
Chitosan-Based Materials for Peripheral Nerve Repair—New Pre-Clinical Data on Degradation Behavior at the Nerve Repair Site and Critical Opinion on Their Translational Impact
 , ,
, ,
Abstract
1. Introduction
- Aim (1): to observe the degree of material degradation and its subsequent behavior. In order to observe this, we macroscopically evaluated the fate of the material and the properties of the degraded material residues (appearance, haptic) at the different explantation time points, thereby determining the degree of degradation of the conduits.
- Aim (2): to compare uncovered and CNC covered end-to-end repaired median nerve samples, with regard to stereo-morphometrical parameters in order to understand if material degradation interferes with axonal regeneration.
- Aim (3): to compare uncovered and CNC covered nerve tissue and surrounding epineurium for the presence of immune reaction or foreign body response related to material degradation.
2. Results
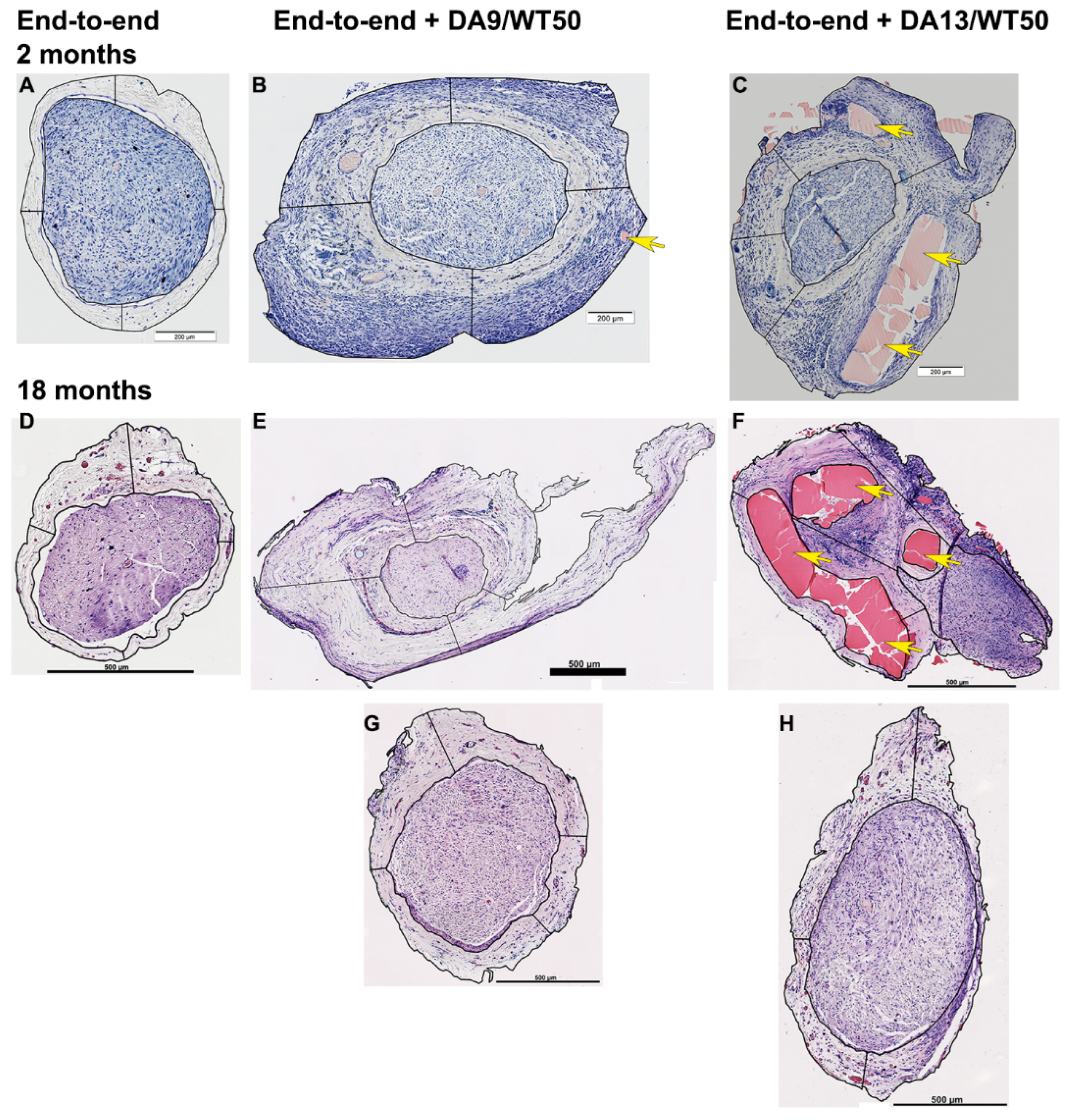
2.1. Macroscopic Assessment of the Implantation Site over Time Confirms Rapid Degradation of DA13/WT50 Variant
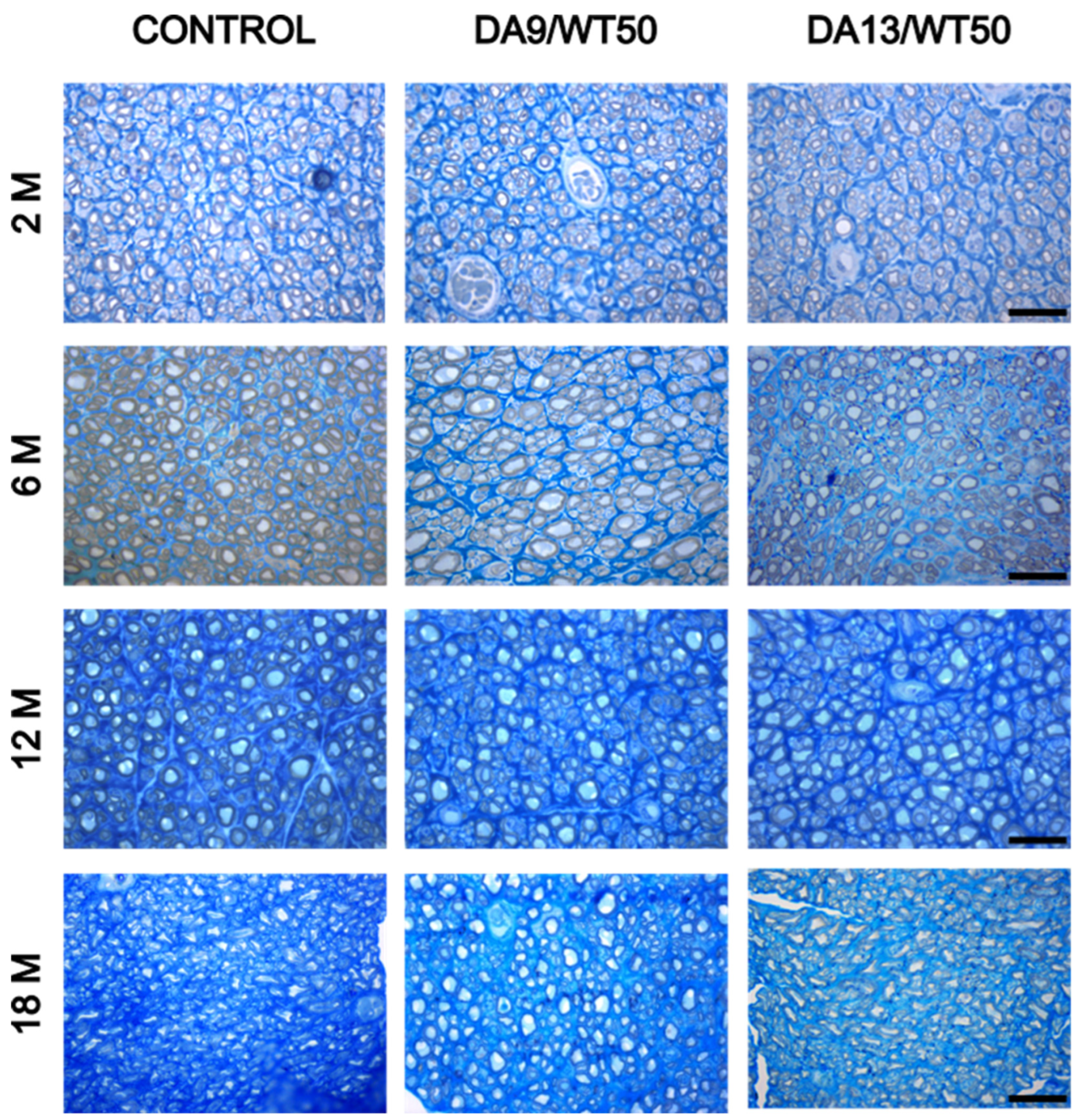
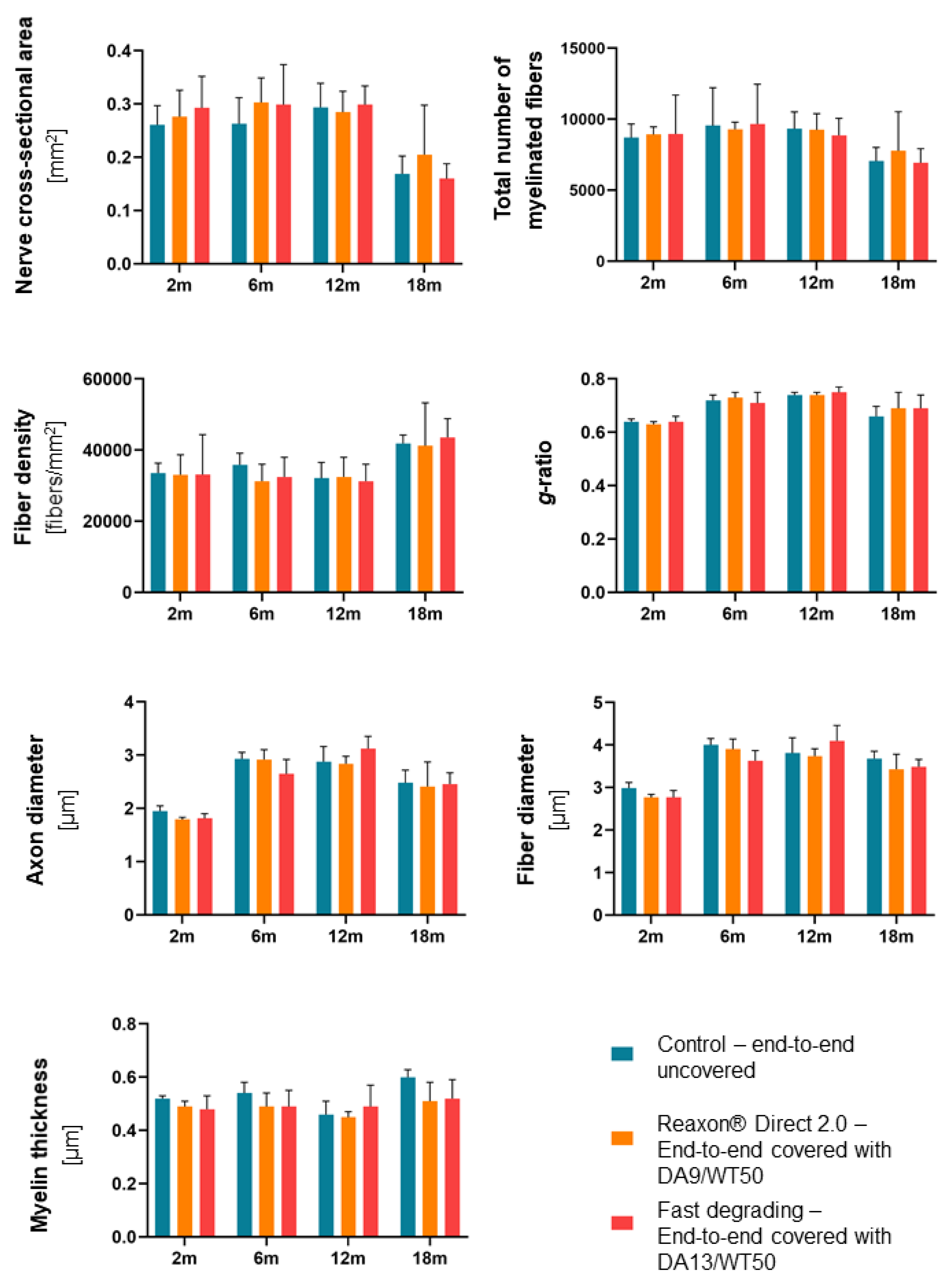
2.2. Histomorphometrical Analysis of Semi-Thin Nerve Cross Sections Distal to the CNC Revealed No Impairment of the Nerve Regeneration Process
2.3. Histological Analysis of the Thickness of the Epineurium Revealed Highest Values in the Reaxon® 2.0—DA9/WT50 Group
2.4. Immunohistological Analysis and Quantification of Activated Macrophages (ED1-Immunopositive Cells) Revealed Pronounced Foreign Body Reaction in the Epineurium Underneath DA9/WT50 Covers
3. Discussion
4. Materials and Methods
4.1. Animals and Surgery
