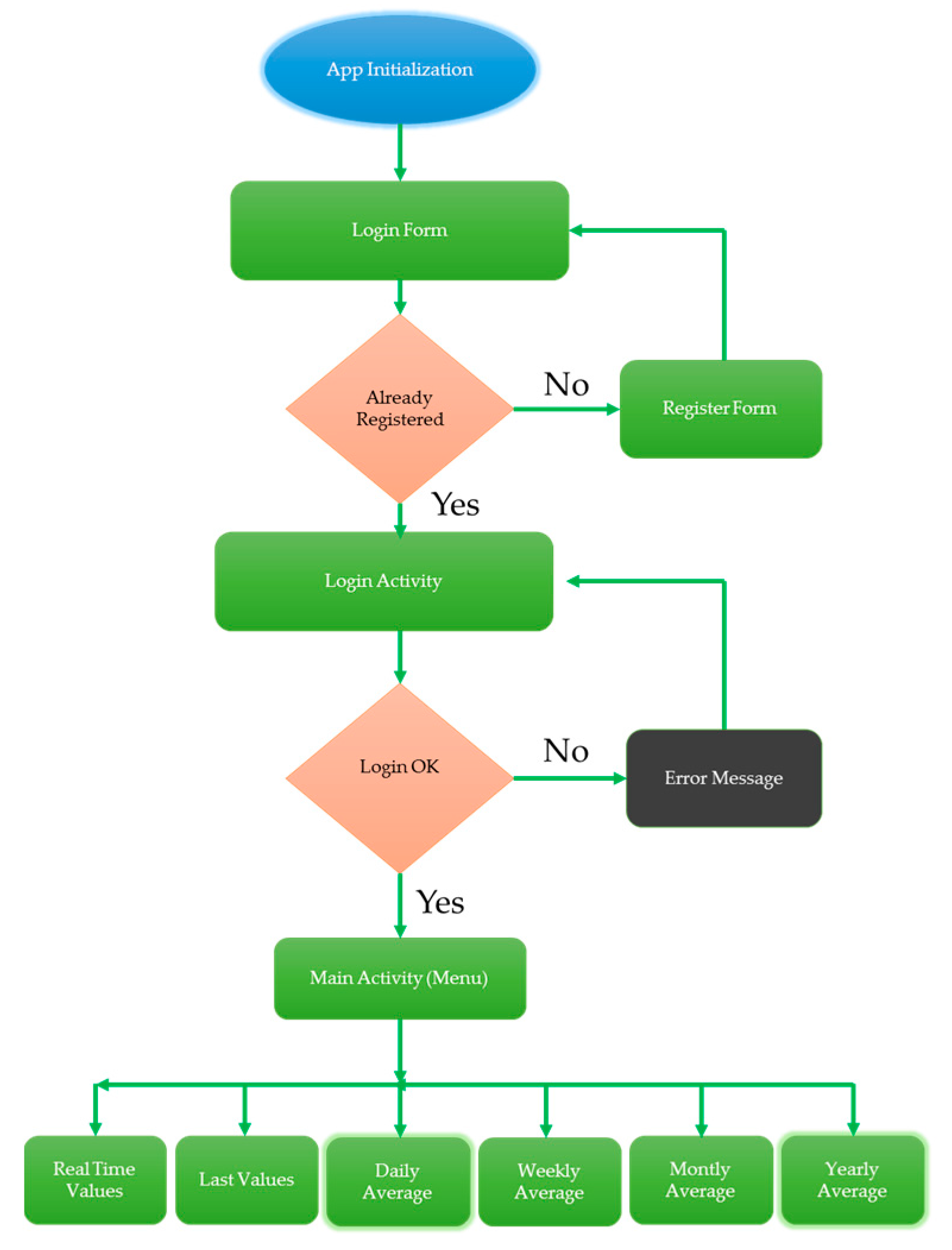
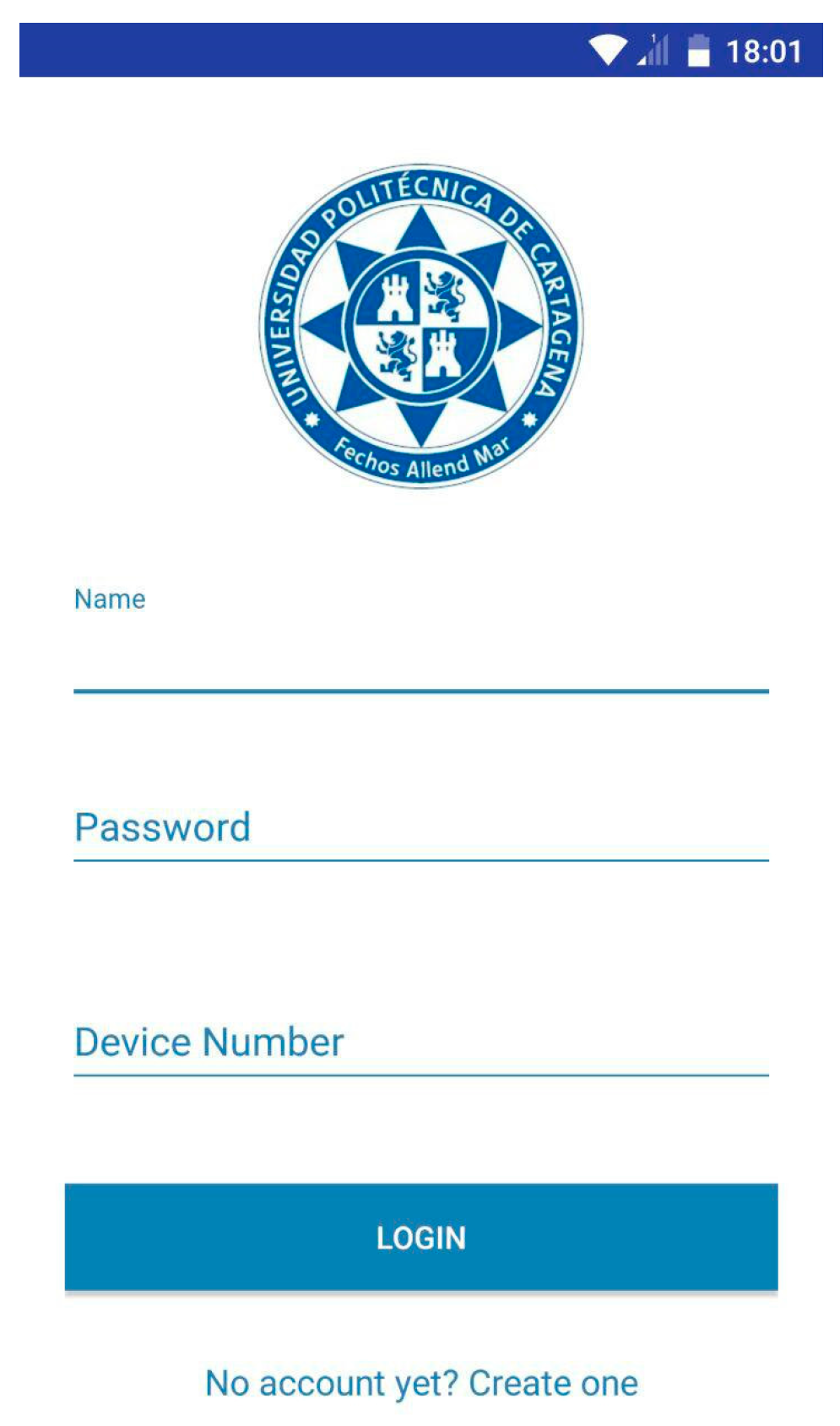
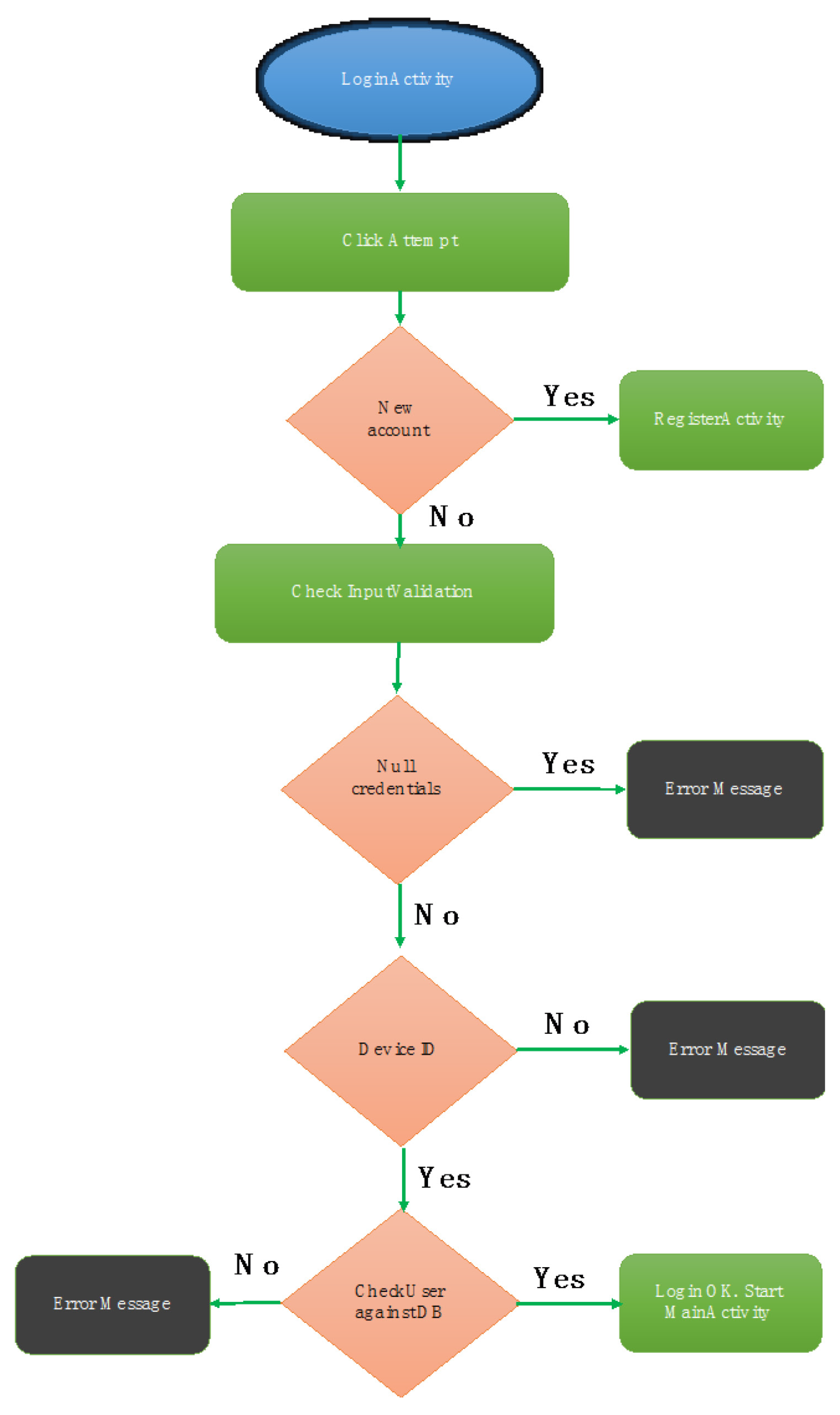
- Android application. The application developed for smartphones is in charge of displaying all the radiation results captured by devices. This application has been implemented in Android because, among other factors, it is an open source. Furthermore, Android makes the simulation and testing of different versions of our application on different devices easier, without the requirement of them having been previously developed in emulators. The development of the app is divided into two main parts: The appearance, focused on the graphic interfaces and the specific functions of each of them.