4.2. Fabrication of Reaxon® Direct Variants
4.3. Macroscopic Assessment of the Implantation Site upon Sample Harvest
4.4. Histological Analysis of the Nerve Tissue
4.4.1. Resin Embedding and Stereomorphometrical Analysis
4.4.2. Paraffin Embedding
4.4.3. Giemsa Staining
4.4.4. Immunofluorescence Against ED1
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zou, X.; Dong, Y.; Alhaskawi, A.; Zhou, H.; Ezzi, S.H.A.; Kota, V.G.; Abdulla, M.; Abdalbary, S.A.; Lu, H.; Wang, C. Techniques and graft materials for repairing peripheral nerve defects. Front. Neurol. 2023, 14, 1307883. [Google Scholar] [CrossRef] [PubMed]
- Boecker, A.; Daeschler, S.C.; Kneser, U.; Harhaus, L. Relevance and Recent Developments of Chitosan in Peripheral Nerve Surgery. Front. Cell. Neurosci. 2019, 13, 104. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Stenberg, L.; Gonzalez-Perez, F.; Wrobel, S.; Ronchi, G.; Udina, E.; Suganuma, S.; Geuna, S.; Navarro, X.; Dahlin, L.B.; et al. Chitosan-film enhanced chitosan nerve guides for long-distance regeneration of peripheral nerves. Biomaterials 2016, 76, 33–51. [Google Scholar] [CrossRef]
- Stossel, M.; Metzen, J.; Wildhagen, V.M.; Helmecke, O.; Rehra, L.; Freier, T.; Haastert-Talini, K. Long-Term In Vivo Evaluation of Chitosan Nerve Guide Properties with respect to Two Different Sterilization Methods. Biomed Res. Int. 2018, 2018, 6982738. [Google Scholar] [CrossRef]
- Bocker, A.; Aman, M.; Kneser, U.; Harhaus, L.; Siemers, F.; Stang, F. Closing the Gap: Bridging Peripheral Sensory Nerve Defects with a Chitosan-Based Conduit a Randomized Prospective Clinical Trial. J. Pers. Med. 2022, 12, 900. [Google Scholar] [CrossRef] [PubMed]
- Neubrech, F.; Heider, S.; Harhaus, L.; Bickert, B.; Kneser, U.; Kremer, T. Chitosan nerve tube for primary repair of traumatic sensory nerve lesions of the hand without a gap: Study protocol for a randomized controlled trial. Trials 2016, 17, 48. [Google Scholar] [CrossRef] [PubMed]
- Dietzmeyer, N.; Forthmann, M.; Leonhard, J.; Helmecke, O.; Brandenberger, C.; Freier, T.; Haastert-Talini, K. Two-Chambered Chitosan Nerve Guides with Increased Bendability Support Recovery of Skilled Forelimb Reaching Similar to Autologous Nerve Grafts in the Rat 10 mm Median Nerve Injury and Repair Model. Front. Cell. Neurosci. 2019, 13, 149. [Google Scholar] [CrossRef]
- Aman, M.; Preisner, F.; Mayrhofer-Schmid, M.; Eisa, A.; Schwarz, D.; Kneser, U.; Harhaus, L.; Boecker, A.H. Inferior long-term Results of a Prospective Randomized Controlled Trial initially demonstrating enhanced Sensory Nerve Recovery using a Chitosan Nerve Tube. Plast. Reconstr. Surg. 2024, 155, 364–373. [Google Scholar] [CrossRef]
- Chiriac, S.; Facca, S.; Diaconu, M.; Gouzou, S.; Liverneaux, P. Experience of using the bioresorbable copolyester poly(DL-lactide-epsilon-caprolactone) nerve conduit guide Neurolac for nerve repair in peripheral nerve defects: Report on a series of 28 lesions. J. Hand Surg. Eur. Vol. 2012, 37, 342–349. [Google Scholar] [CrossRef]
- Taras, J.S.; Nanavati, V.; Steelman, P. Nerve conduits. J. Hand Ther. 2005, 18, 191–197. [Google Scholar] [CrossRef]
- Crabtree, J.R.; Mulenga, C.M.; Tran, K.; Feinberg, K.; Santerre, J.P.; Borschel, G.H. Biohacking Nerve Repair: Novel Biomaterials, Local Drug Delivery, Electrical Stimulation, and Allografts to Aid Surgical Repair. Bioengineering 2024, 11, 776. [Google Scholar] [CrossRef] [PubMed]