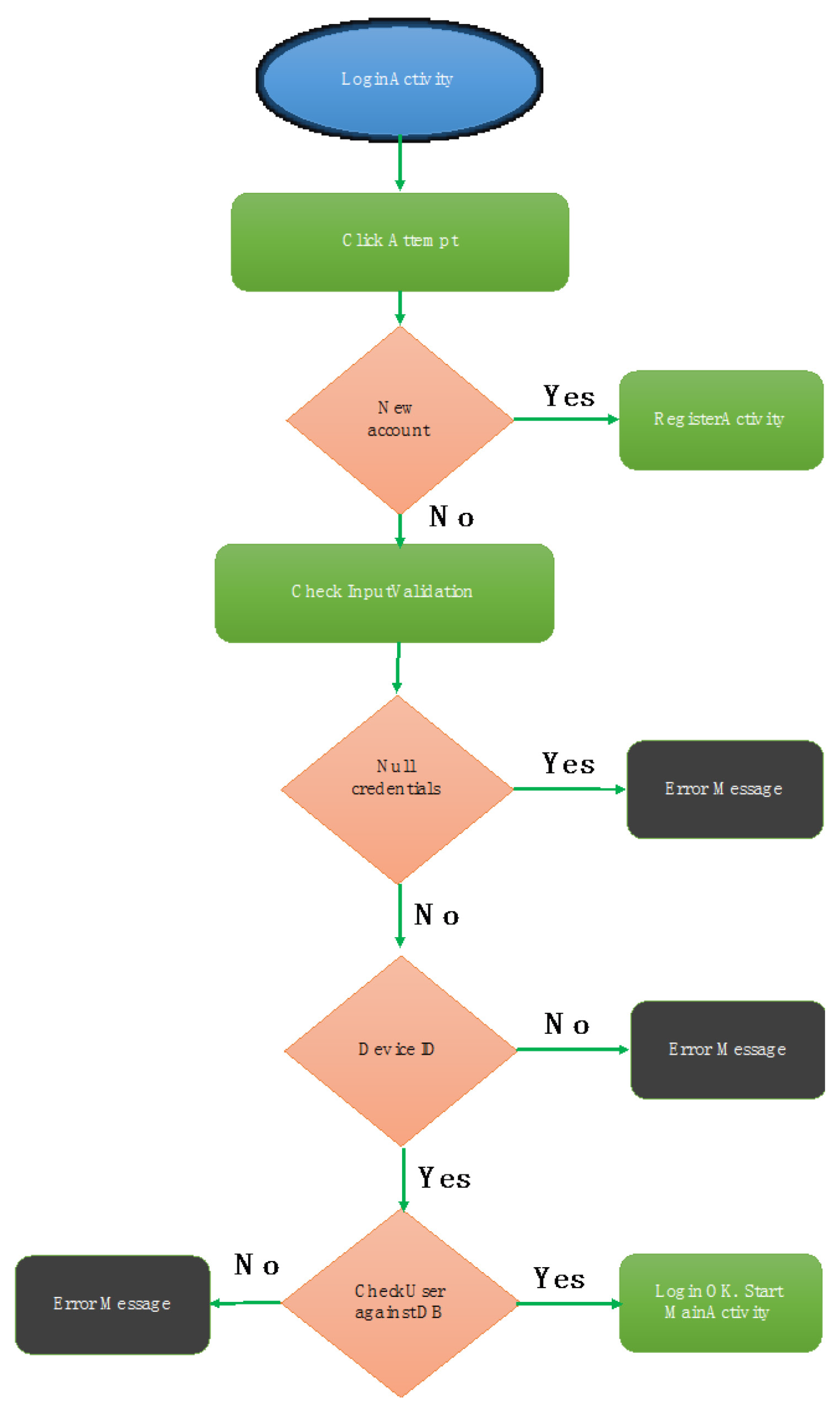
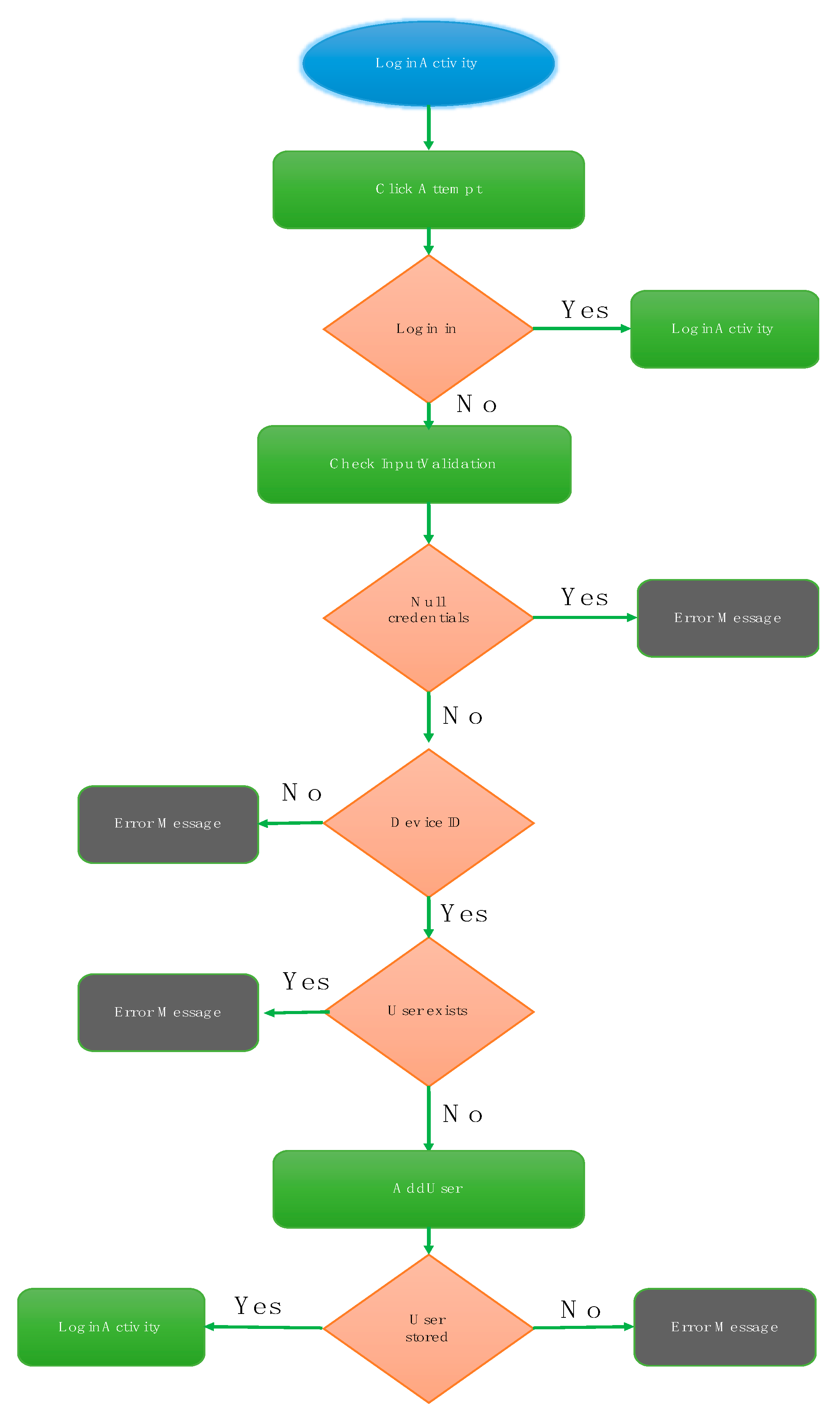
App Initialization
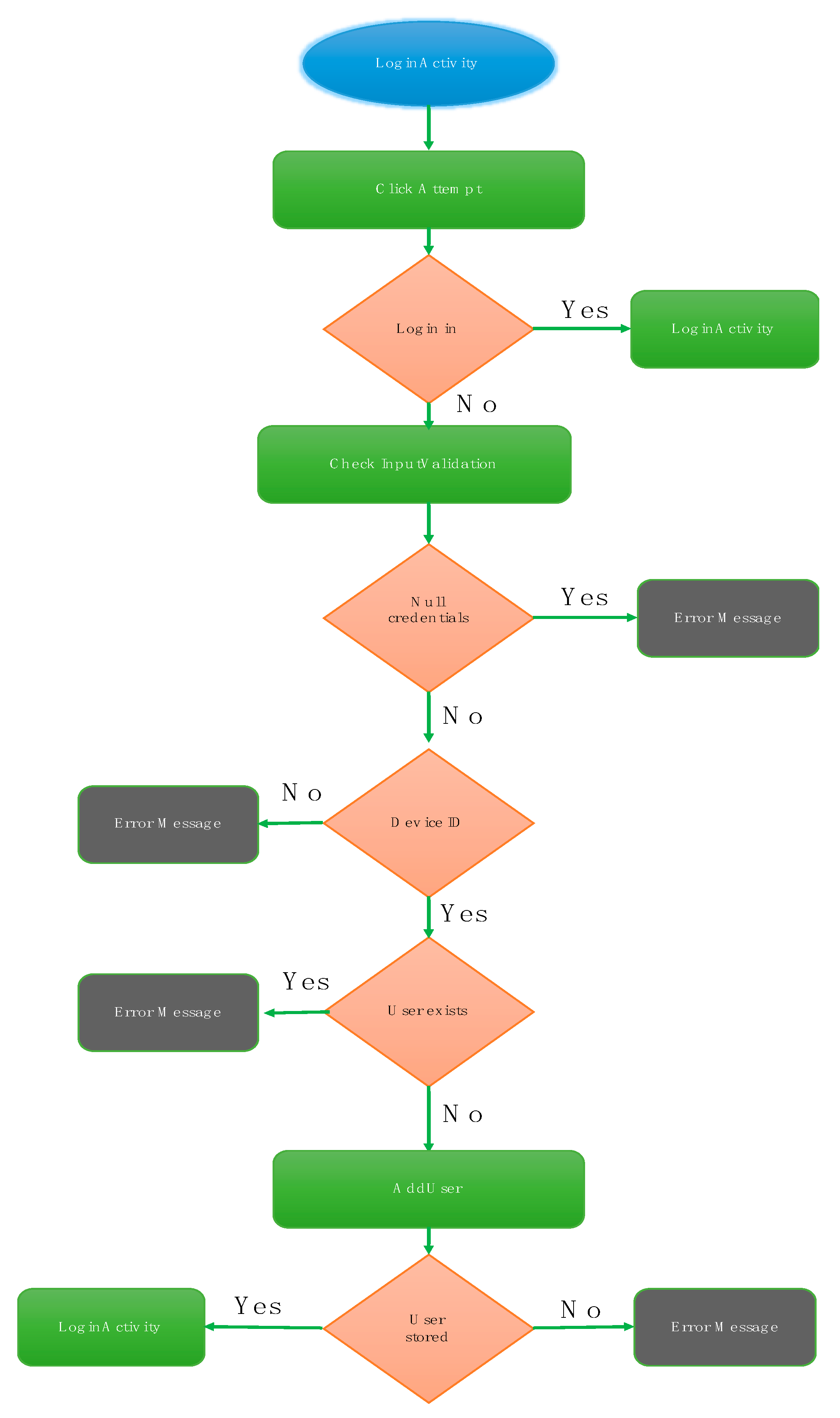
User Register
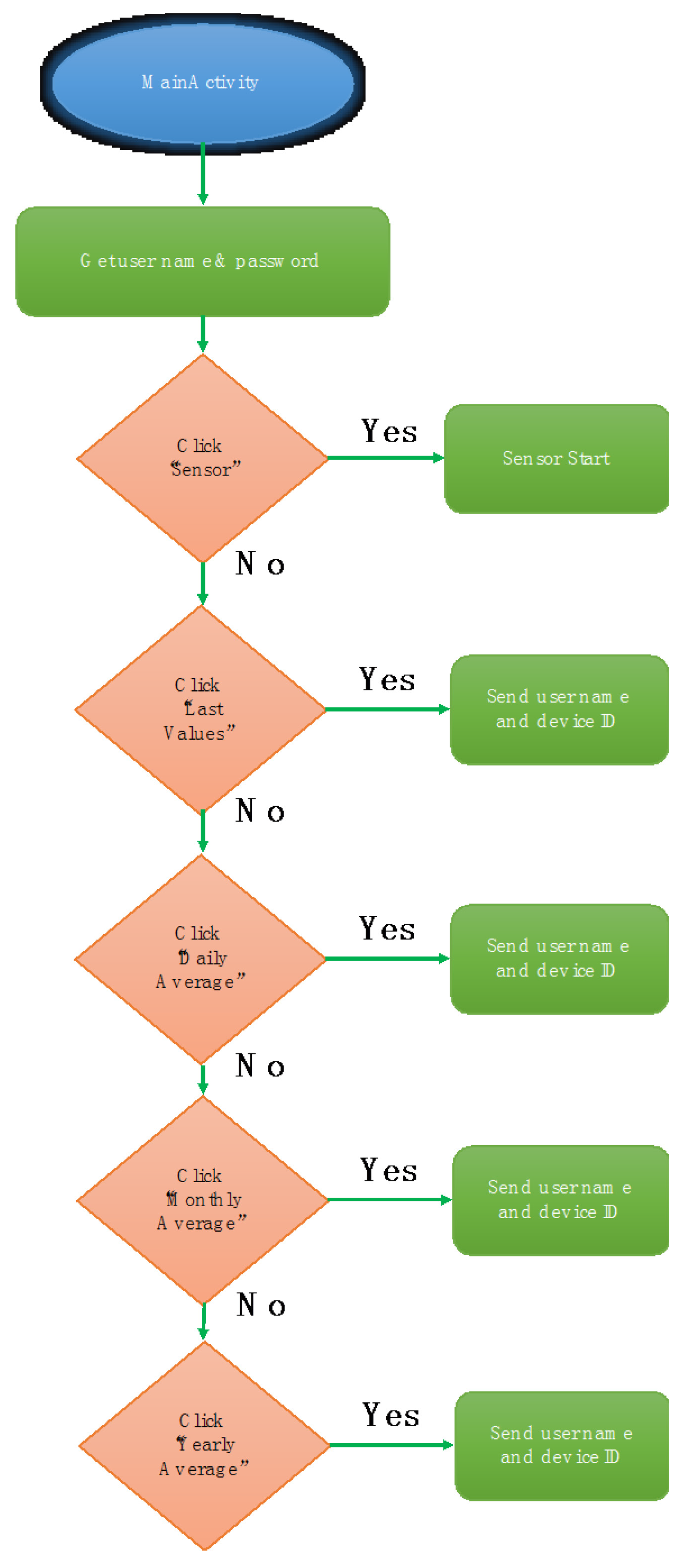
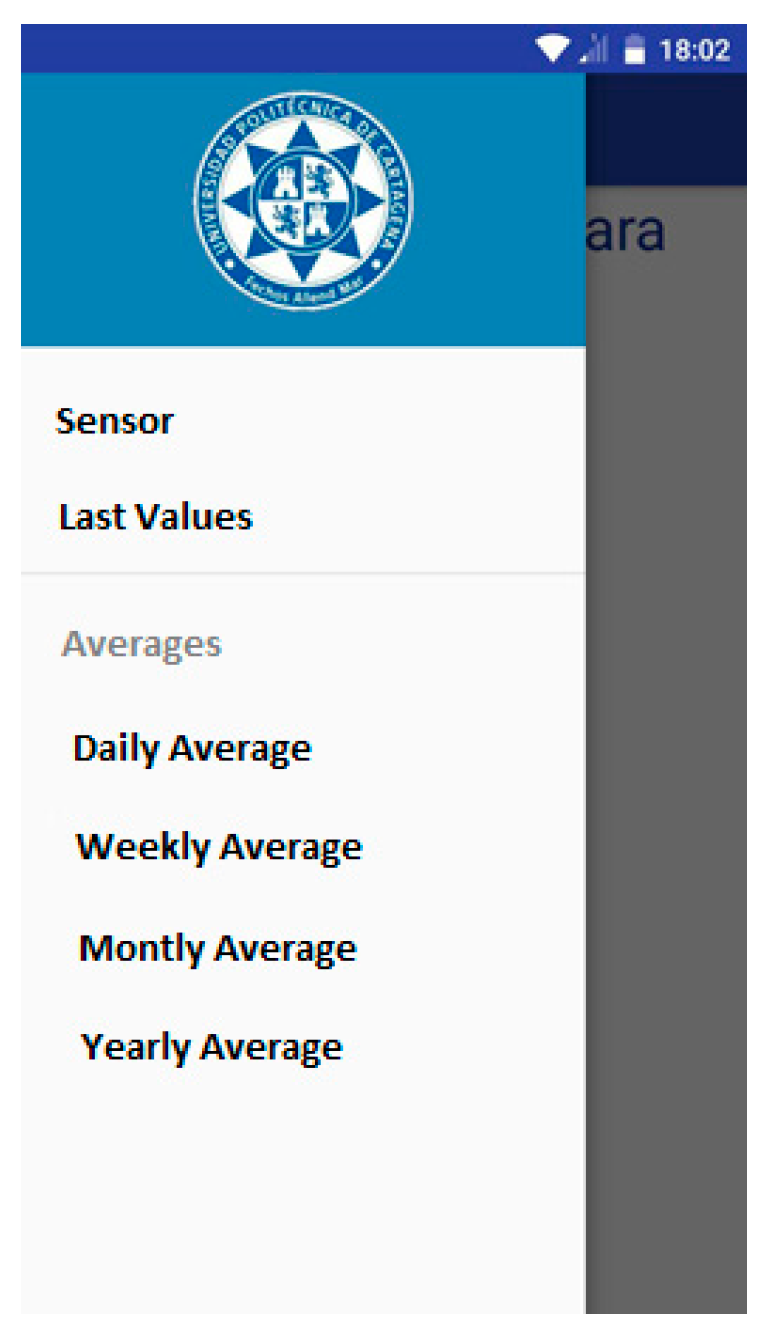
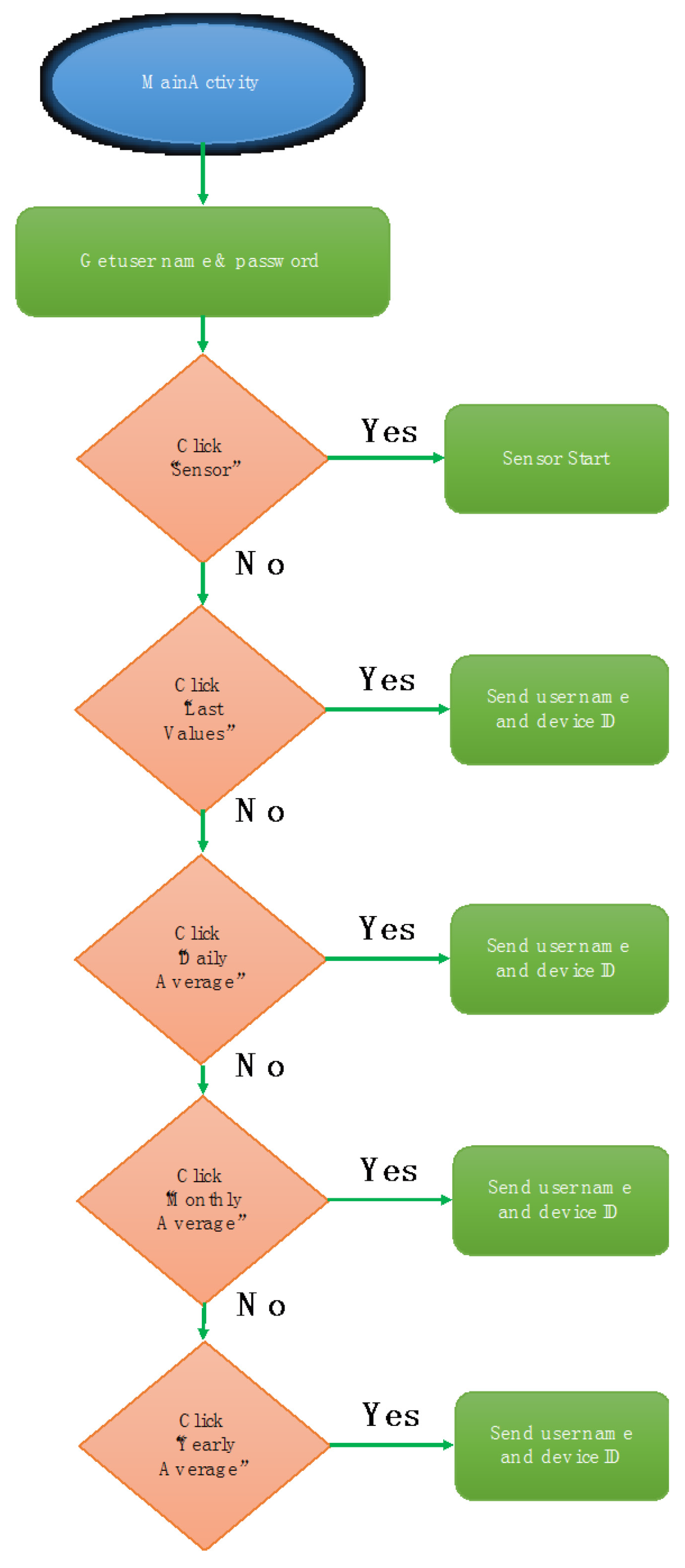
Main Menu
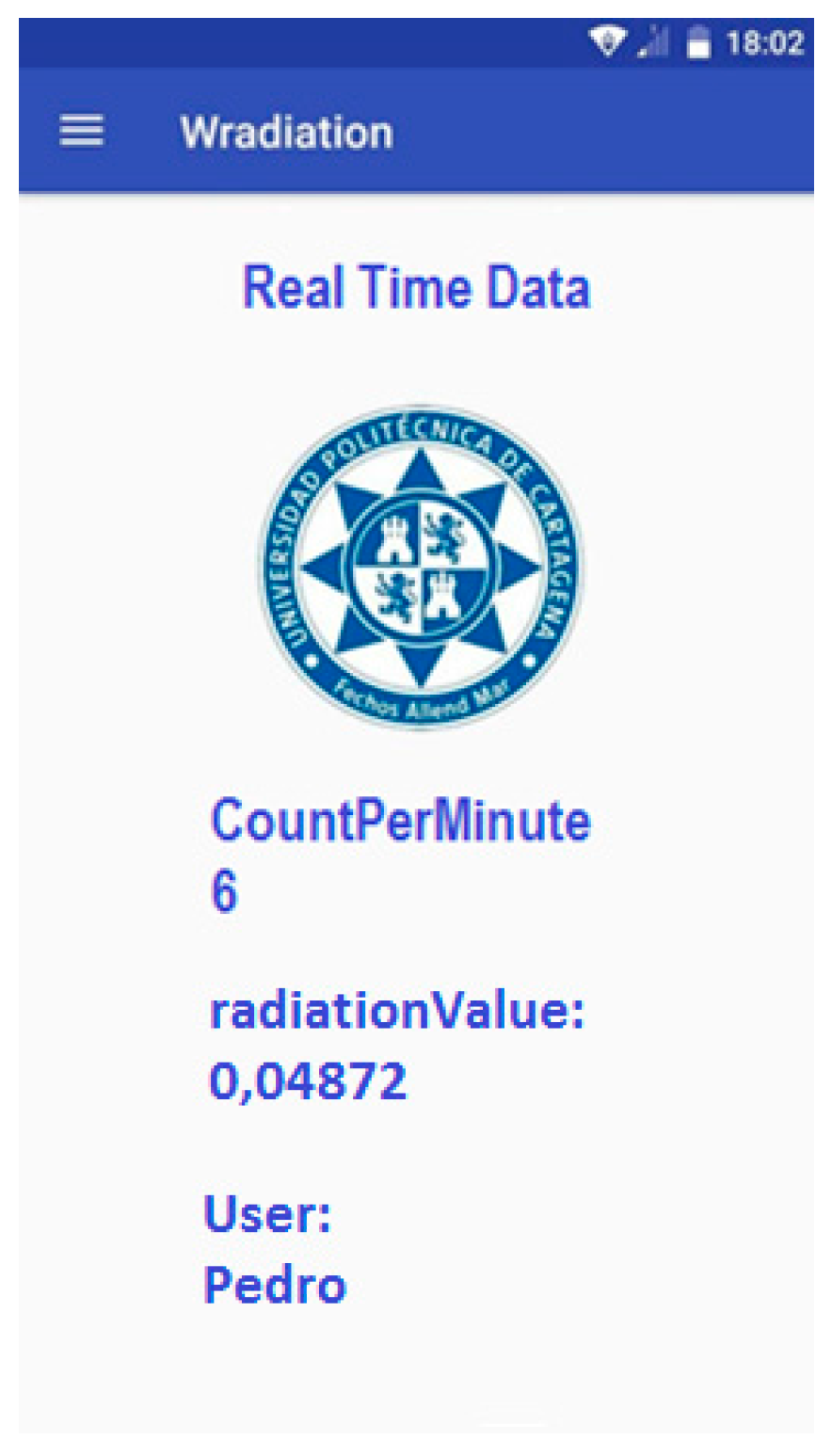