- Schneider, L.A.; Horner, V.K.; Bonaventura, B.; Simunovic, F. Schmerzen nach Verwendung eines Chitosan-Neurotubes bei Medianusverletzung. Handchir. Mikrochir. Plast. Chir. 2023, 55, 373–375. [Google Scholar] [CrossRef] [PubMed]
- Stocco, E.; Barbon, S.; Emmi, A.; Tiengo, C.; Macchi, V.; De Caro, R.; Porzionato, A. Bridging Gaps in Peripheral Nerves: From Current Strategies to Future Perspectives in Conduit Design. Int. J. Mol. Sci. 2023, 24, 9170. [Google Scholar] [CrossRef] [PubMed]
- Valentino, C.; Vigani, B.; Sandri, G.; Ferrari, F.; Rossi, S. Current Status of Polysaccharides-Based Drug Delivery Systems for Nervous Tissue Injuries Repair. Pharmaceutics 2023, 15, 400. [Google Scholar] [CrossRef]
- Dogny, C.; Andre-Levigne, D.; Kalbermatten, D.F.; Madduri, S. Therapeutic Potential and Challenges of Mesenchymal Stem Cell-Derived Exosomes for Peripheral Nerve Regeneration: A Systematic Review. Int. J. Mol. Sci. 2024, 25, 6489. [Google Scholar] [CrossRef]
- Stocco, E.; Barbon, S.; Emmi, A.; Tiengo, C.; De Caro, R.; Macchi, V.; Porzionato, A. Commentary: Techniques and graft materials for repairing peripheral nerve defects. Front. Neurol. 2024, 15, 1420324. [Google Scholar] [CrossRef]
- Li, L.; Chu, Z.; Li, S.; Zheng, T.; Wei, S.; Zhao, Y.; Liu, P.; Lu, Q. BDNF-loaded chitosan-based mimetic mussel polymer conduits for repair of peripheral nerve injury. Front. Cell Dev. Biol. 2024, 12, 1431558. [Google Scholar] [CrossRef]
- Bianchini, M.; Zinno, C.; Micera, S.; Redolfi Riva, E. Improved Physiochemical Properties of Chitosan@PCL Nerve Conduits by Natural Molecule Crosslinking. Biomolecules 2023, 13, 1712. [Google Scholar] [CrossRef]
- Damonte, G.; Zaborniak, I.; Klamut, M.; Di Lisa, D.; Pastorino, L.; Awsiuk, K.; Wolski, K.; Chmielarz, P.; Monticelli, O. Development of functionalized poly(lactide) films with chitosan via SI-SARA ATRP as scaffolds for neuronal cell growth. Int. J. Biol. Macromol. 2024, 273 Pt 1, 132768. [Google Scholar] [CrossRef]
- Qiu, P.; Wang, L.; Wang, J.; Wang, X.; Xu, J.; An, X.; Han, F.; Dong, Z.; Zhang, J.; Shi, P.; et al. Adhesive chitosan-based hybrid biohydrogels for peripheral nerve injury repair. Front. Cell Dev. Biol. 2024, 12, 1499766. [Google Scholar] [CrossRef]
- Raimondo, S.; Fornaro, M.; Di Scipio, F.; Ronchi, G.; Giacobini-Robecchi, M.G.; Geuna, S. Chapter 5: Methods and protocols in peripheral nerve regeneration experimental research: Part II-morphological techniques. Int. Rev. Neurobiol. 2009, 87, 81–103. [Google Scholar] [PubMed]
- Ronchi, G.; Fregnan, F.; Muratori, L.; Gambarotta, G.; Raimondo, S. Morphological Methods to Evaluate Peripheral Nerve Fiber Regeneration: A Comprehensive Review. Int. J. Mol. Sci. 2023, 24, 1818. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | 2 Months | 6 Months | 12 Months | 18 Months |
|---|---|---|---|---|
| Right median nerve: End-to-end uncovered | N = 4 | N = 4 | N = 4 | N = 6 |
| Left median nerve: Reaxon® Direct 2.0—End-to-end covered with DA9/WT50 | ||||
| Group 2 | ||||
| Right median nerve: Fast degrading—End-to-end covered with DA13/WT50 | N = 4 | |||
| extended Group 2 | ||||
| Right median nerve: Fast degrading—End-to-end covered with DA13/WT50 | N = 4 | N = 5 | N = 6 | |
| Left median nerve: Reaxon® Direct 2.0—End-to-end covered with DA9/WT50 |
| 2 Months | 6 Months | 12 Months | 18-Month | |
|---|---|---|---|---|
| End-to-end uncovered (control) | N = 3 | N = 4 | N = 5 | N = 2 |
| Reaxon® Direct 2.0—End-to-end covered DA9/WT50 | N = 4 | N = 8 | N = 9 | N = 5 |