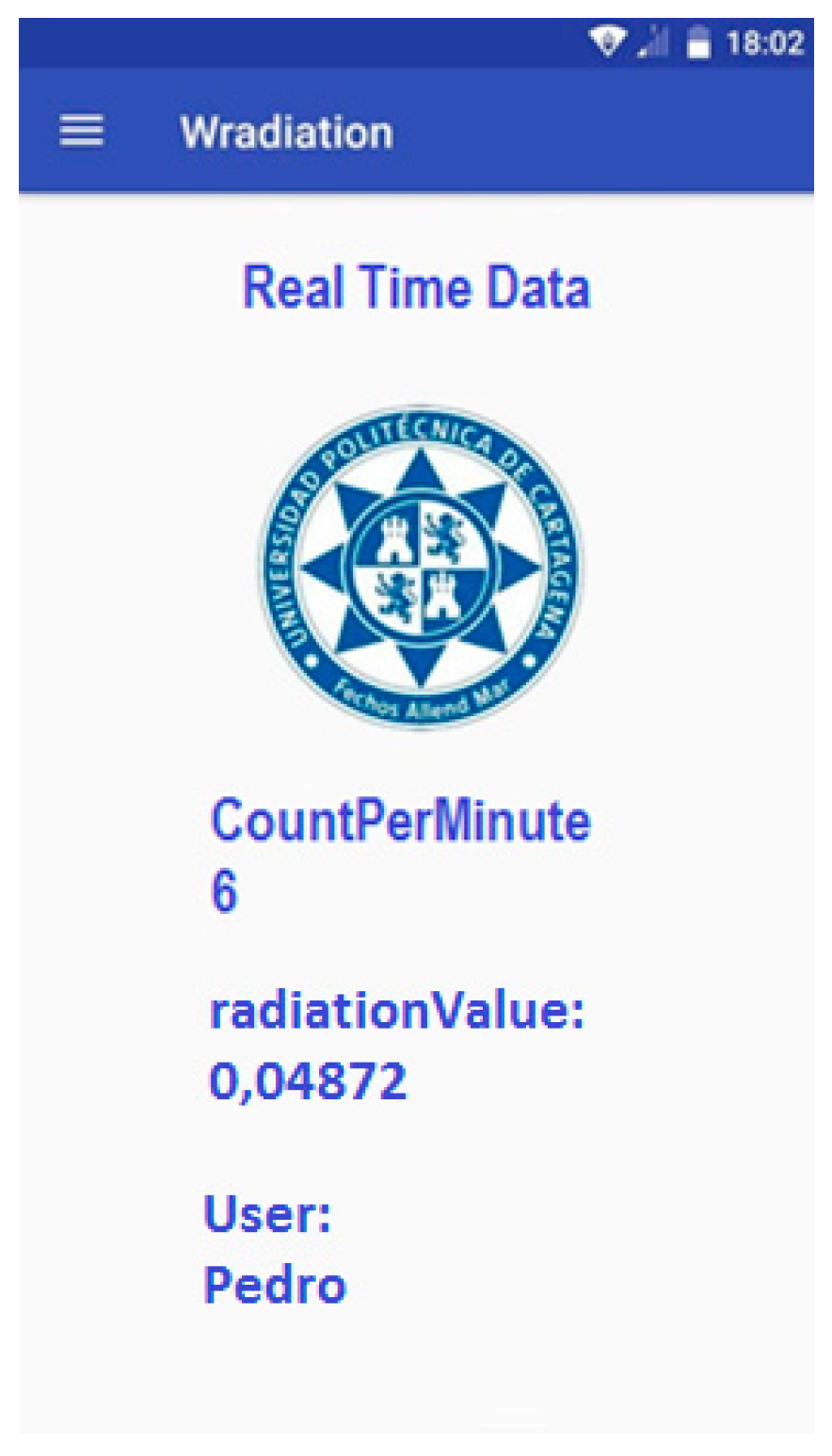
Sensor (GM Detector)
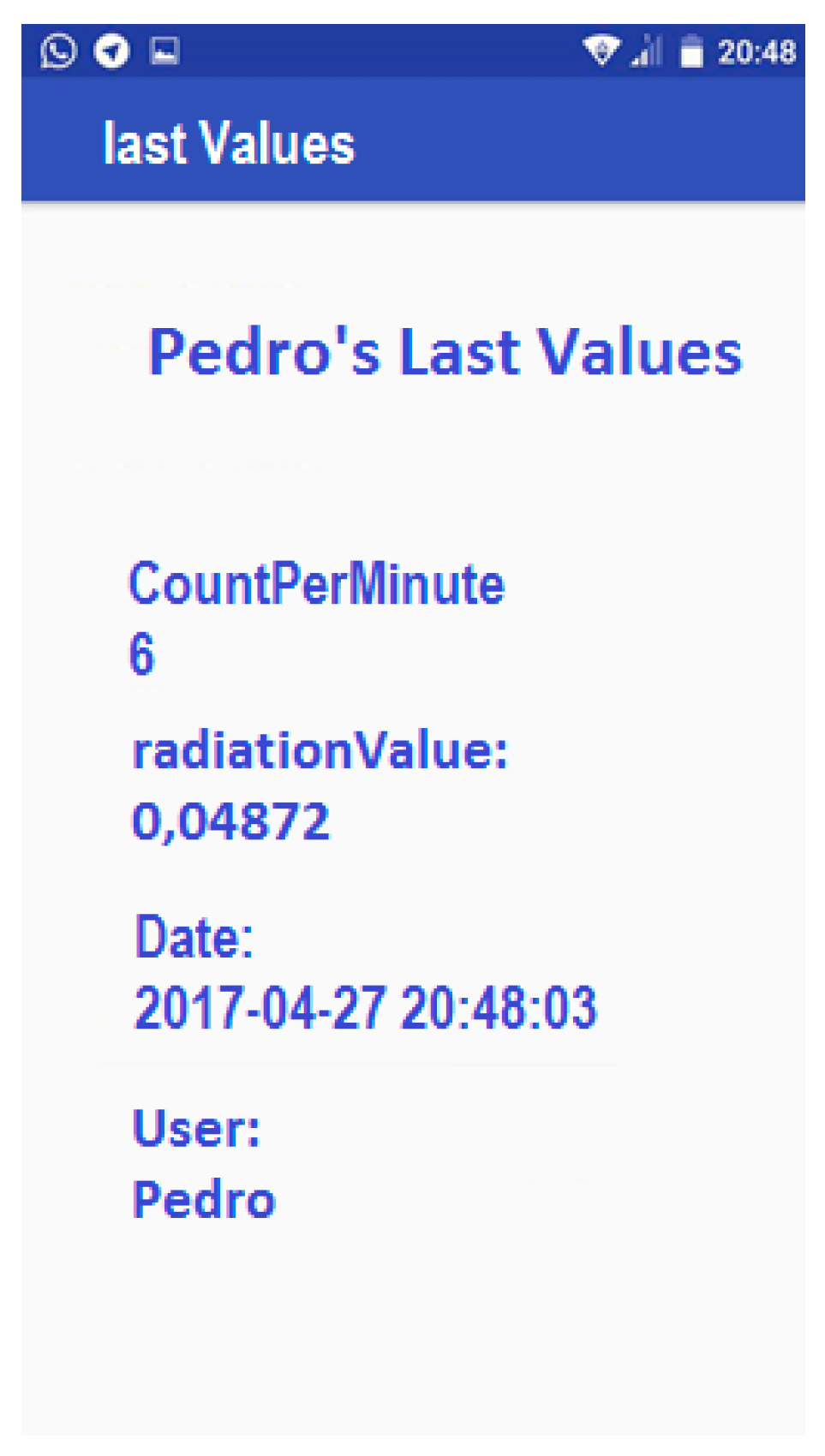
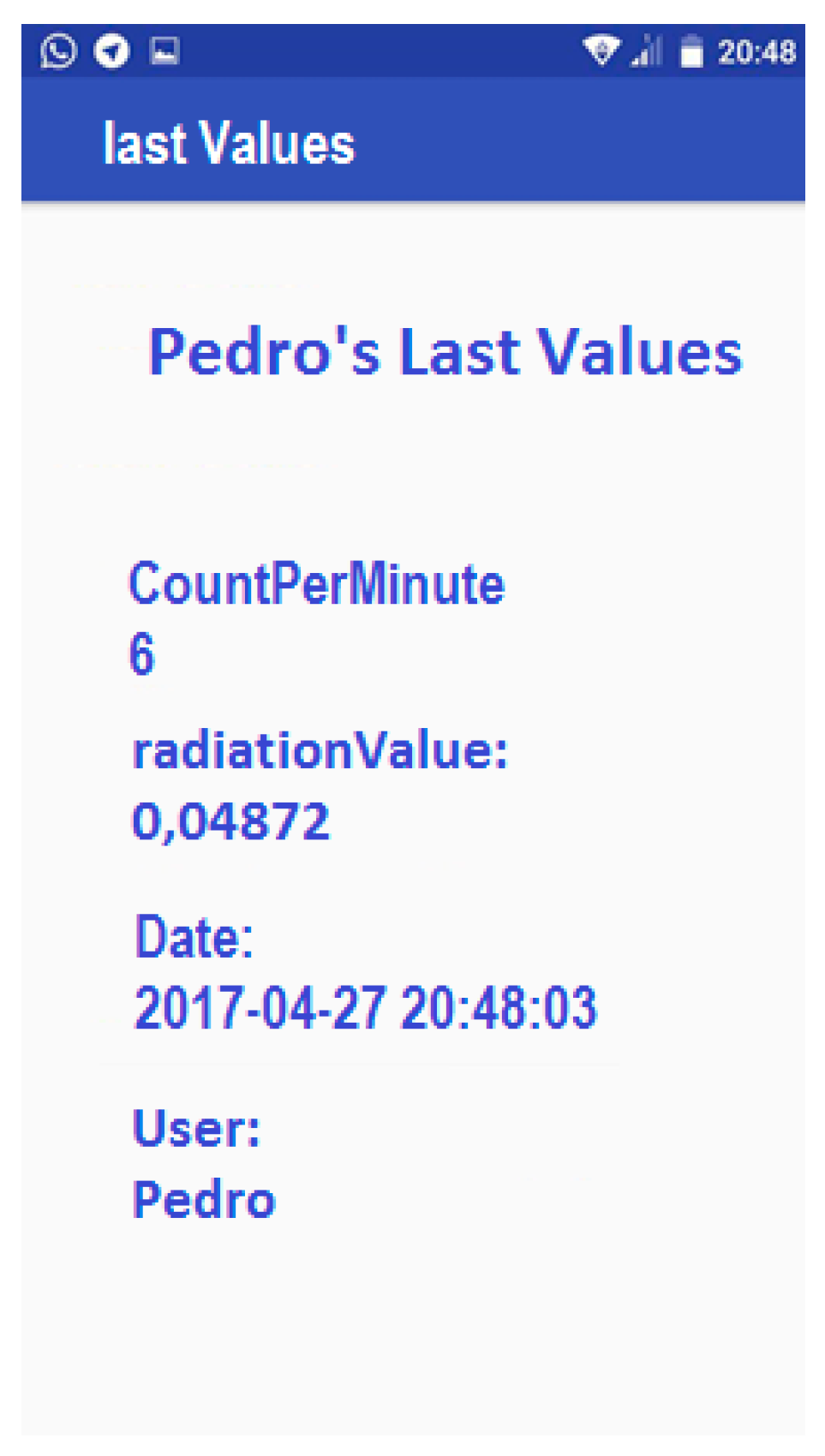
Showing Last Values
Statistics
4. Verification of the Device
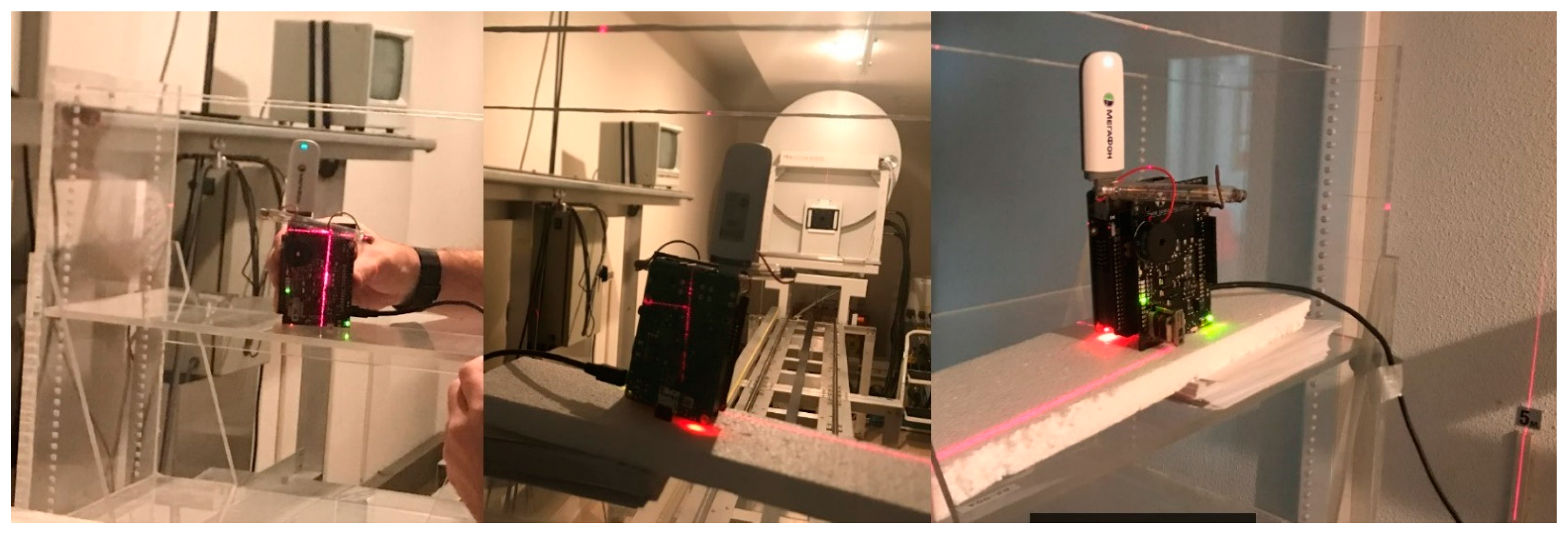
4.1. Verification Procedure
4.2. Verification Results
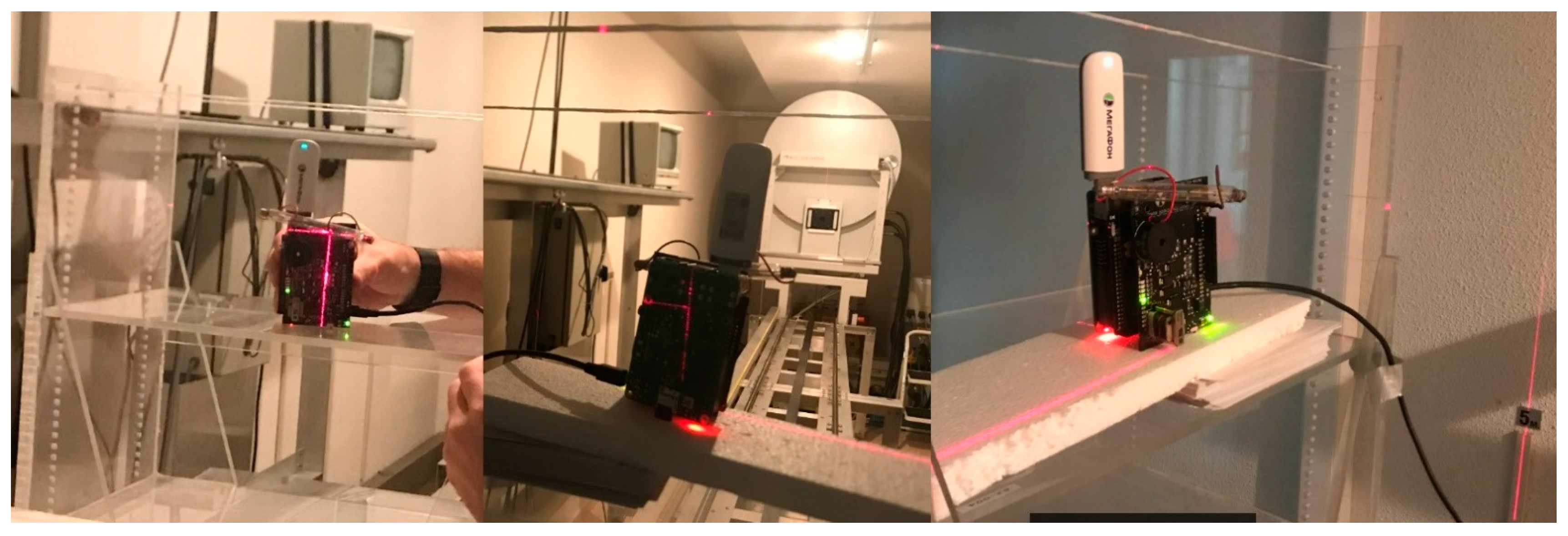
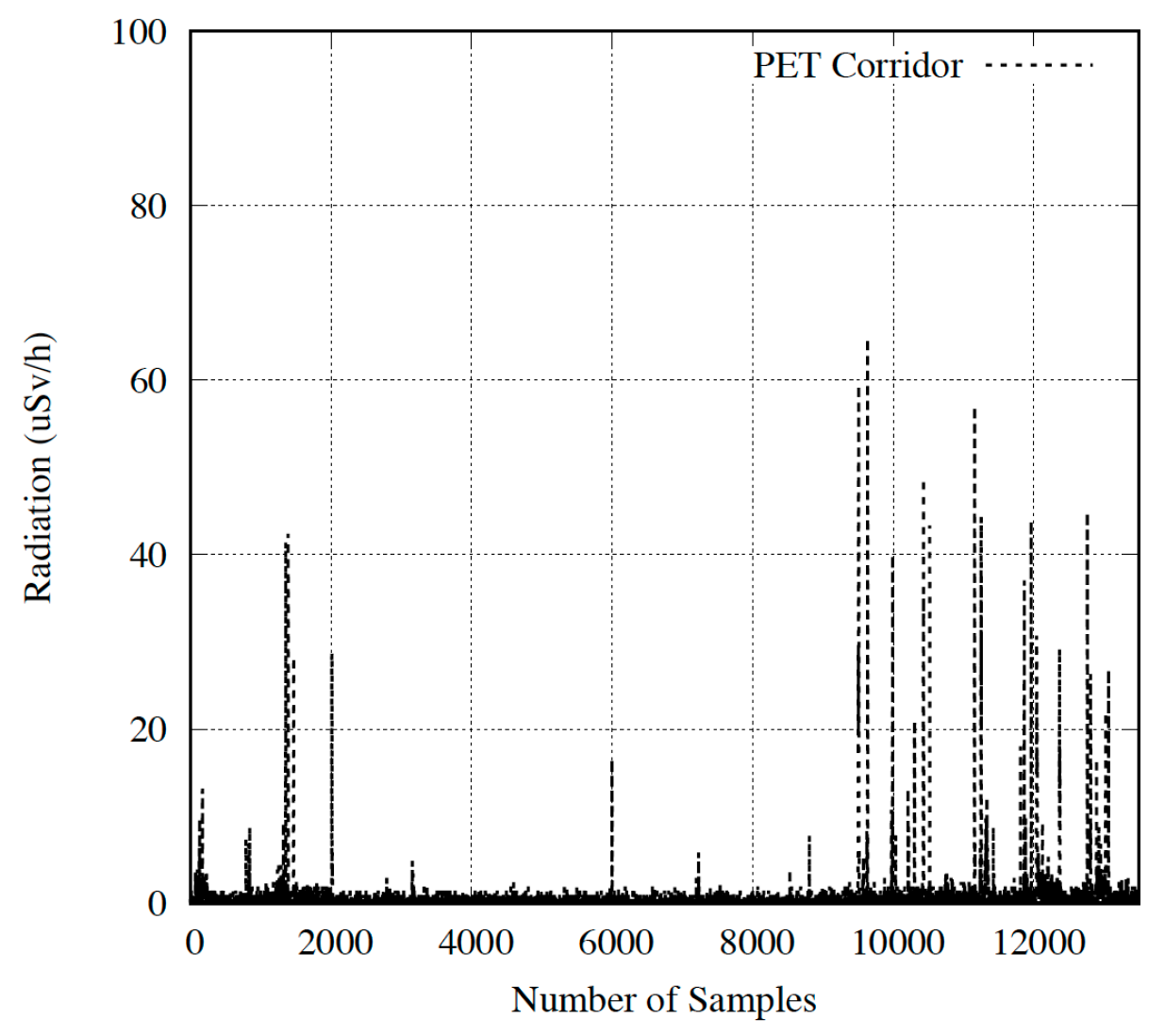
5. Performance Evaluation in the Hospital
Result Discussion
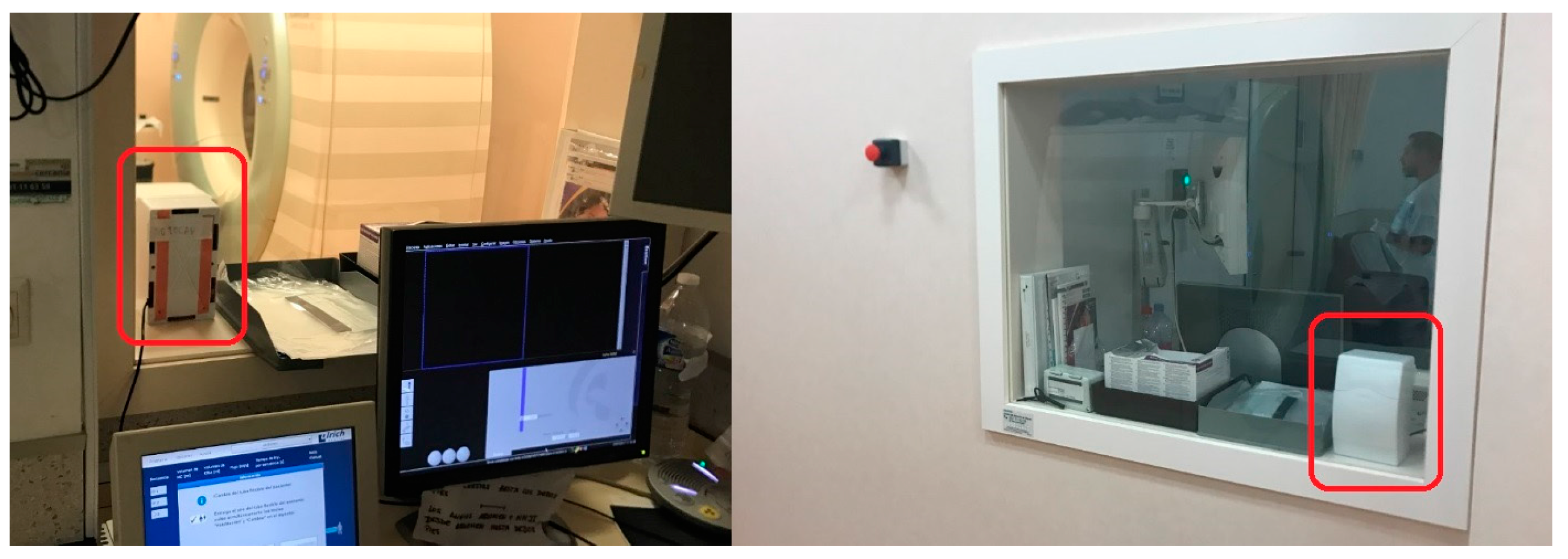
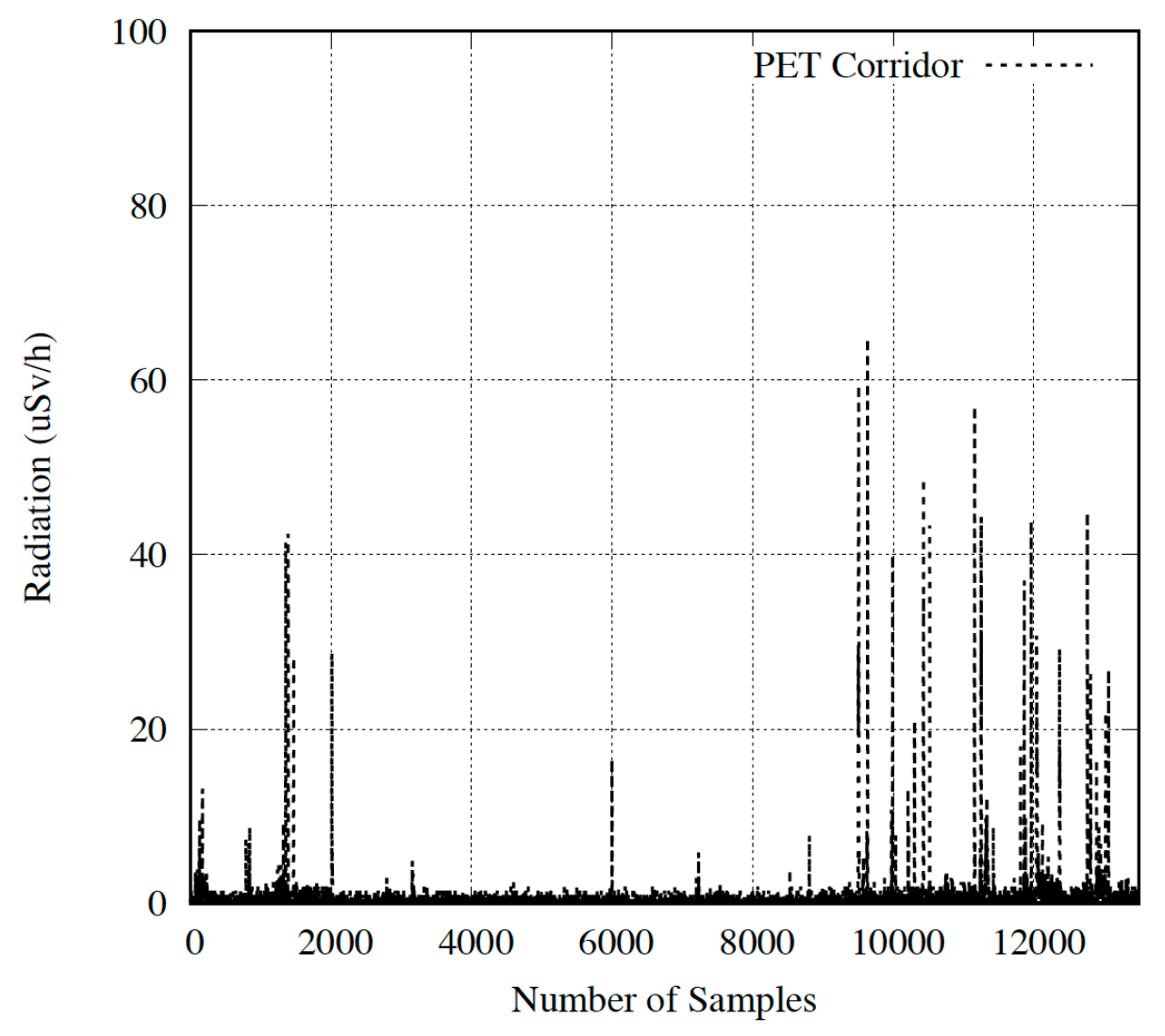
Device Located in the Corridor
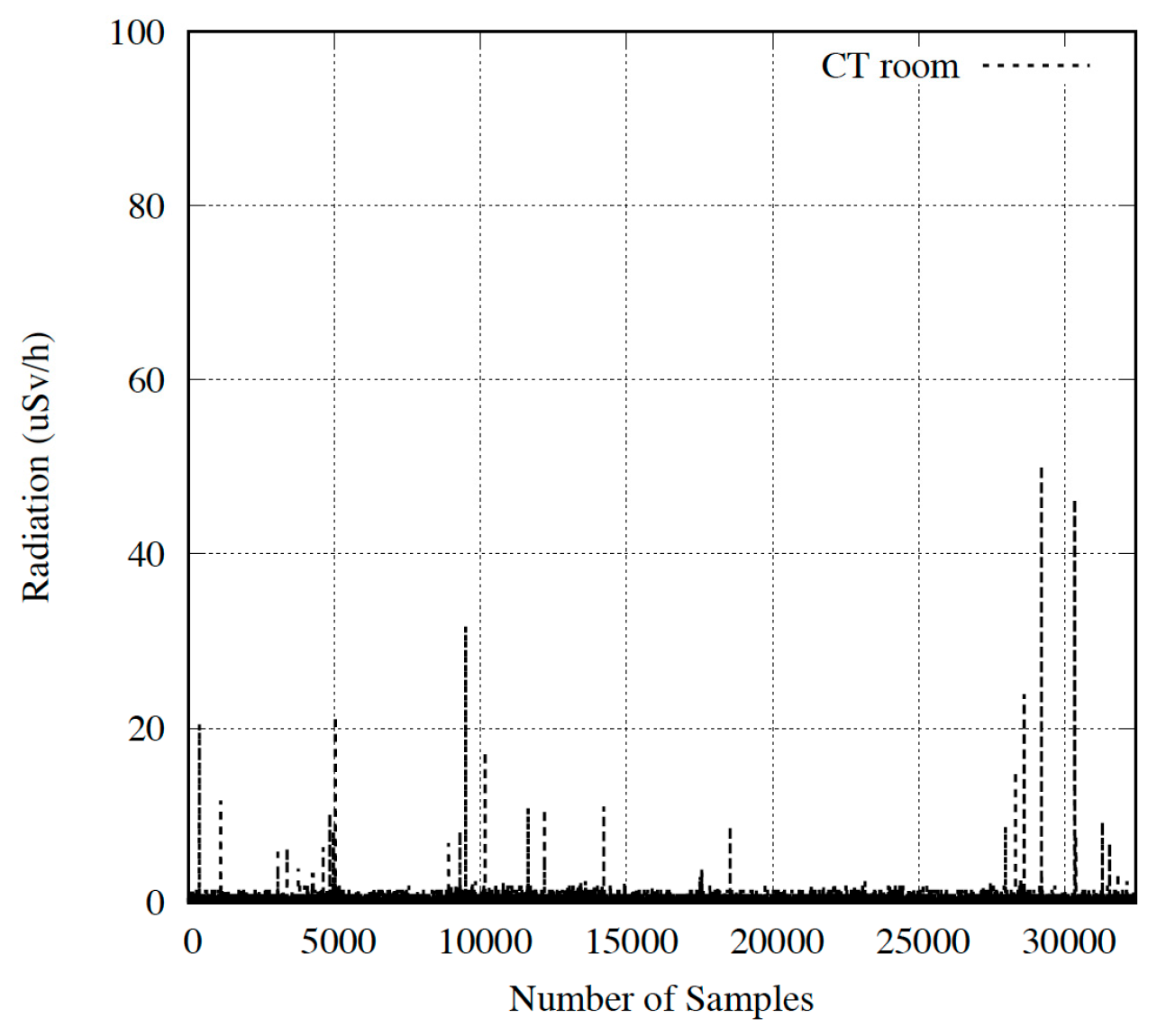
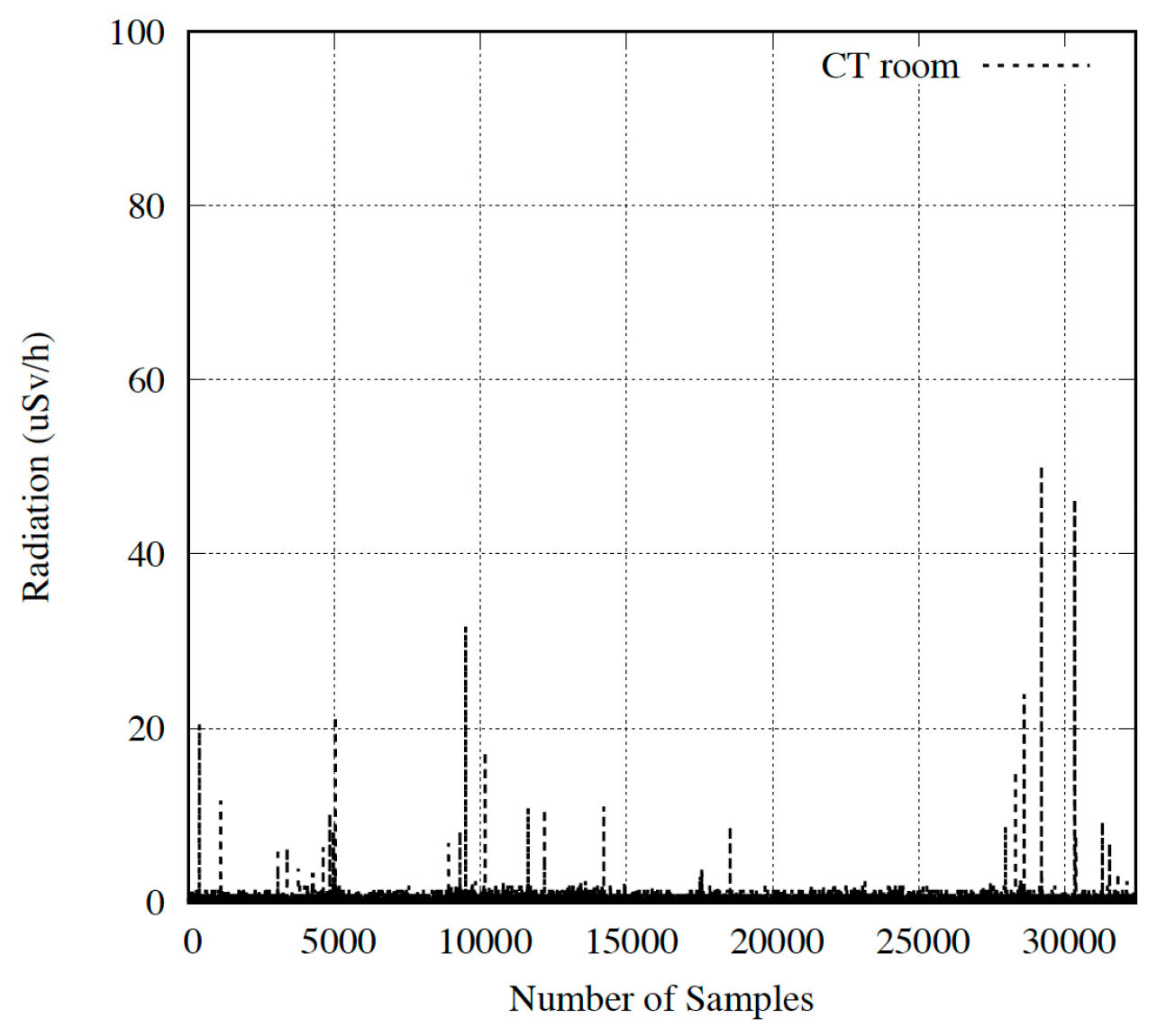
Device Located in the Room Next to CT System
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Richardson, D.B.; Cardis, E. Risk of cancer from occupational exposure to ionising radiation: retrospective cohort study of workers in France, the United Kingdom, and the United States (INWORKS). BMJ 2015, 351. [Google Scholar] [CrossRef] [PubMed]
- Directive 2013/59/Euratom. Available online: https://ec.europa.eu/energy/sites/ener/files/documents/CELEX-32013L0059-EN-TXT.pdf (accessed on 17 December 2017).
- Solution Code. Available online: https://www.dropbox.com/sh/38g9yr34loyeb4h/AADk0q_KMaN7FYKICt0sCkgga?dl=0 (accessed on 17 December 2017).
- Gilmore, G.R. Practical Gamma-Ray Spectrometry, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar] [CrossRef]
- TLD Dosimeter for RE-2000 Readers. Available online: http://nusim.com/wp-content/uploads/2012/07/20996042_TLDdosimeter_EN_A.pdf (accessed on 17 December 2017).