| Fast degrading— End-to-end covered DA13/WT50 | N = 4 | N = 4 | N = 4 | N = 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ronchi, G.; Ackva, C.; Fregnan, F.; Zen, F.; Muratori, L.; Crosio, A.; Metzen, J.; Haastert-Talini, K. Chitosan-Based Materials for Peripheral Nerve Repair—New Pre-Clinical Data on Degradation Behavior at the Nerve Repair Site and Critical Opinion on Their Translational Impact. Int. J. Mol. Sci. 2025, 26, 1214. https://doi.org/10.3390/ijms26031214
Ronchi G, Ackva C, Fregnan F, Zen F, Muratori L, Crosio A, Metzen J, Haastert-Talini K. Chitosan-Based Materials for Peripheral Nerve Repair—New Pre-Clinical Data on Degradation Behavior at the Nerve Repair Site and Critical Opinion on Their Translational Impact. International Journal of Molecular Sciences. 2025; 26(3):1214. https://doi.org/10.3390/ijms26031214
Chicago/Turabian StyleRonchi, Giulia, Christina Ackva, Federica Fregnan, Federica Zen, Luisa Muratori, Alessandro Crosio, Jennifer Metzen, and Kirsten Haastert-Talini. 2025. "Chitosan-Based Materials for Peripheral Nerve Repair—New Pre-Clinical Data on Degradation Behavior at the Nerve Repair Site and Critical Opinion on Their Translational Impact" International Journal of Molecular Sciences 26, no. 3: 1214. https://doi.org/10.3390/ijms26031214
APA StyleRonchi, G., Ackva, C., Fregnan, F., Zen, F., Muratori, L., Crosio, A., Metzen, J., & Haastert-Talini, K. (2025). Chitosan-Based Materials for Peripheral Nerve Repair—New Pre-Clinical Data on Degradation Behavior at the Nerve Repair Site and Critical Opinion on Their Translational Impact. International Journal of Molecular Sciences, 26(3), 1214. https://doi.org/10.3390/ijms26031214