- Noriega Sánchez, K.; Ruiz Manzano, P. Dosimetría de Cristalino de GESTISA y Su Aplicación a Personal. 4º Congreso Conjunto Sociedad Española de Física Médica (SEFM) y la Sociedad Española de Protección Radiológica (SEPR), Valencia, 2015. Available online: http://www.crystallineproject.eu/wp-content/uploads/2015/06/SISTEMA-DOSIMETRIA-GESTISA-Y-APLICACION-AMBITO-SANITARIO-pdf.pdf (accessed on 17 December 2017). (In Spain).
- European Nuclear Society. Film Dosimeter. Available online: https://www.euronuclear.org/info/encyclopedia/f/filmdosimeter.htm (accessed on 17 December 2017).
- LLNL Environmental RPL Dosimeter. Available online: https://www.orau.org/PTP/collection/dosimeters/ron.htm? (accessed on 17 December 2017).
- Dosimetría BeOSL. Available online: http://www.radmedical.com.mx/?page_id=2 (accessed on 17 December 2017).
- Electronic Dosimeter DMC2000. Available online: https://www.dosimetry.com/images/pdf/LIT4319_EDs_combined.pdf (accessed on 17 December 2017).
- Pen Dosimeters. Available online: http://seintl.com/radiationalert/pen_dosimeters.html? (accessed on 17 December 2017).
- Glenn, F.K. Radiation Detection and Measurement, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2000. [Google Scholar]
- Ionization Chamber. Available online: https://www.orau.org/PTP/collection/ionchamber/introionizationchamberr.htm (accessed on 17 December 2017).
- Proportional Counter. Available online: https://www.orau.org/PTP/collection/proportional%20counters/introprops.htm (accessed on 17 December 2017).
- Geiger Muller Counter. Available online: https://www.cpp.edu/~pbsiegel/bio431/texnotes/chapter4.pdf? (accessed on 17 December 2017).
- Scintillation Detectors. Available online: http://www-physics.lbl.gov/~spieler/physics_198_notes/PDF/III-Scint.pdf? (accessed on 17 December 2017).
- Helmuth Spieler. Semiconductor Detector. 1998. Available online: http://www-physics.lbl.gov/~spieler/SLAC_Lectures/PDF/Sem-Det-I.pdf (accessed on 17 December 2017).
- Geiger Counter-Radiation Sensor Board for Arduino and Raspberry Pi. Available online: https://www.cooking-hacks.com/documentation/tutorials/geiger-counter-radiation-sensor-board-arduino-raspberry-pi-tutorial (accessed on 17 December 2017).
- Raspberry Pi. Available online: https://www.raspberrypi.org/ (accessed on 17 December 2017).
- Instadose 1. Available online: https://www.mirion.com/products/instadose-dosimetry-services/ (accessed on 17 December 2017).
- Dosicard. Available online: http://www.canberra.com/products/hp_radioprotection/dosimetry.asp (accessed on 17 December 2017).
- Poudel, S.; Weir, L.; Dowling, D.; Medich, D.C. Changes in Occupational Radiation Exposures after Incorporation of a Real-time Dosimetry System in the Interventional Radiology Suite. Health Phys. 2016, 111, S166–S171. [Google Scholar] [CrossRef] [PubMed]
- Servoli, L.; Bissi, L.; Fabiani, S.; Magalotti, D.; Placidi, P.; Scorzoni, A.; Calandra, A.; Cicioni, R.; Chiocchini, S.; Dipilato, A.C.; et al. Personnel real time dosimetry in interventional radiology. Phys. Med. 2016, 32, 1724–1730. [Google Scholar] [CrossRef] [PubMed]
- Nuclear Open-Source Radiation Monitoring System. Available online: https://www.blackhat.com/docs/us-17/wednesday/us-17-Santamarta-Go-Nuclear-Breaking%20Radition-Monitoring-Devices-wp.pdf (accessed on 17 December 2017).
- Terasaki, K.; Toshioh, F.; Murazaki, H.; Kuramoto, T.; Umezu, Y.; Ishigaki, Y.; Matsumoto, Y. Evaluation of basic characteristics of a semiconductor detector for personal radiation dose monitoring. Radiol. Phys. Technol. 2017, 10, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Ishigaki, Y.; Matsumoto, Y.; Ichimiya, R.; Tanaka, K. Ultra-low-cost radiation monitoring system utilizing smartphone-connected sensors developed with internet community. In Proceedings of the IEEE Sensors Conference, Taipei, Taiwan, 28–31 October 2012; pp. 652–655. [Google Scholar]
- Ishigaki, Y.; Matsumoto, Y.; Ichimiya, R.; Tanaka, K. Development of mobile radiation monitoring system utilizing smartphone and its field tests in Fukushima. IEEE Sens. J. 2013, 13, 3520–3526. [Google Scholar] [CrossRef]
- Raspberry Pi to Arduino Shields Connection Bridge. Available online: https://www.cooking-hacks.com/raspberry-pi-to-arduino-shield-connection-bridge (accessed on 17 December 2017).
- Huawei E173. Available online: https://www.amazon.es/Huawei-E173-M%C3%B3dem-7-2Mbps-blanco/dp/B008BQEFYM (accessed on 17 December 2017).
- Apache. Available online: https://www.apache.org/ (accessed on 17 December 2017).
- PHPMyAdmin. Available online: https://www.phpmyadmin.net/ (accessed on 17 December 2017).
- Async Task—Android. Available online: https://developer.android.com/reference/android/os/AsyncTask.html (accessed on 17 December 2017).
- Intent Class—Android. Available online: https://developer.android.com/reference/android/content/Intent.html (accessed on 17 December 2017).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthcare Professional Category | Effective Dose | Eye Lense Dose | Extremity Dose |
|---|---|---|---|
| Exposed worker A classification | >6 mSv/year | >45 mSv/year | >150 mSv/year |
| Exposed worker B classification | <6 mSv/year | <45 mSv/year | <150 mSv/year |
| Non-exposed workers | <1 mSv/year | <15 mSv/year | <50 mSv/year |
| Job Type | Doctor | Medical Assistant | Operator | Other |
|---|---|---|---|---|
| Outpatient clinic Radiology | 0.0% | 0.40% | 0.0% | 0.0% |
| Hospital Radiology | 2.7% | 1.40% | 0.5% | 0.4% |
| Vascular Radiology | 24.1% | 5.90% | 2.9% | 1.5% |
| Radiotherapy | 0.1% | 2.60% | 0.4% | 0.7% |
| Nuclear Medicine | 1.7% | 50.70% | 36.6% | 13.0% |
| Interventional | 2.2% | 0.40% | 0.0% | 0.1% |
| Others | 0.6% | 0.30% | 0.0% | 0.0% |
| Dosimeter | Range |
|---|---|
| Film and TLD dosimeters | 100 µSv–10 Sv |
| OSL and RPL dosimeters | 10 µSv–10 Sv |
| Self-reading pocket dosimeters | 50 µSv–0.2 Sv |
| Electronic Personal dosimeter | 0.1 µSv–10 Sv |
| Device | Real Time | Reusable | Low-Cost | Internet | Database | Reliability | Smartphone App | Open Source |
|---|---|---|---|---|---|---|---|---|
| TLD Dosimeter | No | Yes | Yes | No | No | Yes | No | No |
| Film Dosimeter | No | No | N/A | No | No | Yes | No | No |
| RPLGD | No | Yes | N/A | No | No | Yes | No | No |
| OSL Dosimeter | No | Yes | N/A | No | No | Yes | No | No |
| Personal Elec. Dosimeter | Yes | Yes | No | No | No | Yes | No | No |
| Pocket Dosimeter | Yes | Yes | Yes | No | No | No | No | No |
| Ionization Chamber | Yes | Yes | No | No | N/A | Yes | No | No |
| Proportional Counter | Yes | Yes | No | No | N/A | Yes | No | No |
| Geiger-Müller Counter | Yes | Yes | No | No | Yes | Yes | No | No |
| Scintillator Counter | Yes | Yes | No | No | N/A | Yes | No | No |
| Semiconductors detector | Yes | Yes | N/A | No | N/A | Yes | No | No |
| Instadose-Mirion | Yes | Yes | N/A | No | Yes | N/A | Yes | No |
| Dosicard-Canberra | Yes | Yes | N/A | No | Yes | N/A | No | No |
| PROPOSED SYSTEM | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Quality Code | Voltage (Kv) | Eavg (keV) | 1st HVL (mm Cu) | 2nd HVL (mm Cu) | Kerma (Air) (µGy/min) Minimum | Kerma (Air) (µGy/min) Maximum |
|---|---|---|---|---|---|---|
| N-80 | 80 | 65 | 0.05776 | 0.619 | 1.9 | 1000 |
| N-300 | 300 | 250 | 6.28 | 6.29 | 2.9 | 450 |
| Quality Code | System Scale | Kerma Air Rate (µGy/h) | Radiation Time |
|---|---|---|---|
| N-80 | 100 | 110–130 | 360 |
| N-80 | 100 | 180–210 | 360 |
| N-300 | 100 | 350–400 | 180 |
| Quality Code | System Scale | Kerma Air Rate (µGy/h) | Radiation Time | NH |
|---|---|---|---|---|
| N-80 | 100 | 110–130 | 360 | 3.37 ± 0.20 |
| N-80 | 100 | 180–210 | 360 | 5.28 ± 0.58 |
| N-300 | 100 | 350–400 | 180 | 10.2 ± 1.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia-Sanchez, A.-J.; Garcia Angosto, E.A.; Moreno Riquelme, P.A.; Serna Berna, A.; Ramos-Amores, D. Ionizing Radiation Measurement Solution in a Hospital Environment. Sensors 2018, 18, 510. https://doi.org/10.3390/s18020510
Garcia-Sanchez A-J, Garcia Angosto EA, Moreno Riquelme PA, Serna Berna A, Ramos-Amores D. Ionizing Radiation Measurement Solution in a Hospital Environment. Sensors. 2018; 18(2):510. https://doi.org/10.3390/s18020510
Chicago/Turabian StyleGarcia-Sanchez, Antonio-Javier, Enrique Angel Garcia Angosto, Pedro Antonio Moreno Riquelme, Alfredo Serna Berna, and David Ramos-Amores. 2018. "Ionizing Radiation Measurement Solution in a Hospital Environment" Sensors 18, no. 2: 510. https://doi.org/10.3390/s18020510
APA StyleGarcia-Sanchez, A.-J., Garcia Angosto, E. A., Moreno Riquelme, P. A., Serna Berna, A., & Ramos-Amores, D. (2018). Ionizing Radiation Measurement Solution in a Hospital Environment. Sensors, 18(2), 510. https://doi.org/10.3390/s18020510